Abstract
Objectives: (1) To compare cytokine levels in participants with serum urate (SU) < 360 µmol/L, SU ≥ 360 µmol/L with and without monosodium urate (MSU) crystal deposition, respectively, and inter-critical gout. (2) To explore the association of IL-1β, IL-6 and high-sensitivity (hs) CRP with disease duration and the frequency of self-reported gout flares. Methods: Samples and data from 184 participants from studies conducted at Academic Rheumatology, Nottingham City Hospital, were included. Serum high-sensitivity CRP and cytokines involved in the pathogenesis of gouty inflammation were measured. MANCOVA and multivariate linear regression were used, as appropriate, and were adjusted for age, sex, body mass index and self-reported comorbidities. p values were adjusted for multiple testing using a 5% false-discovery rate. Results: Participants with inter-critical gout had greater levels of IL-1β (pcorr = 0.009), IL-18 (pcorr = 0.02), IL-6 (pcorr < 0.0001), IP-10 (pcorr < 0.0001), TNF-α (pcorr < 0.0001), GRO-α (pcorr = 0.0006) and hsCRP (pcorr = 0.009) compared to other groups in multivariate analyses and after correcting for multiple testing. There were no differences in cytokine and hsCRP levels in participants with SU < 360 µmol/L and in participants with SU ≥ 360 µmol/L with or without MSU crystal deposition. There was a statistically non-significant trend for association between IL-6 levels and number of self-reported gout flares. Conclusions: Our findings suggest that gout is a chronic inflammatory condition. The pre-clinical phases of gout were not associated with systemic inflammation, potentially due to the modest sample size. Further research is required to understand whether treating gout by targeting the complete dissolution of MSU crystals would reduce systemic inflammation in inter-critical gout.
1. Introduction
Gout, the most common form of inflammatory arthritis, manifests with intermittent flares and chronic arthritis. It is caused by monosodium urate (MSU) crystal deposition that persists during the inter-critical phase [1]. MSU crystals stimulate the expression of cytokines such as interleukin (IL)-1β, IL-6, IL-8, IL-37, etc. [2,3], during gout flares. Joints with MSU crystal deposition also have local inflammation in the inter-critical phase [4]. However, there are conflicting reports on whether inter-critical gout is associated with systemic inflammation. While some studies have reported no differences in cytokine levels and miRNA concentration between individuals with inter-critical gout and controls, others have observed elevated levels of C-X-C motif chemokine ligand-8 (CXCL-8), IL-18, soluble IL-6 receptor, RANTES, leptin and adiponectin in inter-critical gout [5,6,7,8]. Given the paucity of studies and inconsistent findings, further research in this field is needed. Thus, the aim of this study was to examine the association between inter-critical gout and serum cytokine levels compared to other pathophysiologic states on the normouricemia-to-gout spectrum. Additionally, we explored the association of IL-1β, IL-6 and high-sensitivity C-reactive protein (hsCRP) with disease duration and the number of self-reported gout flares during the previous 12 months.
This paper was presented as an abstract at the American College of Rheumatology’s annual meeting in 2019 [9].
2. Methods
2.1. Study Design: Cross-Sectional Study
Participants: Participants of the Sons of Gout study, the Stop Gout Attack Study (SOGAS) and the Biomarker of Gout study at Academic Rheumatology, Nottingham City Hospital, were included in this study. Details of the Sons of Gout study have been published elsewhere [10]. Briefly, 113 men without gout and with a parent suffering from gout that gave additional serum samples for future research were included in the current study. The SOGAS recruited 60 community-dwelling adults with gout who met the American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) classification criteria [11]. It aimed to evaluate the feasibility of undertaking a trial of fish oil versus olive oil for gout flares. Fifty-four participants in this study gave additional serum samples for future research at the baseline visit, i.e., before receiving any intervention, and were included in this study. The Biomarker of Gout study recruited 17 men with gout who met the ACR/EULAR criteria for gout. Patients who had been prescribed urate-lowering treatment and/or anti-inflammatory drugs (e.g., NSAIDs or colchicine) were eligible to be included in the abovementioned studies. These studies were approved by the Nottingham NHS Research Ethics Committee (References: 15/EM/0316, 15/SC/0730 and 18/EM/0324). The participants included in this current study were classified into four groups:
- Normal SU: SU < 360 µmol/L;
- High SU alone: SU ≥ 360 µmol/L without ultrasound evidence of MSU crystal deposition;
- High SU plus asymptomatic MSU crystal deposition: SU ≥ 360 µmol/L, with deposition of MSU crystals ascertained by ultrasonography, but without gout symptoms;
- Inter-critical gout: All gout cases self-reported ≥1 gout flare in the previous 12 months and had a serum urate (SU) level ≥ 360 µmol/L.
