
Does Monosodium Urate Crystal Vascular Deposition Exist? Review of the Evidence



Abstract
:1. Introduction
2. Evidence of MSU Crystals in Vessels of Patients with Gout
2.1. Histological Evidence
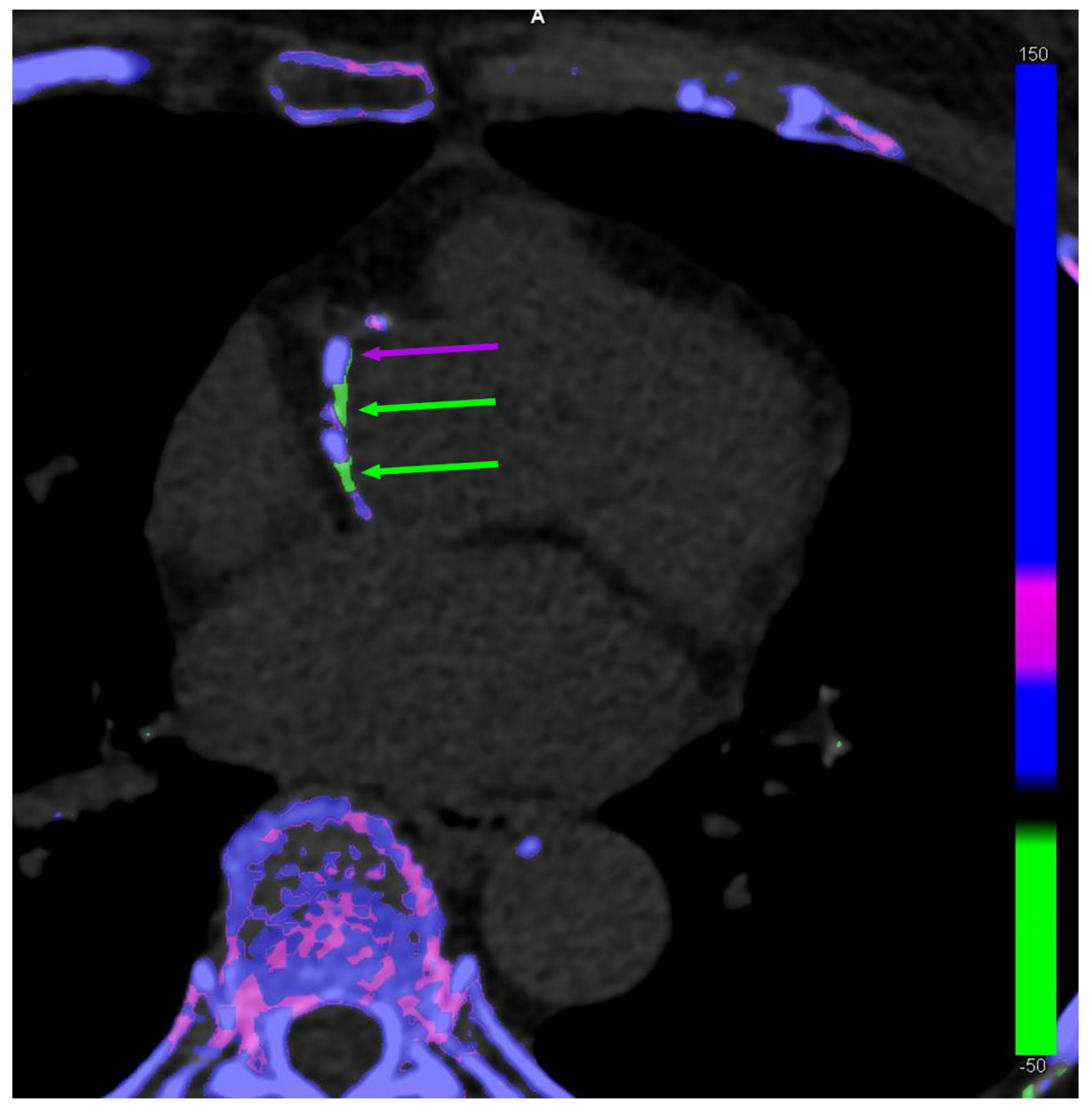
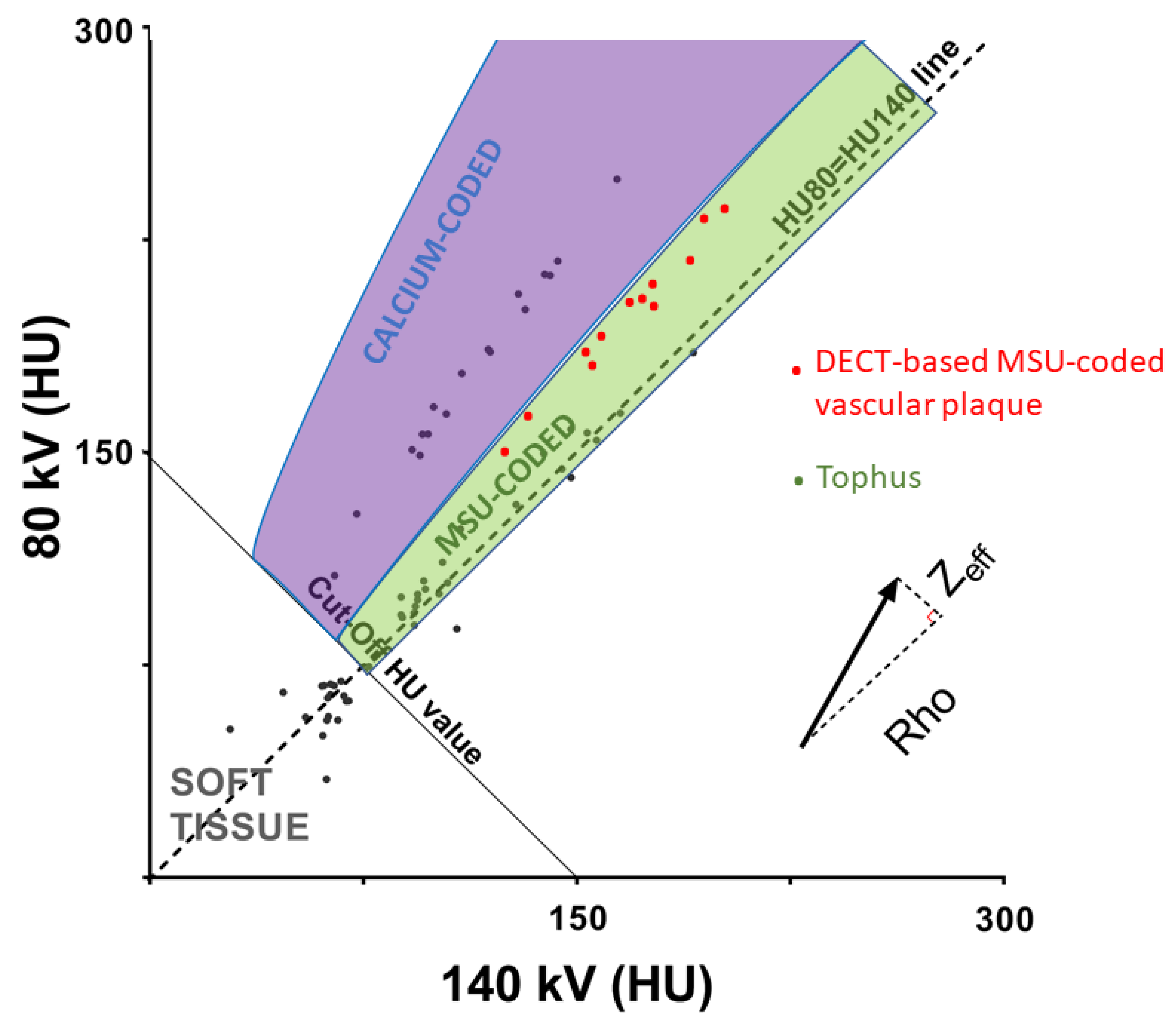
2.2. Imaging Evidence: The Debate on the Evidence Gathered with DECT
3. Evidence of MSU Crystals in Vessels of Patients without Gout
3.1. Histological Evidence
3.2. Biochemical Characterization of Urate Presence in Atherosclerotic Plaques
3.3. Vascular DECT Scans in Patients without Gout

{kind=link}
{kind=link}
| Study | Year | Subjects | Studied Arteries | MSU Crystal Present in Vessels | Technique of Crystal Identification | Urate Plaque Concentration | Xanthine Oxidase Activity | Chemical Characterization of MSU Crystals |
|---|---|---|---|---|---|---|---|---|
| Klauser A.S. et al. [13] | 2019 | 6 cadaveric donors | Coronary and Aorta | Yes | Polarized light microscopy and Dual-energy CT | - | - | No |
| Park J.J. et al. [26] | 2014 | 55 explanted hearts | Coronary | Yes | Polarized light microscopy | - | - | No |
| Patetsios P. et al. [28] | 2001 | 23 endarterectomy samples vs. 10 cadaveric donors | Carotid | Yes | Polarized light microscopy and staining | Increased | Increased | Yes (questionable specificity) |
| Nardi V. et al. [29] | 2022 | 32 endarterectomy samples | Carotid | Unreported | - | Increased | Increased | - |
| Kim S.C. et al. [31] | 2018 | 44 patients | Carotid | No | Dual-energy CT | - | - | - |
4. If DECT-Based MSU-Coded Plaques in Vessels Are Not Made of MSU Crystals, What Are They?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pascart, T.; Liote, F. Gout: State of the art after a decade of developments. Rheumatology 2019, 58, 27–44. [Google Scholar] [CrossRef] [PubMed]
- Andrès, M. Gout and Cardiovascular Disease: Mechanisms, Risk Estimations, and the Impact of Therapies. Gout Urate Cryst. Depos. Dis. 2023, 1, 152–166. [Google Scholar] [CrossRef]
