Abstract
Cerebrovascular disease (CVD) is a global health concern, and early detection is crucial for effective intervention. This case report presents a 31-year-old male patient with multiple cardiac risk factors who underwent positron emission tomography/computed tomography (PET/CT) with 18F-sodium fluoride (NaF) and 18F-fluorodeoxyglucose (FDG) to evaluate for the presence and degree of atherosclerosis in the aorta, carotid arteries, coronary arteries, iliac arteries, and the femoral arteries. Elevated NaF uptake within the bilateral carotid arteries signified substantial ongoing vascular microcalcification. Reduced global brain metabolism and region-specific hypometabolism measured with FDG PET indicated potential cerebrovascular mechanisms that may be influencing neurological function. The findings highlight the potential of emerging PET tracers, such as NaF, to improve the diagnostic accuracy and therapeutic management of CVD. This case emphasizes the importance of a comprehensive diagnostic approach as well as continued investigation into CVD pathophysiology using PET-based techniques, which may guide the development of innovative therapeutic strategies.
1. Introduction
Cerebrovascular disease (CVD) is a major cause of morbidity and mortality worldwide and is often associated with vessel wall abnormalities such as carotid artery atherosclerosis [1]. Early identification of carotid artery atherosclerosis is essential for accurate patient risk stratification while also ensuring the efficiency of lifestyle adjustments and pharmacological measures designed to avert disease progression [2].
18F-fluorodeoxyglucose (FDG) and 18F-sodium fluoride (NaF) are two radiotracers used in hybrid positron emission tomography/computed tomography (PET/CT) imaging that can characterize different molecular targets in carotid artery atherogenesis. FDG, the most widely used PET tracer, is preferentially taken up by cells with high glycolysis rates and becomes trapped within cells as FDG-6-phosphate, resulting in high FDG uptake in areas of inflammation, mediated by activated inflammatory cells [3]. As FDG accumulates intracellularly in activated macrophages, FDG-PET/CT may be used to detect clinically relevant atheromas and predict ischemic risk [4].
FDG-PET/CT exhibits limitations due to its nonspecific uptake, compounded by high cerebral and myocardial physiologic uptake. In addition, though commonly utilized in clinical practice, CT scans often have limitations in detecting calcifications in atherosclerotic plaques due to the presence of blooming artifacts. The resolution of these scans may not be sufficient for the detection of microcalcifications [5]. Consequently, a more sophisticated approach is warranted. This has led to investigations into the potential applications of the NaF-PET/CT imaging technique.
NaF-PET/CT has been proposed as a promising imaging technique for the detection of early stage atherosclerosis [2]. Since the dissociated fluoride ion localizes to areas of active calcium deposition, NaF-PET/CT can detect microcalcification in arterial walls with high sensitivity [2]. Previous studies have utilized NaF-PET in the evaluation of microcirculation in cardiovascular systems, including carotid arteries [6]. For instance, a study by Blomberg et al. revealed that NaF-PET/CT detected microcalcifications in the aortic and coronary arterial vessel walls of healthy subjects and patients with early stage atherosclerosis [7]. Another clinical trial by Joshi et al. demonstrated that NaF-PET was more sensitive than FDG-PET in detecting calcified plaque in the coronary arteries of patients with stable angina [8]. Other studies have investigated the utility of NaF-PET/CT for atherosclerosis detection, demonstrating its ability to identify microcalcification prior to macrocalcification [9,10]. This case report demonstrates the utility of NaF-PET/CT imaging in assessing active carotid atherogenesis in a patient with minimal FDG uptake.
2. Case Report
A 31-year-old male patient with a history of atrial fibrillation (AF) was identified from the Cardiovascular Molecular Calcification Assessed by 18F-NaF PET/CT (CAMONA) study. The patient was enrolled in the study due to his cardiac risk factors, including hypertension, active smoking, a family history of both coronary artery disease and type 1 diabetes, and a body mass index (BMI) of 36.6 kg/m2, which classified him as having class 2 obesity. The patient also reported consuming 15 units of alcohol per week. His physical examination did not reveal any significant findings. Baseline laboratory results revealed normal cholesterol levels with a total cholesterol of 150.8 mg/dL and triglycerides of 141.72 mg/dL.
