Surgery Scheduling and Perioperative Care: Smoothing and Visualizing Elective Surgery and Recovery Patient Flow


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Motivation
1.2. Background Literature
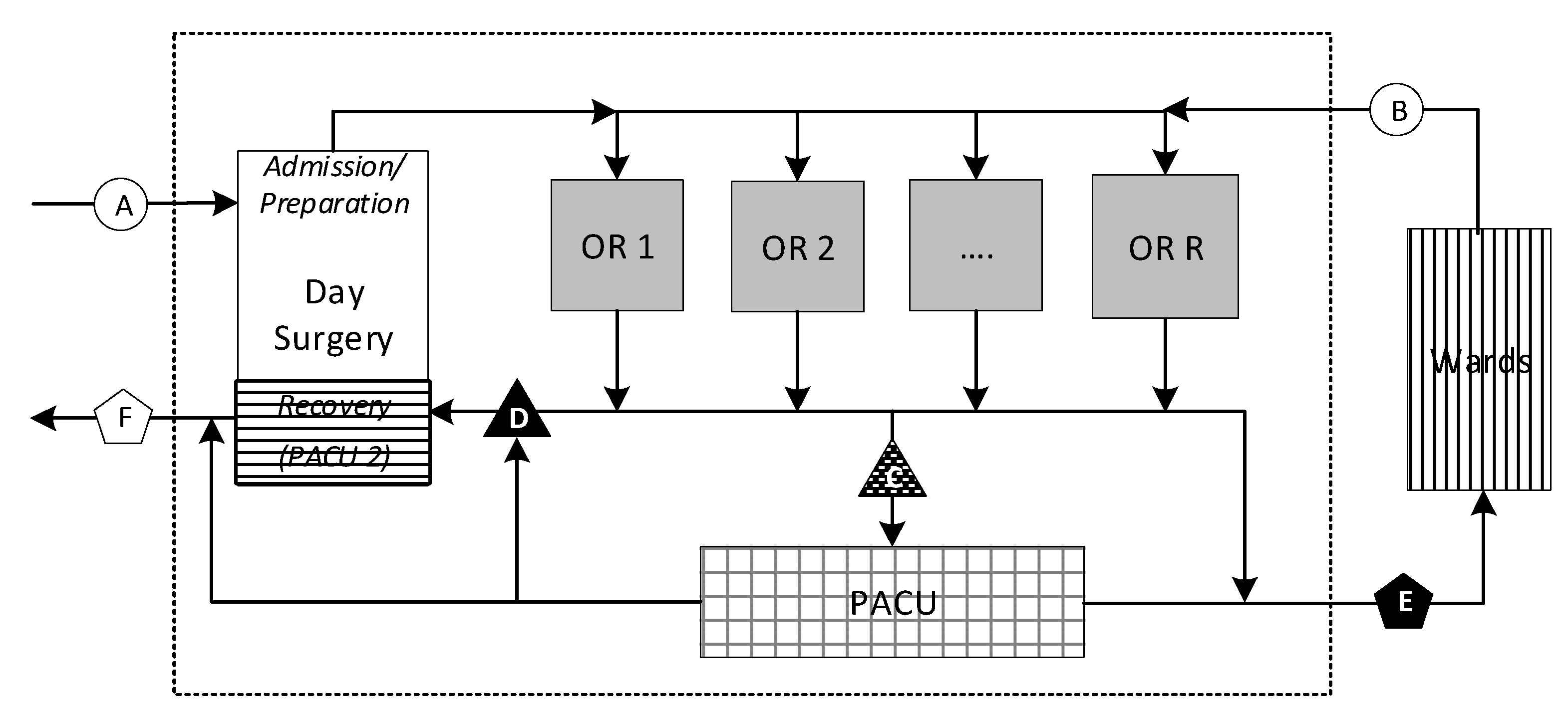
1.3. Problem Description
2. Model Development
2.1. Assumptions
2.2. Hospital Data
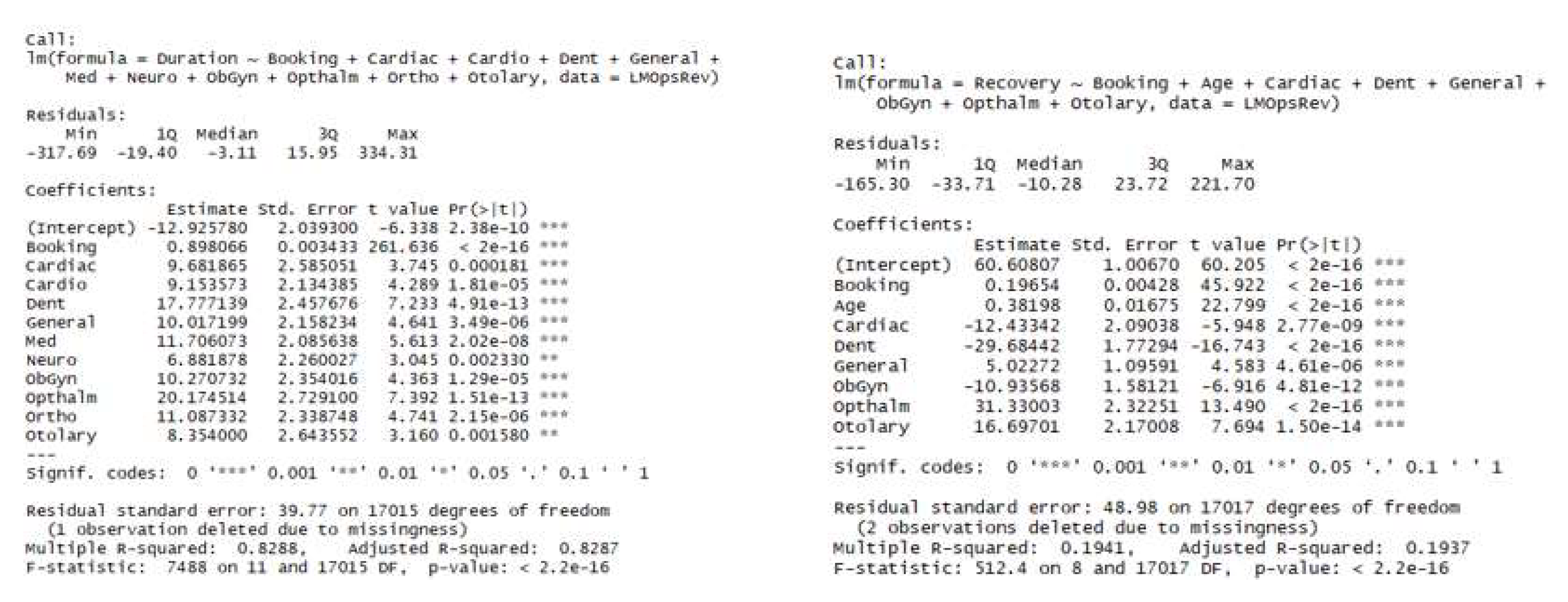
2.3. Procedure and Recovery Durations
2.4. Constraint Programming (CP) Model
2.4.1. Preliminaries
- Tuple Sets (Patients Rooms );
- Deducible Parameters and Relationships (Occupancy Durations , Assignment Matrix );
- Decision Variables;
- Interval (Occupancies , Patient PACU Occupancies , OR Occupied Times );
- Sequence (OR Loads , Patient Paths );
- Interval Parameters (OR Open Windows , Surgical Day Time );
- Setting Specific Parameters (Allowable OR Start Times , OR Cleaning Times );
- Intermediate Functions and Expressions (Patient PACU Pulse , Patient Flow Time );
- Objective Function.
2.4.2. Some Properties
- .start
- an integer value lying with a specified range ‘.in ..’ (see below)
- .end
- an integer value lying in the same specified range ‘.in ..’:
- .size
- an integer value representing the difference
- .optional
- a Boolean value (default: False) if interval not required in a solution
- .in ..
- a specified range constraining the above.
2.4.3. Tuple Sets
- a set of discrete ORs (operating rooms)
- the union of the set with the (a special room):
- For each we introduce a tuple of input data with the following
- .id
- key field
- .room
- OR # or
- .service
- name of the surgical group (e.g., Ortho)
- .open
- (.start) of first prescheduled surgical procedure
- .close
- (.start + .booking) of last prescheduled surgical procedure
- a set of patients on each of whom a surgical procedure is to be performed
- For each we introduce a tuple of inputs with the following properties:
- .patient
- key field
- .service
- name of surgical group performing the service
- .room
- OR # or ;
- .start
- prescheduled start time (e.g., 480 min = 08:00);
- .booking
- a pre-scheduled booking window (e.g., 30, 60, 120 min);
- .procTime
- the expected duration of the procedure;
- .recTime
- the expected duration of the patient’s recovery;
- .patient
- a real number lying in .