- Ridker, P.M.; Bhatt, D.L.; Pradhan, A.D.; Glynn, R.J.; MacFadyen, J.G.; Nissen, S.E.; PROMINENT, REDUCE-IT, and STRENGTH Investigators. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: A collaborative analysis of three randomised trials. Lancet 2023, 401, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Ramon, A.; Ottaviani, S.; Legrand, J.; Ducoulombier, V.; Houvenagel, E.; Norberciak, L.; Richette, P.; Becce, F.; Ornetti, P.; et al. Association of Specific Comorbidities with Monosodium Urate Crystal Deposition in Urate-Lowering Therapy-Naive Gout Patients: A Cross-Sectional Dual-Energy Computed Tomography Study. J. Clin. Med. 2020, 9, 1295. [Google Scholar] [CrossRef]
- Andres, M.; Bernal, J.A.; Sivera, F.; Quilis, N.; Carmona, L.; Vela, P.; Pascual, E. Cardiovascular risk of patients with gout seen at rheumatology clinics following a structured assessment. Ann. Rheum. Dis. 2017, 76, 1263–1268. [Google Scholar] [CrossRef]
- Calabuig, I.; Martinez-Sanchis, A.; Andres, M. Sonographic Tophi and Inflammation Are Associated with Carotid Atheroma Plaques in Gout. Front. Med. 2021, 8, 795984. [Google Scholar] [CrossRef]
- Hammer, H.B.; Rollefstad, S.; Semb, A.G.; Jensen, G.; Karoliussen, L.F.; Terslev, L.; Haavardsholm, E.A.; Kvien, T.K.; Uhlig, T. Urate crystal deposition is associated with inflammatory markers and carotid artery pathology in patients with intercritical gout: Results from the NOR-Gout study. RMD Open 2022, 8, e002348. [Google Scholar] [CrossRef]
- Marty-Ane, A.; Norberciak, L.; Andres, M.; Houvenagel, E.; Ducoulombier, V.; Legrand, J.; Budzik, J.-F.; Pascart, T. Crystal deposition measured with Dual-Energy Computed Tomography: Association with mortality and cardiovascular risks in gout. Rheumatology 2021, 60, 4855–4860. [Google Scholar] [CrossRef]
- Perez-Ruiz, F.; Martinez-Indart, L.; Carmona, L.; Herrero-Beites, A.M.; Pijoan, J.I.; Krishnan, E. Tophaceous gout and high level of hyperuricaemia are both associated with increased risk of mortality in patients with gout. Ann. Rheum. Dis. 2014, 73, 177–182. [Google Scholar] [CrossRef]
- Khanna, P.; Johnson, R.J.; Marder, B.; LaMoreaux, B.; Kumar, A. Systemic Urate Deposition: An Unrecognized Complication of Gout? J. Clin. Med. 2020, 9, 3204. [Google Scholar] [CrossRef]
- Ahmad, M.I.; Masood, S.; Furlanetto, D.M.; Nicolaou, S. Urate Crystals; Beyond Joints. Front. Med. 2021, 8, 649505. [Google Scholar] [CrossRef] [PubMed]
- Traut, E.F.; Knight, A.A.; Szanto, P.B.; Passerelli, E.W. Specific vascular changes in gout. J. Am. Med. Assoc. 1954, 156, 591–593. [Google Scholar] [CrossRef]