Demographic data, clinical history and gout-related information, if applicable, were collected from all participants at the respective study visits.
2.2. Cytokine Assays
Samples for cytokine measurements were collected in serum-separator tubes, centrifuged, aliquoted and stored at −80 °C. Aliquots (2.0 mL), were sent to Affinity Biomarker Labs for quantitation of GRO-α, IL-1β, IL-6, IL-8, IL-18, IP-10, MCP-1, TNF-α, VEGF-α and hsCRP. Cytokines were measured using the Meso Scale Discovery U-plex array (Meso Scale Diagnostics, Rockville, USA), and hsCRP was measured by Latex agglutination using the CardioPhase® hsCRP kit (Siemens Healthcare SA, Luxembourg) and the ADVIA Clinical Chemistry System (Siemens Healthcare SA, Luxembourg).
2.3. Statistical Analyses
The mean ± standard deviation (SD) and median (interquartile range), and the number (n) and proportion (%), were used to describe continuous and categorial data, respectively. Body mass index (BMI) was calculated from weight and height measured at the research assessment visit. One-way Analysis of Variance (ANOVA) and chi-square tests were used to compare continuous and categorical data, respectively. Cytokine measurements were log(10)-transformed to achieve linearity, and the mean values were compared among groups using One-way ANOVA with Tukey’s post hoc test, and MANCOVA with the following covariates: age (years), gender (male or female), BMI (kg/m2) and self-reported physician-diagnosed comorbidity. p values were adjusted for multiple testing using a 5% false-discovery rate, and adjusted p values less than 0.05 were considered significant. The adjusted analyses were repeated, excluding people with any self-reported physician-diagnosed comorbidity, in a sensitivity analysis. In participants with inter-critical gout, linear regression was used to examine the association of IL-1β, IL-6 and hsCRP with the number of flares during the previous 12 months and disease duration. Statistical analyses were performed using SPSS® Statistics v-24. Graphs were produced using GraphPad Prism v-8.
3. Results