2.4.4. Deducible Parameters
- an integer representing the time a patient is expected to spend in room
- a matrix of dimensions with binary values:
2.4.5. Decision Variables
- an interval decision variable such that
- note:
- an interval decision variable representing the time a patient will occupy a bed in
- an interval decision variable representing the time during which room is expected to be open, beginning at and ending with the latest in that room
- an interval decision variable represent a patient’s total length of stay
- a sequence decision variable on every ,
- such that and
- a sequence decision variable on ,
- such that and
2.4.6. Interval Parameters
- an interval parameter representing the range
2.4.7. Setting-Specific Parameters
- a fixed range from 480..1440 (08:00 a.m.–24:00 p.m.)
- a step function which restricts possible start times of procedures
- a minimum allowable clean-up time gap between procedures
- sets of specifying minimum time between procedures in
- a maximum allowable number of patients in the PACU at any time.
2.4.8. Intermediate Functions and Expressions
- , the sum of patients in the PACU at points-in-time
- for all over minutes of the day.
- flow time for each patient, from the opening of
- for all their OR until the expected completion of their surgery completion, given the procedure start time in a proposed schedule solution.
- the earliest procedure start time in a room
- the latest procedure end time in a room.
2.4.9. Objective Function
- , the sum of patient flow times
- the sum of patient flow times weighted by their respective precedence scores.
2.5. Formulation
- (1)
- is the objective function minimizing total flow time.
- (2)
- specifies that decision intervals , which represent each patient’s total length of stay from the start of procedure to the end of recovery, must span their two occupancies in the OR and PACU.
- (3)
- specifies that the last (2nd) occupancy a patient’s path must be in the PACU, numerically the member of .
- (4)
- specifies no overlap between a patient’s occupancies in the OR and PACU.
- (5)
- complements both Equations (2) and (4) specifying further that the size of should exactly match the sum of the patient’s occupancies. A solution must have no delay between them.
- (6)
- specifies that the decision interval for each patient begins with PACU occupancy.
- (7)
- specifies that intervals in sequences cannot overlap and furthermore must be separated by at least a minimum clean time (for two patients with occupancies in a sequence .
- (8)
- specifies that room cannot start before the room’s block time opening .
- (9)
- specifies the latest any procedure can be expected to end is 20:00 p.m. (minute 1200).
- (10)
- requires that patient procedure scheduled starts are only at allowable times in .
- (11)
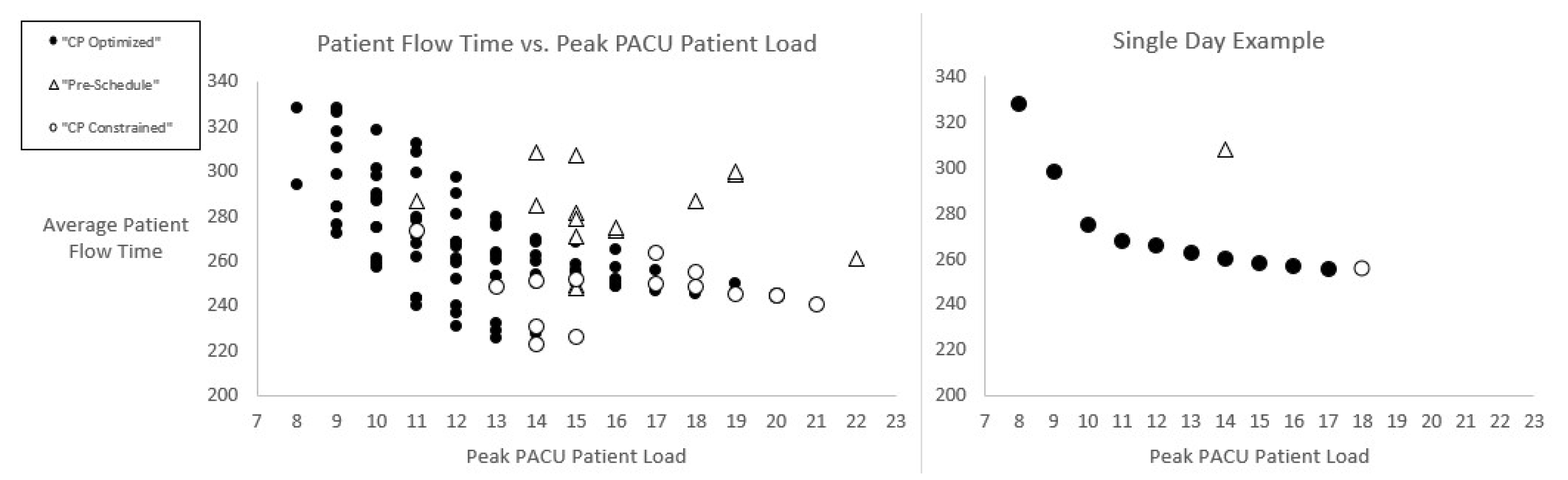
- specifies a peak number of patients in the PACU at any time cannot exceed an integer amount . This is initially set to a high number to ensure that it will not be binding and thus to discover the unbounded peak PACU expected from a solution with the best objective function value. is lowered incrementally through successive iterations of the model until its lowest possible value (with a feasible schedule solution) is achieved. We explain this more next.
