Abstract
Bisphosphonates remain a first-line treatment for osteoporosis. The most-widely used is zoledronate, which is well tolerated by most patients, but may rarely cause acute inflammatory reactions, which resemble those of large vessel vasculitis (LVV). We report a third case of LVV associated with zoledronic acid infusion, presenting with a 2-week history of fever up to 40 °C, flu-like symptoms, left jaw pain, myalgia, arthralgia, ankle stiffness in the morning, and intermittent claudication, diagnosed by the hybrid imaging modality 18F-FDG PET/CT with isolated lower extremity involvement and successfully treated with glucocorticoids.
1. Introduction
Osteoporosis is a progressive metabolic bone disease that decreases bone mineral density, with deterioration of the bone structure, which leads to fractures with minor trauma. Approximately one in two women and one in five men will sustain one or more fragility fractures in their lifetime [1]. In most people at risk of fragility fracture, antiresorptive therapy with bisphosphonates is the first-line option. Bisphosphonates’ positive effects persist for several years after discontinuation [2]. When making decisions regarding therapy, patient preferences, compliance with oral drugs, and specific clinical factors should be taken into account. The therapy includes zoledronic acid, which has been shown to reduce the incidence of vertebral, non-vertebral, and hip fractures in postmenopausal women with osteoporosis. As a rule, zoledronic acid is well tolerated, but may cause a well-known acute-phase reaction (flu-like symptoms) lasting up to 7 days. However, there are extremely rare side effects such as LVV [1]. Two such LVV cases have been previously reported in the literature [3,4]. We report the first case of LVV secondary to zoledronic acid infusion in Russia.
2. Case Presentation
A 52-year-old Caucasian woman presented to our hospital complaining of a 2-week history of fever up to 40 °C, flu-like symptoms, left jaw pain, arthralgia, and ankle stiffness in the morning, as well as calve pain aggravated by walking. The symptoms appeared the day after the first zoledronic acid infusion for osteoporosis (Figure 1). For fever, the patient received therapy with Ibuprofen with short-term relief. Left jaw pain was associated with dental intervention 1.5 months earlier.
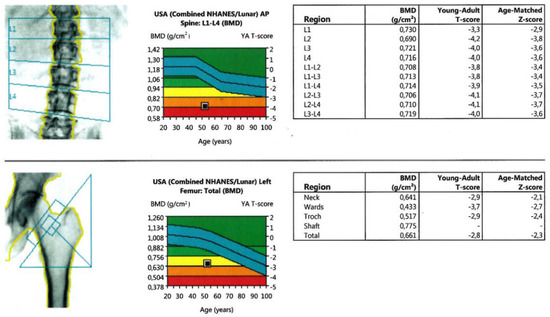
Figure 1.
Bone densitometry results. Decreased bone density indicates severe osteoporosis (T-score is below—2.5 SD).
The patient’s past medical history also includes ovary-sparing hysterectomy due to uterine bleeding during C-section at the age of 36; no hormone therapy was offered. Subsequently, she suffered from obesity, thyroid nodules, and vitamin D deficiency. She had several arm fractures at the age of 6–13. Other conditions, including chronic liver and kidney disease, parathyroid disorders, and chronic diarrhea were denied. Family history represents a hip fracture in her grandmother at the age of 92.
More than 10 years ago, the molar teeth of the upper jaw were removed due to a root cyst that had grown into the maxillary sinus. At that moment, they were under orthopedic crowns. After the teeth’s removal, an oro-antral anastomosis was formed. Then, a sinus lift was performed (subantral augmentation using a xenograft). Dental implants were also loaded. After 5 years, peri-implantitis occurred, and the implants were removed.
The treatment history includes Semaglutide injections and vitamin D 5000IU per day. No glucocorticoid therapy was received.
