

Exploring Infant Physical Activity Using a Population-Based Network Analysis Approach
 , , ,
, , , 

Abstract
:1. Introduction
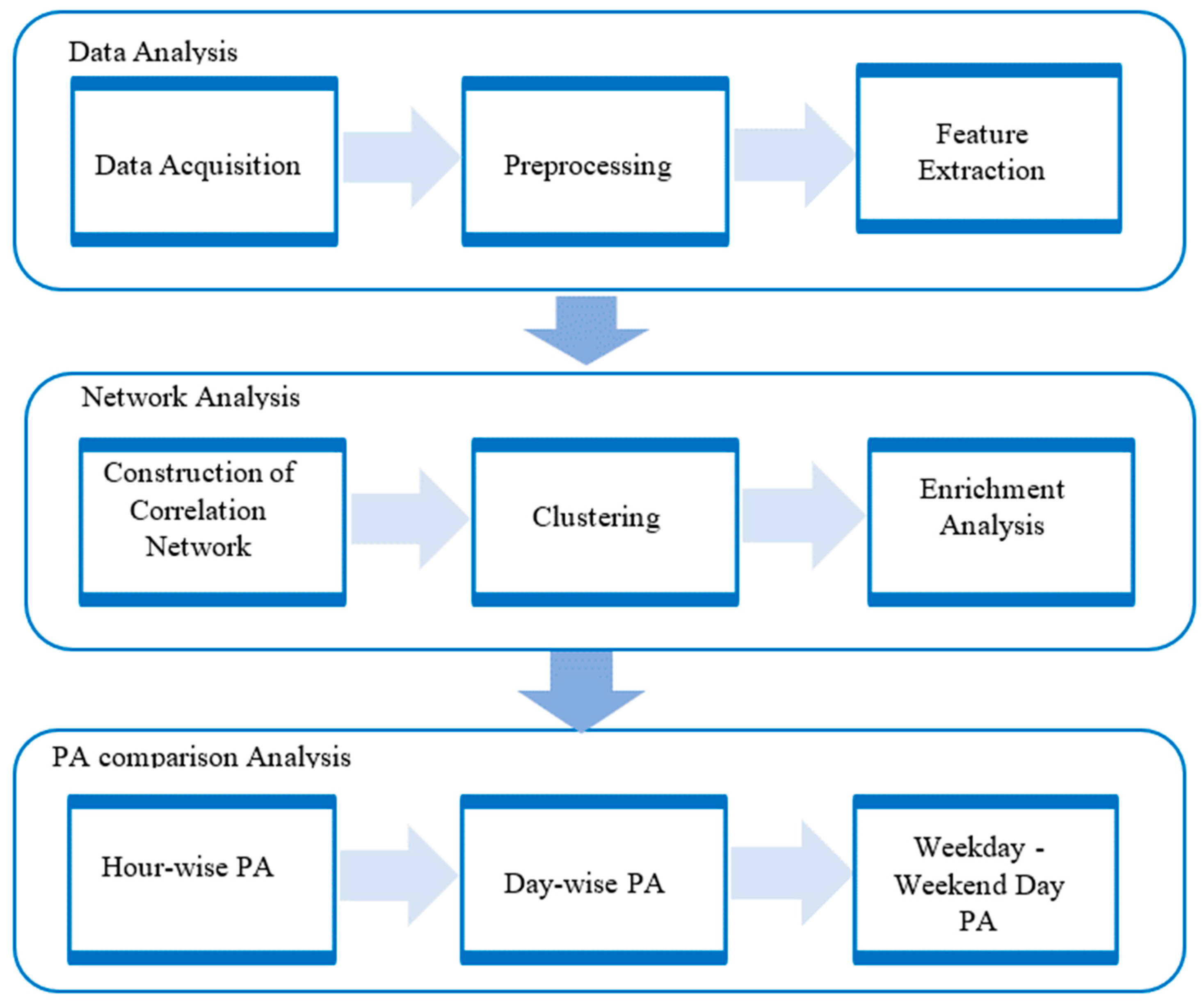
