1. Introduction
Stroke is a serious and common public health problem throughout the world, with high mortality rates [
1]. In recent years, advances in the medical treatment of acute stroke have resulted in a decrease in the mortality rate [
1,
2,
3]. However, many survivors remain with significant commitments [
4], with upper limb impairment occurring in up to 77% of cases [
5]. This is the major cause of functional dependence and the impossibility of carrying out daily life activities [
6]. Therefore, health centers, stroke survivors and their families carry the burden of long-term disability.
The increasing proportion of survivors of stroke is associated with an increase in the number of individuals who persist with sensory motor deficits [
3,
4]. Despite intensive rehabilitation, more than half of the survivors remain with a disability affecting functional independence [
7,
8,
9]. Poststroke rehabilitation has been a challenge because it usually requires repetitive and intensive training. Additionally, there is a shortage of health centers and health professionals to deal with this increasing population [
10].
Several neurorehabilitation techniques have been used for neuromuscular rehabilitation of these types of patients [
11,
12,
13,
14,
15]. Technologies such as augmented reality (AR) have been employed as new therapy tools to improve stroke rehabilitation and provide opportunities to promote the repetitive practice of activities as soon as disengagement and boredom threaten the progress in rehabilitation [
4]. AR is a technology that combines the real world with virtual objects and can be manipulated by the user and controlled by specialists. AR applications constitute a safe environment for users [
16], and they have the potential to be used at home with remote supervision [
17].
AR applied to health and wellness fields has been evaluated in recent years and with promising outcomes in some areas, such as rehabilitation [
12,
16,
18]. Moreover, functional magnetic resonance imaging (fMRI) assessment of brain changes resulting from the use of this type of system in rehabilitation has shown that most result in the restoration of activation patterns or relateralization to the ipsilateral hemisphere [
19]. fMRI is a noninvasive and safe technique for mapping functional connectivity and brain function. Resting-state fMRI (rs-fMRI) data can be acquired using spontaneous signals obtained while the participant is resting in the scanner [
20]. Data from rs-fMRI have been shown to be stable and reproducible across participants [
21]. The rs-fMRI experiments are not used to map brain activation/deactivation of the brain regions during a specific task but rather to investigate brain functional connectivity [
22].
Usually, functional connectivity is inferred from seed-based analysis or independent component analysis (ICA). Seed-based analysis is performed by correlating the fMRI time signals of chosen regions of interest (ROIs) with the remaining fMRI time series, disregarding other significant neural coactivation patterns [
22], while ICA is a data-driven method that does not depend on any chosen ROI [
23].
In this work, for AR training, we chose an AR system, NeuroR, that was initially designed to provide a virtual image to stimulate motor imagery [
24]. It uses an approach similar to mirror therapy, with a virtual tridimensional arm superimposed on the impaired limb, that is, the user’s actual upper limb is substituted in the image by the virtual arm. This AR system seeks to promote neuroplasticity by performing a simple task, where the participant, sitting in front of a projection screen or TV, visualizes him/herself performing exercises of shoulder abduction and flexion with the affected arm, which is replaced by a virtual arm. The virtual arm performs a much larger movement than the real movement the patient is actually capable of executing. Actually, the success of virtual reality and AR games applied to rehabilitation seems to be based on their ability to provide false positive feedback, which is thought to promote appropriate brain reorganization [
25,
26]. Previous experiments showed that three of four stroke patients physically executed shoulder movement when asked to perform motor imagery from the visual feedback of the animation of the tridimensional virtual arm [
24]. Another study, by Brauchle et al., with a multijoint arm exoskeleton reported changes in brain functional connectivity during motor execution and motor imagery of different feedback modalities (visual and proprioceptive) for both healthy participants and stroke survivors [
27]. They evaluated the functional connectivity networks from electroencephalography data by defining a seed electrode in the ipsilesional primary motor cortex. In the same way, we hypothesized that changes in brain functional connectivity can occur, as pointed out by [
27], since the participants also have visual and proprioceptive feedback while they see themselves on the computer screen and see their virtual arm moving during shoulder exercises for mental practice or motor execution.
