Abstract
Objectives: Identification of monosodium urate (MSU) and calcium pyrophosphate (CPP) crystals in synovial fluid should ideally be performed within 24 h to ensure optimal diagnostic accuracy for gout and CPP arthritis. However, crystal identification is often delayed in community-based healthcare facilities due to limited access to specialists or necessary equipment. This study aimed to determine whether MSU and CPP crystals remain detectable in synovial fluid after two weeks of storage at 4 °C and −20 °C. Methods: Anonymized synovial fluid samples were obtained from Thammasat University Hospital between February and March 2024. All samples underwent an initial round of crystal identification using compensated polarized light microscopy, conducted by two experienced examiners blinded to the clinical diagnosis. Following the initial analysis, each sample was divided into two equal portions and placed in ethylenediaminetetraacetic acid (EDTA)-coated tubes. One portion was stored at 4 °C, while the other was frozen at −20 °C. After two weeks, all samples underwent a second round of crystal identification. Results: Forty-nine samples were included for the first evaluation; MSU and CPP crystals were identified in 14 and 6 samples, respectively. On the second examination, MSU crystals were detectable in 13/14 (92.8%) samples stored at 4 °C and 12/14 (85.7%) samples stored at −20 °C. However, CPP crystals were detectable in 2/6 (33.3%) samples stored at both temperatures. No new crystal formation in initially negative samples was observed. Conclusion: MSU crystals remain detectable in synovial fluid for up to two weeks when stored in a standard refrigerator or freezer. However, the identification rate of CPP crystals tends to decline over this period. These findings may help inform best practices for handling synovial fluid samples in cases where immediate access to a specialist or necessary equipment is unavailable.
1. Introduction
Crystal-induced arthritis includes gout and calcium pyrophosphate deposition disease (CPPD), which are two of the most common joint diseases globally [1]. When monosodium urate (MSU) or calcium pyrophosphate (CPP) crystals accumulate in the joints, an inflammatory process is triggered, resulting in gout flare or acute CPP arthritis, respectively. Crystal-induced arthritis can be debilitating, affecting activities of daily living and work productivity. The identification of MSU and CPP crystals in synovial fluid using polarized light microscopy remains the gold standard for diagnosing gout and CPPD [2]. MSU crystals are characterized by their needle-like shape and strong birefringence. In contrast, CPP crystals appear as rhomboidal or rod-shaped with relatively weak birefringence compared to MSU crystals [3].
Synovial fluid analysis should be performed as soon as possible, ideally within 24 h, to prevent leukocyte degradation and potential crystal dissolution [3]. Specific training in crystal identification by experienced examiners has been shown to improve the accuracy and reliability of crystal detection in synovial fluid [4]. Unfortunately, diagnoses of gout and CPPD are typically made by non-specialist clinicians in community healthcare facilities, where most people with acute arthritis seek medical care. In this setting, access to polarized light microscopy and trained examiners is often limited. In Thailand, synovial fluids are often collected at community healthcare facilities, which lack the capability to perform crystal identification promptly. As a result, specimens are sent to specialized laboratories or referral centers, leading to additional storage and transport time before testing.
Previous research has explored how different storage conditions over different time periods affect the rate of MSU and/or CPP crystal identification in synovial fluid. Over 72 h, both MSU and CPP crystals have been shown to remain stable in fresh synovial fluid when stored at refrigerator temperature (4 °C) [5,6]. Beyond 72 h, the rates of crystal identification varied greatly among studies, mostly due to a wide range in observation periods, storage temperatures, and types of preservative used during storage [7,8]. In a study by Pastor et al., synovial fluid samples were stored at 20 °C and 4 °C using either heparin or ethylenediaminetetraacetic acid (EDTA) as preservatives. MSU crystals remained detectable in over 90% of samples after 7 days, while the detection rate of CPP crystals declined to 67% after 7 days of storage at 20 °C with EDTA as a preservative [9]. For frozen synovial fluid, DMSO appeared to help prevent cell lysis and maintained high crystal identification agreement after 3-month storage [10]. However, DMSO is not commonly available in our local health facilities.
The majority of studies that included CPP crystal identification reported a gradual decline in rates of crystal identification over the period of time between 72 h and up to 8 weeks [9,11,12]. However, one study observed no decline in rates of CPP crystal identification for up to 4 weeks when stored at room temperature [13].