2.6. Iterative Solution Approach
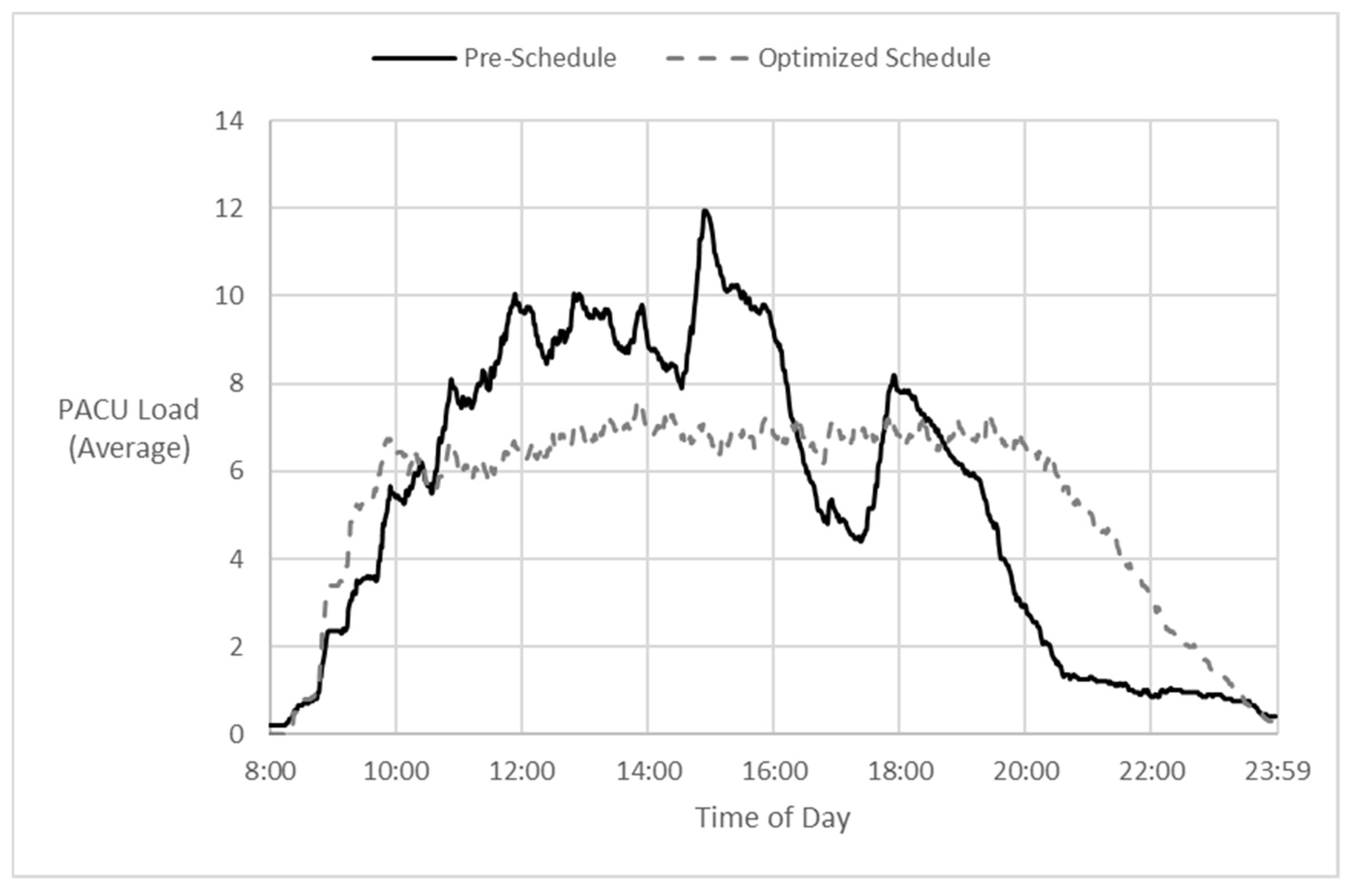
- Solve the problem with an overly generous PACU capacity limit and the objective of minimizing total patient flow time, which also translates into minimizing total OR makespans.