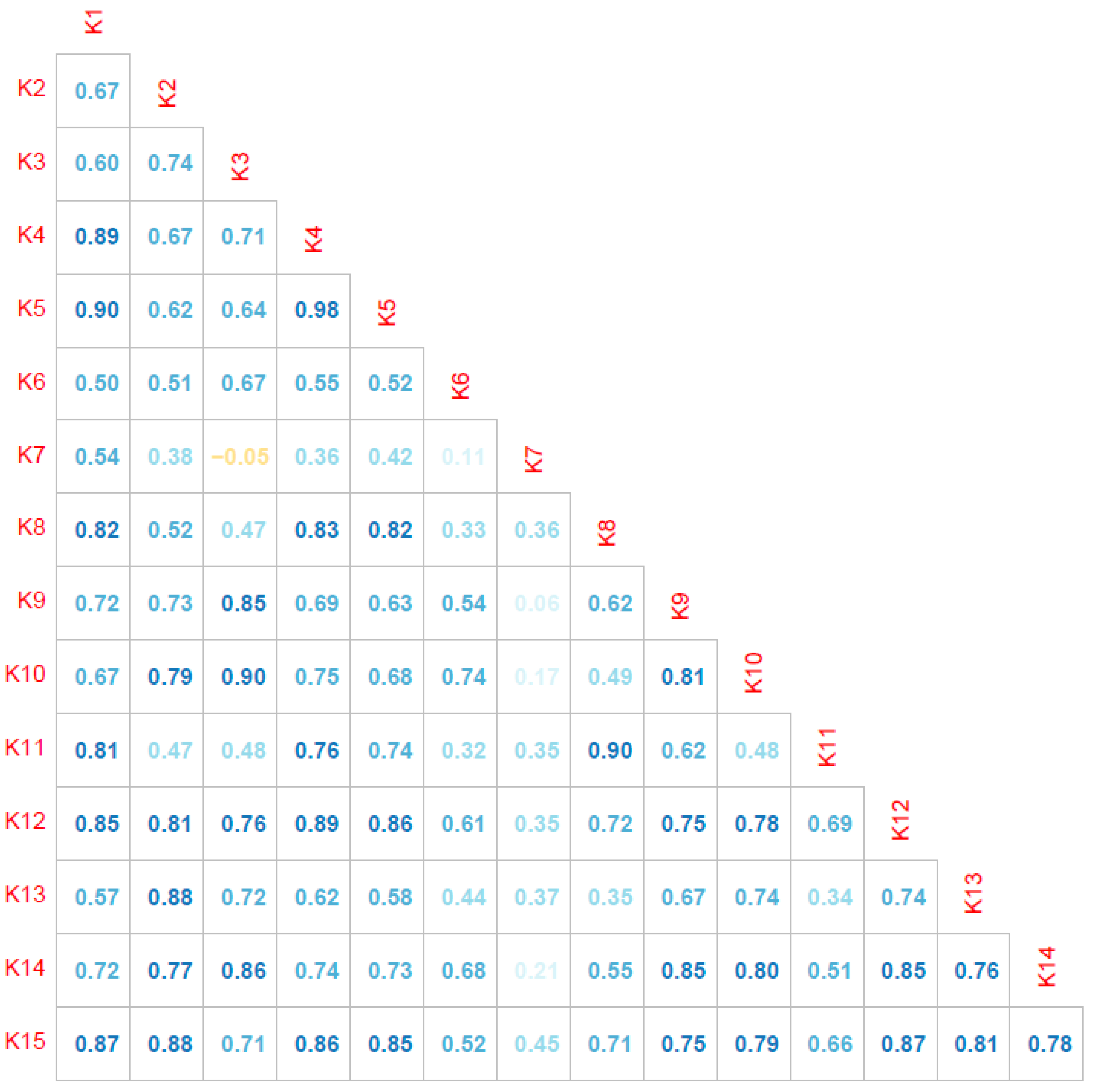
- The creation of a correlation network graph that effectively detects subgroups that are similar with respect to their PA patterns.