The aim of the present work was to explore the use of rs-fMRI data to evaluate possible changes in functional brain connectivity of poststroke participants associated with the use of NeuroR in the context of motor rehabilitation. We also wanted to evaluate the spasticity of the patients and possible changes after therapy in their range of motion (ROM). A pilot study was conducted with an acute stroke participant using rs-fMRI and NeuroR training integrated into the patient’s rehabilitation program [
28]. Herein, we conducted a case series with three chronic poststroke participants. Functional connectivity analyses were performed to investigate whether functional brain reorganization occurred, triggered by the mental practice of stroke participants using NeuroR. Functional brain connectivity was assessed using the seed-based method. The idea was to investigate whether the integration of the virtual arm image into the AR system stimulates neuroplasticity, making the system a new tool to aid the rehabilitation of poststroke patients.
2. Materials and Methods
Case studies were performed at the Clinics Hospital of the University of Campinas, Brazil. Three male chronic stroke participants with left hemiparesis were enrolled in the study.
2.1. Participants
The inclusion criteria were individuals with a clinical diagnosis of ischemic stroke, with motor sequelae of the upper limb, whose conditions were already clinically stabilized and who had already previously participated in conventional rehabilitation therapy but were not at that moment participating in any such therapy.
The exclusion criteria were individuals diagnosed with stroke who were confused and disoriented, with aphasia of understanding or without motor deficits.
Three chronic stroke participants (mean age 65 +/− 12 years) were screened for eligibility. All participants were informed about the procedures and signed the terms of informed consent approved by the Ethics Committee of the University of Campinas (CAAE 49976315.5.0000.5404), and all study procedures were conducted in accordance with the principles expressed in the Declaration of Helsinki. This study followed the CARE guidelines for case reports. Due to time and funding limitations, it was not possible to recruit more patients for this study.
Participant 1 (P1) is a 49-year-old male who sustained a right-sided ischemic stroke in the middle cerebral right artery four years prior to enrollment in the study, resulting in left hemiparesis. He used a wheelchair propelled by a caregiver. He received botulinum toxin injection to treat spasticity after stroke six months prior to admission in this study. He had earlier exposure to intensive and frequent therapy. The clinical evaluation revealed spastic hemiparesis in the left upper limb, with changes in muscle tone, which impaired the control of the limb in space and movement and facial synkinesis during the exercise without assistance.
Participant 2 (P2) is an 84-year-old male who sustained a right-sided ischemic stroke in the middle cerebral right artery two years prior to participating in the study, resulting in left hemiparesis. He primarily used a wheelchair propelled by a caregiver. He had received prior therapy focusing on functional electrical stimulation. The clinical evaluation showed flaccid hemiplegia affecting the left side and no hint of contraction, with only compensation with the trunk.
Participant 3 (P3) is a 45-year-old male who sustained a right-sided ischemic stroke three years prior to participating in the study, resulting in left hemiparesis. He walked without assistance. He had received intensive and frequent therapy prior to the study. The clinical evaluation revealed spastic hemiparesis in the left upper limb.
None of the patients received any other type of therapy (in addition to NeuroR) during the time span of this study. The last rehabilitation therapy that they had had was at least six months prior to the present study.
2.2. Outcome Measures
Baseline, during- and postintervention measures were performed for all participants. Firstly, spasticity of the shoulder muscles was evaluated using the Modified Ashworth Scale (MAS) at the time of enrollment in the study; more specifically, these were assessed for the impaired upper limb for shoulder adduction, abduction, flexion and extension (
Table 1). MAS was evaluated because, in a spasticity condition, the subscapularis muscle remains tonically active, which negatively influences the velocity and ROM of the targets of the intervention (shoulder abduction and flexion). The same physiotherapist assessed all the participants and conducted all AR training sessions.
Study variables were brain functional connectivity and ROM of shoulder abduction and flexion. Goniometer measurements were obtained at the beginning and end of the sessions. Brain connectivity analysis was performed using rs-fMRI at baseline and after the last training session. Functional connectivity analyses of the rs-fMRI data were performed using a seed placed at the noninjured motor cortex.
2.3. Intervention
The rs-fMRI exams and training sessions were carried out at the Clinics Hospital of the University of Campinas. All three subjects completed one hour of AR training with NeuroR twice a week for four consecutive weeks at the outpatient rehabilitation clinic of this hospital. They also underwent two MRI exams, before the first AR training session and after the last AR training session.