- Determine the resulting expected peak PACU patient load, . Call this amount , being the threshold below which capacity has a negative effect, i.e., a restriction on flow time optimization. Set before proceeding to the next step.
- Invoke a PACU capacity constraint one less than the peak determined in the previous step; that is, set and re-solve for the objective of minimizing total patient flow time, subject to: .
- If a feasible solution is not found in the most recent step (3), accept the feasible solution found in the second-most recent step as the recommended schedule and stop. (In effect, after making one too many progressively constrained solve attempts, return to the last successful one.)
- Otherwise, a feasible solution was found in step 3, so repeat steps 3 and 4 until reaching a stop.
2.7. Discussion of Model Features
3. Results
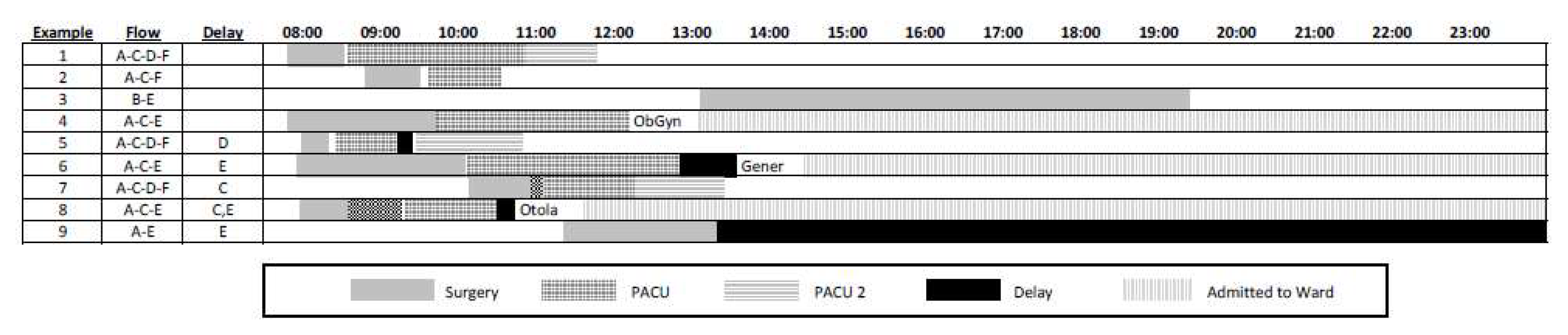
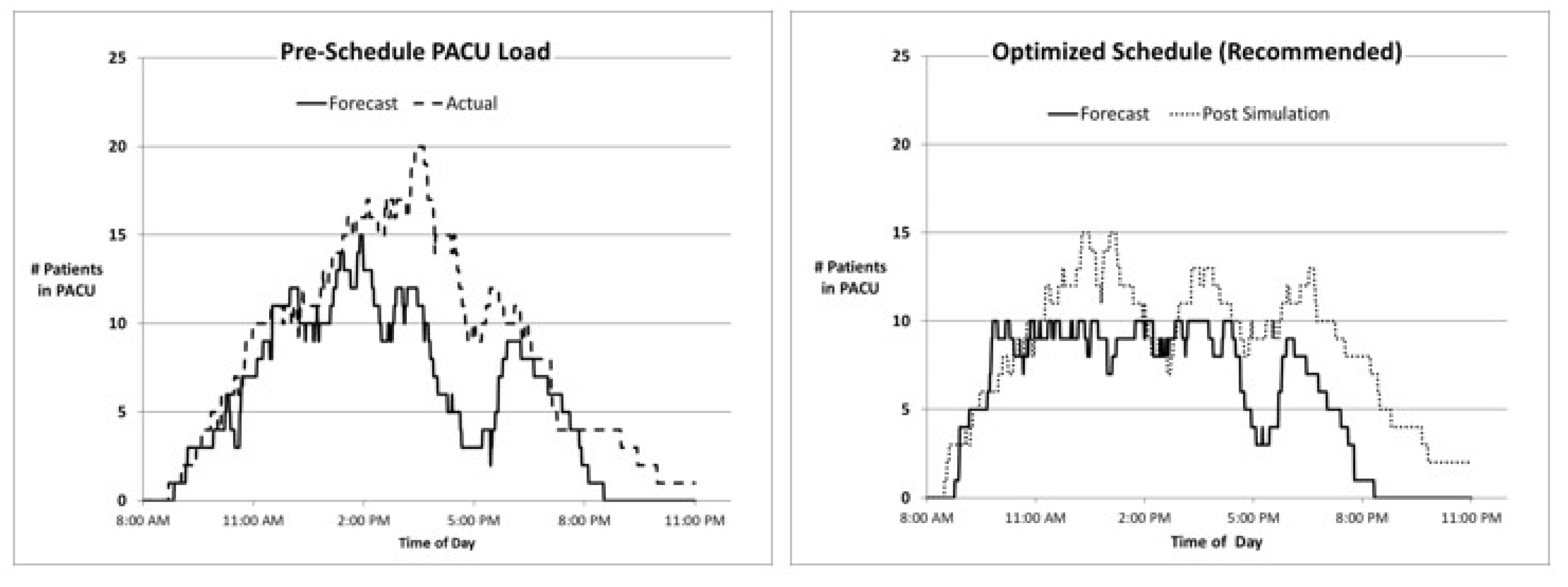
3.1. Timeline Comparision
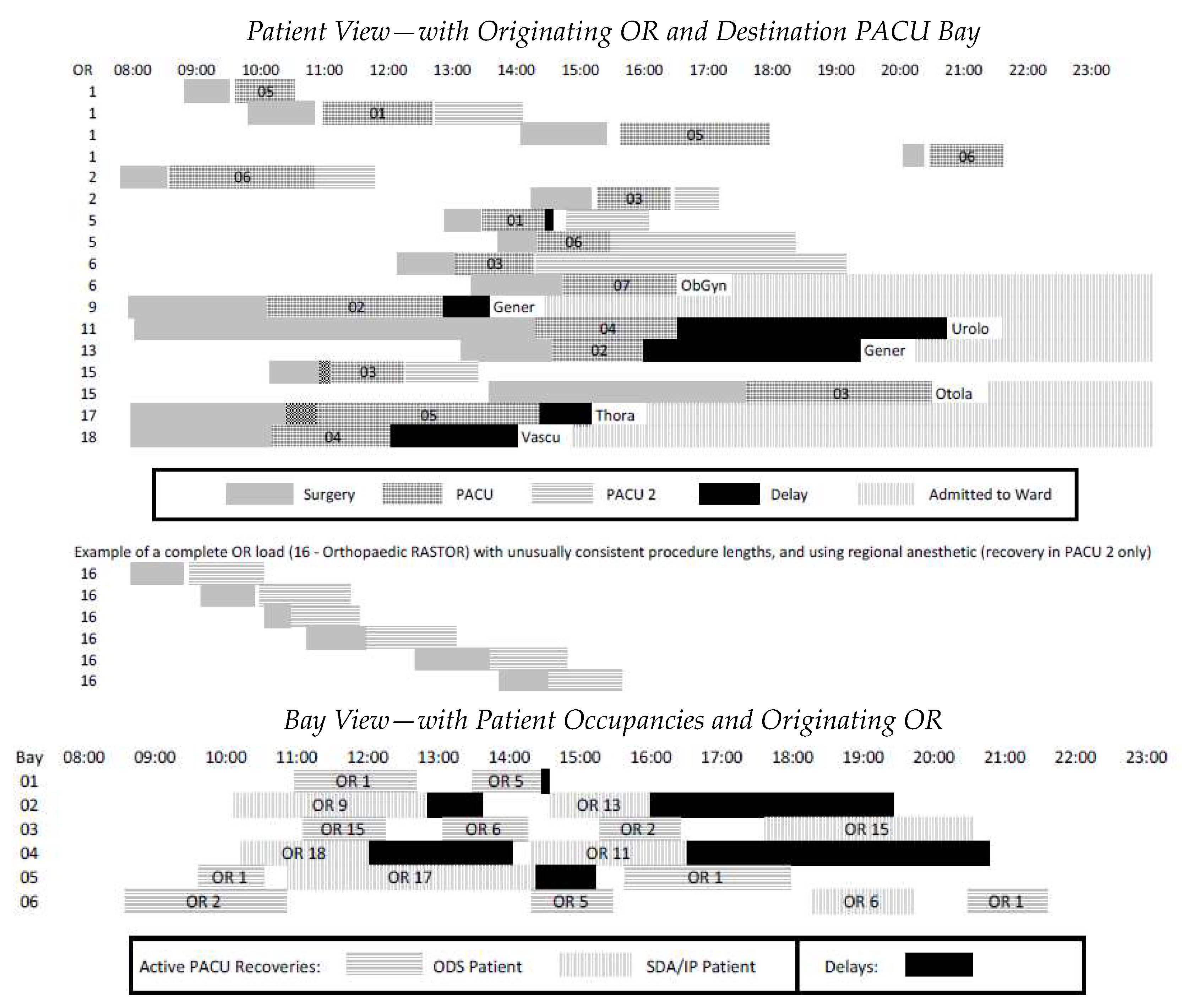
3.2. Flow and Occupancy Visualization Model
3.3. Other PACU Considerations
3.4. Discussion
3.5. Opportunities for Further Research
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ontario, H.Q. System Performance—Wait Times for Surgeries and Procedures; Health Quality Ontario: Toronto, ON, Canada, 2019.
- Available online: https://toronto.ctvnews.ca/ontario-releases-3-step-plan-to-invest-in-private-care-to-reduce-surgical-backlog-1.6232067 (accessed on 10 April 2023).
- Available online: https://globalnews.ca/news/9329715/ontario-long-waiters-pandemic-surgery/ (accessed on 10 April 2023).
- Duong, D. Provinces accept federal health funding deal. CMAJ 2023, 195, E344–E345. [Google Scholar] [CrossRef]
- Naderi, B.; Roshanaei, V.; Begen, M.A.; Aleman, D.M.; Urbach, D.R. Increased surgical capacity without additional resources: Generalized operating room planning and scheduling. Prod. Oper. Manag. 2021, 30, 2608–2635. [Google Scholar] [CrossRef]