- Klauser, A.S.; Halpern, E.J.; Strobl, S.; Gruber, J.; Feuchtner, G.; Bellmann-Weiler, R.; Weiss, G.; Stofferin, H.; Jaschke, W. Dual-Energy Computed Tomography Detection of Cardiovascular Monosodium Urate Deposits in Patients with Gout. JAMA Cardiol. 2019, 4, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.H.; Lichtenstein, L.; Scott, H.W. Pathologic changes in gout; Survey of eleven necropsied cases. Am. J. Pathol. 1956, 32, 871–895. [Google Scholar] [PubMed]
- Neogi, T.; Jansen, T.L.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout classification criteria: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1789–1798. [Google Scholar] [CrossRef]
- Soare, T.; Iordache, A.M.; Nicolae, G.; Iordache, S.M.; Baciu, C.; Marinescu, S.; Rizac, R.I.; Militaru, M. Identification of Uric Acid Crystals Accumulation in Human and Animal Tissues Using Combined Morphological and Raman Spectroscopy Analysis. Diagnostics 2022, 12, 2762. [Google Scholar] [CrossRef]
- Duewell, P.; Kono, H.; Rayner, K.J.; Sirois, C.M.; Vladimer, G.; Bauernfeind, F.G.; Abela, G.S.; Franchi, L.; Nunez, G.; Schnurr, M.; et al. NLRP3 inflammasomes are required for atherogenesis and activated by cholesterol crystals. Nature 2010, 464, 1357–1361. [Google Scholar] [CrossRef]
- Tall, A.R.; Westerterp, M. Inflammasomes, neutrophil extracellular traps, and cholesterol. J. Lipid Res. 2019, 60, 721–727. [Google Scholar] [CrossRef]
- Dalbeth, N.; Alhilali, M.; Riordan, P.; Narang, R.; Chhana, A.; McGlashan, S.; Doyle, A.; Andres, M. Vascular deposition of monosodium urate crystals in gout: Analysis of cadaveric tissue by dual-energy computed tomography and compensated polarizing light microscopy. Arthritis Rheumatol. 2022, 74, 1295–1296. [Google Scholar] [CrossRef]
- Gawoski, J.M.; Balogh, K.; Landis, W.J. Aortic valvular tophus: Identification by X-ray diffraction of urate and calcium phosphates. J. Clin. Pathol. 1985, 38, 873–876. [Google Scholar] [CrossRef]
- Barazani, S.H.; Chi, W.-W.; Pyzik, R.; Chang, H.; Jacobi, A.; O’Donnell, T.; Fayad, Z.A.; Ali, Y.; Mani, V. Quantification of uric acid in vasculature of patients with gout using dual-energy computed tomography. World J. Radiol. 2020, 12, 184–194. [Google Scholar] [CrossRef]