The patient underwent FDG-PET/CT imaging three hours after receiving 4.0 MBq/kg of FDG intravenously. All imaging was performed on a hybrid PET/CT scanner (GE Discovery 690) following an overnight fast of at least eight hours and confirmation of a blood glucose concentration below 8 mmol/L. Twenty-three days later, NaF-PET/CT was conducted 90 min after the intravenous injection of 2.2 MBq/kg of NaF. Low-dose CT imaging (140 kV, 30–110 mA, noise index 25, 0.8 s/rotation, slice thickness 3.75) was performed for attenuation correction and anatomic correlation. Both PET scans were corrected to account for scatter, attenuation, random coincidences, and scanner dead time.
To assess inflammation and microcalcification as FDG and NaF uptake, respectively, we employed OsiriX MD software v.13.0.1 (Pixmeo SARL, Bernex, Switzerland), a DICOM viewer and image-analysis program. On the fused FDG- and NaF-PET/CT images, regions of interest (ROIs) were delineated around the carotid artery wall (Figure 1). The entire common carotid structure was segmented, extending from the origin of the aortic arch (on the left) or the brachiocephalic trunk (on the right), to the point of carotid bifurcation (at the level of the fourth cervical vertebra or the laryngeal prominence). The mean standardized uptake value (SUVmean) was determined for each region of interest by averaging the values of all voxels contained with the defined boundaries.
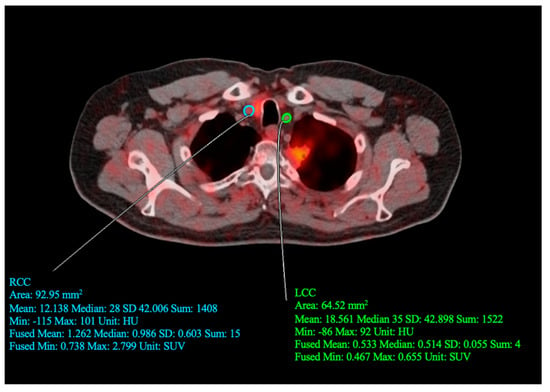
Figure 1.
Quantitative assessment conducted by defining regions of interest (ROI) around the left (LCC) and right (RCC) common carotid arteries. For the drawn RCC ROI, SUVmean = 1.262, SUVmin = 0.0738, and SUVmax = 2.799. For the drawn LCC ROI, SUVmean = 0.533, SUVmin = 0.467, and SUVmax = 0.655.
OsiriX MD was also utilized to perform global assessment of FDG uptake in the brain. CT-based segmentation of cerebral and cerebellar regions of interest were determined using precise anatomical landmarks visible on the fused PET/CT images. Specifically, regions were manually delineated on each sagittal slice (Figure 2). To analyze FDG regional uptake in the brain, quantitative regional analysis was conducted with MIMneuro version 7.1.5 (MIM Software, Inc., Cleveland, OH, USA) through validated methods [11,12]. PET data were mapped on a voxel-to-voxel basis to a standard brain template designed for comparison with an integrated anatomical brain atlas featuring predefined ROIs (Figure 3).
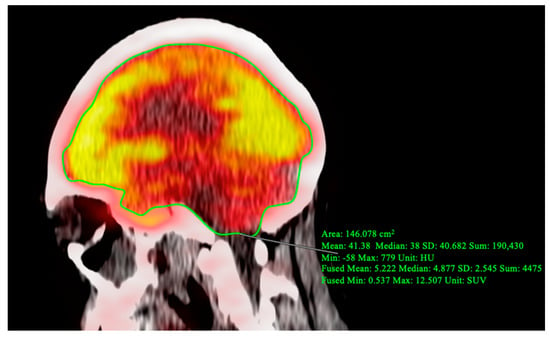
Figure 2.
Region of interest (ROI) delineated for the global assessment of the supratentorial and infratentorial regions of the brain on PET/CT image. For the drawn ROI slice, fused SUVmean = 5.222, indicating hypometabolism.

Figure 3.
Quantitative assessment of FDG-PET/CT slices interpreted by MIMNeuro. (A) Grayscale axial views of FDG-PET/CT. (B) PET/CT shows low FDG uptake, represented by purple and blue contours, in several critical regions. (C) FDG-PET/CT shows low uptake in the medial temporal lobe (yellow), cerebellum (red), and brainstem (blue).