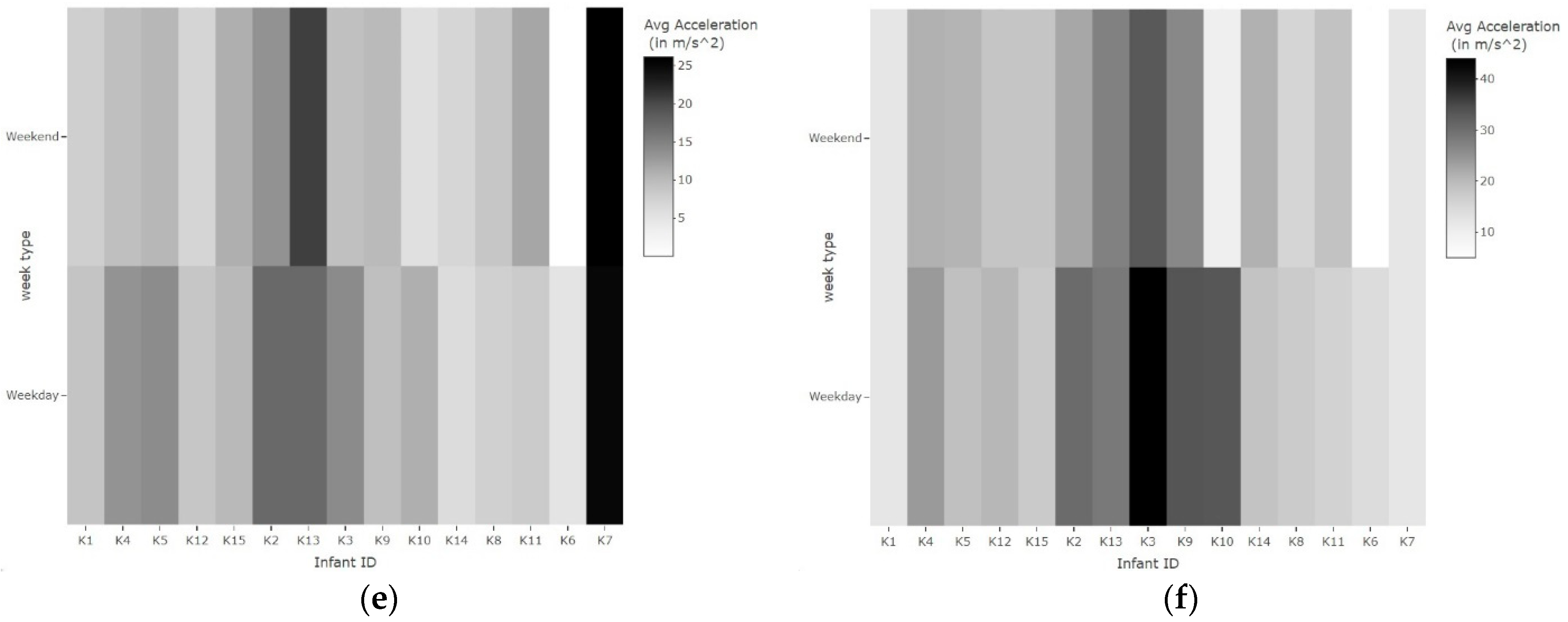
- An analysis of the PA patterns of each infant, both individually and in comparison to other infants in the group, by incorporating different time intervals, including hour, day, and weekday–weekend.
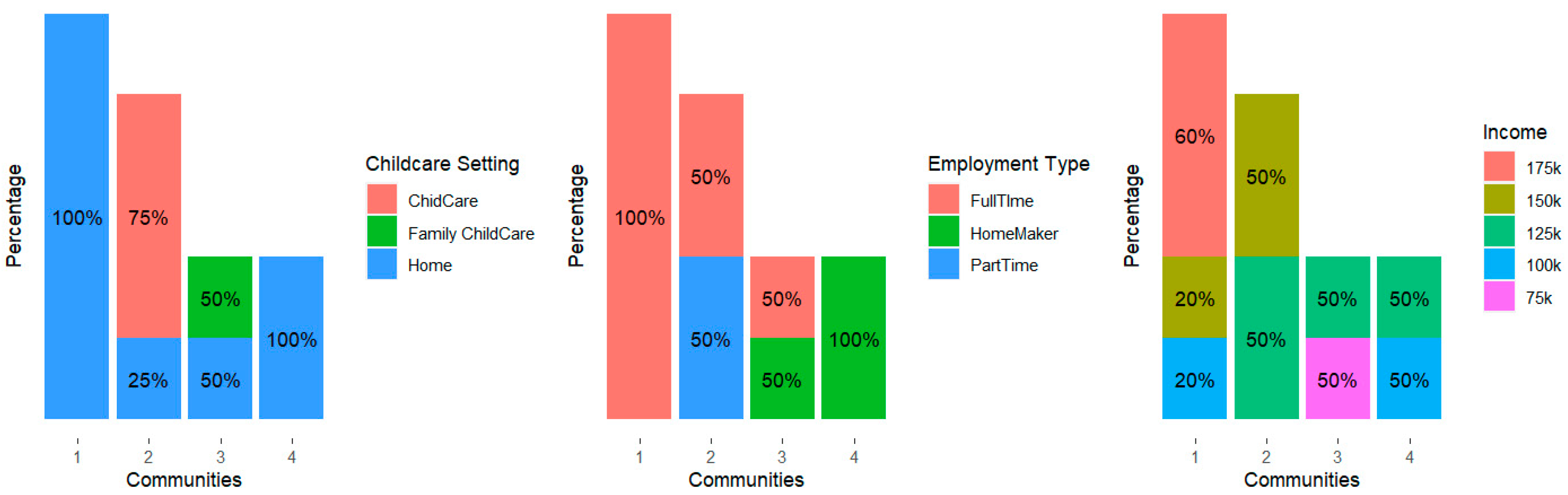
- The completion of an enrichment analysis to understand the social and family dynamics of the identified subgroups, such as demographic parameters.