On admission, the body temperature was 38.3 °C and decreased to normal within 7 h after paracetamol. According to the numeric rating scale from 0 to 10, the pain was rated 3. Physical examination revealed pain under the right ribs; hyperthermia in both the ankle and knee joints; and mild edema in the feet, ankles, and legs.
A significant decrease in bone mineral density in our patient at a young age (<65 years) made us suspect secondary osteoporosis. We ruled out a wide range of conditions and diseases based on a thorough laboratory investigation: vitamin D deficiency, hyperprolactinemia, hyperparathyroidism, thyrotoxicosis, coeliac disease, multiple myeloma and mastocytosis, and vitamin A toxicity. Serum levels of 25-hydroxyvitamin D, parathyroid hormone, albumin-corrected calcium, glucose, prolactin, thyroid function tests, serum protein electrophoresis, serum-free light chain assay, tissue transglutaminase antibodies, vitamin A, and tryptase were normal. Urinary calcium and phosphorus excretion were unremarkable. Only primary hypogonadism was detected: E2 < 55 pmol/L, FSH 132 mIU/mL, LH 45.30 mIU/mL. Given low clinical suspicion for Cushing disease/syndrome, a dexamethasone suppression test was not performed.
We know that the duration of flu-like manifestations is 3–7 days after zoledronic acid infusion. However, the duration of the episode in our patient was longer, which motivated the investigations. Laboratory investigations revealed mild anemia (hemoglobin 97–105 g/L), mild neutrophilic leukocytosis (WBC 12 × 109/L), thrombocytosis, as well as iron deficiency, elevated levels of erythrocyte sedimentation rate (35 mm/h), and C-reactive protein (156 mg/L). No kidney or liver dysfunction was revealed. Biochemical markers for autoimmune diseases including systemic lupus erythematosus, scleroderma, ANCA-associated vasculitis, and rheumatoid arthritis (rheumatoid factor, ANA, ANA IF, ANCA, anti-CCP, HLA-B27) were negative, as well as tumor markers (alpha fetoprotein, CA 125, He4), and a PCR test for COVID-19. Blood and urine cultures were negative.
Diagnostic imaging test results were negative for the most-common other fever causes: sinus CT scan for sinusitis, chest and abdomen/pelvis CT for focal inflammatory and infectious processes and malignancies, and echocardiography for infective endocarditis. Therefore, we opted for the hybrid imaging modality—whole body PET/CT (head from skull-base to toe), which showed abnormal 18F-fluorodeoxyglucose (18F-FDG) uptake in the arterial walls in the lower extremities (Figure 2). Thus, the 18F-FDG PET/CT results allowed revealing arterial wall inflammation—signs of active LVV, as well as assess its extension—and isolated lower extremity involvement. Moreover, performing whole body PET/CT examination allowed ruling out other inflammatory processes, including infectious ones, as well as malignancy.
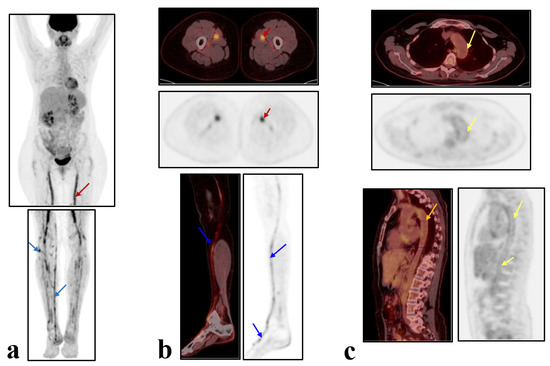
Figure 2.
Whole-body 18F-FDG PET/CT: (a) Virtual 3-D PET image, (b,c) axial (upper) and sagittal (lower) projections of fused PET/CT and PET images. (a,b) Abnormal 18F-FDG uptake in the walls of the femoral arteries—throughout (red arrows) and lower leg arteries and right foot—focal (blue arrows); (a,c) 18F-FDG uptake in the walls of other large arteries including thoracic and abdominal aorta was normal (yellow arrows).