Previous studies that examined MSU crystals found stable rates of MSU crystal identification from 72 h to 8 weeks [9,11]. However, when stored for up to 24 weeks without any preservative, rates of MSU crystal identification declined overtime, ranging between 69% when stored at refrigerator temperature (4 °C) and 89% when stored at room temperature (20 °C) [14].
The heterogeneity of existing studies on the persistence of crystals in stored synovial fluid may prevent clinicians in our community setting from adopting best practices for delayed crystal identification. In Thailand, ethylenediaminetetraacetic acid (EDTA)-coated tubes are widely available in community healthcare facilities. These tubes offer the advantage of preventing clotting, making them more suitable for long-term storage. The typical wait time for specimen shipment for external testing or specialist consultation is within two weeks. Previous studies stored synovial fluid samples at various temperatures, ranging from −70 °C to room temperature. However, the most practical storage temperatures for community-based settings in Thailand are 4 °C (refrigerator) and −20 °C (freezer). It is important to note that maintaining synovial fluid specimens at room temperature (20 °C to 25 °C) is not feasible in Thailand without specialized storage due to the hot and humid tropical climate.
This study aimed to investigate the persistence of MSU and CPP crystals in synovial fluid after two weeks of storage at 4 °C and −20 °C. Findings will help community-based clinicians adopt best practices for accurate crystal identification when specialists and specialized equipment are not immediately available.
2. Methods
2.1. Study Design and Samples
This study was conducted in the laboratory of Thammasat University Hospital, Thailand, between February and March 2024, using a longitudinal design. Synovial fluid samples were collected from the central laboratory at Thammasat University Hospital between 1 February and 31 March 2024. All specimens were obtained from patients who visited the hospital and underwent joint aspiration for any indication. Only leftover samples from routine analysis by the central laboratory were used in this study. Before being provided to the investigators for further analysis, all samples were anonymized by the central laboratory. Specimens with a volume of 5 mL or less were excluded to ensure a sufficient amount of fluid for repeated microscopic examinations.
We calculated the sample size based on the assumption that crystals would persist in synovial fluid stored at −20 °C for two weeks, whereas approximately half of the crystal-positive samples stored at 4 °C would no longer be detectable [9,11]. A minimum of 22 crystal-positive samples was required to detect this difference in proportions with 80% power and a significance level (alpha) of 0.05. We anticipated that 50% of all synovial fluid samples submitted to the lab would be crystal-positive. Based on this assumption, we originally planned to collect 50 consecutive samples, expecting that around 25 would be crystal-positive.
2.2. Procedures
Synovial fluid examination was conducted on the same day that samples were obtained from the hospital laboratory. Specimens were prepared by one of the co-investigators (JS) as soon as possible after collection. Two examiners (KJ and NW) performed crystal identification sequentially using the same compensated polarized light microscope (Olympus CX33, Olympus Corporation, Tokyo, Japan) and slide. First, KJ examined the slide at 400× magnification under both bright and polarized light and recorded the presence or absence of crystals. Subsequently, NW conducted an independent examination, also noting the presence or absence of crystals. In addition to crystal identification, NW performed crystal counting from 10 high-power fields following a pre-set clockwise pattern. KJ and NW were blinded to each other’s findings. For synovial fluid samples without crystals, at least 10 high-power fields were surveyed before the absence of crystals could be reported. The examination typically required no more than 15 min for KJ and no more than 30 min for NW (due to the additional crystal count). In cases of inconsistent findings (i.e., one positive and one negative result), a second examination was planned to be performed by the same two examiners (KJ and NW) within one hour of the initial reading to reach a consensus and minimize the risk of sample deterioration.