2. Methods
2.1. Data Acquisition and Preprocessing
2.2. Feature Extraction
2.3. Network Analysis
2.4. PA Analysis
3. Results
3.1. Physical Activity Analysis
3.2. Enrichment Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dutta, A.; Ma, O.; Toledo, M.; Pregonero, A.F.; Ainsworth, B.E.; Buman, M.P.; Bliss, D.W. Identifying free-living physical activities using lab-based models with wearable accelerometers. Sensors 2018, 18, 3893. [Google Scholar] [CrossRef] [PubMed]
- Fruchterman, T.M.; Reingold, E.M. Graph drawing by force-directed placement. Softw. Pract. Exp. 1991, 21, 1129–1164. [Google Scholar] [CrossRef]
- Thelagathoti, R.K.; Ali, H.H. Quantitative Approaches for Detecting Early Childhood Developmental Disorders using Wireless Sensors and Mobility Data. Int. J. Adv. Life Sci. 2022, 14, 2022. [Google Scholar]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2006, 95, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Hauck, J.L.; Zott, G.R.; Felzer-Kim, I.T.; Adkins, C.M. A comparison of low-intensity physical activity, growth, and sleep behavior in 6-month old infants. Infant Behav. Dev. 2018, 53, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Bredin, S.S. Reflections on physical activity and health: What should we recommend? Can. J. Cardiol. 2016, 32, 495–504. [Google Scholar] [CrossRef]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef]
- Ketcheson, L.; Pitchford, E.A.; Kwon, H.J.; Ulrich, D.A. Physical activity patterns in infants with and without down syndrome. Pediatr. Phys. Ther. 2017, 29, 200–206. [Google Scholar] [CrossRef]
- Hauck, J.L.; Felzer-Kim, I.T.; Gwizdala, K.L. Early movement matters: Interplay of physical activity and motor skill development in infants with Down syndrome. Adapt. Phys. Act. Q. 2020, 37, 160–176. [Google Scholar] [CrossRef]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J.Y. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef]
- De Vries, S.; Van Hirtum, H.; Bakker, I.; Hopman-Rock, M.; Hirasing, R.; Van Mechelen, W. Validity and reproducibility of motion sensors in youth: A systematic update. Med. Sci. Sports Exerc. 2009, 41, 818. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Mciver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, S531. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; Reilly, J.J.; Okely, A.D. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0–5 years. J. Sci. Med. Sport 2009, 12, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.S.; Evenson, K.R.; Vaughn, A.; Rodgers, A.B.; Troiano, R.P. Accelerometer use in physical activity: Best practices and research recommendations. Med. Sci. Sports Exerc. 2005, 37 (Suppl. S11), S582–S588. [Google Scholar] [CrossRef] [PubMed]
- Radu, L.E.; Făgăraş, S.P.; Vanvu, G. Physical activity index of female university students. Procedia-Soc. Behav. Sci. 2015, 191, 1763–1766. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Gubbels, J.; De Bourdeaudhuij, I.; Cardon, G. Feasibility and validity of accelerometer measurements to assess physical activity in toddlers. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 67. [Google Scholar] [CrossRef]
- Costa, S.; Barber, S.E.; Cameron, N.; Clemes, S.A. The objective measurement of physical activity and sedentary behaviour in 2–3 year olds and their parents: A cross-sectional feasibility study in the bi-ethnic Born in Bradford cohort. BMC Public Health 2015, 15, 1109. [Google Scholar] [CrossRef]