- Feuchtner, G.M.; Plank, F.; Beyer, C.; Schwabl, C.; Held, J.; Bellmann-Weiler, R.; Weiss, G.; Gruber, J.; Widmann, G.; Klauser, A.S. Monosodium Urate Crystal Deposition in Coronary Artery Plaque by 128-Slice Dual-Energy Computed Tomography: An Ex Vivo Phantom and In Vivo Study. J. Comput. Assist. Tomogr. 2021, 45, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Becce, F.; Ghoshhajra, B.; Choi, H.K. Identification of Cardiovascular Monosodium Urate Crystal Deposition in Patients with Gout Using Dual-Energy Computed Tomography. JAMA Cardiol. 2020, 5, 486. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Carpentier, P.; Choi, H.K.; Norberciak, L.; Ducoulombier, V.; Luraschi, H.; Houvenagel, E.; Legrand, J.; Verclytte, S.; Becce, F.; et al. Identification and characterization of peripheral vascular color-coded DECT lesions in gout and non-gout patients: The VASCURATE study. Semin. Arthritis Rheum. 2021, 51, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Khanna, I.M.V.; Pyzik, R.; Kaufman, A.; Chi, W.; Bagiella, E.; Robson, P.; Ali, Y. Assessing Urate Deposition and Inflammation in the Vasculature of Gout Patients Using Dual Energy Computed Tomography and Positron Emission Tomography Pre and Post Pegloticase—A Pilot Study [abstract]. Arthritis Rheumatol. 2022, 74, 3592–3594. [Google Scholar]
- Park, J.J.; Roudier, M.P.; Soman, D.; Mokadam, N.A.; Simkin, P.A. Prevalence of birefringent crystals in cardiac and prostatic tissues, an observational study. BMJ Open 2014, 4, e005308. [Google Scholar] [CrossRef]
- Bursill, D.; Taylor, W.J.; Terkeltaub, R.; Kuwabara, M.; Merriman, T.R.; Grainger, R.; Pineda, C.; Louthrenoo, W.; Edwards, N.L.; Andres, M.; et al. Gout, Hyperuricemia, and Crystal-Associated Disease Network Consensus Statement Regarding Labels and Definitions for Disease Elements in Gout. Arthritis Care Res. 2019, 71, 427–434. [Google Scholar] [CrossRef]
- Patetsios, P.; Song, M.; Shutze, W.P.; Pappas, C.; Rodino, W.; Ramirez, J.A.; Panetta, T.F. Identification of uric acid and xanthine oxidase in atherosclerotic plaque. Am. J. Cardiol. 2001, 88, 188–191. [Google Scholar] [CrossRef]
- Nardi, V.; Franchi, F.; Prasad, M.; Fatica, E.M.; Alexander, M.P.; Bois, M.C.; Lam, J.; Singh, R.J.; Meyer, F.B.; Lanzino, G.; et al. Uric Acid Expression in Carotid Atherosclerotic Plaque and Serum Uric Acid Are Associated with Cerebrovascular Events. Hypertension 2022, 79, 1814–1823. [Google Scholar] [CrossRef]