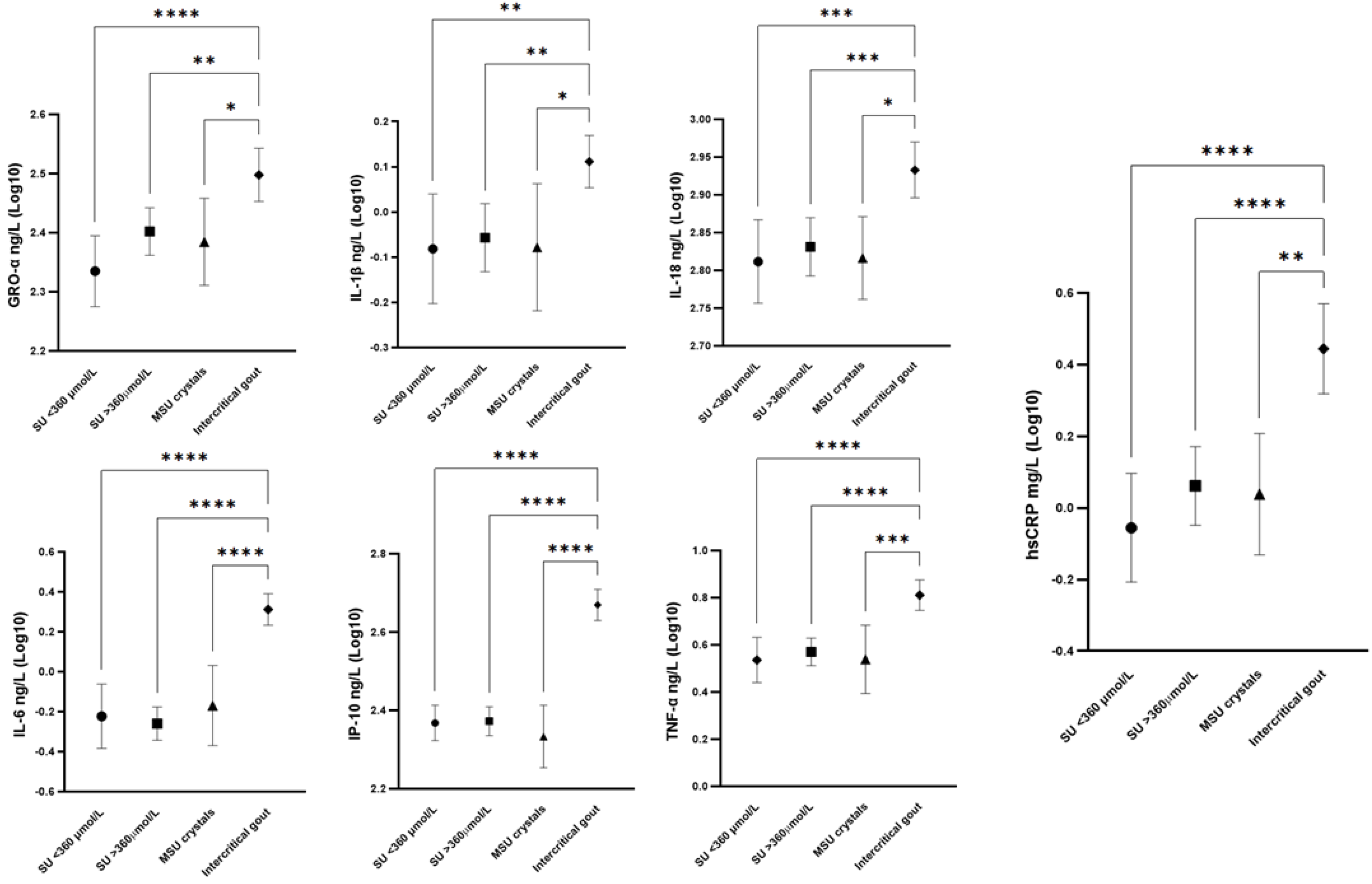
Data for 184 participants were included (Table 1). Participants with gout were older, had a higher BMI, and had a greater comorbidity burden than those without gout (p < 0.001 for all). Twenty-four gout patients were taking urate-lowering treatment. The median (interquartile range) number of gout flares was 3 (1–5). The SU was comparable in the inter-critical gout and other hyperuricaemia groups. Of the cytokines evaluated, GRO-α, IL-1β, IL-18, IL-6, IP-10, MCP1 and TNF-α, as well as hsCRP, showed significantly greater levels in the inter-critical gout group, compared to the normal SU and asymptomatic hyperuricaemia groups, in univariate analysis. There were no differences in cytokine and hsCRP levels among participants with SU < 360 µmol/L, or with SU ≥ 360 µmol/L with and without MSU crystal deposits. After adjusting for age, sex, BMI and self-reported comorbidities, and after correcting for multiple testing, elevated levels of GRO-α, IL-1β, IL-18, IL-6, IP-10, TNF-α and hsCRP remained significantly associated with inter-critical gout (Table 2 and Figure 1). These associations remained statistically significant after excluding cases with any self-reported physician-diagnosed comorbidities.

Table 1.
Demographic characteristics.
Table 2.
Comparison of cytokine measurements and hsCRP among the study groups.
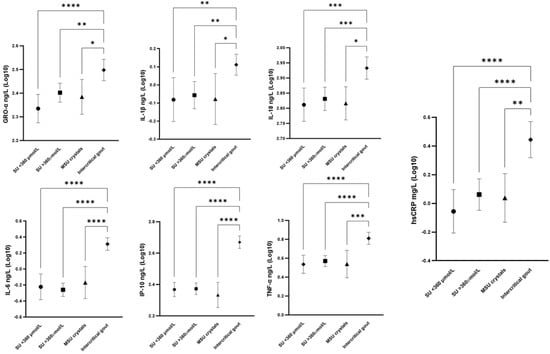
Figure 1.
Cytokine levels of GRO-α, IL-1β, IL-6, IL-18, IP-10, TNF-α and hsCRP in participants with SU < 360 µmol/L, SU ≥ 360 µmol/L, SU ≥ 360 µmol/L + MSU crystals deposits, and inter-critical gout. Values were log(10)-transformed and are shown as the mean (95% CI). Differences among groups were compared using Tukey’s post hoc test. * p < 0.05, ** p< 0.01, *** p < 0.001; **** p < 0.0001.
Based on linear regression adjusted for age, sex, BMI and comorbidities, there was no association between the number of gout flares in the previous 12 months and IL-6 levels (Adjβ (SE) = 0.250 (0.012), p = 0.058). There was no association between any cytokine levels or hsCRP concentration and disease duration.