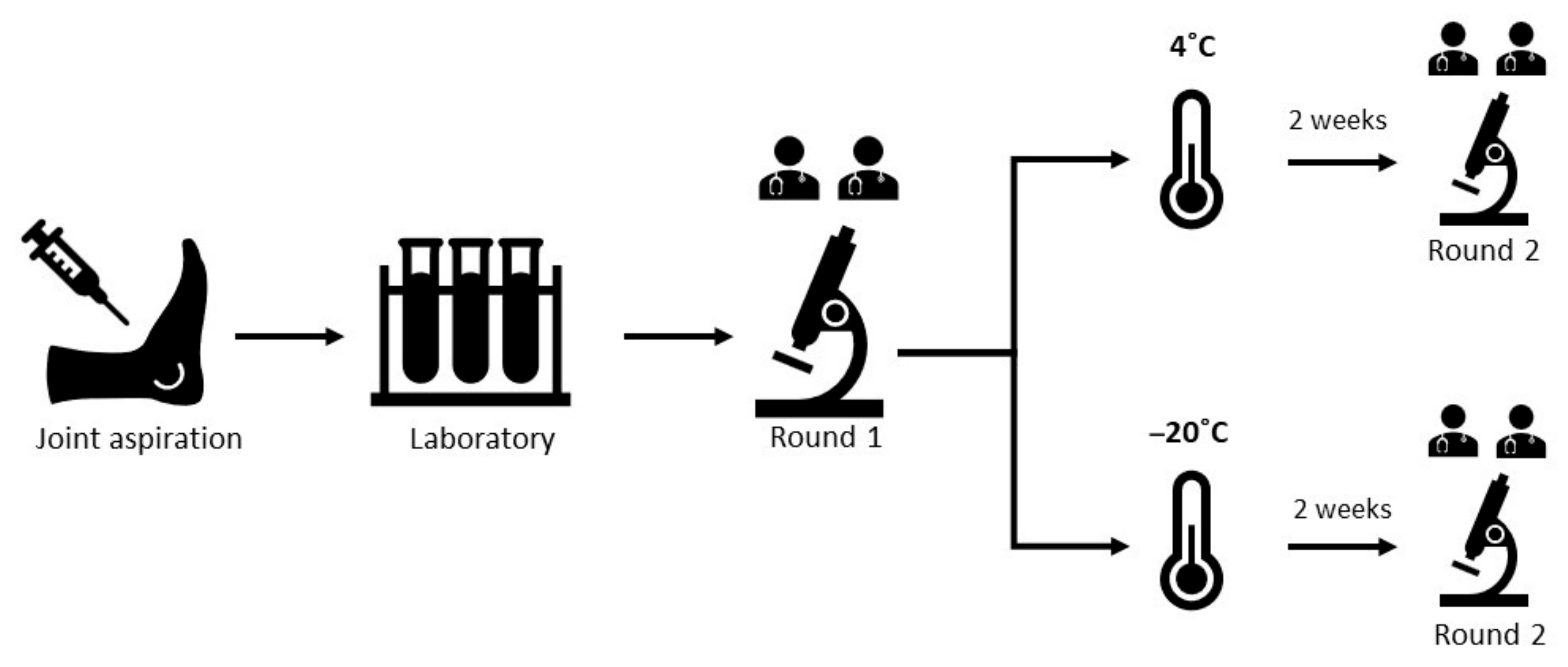
Following the initial analysis, each sample was divided into two equal portions and placed in ethylenediaminetetraacetic acid (EDTA) tubes. One portion was stored at 4 °C, while the other was frozen at −20 °C. To ensure blinding, all samples were labeled in a non-sequential manner by the study coordinator. On day 15, the same two examiners re-evaluated the samples using the same protocol as the baseline examination. Frozen samples were thawed for 20 min before being mounted on a slide for crystal analysis. Both examiners received only prepared slides and were therefore blinded to the storage condition of the samples. Findings were recorded based on the type of crystals present (MSU, CPP, or no crystals) and the number of crystals remaining after storage. The study procedure is summarized in Figure 1.
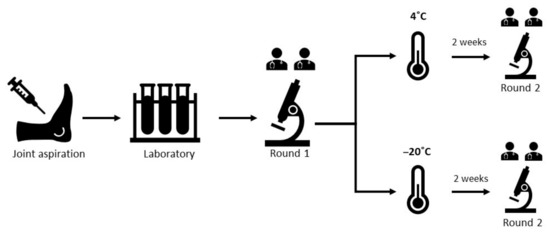
Figure 1.
Study flow chart (N = 49).
2.3. Statistical Analysis
The number and percentage of synovial fluid samples containing each type of crystal were reported at baseline and after two weeks for 4 °C and −20 °C storage groups. The mean and standard deviation (SD) were used to summarize crystal counts at baseline and after two weeks for each storage condition. The number and percentage of samples with a decreased number of crystals were also reported—these included both samples in which crystals became undetectable after storage and those in which crystals remained identifiable but were reduced in number after storage.