- Polito, L.; Bortolotti, M.; Battelli, M.G.; Bolognesi, A. Xanthine oxidoreductase: A leading actor in cardiovascular disease drama. Redox Biol. 2021, 48, 102195. [Google Scholar] [CrossRef]
- Kim, S.C.; Di Carli, M.F.; Garg, R.K.; Vanni, K.; Wang, P.; Wohlfahrt, A.; Yu, Z.; Lu, F.; Campos, A.; Bibbo, C.F.; et al. Asymptomatic hyperuricemia and coronary flow reserve in patients with metabolic syndrome. BMC Rheumatol. 2018, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Budzik, J.F. Dual-energy computed tomography in crystalline arthritis: Knowns and unknowns. Curr. Opin. Rheumatol. 2022, 34, 103–110. [Google Scholar] [CrossRef]
- Park, E.H.; Yoo, W.H.; Song, Y.S.; Byon, J.H.; Pak, J.; Choi, Y. Not All Green Is Tophi: The Importance of Optimizing Minimum Attenuation and Using a Tin Filter to Minimize Clumpy Artifacts on Foot and Ankle Dual-Energy CT. AJR Am. J. Roentgenol. 2020, 214, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, S.N.; Muller, F.C.; Ostergaard, M.; Slot, O.; Moller, J.M.; Borgesen, H.F.; Gosvig, K.K.; Terslev, L. Dual-energy CT in gout patients: Do all colour-coded lesions actually represent monosodium urate crystals? Arthritis Res. Ther. 2020, 22, 212. [Google Scholar] [CrossRef] [PubMed]
- Toprover, M.; Mechlin, M.; Fields, T.; Oh, C.; Becce, F.; Pillinger, M.H. Monosodium urate deposition in the lumbosacral spine of patients with gout compared with non-gout controls: A dual-energy CT study. Semin. Arthritis Rheum. 2022, 56, 152064. [Google Scholar] [CrossRef] [PubMed]
- McQueen, F.M.; Doyle, A.J.; Reeves, Q.; Gamble, G.D.; Dalbeth, N. DECT urate deposits: Now you see them, now you don’t. Ann. Rheum. Dis. 2013, 72, 458–459. [Google Scholar] [CrossRef]
- Nakajima, S.; Ito, H.; Mitsuhashi, T.; Kubo, Y.; Matsui, K.; Tanaka, I.; Fukui, R.; Omori, H.; Nakaoka, T.; Sakura, H.; et al. Clinical application of effective atomic number for classifying non-calcified coronary plaques by dual-energy computed tomography. Atherosclerosis 2017, 261, 138–143. [Google Scholar] [CrossRef]
- Dossing, A.; Muller, F.C.; Becce, F.; Stamp, L.; Bliddal, H.; Boesen, M. Dual-Energy Computed Tomography for Detection and Characterization of Monosodium Urate, Calcium Pyrophosphate, and Hydroxyapatite: A Phantom Study on Diagnostic Performance. Investig. Radiol. 2021, 56, 417–424. [Google Scholar] [CrossRef]