4. Discussion
In this cross-sectional study, inter-critical gout was associated with systemic inflammation, as measured using cytokines and hsCRP, compared to SU < 360 µmol/L, and to SU ≥ 360 µmol/L with or without MSU crystal deposition. The associations remained statistically significant after excluding cases with self-reported comorbidities in a sensitivity analysis. However, this study found no differences in cytokine and hsCRP levels between people with SU < 360 µmol/L and people with SU ≥ 360 µmol/L either with or without MSU crystal deposition. This observation is inconsistent with prior reports of immune priming induced by soluble and crystalline urate. Due to the cross-sectional nature of this study, our findings do not refute such an effect, because people with immune priming by urate could have seen their condition progress to symptomatic gout, and therefore have been excluded from the asymptomatic groups.
To the best of our knowledge, this is the first study to demonstrate an association between inter-critical gout and elevated IL-1β, IL-6 and hsCRP levels. It is possible that this study found statistically significant differences, while others did not, due to the selection of gout patients with ≥1 flare in the previous 12 months, indicating gout cases with inflammatory tendencies. Previous large studies have reported a high prevalence of tophi, in the included individuals with gout which may indicate a less inflammatory state [5]. Unlike Estevez-Garcia et al. [7], we did not find any significant differences for IL-8 between individuals with normouricaemia, hyperuricaemia and asymptomatic MSU crystal deposition.
Additionally, no association was found of elevated SU and asymptomatic MSU crystal deposition with cytokine levels, when compared to elevated SU alone or SU < 360 µmol/L, in our study. Our observations were limited by the relatively small number of participants. Nevertheless, these findings raise the possibility that the elevation in cytokine levels may be driven by factors other than the interaction between circulating leucocytes and MSU crystal deposits. Such factors may influence the transition from asymptomatic MSU crystal deposition to gout flares. Potential candidate factors include the rs2228611 polymorphism in DNA methyltransferase, which is associated with gout, and nine methylation loci in interleukin-1β-regulating genes that are associated with gouty inflammation [12,13]. Similarly, the rs9952962 polymorphism in the micro-RNA (MIR302F) gene was associated with the asymptomatic-hyperuricaemia-to-gout transition in a genome-wide association study (GWAS) on the Japanese population [14]; and reduced expression of miR-221-5p has been associated with increased levels of cytokines, including IL-1-beta [15]. A pro-inflammatory microbiome has been reported in gout, and this may also contribute [16].
The contribution of some of these cytokines to the inflammatory response in gout flares is more evident, for example, for IL-1β and IL-18 [2,3]. However, the secretion of GRO-α, IL-6 and TNF-α has also been described in monocytes and synoviocytes upon stimulation with MSU crystals [17]. In addition to their chemotactic activity which amplifies the inflammatory response, they have an important role up- and downstream of TLRs and NLRP3 activation. For instance, TNF-α activates NFκB, which regulates the transcription of other pro-inflammatory cytokines and the NLRP3 component [18]. GRO-α and IL-6, on the other hand, work upstream of the activation of the NLRP3 inflammasome by interacting with other receptors, including CXCR2 [19], or by contributing to the signals required for NLRP3 assembly, such as the generation of reactive oxygen species [20], respectively.
Within the limits of the data available to us, it is difficult to comment on whether the systemic inflammation observed in this study resulted from local inflammation, or whether there was a persistent systemic pro-inflammatory state. We believe that this question was addressed in a small study where peripheral blood mononuclear cells (PBMCs) from gout patients in remission, but with MSU crystal deposition, showed activated inflammatory pathways, strengthened inflammatory cell–cell interactions and elevated arachidonic acid metabolic activity [21].
The strengths of this study included community-based recruitment and well-characterized study groups. However, this research had several limitations. First, a single SU measurement was used to classify participants. Second, the sample sizes for several groups, specifically for the group of participants with hyperuricaemia with MSU crystal deposits, were small, and further validation in independent and larger cohorts is required. Third, data on dietary and lifestyle factors were not collected. Fourth, we did not ascertain the date of the latest gout flare in the Biomarker of Gout and SOGAS studies. A more recent gout flare could have influenced cytokine levels. Fifth, we did not collect information on the use of anti-inflammatory drugs, e.g., NSAIDs or colchicine. These are more likely to be used in people with gout, and can reduce cytokine levels in people with gout.