All training sessions were carried out on an individual basis. A licensed physical therapist conducted the training sessions. At the beginning of each session, the physiotherapist showed the participants how to perform the shoulder exercises following the virtual arm. At least two series of ten repetitions of the activities were performed at each training session with 20–40 s of rest after each set. The participants carried out shoulder abduction and flexion exercises with the injured arm, staying seated. At the end of each session, a stretching exercise was performed with the AR arm.
Figure 1 shows the visual feedback in front of the participant while the virtual arm is running shoulder abduction.
The training setup comprised the AR software, a camera attached to a tripod, a multimedia projector, a cloth glove and a physical marker. Virtual arm animations were triggered by the physiotherapist using a keyboard. Images mixing the virtual arm and real-time video were projected onto a white wall in front of the participant. The room layout was arranged so as not to have any object cluttering the line of sight, and no extra illumination was needed. A resolution of 640 × 480 was adopted for all video frames, which were generated by the AR system running on a laptop with a refresh rate of 60 Hz.
2.4. Data Acquisition and Analysis
Before the first (pretest) and after the last (post-test) AR training sessions, the participants were scanned in a 3T magnetic resonance scanner (Achieva, Philips, The Netherlands) to acquire resting-state functional images of the brain. First, anatomical images were acquired on the sagittal plane with the following parameters: T1-weighted, voxel size = 1 × 1 × 1 mm³, image matrix = 240 × 240 × 180, repetition time (TR) = 7.7 ms, echo time (TE) = 3.1 ms and flip angle = 8°. Second, rs-fMRI images were acquired on the axial plane in a 6-min scan with a T2*-weighted echo-planar imaging (EPI) sequence, voxel size = 3 × 3 × 3 mm³, image matrix = 80 × 80 × 40, gap = 0.6 mm, TR = 2000 ms, TE = 30 ms, ascending acquisition and 180 volumes. During the rs-fMRI exams, the participants were instructed to open their eyes (so as not to fall asleep) and to not think of anything in particular.
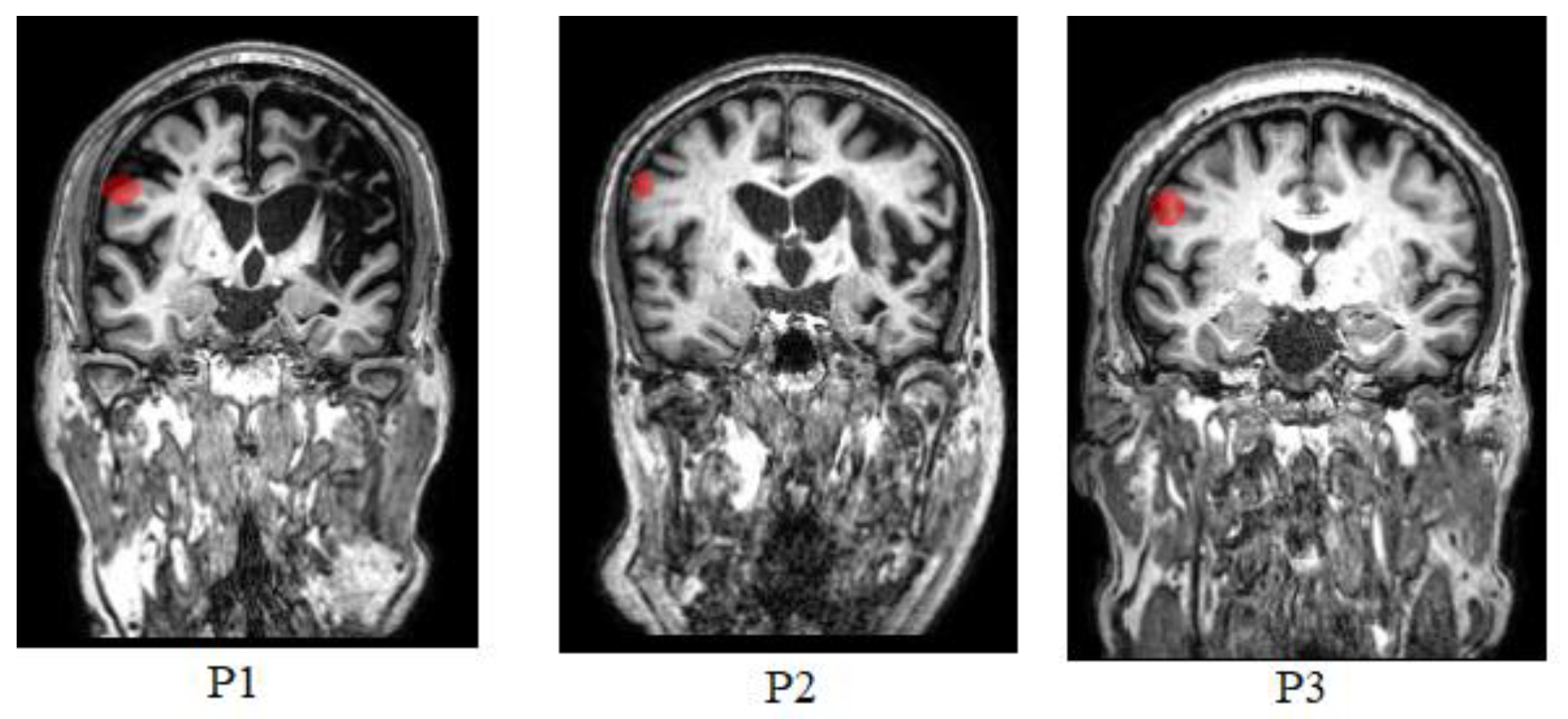
Figure 2 shows the structural 3D data obtained at baseline for the three participants.
Functional connectivity analyses of the rs-fMRI data were performed using a seed placed at the noninjured (left) motor cortex. This is because the injured motor cortex would possibly have little or no signal due to the stroke lesion, particularly before the intervention. Since healthy homotopic motor areas usually have strong connectivity [
29], we expected that neuroplasticity in the injured motor cortex after AR rehabilitation would appear as a signal restoration and therefore as an increase in connectivity (with the noninjured motor cortex) in those regions. According to [