NaF-PET/CT imaging demonstrated elevated NaF uptake in the bilateral carotid arteries, with an average SUVmean of 1.12 for both right and left carotids. This yielded a z-score of 0.012 when compared to a cohort of 38 patients with elevated cardiovascular risk. Conversely, FDG-PET/CT imaging revealed low FDG uptake in the carotid arteries, with an average SUVmean of 0.66 for both right and left carotids and a z-score of −2.32.
Brain FDG-PET/CT demonstrated decreased global brain metabolism, with an average SUVmean of 3.42 when compared to the average of 7.59 SUVmean for a cohort of 38 patients at increased cardiovascular risk. Furthermore, regional hypometabolism was observed, particularly in the brainstem (z score = −1.95), medial temporal lobe (z-score = −1.81), cerebellum (z–score = −2.13), hippocampus (z-score = −2.13), inferior frontal gyrus (z-score = −3.53), lateral orbital gyrus (z-score = −3.24), and putamen (z-score = −2.47).
3. Discussion
This case report describes a 31-year-old patient with AF, cardiac risk factors, and class 2 obesity who was included in the CAMONA study. The NaF and FDG-PET/CT imaging findings revealed high NaF uptake and low FDG uptake in the bilateral carotid arteries. Additionally, we observed decreased global brain metabolism and regional hypometabolism in several critical brain regions of the patient.
Although FDG-PET/CT has found broad application in assessing glucose metabolism and inflammation across a variety of conditions [13], it also has certain limitations. In contrast, NaF-PET/CT targets active areas of calcification, potentially offering a more precise evaluation of the extent and activity of microcalcification in atherosclerosis. This is demonstrated by the pronounced NaF uptake in the patient’s carotid arteries and the concurrent decreased FDG uptake in the brain [7]. In terms of correcting for blood pool activity when measuring microcalcification, it might not be a requisite due to the nearly complete clearance of NaF from the circulation around 45 min post-administration [14,15]. This stands in contrast to the dynamics of FDG, which persists in the bloodstream for a prolonged duration. This extended presence necessitates imaging at later time points and requires an assessment of blood activity to accurately quantify uptake in the atherosclerotic plaques. Despite the potential of the NaF-PET/CT imaging technique, it is important to acknowledge the limitations. The use of the PET/CT scan can be more expensive and involves a higher radiation dose compared to the standard CT scan. Furthermore, alternative methods for early detection of atherosclerosis, such as lab tests of biomarkers and computational simulation of hemodynamic risks, could offer less costly and less radiation-intense options [16,17]. The challenge of in vivo measurements for quantitative evaluation of calcification volume is another limitation, although ex vivo measurements could be considered in future studies.
NaF-PET/CT has emerged as a promising tracer for detecting vascular microcalcification, a significant factor in the development and progression of atherosclerosis and other cardiovascular diseases. The 18F- ion of NaF readily exchanges with the OH- ion of hydroxyapatite, underpinning its uptake at sites of bone turnover. Recently, vascular microcalcification has been identified as a new target for this radiotracer [18]. The presented case underscores the potential of NaF-PET/CT to detect substantial vascular microcalcification in a young patient, suggesting it might offer additional insights into disease processes that traditional tracers such as FDG cannot provide. In our study, the patient did not present any neurological deficits, which typically suggests inactive carotid plaque lesions. However, despite the absence of symptoms, the NaF-PET/CT scans indicated a noteworthy accumulation of activity at the site of the lesion. This observation suggests the existence of microcalcification and signifies an active case despite being asymptomatic. This highlights the subtle, yet potent, potential of NaF-PET/CT scans to detect active, asymptomatic cases where FDG-PET/CT scans may not indicate high activity. The findings suggest that NaF-PET could play a pivotal role in diagnosing and managing CVD where traditional tracers encounter limitations [7].
The findings of this case report may have significant implications for the broader field of CVD diagnosis and management. By detecting vascular microcalcification at an earlier stage with enhanced precision, NaF-PET/CT has the potential to significantly improve risk assessment and enable targeted interventions [19]. Furthermore, the development of novel PET tracers may enable the identification of specific disease mechanisms, such as inflammation or oxidative stress, which could inform the development of personalized treatment strategies tailored to an individual’s unique pathophysiological profile [20].