- Santibáñez, P.; Begen, M.; Atkins, D. Surgical block scheduling in a system of hospitals: An application to resource and wait list management in a British Columbia health authority. Health Care Manag. Sci. 2007, 10, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, U.; Jaensson, M.; Dahlberg, K.; Hugelius, K. Postoperative Recovery After General and Regional Anesthesia in Patients Undergoing Day Surgery: A Mixed Methods Study. J. PeriAnesthesia Nurs. 2019, 34, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.W.; Maxwell, W.L.; Miller, L.W. Theory of Scheduling; Addison-Wesley Pub. Co.: Boston, MA, USA, 1967. [Google Scholar]
- Blake, J.T.; Carter, M.W. Surgical process scheduling: A structured review. J. Soc. Health Syst. 1997, 5, 17–30. [Google Scholar] [PubMed]
- Cardoen, B.; Demeulemeester, E.; Beliën, J. Operating room planning and scheduling: A literature review. Eur. J. Oper. Res. 2010, 201, 921–932. [Google Scholar] [CrossRef]
- Guerriero, F.; Guido, R. Operational research in the management of the operating theatre: A survey. Health Care Manag. Sci. 2011, 14, 89–114. [Google Scholar] [CrossRef]
- Gür, Ş.; Eren, T. Application of Operational Research Techniques in Operating Room Scheduling Problems: Literature Overview. J. Healthc. Eng. 2018, 5341394. [Google Scholar] [CrossRef]
- Sauré, A.; Begen, M.A.; Patrick, J. Dynamic multi-priority, multi-class patient scheduling with stochastic service times. Eur. J. Oper. Res. 2020, 280, 254–265. [Google Scholar] [CrossRef]
- Sang, P.; Begen, M.A.; Cao, J. Appointment scheduling with a quantile objective. Comput. Oper. Res. 2021, 132, 105295. [Google Scholar] [CrossRef]