- Johansson, E.; Hagströmer, M.; Svensson, V.; Ek, A.; Forssén, M.; Nero, H.; Marcus, C. Objectively measured physical activity in two-year-old children–levels, patterns and correlates. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 3. [Google Scholar] [CrossRef]
- Thelagathoti, R.; Ali, H. A population analysis approach using mobility data and correlation networks for depression episodes detection. Ann Depress. Anxiety 2022, 9, 1112. [Google Scholar]
- Rastegari, E.; Azizian, S.; Ali, H. Machine learning and similarity network approaches to support automatic classification of parkinson’s diseases using accelerometer-based gait analysis. In Proceedings of the Hawaii International Conference on System Sciences 2019, Maui, HI, USA, 8–11 January 2019. [Google Scholar]
- Thelagathoti, R.K.; Ali, H.H. A Data-Driven Approach for the Analysis of Behavioral Disorders with a Focus on Classification and Severity Estimation. In Proceedings of the 2022 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Las Vegas, NV, USA, 6–8 December 2022; pp. 821–825. [Google Scholar]
- Gosak, M.; Markovič, R.; Dolenšek, J.; Rupnik, M.S.; Marhl, M.; Stožer, A.; Perc, M. Network science of biological systems at different scales: A review. Phys. Life Rev. 2018, 24, 118–135. [Google Scholar] [CrossRef]
- Benesty, J.; Chen, J.; Huang, Y. On the importance of the Pearson correlation coefficient in noise reduction. IEEE Trans. Audio Speech Lang. Process. 2008, 16, 757–765. [Google Scholar] [CrossRef]
- Qualtrics. Qualtrics Research Suite [Software]. 2022. Available online: http://www.qualtrics.com (accessed on 14 November 2022).
- GT9X link: ActiGraph Wearable Devices [Internet]. Available online: https://theactigraph.com/actigraph-link (accessed on 7 July 2023).
- De Meo, P.; Ferrara, E.; Fiumara, G.; Provetti, A. Generalized louvain method for community detection in large networks. In Proceedings of the 2011 11th International Conference on Intelligent Systems Design and Applications, Cordoba, Spain, 22–24 November 2011; pp. 88–93. [Google Scholar]
- Girvan, M.; Newman, M.E. Community structure in social and biological networks. Proc. Natl. Acad. Sci. USA 2002, 99, 7821–7826. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [PubMed]
- Berahmand, K.; Bouyer, A.; Samadi, N. A new local and multidimensional ranking measure to detect spreaders in social networks. Computing 2019, 101, 1711–1733. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | |
|---|---|---|
| Age | 6–15 months | |
| Gender | ||
| Male | 10 | |
| Female | 10 | |
| Race/Ethnicity | ||
| White | 17 | |
| Asian | 3 | |
| Mothers Employment | ||
| Full time | 11 | |
| Housemaker | 8 | |
| Part time | 1 | |
| Annual household income | ||
| USD 25,000–75,000 | 3 | |
| USD 75,000–125,000 | 7 | |
| USD 125,000–175,000 | 10 | |
| Childcare status | ||
| At home with mother | 15 | |
| Childcare center/home | 5 | |
| Infant anthropometrics | Mean | SD |
| Infant weight | 9.2 | 1.8 |
| Head circumference | 17.8 | 0.61 |
| Waist circumference | 17.53 | 0.95 |
| Feature Set | Features | Count | Description |
|---|---|---|---|
| Hour-wise features | m_w_7– m_w_18 | 12 | Mean (average) of PA measured from the waist sensor across 4 days for each hour |
| sd_w_7–sd_w_18 | 12 | Standard deviation (SD) of PA measured from the waist sensor across 4 days for each hour | |
| m_a_7– m_a_18 | 12 | Mean (average) of PA measured from the ankle sensor across 4 days for each hour | |
| sd_a_7– sd_a_18 | 12 | Standard deviation (SD) of PA measured from the ankle sensor across 4 days for each hour | |
| Total | 48 | ||
| Day-wise PA features | dm_w_1– dm_w_4 | 4 | Mean (average) of PA measured from the waist sensor across 7 a.m. to 18:59 p.m. for each of the 4 days |