This unique case raises several questions regarding the potential relationship between vascular calcification, glucose metabolism, and cerebral hypometabolism. Decreased metabolism in the brainstem, medial temporal lobe, cerebellum, and hippocampus could indicate neurodegenerative processes [21], while hypometabolism observed in the inferior frontal gyrus, lateral orbital gyrus, and putamen might reflect a combination of cerebrovascular and neurodegenerative processes [22]. The observed decrease in brain metabolic activity, as reflected in the FDG-PET/CT scans, could be attributed to an array of factors. However, the inherent limitations of a single time point analysis cloud our understanding of whether this detected hypometabolism represents a persistent or transitory phenomenon. For a more comprehensive understanding of the dynamic alterations of metabolic activity in the brain, particularly in relation to vascular calcification, future longitudinal studies employing multiple measurements over extended durations are warranted. Yet, in the absence of exhaustive patient history and supplementary diagnostic tests, pinpointing the exact causality in this specific case remains a complex challenge. This uncertainty highlights the need for more thorough investigations into the reasons behind the observed decrease in brain metabolic activity in FDG-PET/CT scans, especially in asymptomatic patients.
As for the association of the asymptomatic lesion with the 18F-NaF accumulation at the carotid bifurcation, our findings suggest a probable link. The presence of significant carotid artery calcification at a young age may lead to compromised cerebral perfusion, potentially accounting for the observed decline in cerebral metabolic activity. However, given the limited data available from a single case, we cannot conclusively establish this connection. Further studies involving a larger cohort of patients presenting similar characteristics would be instrumental in confirming this relationship and further exploring the underlying mechanisms. This highlights an important area for future research in the field of vascular disease diagnostics.
Moreover, this case report demonstrates the potential clinical utility of emerging PET tracers in detecting and monitoring CVD in younger populations. This is particularly important given the increasing prevalence of risk factors for CVD, such as obesity, hypertension, and diabetes, among younger individuals. Early detection and intervention are crucial to prevent or mitigate the long-term consequences of CVD, and the use of novel PET tracers may facilitate more accurate and timely diagnosis, ultimately leading to improved patient care and outcomes. While our case report indicates potential benefits of using NaF-PET/CT over FDG-PET/CT for identifying microcalcifications, it is important to stress that these findings are drawn from a single case. Therefore, to make definitive assertions about the superiority of one modality over the other, larger-scale, controlled studies with more diverse subject cohorts are required.
In conclusion, this case report highlights the potential of NaF-PET, for improving the diagnosis and management of CVD. This case report also underscores the importance of a comprehensive diagnostic approach and continued research on PET tracers to further refine our understanding of the pathophysiology of CVD and guide the development of innovative therapeutic strategies.
Author Contributions
Conceptualization, A.A.; methodology, E.M.T.; software, E.M.T. and R.C.S.; formal analysis, Y.S.; data curation, E.M.T., R.C.S., O.A.-D. and M.I.; writing—original draft preparation, E.M.T., R.C.S. and A.B.A.; writing—review and editing, V.A.A., W.Y.R., P.F.H.-C. and M.-E.R.; visualization, E.M.T., R.C.S. and M.W.; supervision, T.J.W.; project administration, T.J.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Institutional Review Board approval was obtained. The CAMONA study was approved by the Danish National Committee on Biomedical Research Ethics, registered at ClinicalTrials.gov (NCT01274749) and conducted from 2012 to 2016 in accordance with the Declaration of Helsinki.