- Batun, S.; Begen, M.A. Optimization in healthcare delivery modeling: Methods and applications. In Handbook of Healthcare Operations Management: Methods and Applications; Springer: New York, NY, USA, 2013; pp. 75–119. [Google Scholar]
- Begen, M.A.; Queyranne, M. Appointment scheduling with discrete random durations. Math. Oper. Res. 2011, 36, 240–257. [Google Scholar] [CrossRef]
- Gür, Ş.; Pinarbaşi, M.; Alakaş, H.M.; Eren, T. Operating room scheduling with surgical team: A new approach with constraint programming and goal programming. Cent. Eur. J. Oper. Res. 2022, 1–25. [Google Scholar] [CrossRef]
- Gür, Ş.; Eren, T.; Alakaş, H.M. Surgical operation scheduling with goal programming and constraint programming: A case study. Mathematics 2019, 7, 251. [Google Scholar] [CrossRef]
- Wang, T.; Meskens, N.; Duvivier, D. Scheduling operating theatres: Mixed integer programming vs. constraint programming. Eur. J. Oper. Res. 2015, 247, 401–413. [Google Scholar] [CrossRef]
- Abedini, A.; Li, W.; Ye, H. An Optimization Model for Operating Room Scheduling to Reduce Blocking Across the Perioperative Process. Procedia Manuf. 2017, 10, 60–70. [Google Scholar] [CrossRef]
- Bam, M.; Denton, B.T.; Van Oyen, M.P.; Cowen, M.E. Surgery scheduling with recovery resources. IISE Trans. 2017, 49, 942–955. [Google Scholar] [CrossRef]
- Fairley, M.; Scheinker, D.; Brandeau, M.L. Improving the efficiency of the operating room environment with an optimization and machine learning model. Health Care Manag. Sci. 2018, 22, 756–767. [Google Scholar] [CrossRef]
- Larsson, A. The accuracy of surgery time estimations. Prod. Plan. Control 2013, 24, 891–902. [Google Scholar] [CrossRef]
- Wright, I.H.; Kooperberg, C.; Bonar, B.A.; Bashein, G. Statistical modeling to predict elective surgery time. Comparison with a computer scheduling system and surgeon-provided estimates. Anesthesiology 1996, 85, 1235–1245. [Google Scholar] [CrossRef]