| dsd_w_1–dsd_w_4 | 4 | Standard deviation (SD) of PA measured from the waist sensor across 7 a.m. to 18:59 p.m. for each of the 4 days | |
| dm_a_1– dm_a_4 | 4 | Mean (average) of PA measured from the ankle sensor across 7 a.m. to 18:59 p.m. for each of the 4 days | |
| dsd_a_1– dsd_a_4 | 4 | Standard deviation (SD) of PA measured from the ankle sensor across 7 a.m. to 18:59 p.m. for each of the 4 days | |
| Total | 16 | ||
| Weekday–weekend day PA features | wm_w_1– wm_w_4 | 4 | Mean (average) of PA measured from the waist sensor for 2 weekdays and 2 weekends |
| wsd_w_1–wsd_w_4 | 4 | Standard deviation (SD) of PA measured from the waist sensor for 2 weekdays and 2 weekends | |
| wm_a_1– wm_a_4 | 4 | Mean (average) of PA measured from the ankle sensor for 2 weekdays and 2 weekends | |
| wsd_a_1–wsd_a_4 | 4 | Standard deviation (SD) of PA measured from the ankle sensor for 2 weekdays and 2 weekends | |
| Total | 16 |
| Subject ID | P1 | P2 | P3 | P4 |
|---|---|---|---|---|
| P1 | 0 | 0.4 | 0.75 | 0.7 |
| P2 | 0.4 | 0 | 0.5 | 0.55 |
| P3 | 0.75 | 0.5 | 0 | 0.9 |
| P4 | 0.7 | 0.55 | 0.9 | 0 |
| ID | Childcare Setting | Parent Demographics | Infant Anthropometrics | Community ID | ||||
|---|---|---|---|---|---|---|---|---|
| Childcare/Home | Duration (Hours) | Employment | Income (USD) | Weight | Head Circumference | Waist Circumference | ||
| K1 | Home | NA | Full-time | 100 k | 8.67 | 17.51 | 18.24 | 1 |
| K4 | Home | NA | Full-time | 175 k | 9.29 | 17.9 | 17.58 | 1 |
| K5 | Home | NA | Full-time | 175 k | 9.11 | 17.66 | 18.61 | 1 |
| K12 | Home | NA | Full-time | 150 k | 11.19 | 19.18 | 19.18 | 1 |
| K15 | Home | NA | Full-time | 175 k | 15.12 | 18.5 | 16.66 | 1 |
| K3 | Childcare center | >40 | Full-time | 150 k | 8.59 | 18.03 | 16.89 | 2 |
| K9 | Home | NA | Part-time | 150 k | 8.25 | 17.13 | 16.06 | 2 |
| K10 | Childcare center | 31–40 | Full-time | 125 k | 7.74 | 16.98 | 17.34 | 2 |
| K14 | Childcare center | 10–20 | Part-time | 125 k | 8.61 | 18.03 | 16.08 | 2 |
| K2 | Family childcare home | 31–40 | Full-time | 125 k | 8.05 | 17.45 | 18.86 | 3 |
| K13 | Home | NA | Housemaker | 75 k | 9.43 | 18.63 | 17.68 | 3 |
| K8 | Home | NA | Housemaker | 100 k | 9.23 | 17.29 | 17.68 | 4 |
| K11 | Home | NA | Housemaker | 125 k | 8.15 | 17.33 | 17.78 | 4 |
| K6 | Childcare center | >40 | Full-time | 125 k | 8.27 | 18.17 | 16.63 | NA |
| K7 | Home | NA | Housemaker | 50 k | 8.74 | 18.08 | 17.68 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thelagathoti, R.K.; Chaudhary, P.; Knarr, B.; Schenkelberg, M.; Ali, H.H.; Dinkel, D. Exploring Infant Physical Activity Using a Population-Based Network Analysis Approach. Analytics 2024, 3, 14-29. https://doi.org/10.3390/analytics3010002
Thelagathoti RK, Chaudhary P, Knarr B, Schenkelberg M, Ali HH, Dinkel D. Exploring Infant Physical Activity Using a Population-Based Network Analysis Approach. Analytics. 2024; 3(1):14-29. https://doi.org/10.3390/analytics3010002
Chicago/Turabian StyleThelagathoti, Rama Krishna, Priyanka Chaudhary, Brian Knarr, Michaela Schenkelberg, Hesham H. Ali, and Danae Dinkel. 2024. "Exploring Infant Physical Activity Using a Population-Based Network Analysis Approach" Analytics 3, no. 1: 14-29. https://doi.org/10.3390/analytics3010002
APA StyleThelagathoti, R. K., Chaudhary, P., Knarr, B., Schenkelberg, M., Ali, H. H., & Dinkel, D. (2024). Exploring Infant Physical Activity Using a Population-Based Network Analysis Approach. Analytics, 3(1), 14-29. https://doi.org/10.3390/analytics3010002