Informed Consent Statement
Written informed consent was obtained from all subjects (patients) in this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Writing Group Members; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J. Heart disease and stroke statistics: 2016 update—A report from the American Heart Association. Circulation 2016, 133, e38–360. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.B.; Ng, S.J.; Lau, H.C.; Khanal, K.; Bhattarai, S.; Paudyal, P.; Shrestha, B.B.; Naseer, R.; Sandhu, S.; Gokhale, S.; et al. Emerging PET Tracers in Cardiac Molecular Imaging. Cardiol. Ther. 2023, 12, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Glaudemans, A.W.J.M.; de Vries, E.F.J.; Galli, F.; Dierckx, R.A.J.O.; Slart, R.H.J.A.; Signore, A. The Use of (18)F-FDG-PET/CT for Diagnosis and Treatment Monitoring of Inflammatory and Infectious Diseases. Clin. Dev. Immunol. 2013, 2013, 623036. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.L.; Subramanian, S.S.; Cury, R.C.; Truong, Q.A.; Gardecki, J.A.; Tearney, G.J.; Hoffmann, U.; Brady, T.J.; Tawakol, A. Distribution of Inflammation within Carotid Atherosclerotic Plaques with High-Risk Morphological Features: A Comparison between Positron Emission Tomography Activity, Plaque Morphology, and Histopathology. Circ. Cardiovasc. Imaging 2012, 5, 69–77. [Google Scholar] [CrossRef]
- Liu, H.; Wingert, A.; Wang, J.; Zhang, J.; Wang, X.; Sun, J.; Chen, F.; Khalid, S.G.; Jiang, J.; Zheng, D. Extraction of Coronary Atherosclerotic Plaques From Computed Tomography Imaging: A Review of Recent Methods. Front. Cardiovasc. Med. 2021, 8, 597568. [Google Scholar] [CrossRef] [PubMed]
- Tzolos, E.; Dweck, M.R. 18F-Sodium Fluoride (18F-NaF) for Imaging Microcalcification Activity in the Cardiovascular System. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1620–1626. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, B.A.; Thomassen, A.; de Jong, P.A.; Simonsen, J.A.; Lam, M.G.E.H.; Nielsen, A.L.; Mickley, H.; Mali, W.P.T.M.; Alavi, A.; Høilund-Carlsen, P.F. Impact of Personal Characteristics and Technical Factors on Quantification of Sodium 18F-Fluoride Uptake in Human Arteries: Prospective Evaluation of Healthy Subjects. J. Nucl. Med. 2015, 56, 1534–1540. [Google Scholar] [CrossRef]
- Joshi, N.V.; Vesey, A.T.; Williams, M.C.; Shah, A.S.V.; Calvert, P.A.; Craighead, F.H.M.; Yeoh, S.E.; Wallace, W.; Salter, D.; Fletcher, A.M.; et al. 18F-Fluoride Positron Emission Tomography for Identification of Ruptured and High-Risk Coronary Atherosclerotic Plaques: A Prospective Clinical Trial. Lancet 2014, 383, 705–713. [Google Scholar] [CrossRef]
- Høilund-Carlsen, P.F.; Piri, R.; Gerke, O.; Sturek, M.; Werner, T.J.; Revheim, M.-E.; Alavi, A. NaF-PET Imaging of Atherosclerosis Burden. J. Imaging 2023, 9, 31. [Google Scholar] [CrossRef]
- Paydary, K.; Revheim, M.-E.; Emamzadehfard, S.; Gholami, S.; Pourhassan, S.; Werner, T.J.; Høilund-Carlsen, P.F.; Alavi, A. Quantitative Thoracic Aorta Calcification Assessment by 18F-NaF PET/CT and Its Correlation with Atherosclerotic Cardiovascular Disorders and Increasing Age. Eur. Radiol. 2021, 31, 785–794. [Google Scholar] [CrossRef]