We performed McNemar’s test to compare the proportion of samples with detectable crystals at baseline to those after 2-week storage at 4 °C and –20 °C. When expected values in any cell of the 2 × 2 contingency table were too low, a binomial sign test was used instead. Similar comparisons were conducted separately for the proportion of samples with detectable MSU crystals and CPP crystals. A p-value of 0.05 or higher was interpreted as indicating no significant difference in the proportion of detectable crystals between baseline and after storage, whereas a p-value below 0.05 indicated a statistically significant difference. Comparisons between the mean crystal count between baseline and at 2 weeks for both 4 °C and −20 °C storage were performed using paired t-tests.
We also constructed a multivariable logistic regression model to explore factors associated with the persistence of crystals after 2-week storage. The model included all samples that were crystal-positive at baseline (20 stored at 4 °C and 20 stored at –20 °C). The dependent variable was the presence of detectable crystals at 2 weeks. Covariates included storage temperature (4 °C vs. –20 °C), crystal type (MSU vs. CPP), and baseline crystal count. For each covariate, we reported the regression coefficient, odds ratio, 95% confidence interval, and p-value. A p-value < 0.05 was considered indicative of a statistically significant association with crystal persistence at 2 weeks.
All statistical analyses were conducted using IBM SPSS Statistics version 26.
2.4. Ethical Approval
Ethical approval was obtained from the Human Research Ethics Committee of Thammasat University (Medicine) (Study protocol No. MTU-EC-IM-0-249/66). All methods adhered to the ethical principles of the Declaration of Helsinki. As this study used anonymized synovial fluid samples collected during routine care and sent to the hospital’s central laboratory, informed consent from individual participants was not required.
3. Results
A total of 57 anonymized synovial fluid samples were collected from the central laboratory. Eight samples were excluded due to insufficient volume, leaving 49 samples for analysis. At baseline, crystals were identified in 20 samples (40.8%), with MSU crystals detected in 14 samples and CPP crystals in 6 samples (Table 1). The mean (SD) crystal count at baseline was 13.5 (13.5) per 10 high-power fields for MSU crystals and 9.5 (7.9) per 10 high-power fields for CPP crystals.