- Andres, M.; Quintanilla, M.-A.; Sivera, F.; Sanchez-Paya, J.; Pascual, E.; Vela, P.; Ruiz-Nodar, J.-M. Silent Monosodium Urate Crystal Deposits Are Associated with Severe Coronary Calcification in Asymptomatic Hyperuricemia: An Exploratory Study. Arthritis Rheumatol. 2016, 68, 1531–1539. [Google Scholar] [CrossRef]
| Study | Year | Subjects | Studied Arteries | MSU Crystal Present in Vessels | Technique of Crystal Identification | Chemical Characterization of MSU Crystals |
|---|---|---|---|---|---|---|
| Traut E.F. et al. [12] | 1954 | 2 cadaveric donors with gout | Coronary | Yes | Polarized light microscopy | No |
| Lievin M.H. et al. [14] | 1956 | 11 cadaveric donors with gout | Coronary and Aorta | No | Polarized light microscopy | No |
| Klauser A.S. et al. [13] | 2019 | 59 Patients | Coronary and Aorta | Yes | Dual-energy CT | No |
| Barazani S. et al. [21] | 2020 | 31 patients | Coronary and Aorta | Yes | Dual-energy CT | No |
| Feuchtner G.M. et al. [22] | 2021 | 37 Patients | Coronary and Aorta | Yes | Dual-energy CT | No |
| Dalbeth N. et al. [19] | 2022 | 6 cadaveric donors | Aorta | No (doubt on 1 crystal) | Polarized light microscopy | No |
| Pascart T. et al. [24] | 2021 | 126 patients | Popliteal arteries | No | Dual-energy CT | Non-invasive (DECT parameter analysis) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascart, T.; Budzik, J.-F. Does Monosodium Urate Crystal Vascular Deposition Exist? Review of the Evidence. Gout Urate Cryst. Depos. Dis. 2023, 1, 208-216. https://doi.org/10.3390/gucdd1030017
Pascart T, Budzik J-F. Does Monosodium Urate Crystal Vascular Deposition Exist? Review of the Evidence. Gout, Urate, and Crystal Deposition Disease. 2023; 1(3):208-216. https://doi.org/10.3390/gucdd1030017
Chicago/Turabian StylePascart, Tristan, and Jean-François Budzik. 2023. "Does Monosodium Urate Crystal Vascular Deposition Exist? Review of the Evidence" Gout, Urate, and Crystal Deposition Disease 1, no. 3: 208-216. https://doi.org/10.3390/gucdd1030017
APA StylePascart, T., & Budzik, J.-F. (2023). Does Monosodium Urate Crystal Vascular Deposition Exist? Review of the Evidence. Gout, Urate, and Crystal Deposition Disease, 1(3), 208-216. https://doi.org/10.3390/gucdd1030017