The diagnosis of LVV was established based on symptoms, elevated CRP, and typical PET/CT findings; the patient refused to undergo biopsy.
Treatment with oral methylprednisolone 24 mg per day was initiated with complete resolution of the symptoms within 1 week. After 4 weeks of the 24 mg treatment, the dose was reduced by 4 mg every week until 12 mg with measuring CRP every week. At the dose of 12 mg, the patient experienced an episode of ankle and arm joint pain with a slight increase in CRP up to 6 mg/L. The dose was increased to 16 mg for 2 weeks and reduced afterwards every two weeks by 2 mg up to a total dose of 8 mg. After the next 8 weeks of decreasing the dose by 1 mg per week, methylprednisolone was discontinued without relapses. Follow-up during 9 months after treatment was unremarkable, and CRP remained low. The patient refused to undergo repeated PET/CT examination for the treatment effectiveness assessment. However the effectiveness of the glucocorticoid therapy additionally confirmed the diagnosis of LVV.
The uptake intensity was analyzed using a standardized uptake volume (SUV) with calculation of the SUV ratio (SUVmax in the arterial wall to SUVmean in the reference zone—liver parenchyma), which was up to 2.7.
3. Discussion
Bisphosphonates remain a first-line treatment for osteoporosis and decrease vertebral and hip fractures. The most-widely used drug is zoledronate, which is well tolerated by most patients, but may rarely cause acute inflammatory reactions. The most-common side effects are post-dose fever, flu-like symptoms, myalgia, arthralgia, and headache, which usually occur in the first 3 days after infusion and are self-limited [5]. Rare adverse events of long-term zoledronate therapy include osteonecrosis of the jaw, atypical femoral fracture, renal dysfunction, hypocalcemia, symptomatic atrial fibrillation, uveitis, and episcleritis [4].
All the above-mentioned inflammatory side effects are also symptoms and signs of LVV, which was suspected and confirmed by the 18F-FDG PET/CT results in the presented case of a female patient aged over 50 years old after receiving her first zoledronate infusion for osteoporosis.
A search using the keywords “giant cell arteritis”, “vasculitis”, “zoledronic acid”, “zoledronate”, and “bisphosphonates” in PubMed, Medline, and the Cochrane database, SIDER 4.1, yielded only two results reporting giant cell arteritis (GCA) occurring after zoledronate infusion for osteoporosis, both with orbital manifestation and temporal artery involvement [2,3]. Therefore, our case is the first in Russia presenting LVV after zoledronate infusion and the first case of isolated lower extremity involvement.
The pathogenesis of LVV after zoledronate therapy remains unknown. Several reports suggested that zoledronate is taken up by monocytes and dendritic cells, which inhibits farnesyl pyrophosphate synthase activity, resulting in the intracellular accumulation of metabolites. These metabolites are gamma-delta T cell receptor agonists, which activate the gamma-delta T cells and release cytokines such as interleukin-6 (IL-6), tumor necrosis factor alpha (TNF- alpha), and interferon-gamma (IFN-gamma), which modulate the synthesis of acute-phase proteins by hepatocytes [6]. As is known, the pro-inflammatory cytokines TNF-alpha and IL-6 were identified as the most-important mediators of acute-phase response [7]. Furthermore, IL-6 is known to play a key role in the pathogenesis of LVV to promote arterial wall inflammation [8]. Therefore, it is reasonable to suggest that gamma-delta T cells contribute to the immune response in vasculitis [9].