Table 1.
Crystal identification from synovial fluids at baseline and after 2-week storage (N = 49).
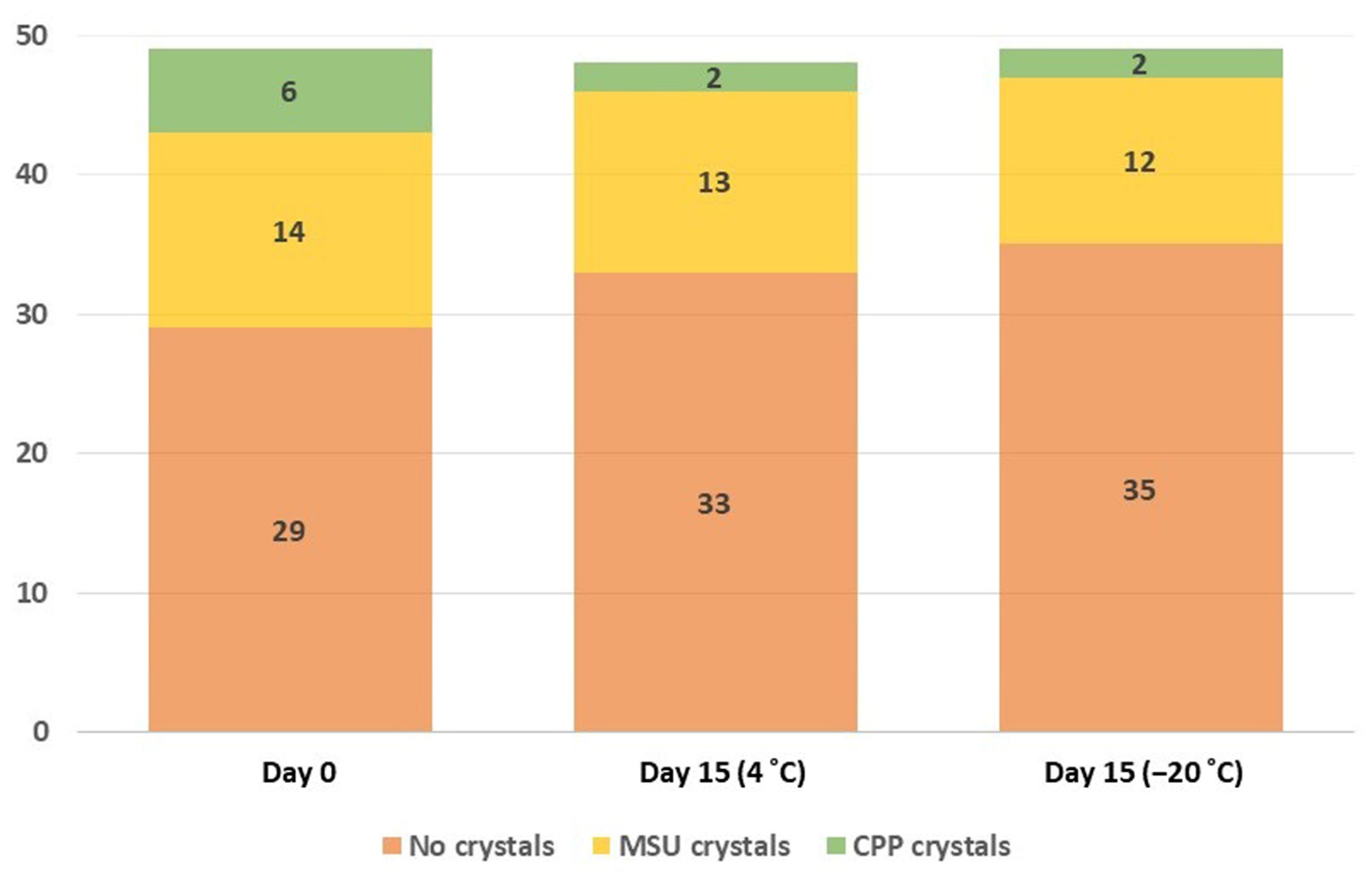
After two weeks, MSU crystals persisted in 13 of 14 samples (92.8%) stored at 4 °C and in 12 of 14 samples (85.7%) stored at −20 °C (Figure 2). In most cases, the number of MSU crystals remained stable: 11 of 14 samples (78.5%) in the 4 °C group and 10 of 14 samples (71.4%) in the −20 °C group (Table 1). The proportion of samples with detectable crystals did not change significantly over two weeks in both storage groups.
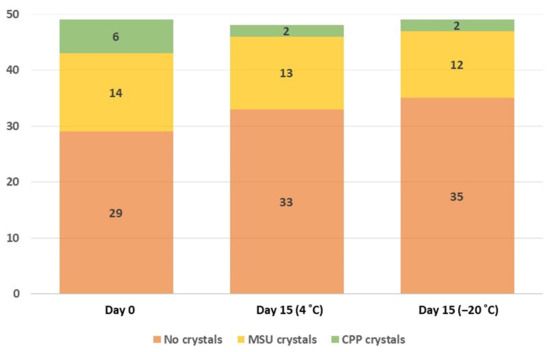
Figure 2.
Number of synovial fluid samples with MSU crystals, CPP Crystals, and no crystals over two weeks at 4 and −20 degrees Celsius.
Among the six samples with CPP crystals at baseline, CPP crystals remained identifiable in two of six samples (33.3%) in both the 4 °C and −20 °C storage groups. However, the decreased proportion of samples with detectable crystals over 2 weeks did reach statistical significance. The number of CPP crystals declined after two weeks in five of six samples from each group (Table 1).
No new crystals were observed in the crystal-negative group during the two-week follow-up. The persistence of MSU and CPP crystals and crystal count in synovial fluid samples are shown in Table 1, Figure 2, and Table S1.
Multivariable logistic regression analysis showed that, compared to CPP crystals, the presence of MSU crystals at baseline was significantly associated with crystal persistence at 2 weeks (OR 15.98; 95% CI 2.87–89.10; p = 0.002) after adjusting for baseline crystal count and storage temperature (Table S2).
4. Discussion
Our study suggested that the rate of MSU crystal identification remained consistent after two weeks of storage at both 4 °C (92.8%) and −20 °C (85.7%). The number of MSU crystals also remained stable in both storage conditions. In contrast, the identification rate of CPP crystals appeared to decline in both storage conditions over two weeks, although statistical significance was not reached. Additionally, most samples with CPP crystals (83.3%) showed a decreased crystal count, regardless of storage temperature (Table 1).