- Millstein, M.A.; Martinich, J.S. Takt Time Grouping: Implementing kanban-flow manufacturing in an unbalanced, high variation cycle-time process with moving constraints. Int. J. Prod. Res. 2014, 52, 6863–6877. [Google Scholar] [CrossRef]
- Dexter, F. Bed Management Displays to Optimize Patient Flow From the OR to the PACU. J. PeriAnesthesia Nurs. 2007, 22, 218–219. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, C.; Liu, N.; Begen, M.A. Dynamic interday and intraday scheduling. Oper. Res. 2022. [Google Scholar] [CrossRef]
- Caglar Gencosman, B.; Begen, M.A.; Ozmutlu, H.C.; Ozturk Yilmaz, I. Scheduling methods for efficient stamping operations at an automotive company. Prod. Oper. Manag. 2016, 25, 1902–1918. [Google Scholar] [CrossRef]
- Caglar Gencosman, B.; Begen, M.A. Exact optimization and decomposition approaches for shelf space allocation. Eur. J. Oper. Res. 2022, 299, 432–447. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyons, J.S.F.; Begen, M.A.; Bell, P.C. Surgery Scheduling and Perioperative Care: Smoothing and Visualizing Elective Surgery and Recovery Patient Flow. Analytics 2023, 2, 656-675. https://doi.org/10.3390/analytics2030036
Lyons JSF, Begen MA, Bell PC. Surgery Scheduling and Perioperative Care: Smoothing and Visualizing Elective Surgery and Recovery Patient Flow. Analytics. 2023; 2(3):656-675. https://doi.org/10.3390/analytics2030036
Chicago/Turabian StyleLyons, John S. F., Mehmet A. Begen, and Peter C. Bell. 2023. "Surgery Scheduling and Perioperative Care: Smoothing and Visualizing Elective Surgery and Recovery Patient Flow" Analytics 2, no. 3: 656-675. https://doi.org/10.3390/analytics2030036
APA StyleLyons, J. S. F., Begen, M. A., & Bell, P. C. (2023). Surgery Scheduling and Perioperative Care: Smoothing and Visualizing Elective Surgery and Recovery Patient Flow. Analytics, 2(3), 656-675. https://doi.org/10.3390/analytics2030036