The diagnosis of GCA is commonly based on a scoring system developed by the American College of Rheumatology (ACR) in 1990 and revised in 2016 [10]. Temporal artery biopsy has been considered the gold standard for a long time, but negative biopsy results can be seen in up to half of cases due to non-involvement of the temporal artery or skip lesions [7]. According to the revised ACR criteria, the diagnosis of GCA can be established with a score of 3 or more out of 11 points, based on clinical and biochemical features [7]. Therefore, it allows changing clinical management and avoiding biopsy in a number of cases. Moreover, advances in technology allow non-invasive imaging modalities, such as ultrasound, CT, MRI, and PET/CT, which aid in the diagnosis with higher sensitivities than biopsy alone [7,11,12]. Each technique has its own advantages and disadvantages; however, ultrasound, CT, and MRI are structural imaging modalities and reveal only morphological disorders.
PET/CT is a hybrid—functional and structural—imaging technique that has proven its role in the detection of inflammatory processes due to its ability to detect the accumulation of radiopharmaceutical 18F-FDG in phagocytic cells due to their high glycolytic activity. A potential advantage of PET/CT is in its early detection of inflammatory processes, before morphologic damages ensue [13]. Thus, PET/CT results allow the detection of inflammatory processes even in a structurally unchanged vascular wall, i.e., in the early stages of LVV. This allows reducing the time to final diagnosis, initiating the treatment in a timely manner, and reducing the risk of complications [9,14,15]. According to multiple research results, 18F-FDG PET/CT is a non-invasive technique with a good accuracy for the early diagnosis of LVV: in the latest meta-analysis (n = 400), the pooled sensitivity and specificity were 75.9% (95% CI 68.7–82.1) and 93.0% (95% CI 88.9–96.0), respectively; with data limited to GCA—of 83.3% (95% CI 72.1–91.4) and 89.6% (95% CI 79.7–95.7), respectively [9].
In the present clinical case, the patient underwent a clinical laboratory and diagnostic examination (inclusive of the sinus, chest, and abdominal/pelvic CT scans, echocardiography), which allowed ruling out the most-common causes of fever and, therefore, suspecting LVV. According to the revised ACR criteria, the patient scored four. Therefore, given its high diagnostic performance for LVV, we decided to perform 18F-FDG PET/CT, and an inflammatory process in the arterial walls was revealed.
Another feature of this case is the isolated involvement of the lower extremity large and medium arteries, which, as a rule, is a challenge for clinicians. The standard “whole body” PET/CT protocol includes skull-base to proximal thigh scan. In the presented case, based on preliminary results after the main scan, the standard protocol was extended with an additional scan of the lower extremities up to the toes. Therefore, the PET/CT results allowed diagnosing LVV and, moreover, accurately assessing its extent, revealing isolated lesions of the lower extremity arteries, which is consistent with the results of other studies [9,11,12].
It should be also noted that PET/CT results allow assessing the activity of the inflammatory process, which is possible using both visual and semi-quantitative analysis with SUV ratio calculation. This is crucial for the monitoring of the treatment’s effectiveness [12,16].
Although our patient refused to undergo biopsy and repeated PET/CT, her symptoms, elevated acute-phase markers, and PET/CT findings were typical for LVV. In the other two reported cases, the diagnosis of GCA was established without histopathologic proof as well: in one, the biopsy was negative [2]; in another, the patient refused to undergo the procedure, and the diagnosis was based on the ultrasound results [3].
Both previously reported cases of GCA had ophthalmic manifestation [2,3]. In the literature, there are also single reports of orbital vasculitis secondary to zoledronate without defining GCA, but these cases might be consistent with this diagnosis as well [17,18].
In 2020, Mahmood et al. using Medicare data reviewed the incidence of GCA after bisphosphonate administration (zoledronate or ibandronate) in a retrospective study in elderly patients from nationwide data [19]. The incidence of GCA was 0.010% and 0.013% after zoledronate and ibandronate injection, respectively, and there was no association between bisphosphonates and the subsequent development of GCA revealed. However, further cases should be considered.