Our findings align with previous reports on the persistence of MSU crystals in synovial fluid over two to eight weeks at room temperature or lower, regardless of the preservative used [9,11]. The stability of MSU crystals can be explained by their temperature-dependent solubility, as urate crystals become less soluble at lower temperatures [15]. Additionally, the use of EDTA-coated containers prevents white blood cell lysis, which may further help preserve neutrophils containing phagocytosed crystals [16]. Another possible explanation for the persistence of identifiable MSU crystals in stored synovial fluid is the continued formation of new crystals during storage, driven by the high urate concentration in synovial fluid from individuals with gout [17]. However, this phenomenon is unlikely to play a significant role in MSU crystal persistence, as the necessary supporting structure for urate crystallization is absent [18]. In our study, we observed a slight increase in the number of MSU crystals after 2 weeks of storage (Table 1). We believe this might be explained by observer bias and the formation of debris clusters that concentrated pre-existing MSU crystals, creating the appearance of a higher crystal count.
The decline in CPP crystal identification and count observed in our study is consistent with previous reports, with a more pronounced decrease occurring after 72 h [9,12]. Given that CPP crystals are primarily identified based on their characteristic morphology rather than strong birefringence, cell clotting and debris formation during storage may have contributed to the decline in CPP crystal detection by obscuring the crystals. CPP crystals are smaller than MSU crystals and have a relatively high surface area due to their rhomboidal or rod-like shapes [19]. Smaller crystals tend to dissolve more quickly in synovial fluid samples [20]. One study suggested that EDTA might increase the solubility of CPP crystals, accelerating their decline in detectability [9]. The use of EDTA-coated containers may have contributed to the marked decrease in CPP crystal identification in our study. Other factors proposed to promote CPP crystal dissolution include decreased pH and a reduction in calcium concentration [20].
Our study suggests that synovial fluid examination for MSU crystal identification remains reliable for at least two weeks when samples are stored in EDTA-coated containers at either 4 °C (refrigerator) or −20 °C (freezer). This storage method allows for relatively accurate delayed MSU crystal identification, particularly in cases requiring referrals or specialist consultation.
However, delayed identification of CPP crystals may be more challenging under these conditions, as CPP crystals were no longer identifiable in more than half of the samples after two weeks in our study. Therefore, our findings support the recommendation that synovial fluid crystal identification should be performed as soon as possible, particularly when CPP arthritis is suspected. In cases where delayed crystal identification is unavoidable, synovial fluid samples should be stored in containers without preservatives or with non-EDTA preservatives. When crystal identification is not immediately available, the clinical diagnosis of CPP arthritis may rely on supporting evidence from radiographic studies or classification criteria [21]. Conversely, a negative synovial fluid examination in patients suspected of having CPP arthritis should be interpreted with caution, taking storage conditions and duration into consideration.
Our study provides practical insights for resource-limited settings where synovial fluid analysis for crystals may be delayed. Standard refrigerators, freezers, and EDTA-coated containers are widely available in most clinical settings. The accuracy of crystal identification in synovial fluid samples largely depends on the skill and experience of the examiner, particularly rheumatologists. However, access to rheumatologists remains a challenge in the Thai public health system due to their low numbers and uneven distribution [22].
One of the strengths of this study is that all examiners were blinded to clinical diagnoses and prior examination results, minimizing bias. Additionally, anonymized synovial fluid samples were consecutively obtained from the central hospital laboratory without specification for clinical diagnosis or department of origin, reducing selection bias and ensuring that these samples reflected general practice in Thailand as accurately as possible. The number of high-power fields required to confirm the presence of crystals has not been widely explored. In our study, a sample was considered negative if no crystals were identified in at least 10 high-power fields. Notably, under this protocol, no inconsistencies were reported between the two examiners. This may provide some support for the adequacy of the 10-field threshold in distinguishing crystal-positive from crystal-negative samples. Nonetheless, further research is needed to confirm its validity.