- Teichner, E.M.; You, J.C.; Hriso, C.; Wintering, N.A.; Zabrecky, G.P.; Alavi, A.; Bazzan, A.J.; Monti, D.A.; Newberg, A.B. Alterations in Cerebral Glucose Metabolism as Measured by 18F-Fluorodeoxyglucose-PET in Patients with Persistent Postconcussion Syndrome. Nucl. Med. Commun. 2021, 42, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Partovi, S.; Yuh, R.; Pirozzi, S.; Lu, Z.; Couturier, S.; Grosse, U.; Schluchter, M.D.; Nelson, A.; Jones, R.; O’Donnell, J.K.; et al. Diagnostic Performance of an Automated Analysis Software for the Diagnosis of Alzheimer’s Dementia with 18F FDG PET. Am J. Nucl. Med. Mol. Imaging 2017, 7, 12–23. [Google Scholar] [PubMed]
- Jadvar, H.; Alavi, A.; Gambhir, S.S. 18F-FDG Uptake in Lung, Breast, and Colon Cancers: Molecular Biology Correlates and Disease Characterization. J. Nucl. Med. 2009, 50, 1820–1827. [Google Scholar] [CrossRef]
- Irkle, A.; Vesey, A.T.; Lewis, D.Y.; Skepper, J.N.; Bird, J.L.E.; Dweck, M.R.; Joshi, F.R.; Gallagher, F.A.; Warburton, E.A.; Bennett, M.R.; et al. Identifying Active Vascular Microcalcification by 18F-Sodium Fluoride Positron Emission Tomography. Nat. Commun. 2015, 6, 7495. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, B.A.; Thomassen, A.; Takx, R.A.P.; Vilstrup, M.H.; Hess, S.; Nielsen, A.L.; Diederichsen, A.C.P.; Mickley, H.; Alavi, A.; Høilund-Carlsen, P.F. Delayed Sodium 18F-Fluoride PET/CT Imaging Does Not Improve Quantification of Vascular Calcification Metabolism: Results from the CAMONA Study. J. Nucl. Cardiol. 2014, 21, 293–304. [Google Scholar] [CrossRef]
- Leng, X.; Lan, L.; Ip, V.H.L.; Liu, H.; Abrigo, J.; Liebeskind, D.S.; Wong, L.K.S.; Leung, T.W. Noninvasive Fractional Flow in Intracranial Atherosclerotic Stenosis: Reproducibility, Limitations, and Perspectives. J. Neurol. Sci. 2017, 381, 150–152. [Google Scholar] [CrossRef]
- Leng, X.; Lan, L.; Ip, H.L.; Abrigo, J.; Scalzo, F.; Liu, H.; Feng, X.; Chan, K.L.; Fan, F.S.Y.; Ma, S.H.; et al. Hemodynamics and Stroke Risk in Intracranial Atherosclerotic Disease. Ann. Neurol. 2019, 85, 752–764. [Google Scholar] [CrossRef]
- Beheshti, M.; Saboury, B.; Mehta, N.N.; Torigian, D.A.; Werner, T.; Mohler, E.; Wilensky, R.; Newberg, A.B.; Basu, S.; Langsteger, W.; et al. Detection and Global Quantification of Cardiovascular Molecular Calcification by Fluoro18-Fluoride Positron Emission Tomography/Computed Tomography--A Novel Concept. Hell J. Nucl. Med. 2011, 14, 114–120. [Google Scholar]
- Dweck, M.R.; Chow, M.W.L.; Joshi, N.V.; Williams, M.C.; Jones, C.; Fletcher, A.M.; Richardson, H.; White, A.; McKillop, G.; van Beek, E.J.R.; et al. Coronary Arterial 18F-Sodium Fluoride Uptake: A Novel Marker of Plaque Biology. J. Am. Coll. Cardiol. 2012, 59, 1539–1548. [Google Scholar] [CrossRef]
- Tawakol, A.; Fayad, Z.A.; Mogg, R.; Alon, A.; Klimas, M.T.; Dansky, H.; Subramanian, S.S.; Abdelbaky, A.; Rudd, J.H.F.; Farkouh, M.E.; et al. Intensification of Statin Therapy Results in a Rapid Reduction in Atherosclerotic Inflammation: Results of a Multicenter Fluorodeoxyglucose-Positron Emission Tomography/Computed Tomography Feasibility Study. J. Am. Coll. Cardiol. 2013, 62, 909–917. [Google Scholar] [CrossRef]
- Cistaro, A.; Pagani, M.; Montuschi, A.; Calvo, A.; Moglia, C.; Canosa, A.; Restagno, G.; Brunetti, M.; Traynor, B.J.; Nobili, F.; et al. The Metabolic Signature of C9ORF72-Related ALS: FDG PET Comparison with Nonmutated Patients. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Marquié, M.; Normandin, M.D.; Vanderburg, C.R.; Costantino, I.M.; Bien, E.A.; Rycyna, L.G.; Klunk, W.E.; Mathis, C.A.; Ikonomovic, M.D.; Debnath, M.L.; et al. Validating Novel Tau Positron Emission Tomography Tracer [F-18]-AV-1451 (T807) on Postmortem Brain Tissue. Ann Neurol 2015, 78, 787–800. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).