In summary, our study suggests that inter-critical gout is associated with a systemic pro-inflammatory state. Further research is required to explore the underlying reasons and to examine whether treating gout to target serum urate, over a long period of time, with the eventual dissolution of MSU crystals reduces systemic inflammation.
Author Contributions
Conceptualization, A.A. and M.D. and K.M.M.; methodology, G.S.-P. and K.M.M.; software, G.S.-P. and K.M.M.; validation, G.S.-P. and K.M.M.; formal analysis, G.S.-P.; investigation, A.A. and M.D. and K.M.M. and G.S.-P.; resources, A.A. and K.M.M.; data curation, G.S.-P.; writing—original draft preparation, A.A. and G.S.-P.; writing—review and editing, A.A. and M.D. and K.M.M. and G.S.-P.; visualization, G.S.-P.; supervision, A.A. and M.D.; project administration, G.S.-P.; funding acquisition, A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Rosetrees Trust grant number M688 and no specific funding was received for the APC. The collection of samples was undertaken in previous studies funded by Versus Arthritis, Astra Zeneca, and Oxford Immunotec.
Institutional Review Board Statement
This study involved human participants from three clinical studies. Ethical approval was given by the Nottingham NHS Research Ethics Committee (References: 15/EM/0316 (10 September 2015), 15/SC/0730 (27 November 2015) and 18/EM/0324 (12 December 2018)).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is available upon reasonable request.
Conflicts of Interest
A.A. reports royalties from UpToDate, lecture fees from SOBI, and consultancy fees from Eli Lilly and Novartis, all unrelated to the presented work. Other authors report no conflicts of interest.
References
- Dalbeth, N.; Stamp, L. Hyperuricaemia and gout: Time for a new staging system? Ann. Rheum. Dis. 2014, 73, 1598. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, T.; Moriwaki, Y.; Tsutsui, H.; Yamamoto, A.; Takahashi, S.; Tsutsumi, Z.; Ka, T.; Nakanishi, K.; Yamamoto, T. Plasma interleukin (IL)-18 (interferon-γ-inducing factor) and other inflammatory cytokines in patients with gouty arthritis and monosodium urate monohydrate crystal-induced secretion of IL-18. Cytokine 2006, 33, 21–27. [Google Scholar] [CrossRef] [PubMed]
- So, A.K.; Martinon, F. Inflammation in gout: Mechanisms and therapeutic targets. Nat. Rev. Rheumatol. 2017, 13, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Andrés, M.; Bernal, J.-A.; Arenas, M.-D.; Pascual, E. Synovial fluid leukocyte count in asymptomatic hyperuricaemia with crystal deposition: A proof-of-concept study. Rheumatology 2019, 58, 1104–1105. [Google Scholar] [CrossRef]
- Kienhorst, L.B.E.; van Lochem, E.; Kievit, W.; Dalbeth, N.; Merriman, M.E.; Phipps-Green, A.; Loof, A.; van Heerde, W.; Vermeulen, S.; Stamp, L.K.; et al. Gout Is a Chronic Inflammatory Disease in Which High Levels of Interleukin-8 (CXCL8), Myeloid-Related Protein 8/Myeloid-Related Protein 14 Complex, and an Altered Proteome Are Associated With Diabetes Mellitus and Cardiovascular Disease. Arthritis Rheumatol. 2015, 67, 3303–3313. [Google Scholar] [CrossRef]
- Diaz-Torne, C.; Ortiz, M.A.; Garcia-Guillen, A.; Jeria-Navarro, S.; Sainz, L.; Fernandez-Sanchez, S.; Corominas, H.; Vidal, S. The inflammatory role of silent urate crystal deposition in intercritical gout. Rheumatology 2021, 60, 5463–5472. [Google Scholar] [CrossRef]
- Estevez-Garcia, I.O.; Gallegos-Nava, S.; Vera-Pérez, E.; Silveira, L.H.; Ventura-Ríos, L.; Vancini, G.; Hernández-Díaz, C.; Sánchez-Muñoz, F.; Ballinas-Verdugo, M.A.; Gutierrez, M.; et al. Levels of Cytokines and MicroRNAs in Individuals with Asymptomatic Hyperuricemia and Ultrasonographic Findings of Gout: A Bench-to-Bedside Approach. Arthritis Care Res. 2018, 70, 1814–1821. [Google Scholar] [CrossRef]
- Horváthová, V.; Bohatá, J.; Pavlíková, M.; Pavelcová, K.; Pavelka, K.; Šenolt, L.; Stibůrková, B. Interaction of the p.Q141K Variant of the ABCG2 Gene with Clinical Data and Cytokine Levels in Primary Hyperuricemia and Gout. J. Clin. Med. 2019, 8, 1965. [Google Scholar] [CrossRef]
- Sandoval-Plata, G.; Morgan, K.; Guetta-Baranes, T.; Valdes, A.; Doherty, M.; Abhishek, A. Asymptomatic Monosodium Urate Crystal Deposition Associates with Increased Expression of Pro-Inflammatory Genes. Arthritis Rheumatol. 2019, 71 (Suppl. S10). Available online: https://acrabstracts.org/abstract/asymptomatic-monosodium-urate-crystal-deposition-associates-with-increased-expression-of-pro-inflammatory-genes/ (accessed on 20 December 2024).