However, this study had some limitations. The requirement that only synovial fluid samples with a volume greater than 5 mL be included for analysis may have introduced selection bias, as higher-volume samples (i.e., more inflammatory) were more likely to be selected. However, we believe this limitation did not significantly affect our primary objective, which was to evaluate changes in crystal presence over time within the same samples, rather than to compare findings across different samples. The absence of white blood cell counts prevented us from confirming whether the persistence of crystals was due to cellular preservation by EDTA. The smaller-than-anticipated sample size was due to the requirement that only synovial fluid samples with a volume greater than 5 mL be included. Additionally, several samples were not processed because one or more investigators were unavailable at the time the sample arrived at the central laboratory, as analysis had to be performed on the same day of collection. Finally, the single-center design may limit the generalizability of these findings to diverse clinical settings. Expanding this research to multiple centers with a larger sample size could provide more robust data for standardizing synovial fluid preservation methods in future studies.
In conclusion, our study supports the existing understanding that MSU crystals tend to persist in synovial fluid longer than CPP crystals do. The protocol used in our study aligns with practices in most local settings: storage at 4 °C or −20 °C in EDTA-coated containers, with a typical wait time of approximately 1–2 weeks. These findings may help guide best practices for handling synovial fluid samples for delayed examination or specialist consultation when gout is suspected. However, when CPP arthritis is suspected, clinicians should prioritize early synovial fluid examination and interpret negative results with caution.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/gucdd3030012/s1, Table S1. The type of crystal and crystal count in synovial fluid samples at baseline and after 2-week storage at 4 °C and −20 °C. Table S2. Multivariable logistic regression analysis with detectable crystal at 2 weeks set as dependent variable.
Author Contributions
K.J.: conceptualization, formal analysis, investigation, methodology, supervision, writing—review and editing: J.S.; investigation, methodology, project administration, writing—original draft preparation: N.N.; formal analysis, visualization, writing—original draft preparation: N.W.; investigation, methodology, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Human Research Ethics Committee of Thammasat University (Medicine) (Study protocol No. MTU-EC-IM-0-249/66 and date of approval 18 January 2024).
Informed Consent Statement
Informed consent was waived for our study as we performed examinations on anonymized synovial fluid samples that were leftover from routine clinical procedures at the hospital’s central laboratory. The investigators did not have access to any specific patient information from which the samples were taken, and the use of these existing samples incurred no additional burden or risk to the patients. Therefore, individual informed consent was not acquired, as obtaining it would have inevitably required us to gain access to patients’ identifiable information.
Data Availability Statement
All data are available within the article or its Supplementary Materials.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cross, M. Global, regional, and national burden of gout, 1990–2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021. Lancet. Rheumatol. 2024, 6, E507–E517. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castaneda, J.; Coyfish, M.; Guillo, S.; Jansen, T.; Janssens, H.; et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Ann. Rheum. Dis. 2019, 79, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Pascual, E.; Sivera, F.; Andres, M. Synovial fluid analysis for crystals. Curr. Opin. Rheumatol. 2011, 23, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Lumbreras, B.; Pascual, E.; Frasquet, J.; Gonzalez-Salinas, J.; Rodriguez, E.; Hernandez-Aguado, I. Analysis for crystals in synovial fluid: Training of the analysts results in high consistency. Ann. Rheum. Dis. 2005, 64, 612–615. [Google Scholar] [CrossRef]