Another question is the reason for the patient’s osteoporosis. We supposed it was primary hypogonadism due to a hysterectomy 16 years ago. Premenopausal hysterectomy may impair ovarian blood supply and function [20] and is associated with a decreased ovarian reserve, follicular atresia, and subsequently, reduced long-term estrogen secretion unrelated to baseline ovarian reserve [21]. Some papers demonstrated that osteoporosis or bone fracture was higher in hysterectomized women due to earlier menopause than in the general population [22]. Other studies do not represent osteoporotic fractures for most women undergoing hysterectomy, whether or not an oophorectomy is performed [23,24]. Perhaps we faced one of the rare skeletal diseases in which premature sex-steroid deficiency accelerated the decline of BMD. The search for rare skeletal diseases will continue.
In conclusion, we suggest that our case is an association between zoledronate infusion and the subsequent development of LVV. Clinicians should be aware of the rare development of auto-inflammatory reactions including LVV after bisphosphonate infusion and consider 18F-FDG PET/CT for the diagnosis and assessment of the inflammatory process extent in such cases.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The patient’s written informed consent was obtained for publication.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gregson, C.L.; Armstrong, D.J.; Bowden, J.; Cooper, C.; Edwards, J.; Gittoes, N.J.L.; Harvey, N.; Kanis, J.; Leyland, S.; Low, R.; et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch. Osteoporos. 2022, 17, 80. [Google Scholar] [CrossRef] [PubMed]
- Eastell, R.; Rosen, C.J.; Black, D.M.; Cheung, A.M.; Murad, M.H.; Shoback, D. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society* Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2019, 104, 1595–1622. [Google Scholar] [CrossRef] [PubMed]
- Metyas, S.; Ibrahim, M.; Solyman, J.; Yeter, K.C.; Arkfeld, D.G. Giant cell arteritis with visual loss following zoledronic acid infusion. Int. J. Rheum. Dis. 2014, 17, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Naderi, N. Rare orbital manifestations and vasculitis, giant cell arteritis or side effects of zoledronic acid infusion? Arch. Gen. Intern. Med. 2019, 3, 6–7. [Google Scholar]
- Adler, R.A. Update on Rare Adverse Events from Osteoporosis Therapy and Bisphosphonate Drug Holidays. Endocrinol. Metab. Clin. N. Am. 2021, 50, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Galluzzo, S.; Santini, D.; Vincenzi, B.; Caccamo, N.; Meraviglia, F.; Salerno, A.; Dieli, F.; Tonini, G. Immunomodulating role of bisphosphonates on human gamma delta T cells: An intriguing and promising aspect of their antitumour activity. Expert Opin. Ther. Targets 2007, 11, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Dicuonzo, G.; Vincenzi, B.; Santini, D.; Avvisati, G.; Rocci, L.; Battistoni, F.; Gavasci, M.; Borzomati, D.; Coppola, R.; Tonini, G. Fever after zoledronic acid administration is due to increase in TNF-alpha and IL-6. J. Interferon. Cytokine Res. 2003, 23, 649–654. [Google Scholar] [CrossRef]
- Tanaka, T.; Kishimoto, T. Targeting interleukin-6: All the way to treat autoimmune and inflammatory diseases. Int. J. Biol. Sci. 2012, 8, 1227–1236. [Google Scholar] [CrossRef]
- Kabelitz, D.; Fazio, J.; Adam-Klages, S.; Marget, M.; Oberg, H.H.; Wesch, D.; Lamprecht, P. Gammadelta T-cells: Basic features and potential role in vasculitis. Clin. Exp. Rheumatol. 2010, 28 (Suppl. 57), 104–109. [Google Scholar]