- Abhishek, A.; Courtney, P.; Jenkins, W.; Sandoval-Plata, G.; Jones, A.C.; Zhang, W.; Doherty, M. Monosodium urate crystal deposits are common in asymptomatic sons of people with gout—The Sons of gout study. Arthritis Rheumatol. 2018, 70, 1847–1852. [Google Scholar] [CrossRef]
- Neogi, T.; A Jansen, T.L.T.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Peng, Y.; Yao, C.; Qing, Y.; Yang, Q.; Guo, X.; Xie, W.; Zhao, M.; Cai, X.; Zhou, J.-G. Association of DNA methyltransferase polymorphisms with susceptibility to primary gouty arthritis. Biomed. Rep. 2016, 5, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-C.; Liao, W.-T.; Wong, M.-C.; Chen, C.-J.; Lee, S.-C.; Yen, J.-H.; Chang, S.-J. Cell lineage-specific methylome and genome alterations in gout. Aging 2021, 13, 3843–3865. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, Y.; Nakaoka, H.; Nakayama, A.; Okada, Y.; Yamamoto, K.; Higashino, T.; Sakiyama, M.; Shimizu, T.; Ooyama, H.; Ooyama, K.; et al. Genome-wide association study revealed novel loci which aggravate asymptomatic hyperuricaemia into gout. Ann. Rheum. Dis. 2019, 78, 1430–1437. [Google Scholar] [CrossRef]
- Li, G.; Zhang, H.; Ma, H.; Qu, S.; Xing, Q.; Wang, G. MiR-221-5p is involved in the regulation of inflammatory responses in acute gouty arthritis by targeting IL-1β. Int. J. Rheum. Dis. 2021, 24, 335–340. [Google Scholar] [CrossRef]
- Chu, Y.; Sun, S.; Huang, Y.; Gao, Q.; Xie, X.; Wang, P.; Li, J.; Liang, L.; He, X.; Jiang, Y.; et al. Metagenomic analysis revealed the potential role of gut microbiome in gout. NPJ Biofilms Microbiomes 2021, 7, 66. [Google Scholar] [CrossRef]
- di Giovine, F.S.; E Malawista, S.; Thornton, E.; Duff, G.W. Urate crystals stimulate production of tumor necrosis factor alpha from human blood monocytes and synovial cells. Cytokine mRNA and protein kinetics, and cellular distribution. J. Clin. Investig. 1991, 87, 1375–1381. [Google Scholar] [CrossRef]
- Hayden, M.S.; Ghosh, S. Regulation of NF-κB by TNF family cytokines. Semin. Immunol. 2014, 26, 253–266. [Google Scholar] [CrossRef]
- Boro, M.; Balaji, K.N. CXCL1 and CXCL2 Regulate NLRP3 Inflammasome Activation via G-Protein–Coupled Receptor CXCR2. J. Immunol. 2017, 199, 1660–1671. [Google Scholar] [CrossRef]
- Kim, J.-A.; Grung, P.; Banskota, S.; Jeong, B.-S.; Nam, T.-G. P057 IL-6 induces NLRP3 inflammasome activation through JAK/STAT3-dependent NOX2 induction in colon epithelial cells. J. Crohn’s Colitis 2017, 11 (Suppl. S1), S106–S107. [Google Scholar] [CrossRef]
- Gu, H.; Yu, H.; Qin, L.; Yu, H.; Song, Y.; Chen, G.; Zhao, D.; Wang, S.; Xue, W.; Wang, L.; et al. MSU crystal deposition contributes to inflammation and immune responses in gout remission. Cell Rep. 2023, 42, 113139. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Gout, Hyperuricemia and Crystal Associated Disease Network. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).