- Gálvez, J.; Sáiz, E.; Linares, L.F.; Climent, A.; Marras, C.; Pina, M.F.; Castellón, P. Delayed examination of synovial fluid by ordinary and polarised light microscopy to detect and identify crystals. Ann. Rheum. Dis. 2002, 61, 444–447. [Google Scholar] [CrossRef]
- Tausche, A.K.; Gehrisch, S.; Panzner, I.; Winzer, M.; Range, U.; Bornstein, S.R.; Siegert, G.; Wunderlich, C.; Aringer, M. A 3-day delay in synovial fluid crystal identification did not hinder the reliable detection of monosodium urate and calcium pyrophosphate crystals. J. Clin. Rheumatol. Pract. Rep. Rheum. Musculoskelet. Dis. 2013, 19, 241–245. [Google Scholar] [CrossRef]
- Graf, S.W.; Buchbinder, R.; Zochling, J.; Whittle, S.L. The accuracy of methods for urate crystal detection in synovial fluid and the effect of sample handling: A systematic review. Clin. Rheumatol. 2013, 32, 225–232. [Google Scholar] [CrossRef]
- Meyer, M.M.; Marks, L.A.; Aslam, F. Clinical implications of synovial fluid specimen handling for crystal associated arthritides: A systematic review. Int. J. Rheum. Dis. 2020, 24, 10–20. [Google Scholar] [CrossRef]
- Pastor, S.; Bernal, J.A.; Caño, R.; Gómez-Sabater, S.; Borras, F.; Andrés, M. Persistence of Crystals in Stored Synovial Fluid Samples. J. Rheumatol. 2020, 47, 1416–1423. [Google Scholar] [CrossRef]
- Pérez-ruiz, F.; Lopez-bardón, E.; Lioté, F.; Schlesinger, N.; Uhlig, T.; Mateos-mazón, J.J. Utility of dimethylsulfoxide to preserve synovial fluid samples for microcrystal detection and identification. Explor. Musculoskelet. Dis. 2023, 1, 4–10. [Google Scholar] [CrossRef]
- Kerolus, G.; Clayburne, G.; Schumacher, H.R., Jr. Is it mandatory to examine synovial fluids promptly after arthrocentesis? Arthritis Rheum. 1989, 32, 271–278. [Google Scholar] [CrossRef] [PubMed]
- McGill, N.W.; Swan, A.; Dieppe, P.A. Survival of calcium pyrophosphate crystals in stored synovial fluids. Ann. Rheum. Dis. 1991, 50, 939–941. [Google Scholar] [CrossRef] [PubMed]
- McKnight, K.M.; Agudelo, C. Comment on the article by Kerolus et al. Arthritis Rheum. 1991, 34, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Kienhorst, L.B.; Janssens, H.J.; Eijgelaar, R.S.; Radstake, T.R.; van Riel, P.L.; Janssen, M. The detection of monosodium urate crystals in synovial fluid after long-term and varying storage conditions. Jt. Bone Spine 2015, 82, 470–471. [Google Scholar] [CrossRef]
- Chhana, A.; Lee, G.; Dalbeth, N. Factors influencing the crystallization of monosodium urate: A systematic literature review. BMC Musculoskelet. Disord. 2015, 16, 296. [Google Scholar] [CrossRef]
- Salinas, M.; Rosas, J.; Iborra, J.; Manero, H.; Pascual, E. Comparison of manual and automated cell counts in EDTA preserved synovial fluids. Storage has little influence on the results. Ann. Rheum. Dis. 1997, 56, 622–626. [Google Scholar] [CrossRef]
- Beutler, A.M.; Keenan, G.F.; Soloway, S.; Norden, D.; Luchi, M.; Schumacher, H.R., Jr. Soluble urate in sera and synovial fluids from patients with different joint disorders. Clin. Exp. Rheumatol. 1996, 14, 249–254. [Google Scholar]
- Pascual, E.; Ordóñez, S. Orderly arrayed deposit of urate crystals in gout suggest epitaxial formation. Ann. Rheum. Dis. 1998, 57, 255. [Google Scholar] [CrossRef]
- Zell, M.; Aung, T.; Kaldas, M.; Rosenthal, A.K.; Bai, B.; Liu, T.; Ozcan, A.; FitzGerald, J.D. Calcium pyrophosphate crystal size and characteristics. Osteoarthr. Cart. Open 2021, 3, 100133. [Google Scholar] [CrossRef]
- Bennett, R.M.; Lehr, J.R.; McCarty, D.J. Factors affecting the solubility of calcium pyrophosphate dihydrate crystals. J. Clin. Investig. 1975, 56, 1571–1579. [Google Scholar] [CrossRef]
- Abhishek, A.; Tedeschi, S.K.; Pascart, T.; Latourte, A.; Dalbeth, N.; Neogi, T.; Fuller, A.; Rosenthal, A.; Becce, F.; Bardin, T.; et al. The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease. Ann. Rheum. Dis. 2023, 82, 1248–1257. [Google Scholar] [CrossRef]
- Jatuworapruk, K.; Lertnawapan, R.; Watcharajittanont, N.; Gupta, L. Thai rheumatology training, leadership, and gender parity in the last 3 decades: An analysis of a nation-wide database. Int. J. Rheum. Dis. 2023, 26, 2107–2109. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Gout, Hyperuricemia and Crystal Associated Disease Network. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).