- Mansoor, T.; Lynch, N.P.; Rifai, H.; Hamlin, S.; Moneley, D. Utilization of the Revised American College of Rheumatology (rACR) Scoring to Avoid Unnecessary Temporal Artery Biopsies—A Case Series. Med. Sci. 2022, 10, 11. [Google Scholar] [CrossRef]
- Bardi, M.; Diamantopoulos, A.P. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice summary. Radiol. Med. 2019, 124, 965–997. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Choi, S.J.; Ji, J.D.; Song, G.G. Diagnostic accuracy of 18F-FDG PET or PET/CT for large vessel vasculitis: A meta-analysis. Z. Rheumatol. 2016, 75, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Kim, J.; Molchanova-Cook, O.P.; Dilsizian, V. The Potential of FDG PET/CT for Early Diagnosis of Cardiac Device and Prosthetic Valve Infection Before Morphologic Damages Ensue. Curr. Cardiol. Rep. 2014, 16, 459. [Google Scholar] [CrossRef] [PubMed]
- Slart, R.H.J.A. Writing Group; Reviewer Group; Members of EANM Cardiovascular; Members of EANM Infection & Inflammation; Members of Committees; SNMMI Cardiovascular; Members of Council; PET Interest Group; Members of ASNC & EANM Committee Coordinator. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: Joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1250–1269. [Google Scholar] [PubMed]
- Aslanidi, I.P.; Manukova, V.A.; Mukhortova, O.V.; Katunina, T.A.; Rudas, M.S.; Pozharov, I.V.; Novikov, P.I.; Meshkov, A.D. 18F-fluorodeoxyglucose positron emission tomography in monitoring of therapy effectiveness in large vessel vasculitides. Byulleten’ Nauchnogo Tsentra Serdechno-Sosud. Khirurgii Im. A.N. Bakuleva RAMN 2017, 18, 380–390. [Google Scholar] [CrossRef]
- van der Geest, K.S.M.; Treglia, G.; Glaudemans, A.W.J.M.; Brouwer, E.; Sandovici, M.; Jamar, F.; Gheysens, O.; Slart, R.H.J.A. Diagnostic value of [18F]FDG-PET/CT for treatment monitoring in large vessel vasculitis: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3886–3902. [Google Scholar] [CrossRef]
- Lefebvre, D.R.; Mandeville, J.T.; Yonekawa, Y.; Arroyo, J.G.; Torun, N.; Freitag, S.K. A case series and review of bisphosphonate-associated orbital inflammation. Ocul. Immunol. Inflamm. 2016, 24, 134–139. [Google Scholar] [CrossRef]
- Swarnkar, B.; Biswal, S.; Agarwal, S.; Gupta, S. Zoledronate induced urticarial vasculitis. Dermatol. Ther. 2021, 34, 15164. [Google Scholar] [CrossRef]
- Mahmood, S.D.; Ji, Y.; Peng, Y.; Abou Zahr, Z. Incidence of giant cell arteritis after bisphosphonate exposure: A retrospective cohort study. Int. J. Rheum. Dis. 2021, 24, 63–68. [Google Scholar] [CrossRef]
- Xiangying, H.; Lili, H.; Yifu, S. The effect of hysterectomy on ovarian blood supply and endocrine function. Climacteric 2006, 9, 283–289. [Google Scholar] [CrossRef]
- Trabuco, E.C.; Moorman, P.G.; Algeciras-Schimnich, A.; Weaver, A.L.; Cliby, W.A. Association of Ovary-Sparing Hysterectomy with Ovarian Reserve. Obstet. Gynecol. 2016, 127, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Durães Simões, R.; Chada Baracat, E.; Szjenfeld, V.L.; de Lima, G.R.; José Gonçalves, W.; de Carvalho Ramos Bortoletto, C. Effects of simple hysterectomy on bone loss. Sao Paulo Med. J. 1995, 113, 1012–1015. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Larcos, G. Hysterectomy with ovarian conservation: Effect on bone mineral density. Aust. N. Z. J. Obstet. Gynaecol. 1998, 38, 452–454. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J., 3rd; Achenbach, S.J.; Gebhart, J.B.; Babalola, E.O.; Atkinson, E.J.; Bharucha, A.E. Influence of hysterectomy on long-term fracture risk. Fertil. Steril. 2007, 88, 156–162. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).