30], functional connectivity between most motor areas is increased in the motor-planning state, while functional connectivity with the cerebellum and basal ganglia is increased during movement. Therefore, we carried out a statistical analysis between the chosen ROI, motor areas and cerebellum parcellations. Several tools were used to perform rs-fMRI data analysis: MATLAB MathWorks
® software, SPM12 software, MRIcron and UF2C [
31]. The image data were processed, and statistical analysis was performed according to the UF2C standard pipeline [
31], namely, definition of the anterior commissure as the origin of the reference system of the structural T1 and rs-fMRI images; fMRI volume realignment (using the mean image as a reference); image registration (fMRI mean image with structural T1); spatial normalization of all images to a standard space and spatial smoothing of fMRI images; and structural T1 tissue segmentation (gray matter, white matter, and cerebral spinal fluid). Additionally, six head motion parameters (three rotational and three translational) were regressed out of the time series as well as the white matter and cerebral spinal fluid average signals. Finally, the time series were bandpass-filtered (0.008–0.1 Hz).
With all the images in a standard space, the Automated Anatomical Labelling (AAL) atlas [
32] was used to segment the images and choose the seed for functional connectivity. This seed was a region of interest (ROI) of 4 × 4 × 4 voxels located in the left precentral area in Brodmann area 4. The ROI was selected in analogous locations for all participants to evaluate functional connectivity related to motor networks. The average time series of all ROI voxels within the participants’ gray matter was computed for use as the seed’s time series. Pearson’s correlation scores were calculated between the seed’s time series and the time series of all gray matter voxels of the brain. Subsequently, average correlation values (over the voxels of a given region) were computed for every AAL area. This was performed by converting these values to z scores (Fisher’s Z transformation), calculating the mean value and transforming them back to the correlation space. Finally, to evaluate and characterize differences between pretest and post-test data, the average correlation values of the AAL atlas regions related to movement (
Table 2) were compared. An intrasubject comparison (for each subject individually) was performed. A paired
t-test was used with a significance level of 0.05.
Additionally, an evaluation of the ROM of the injured shoulder was carried out. Angles of shoulder abduction and flexion were measured before starting and after the end of most AR training sessions to determine the ROM of the injured shoulder, using mechanical goniometers. Goniometer measurements were recorded in a spreadsheet.
3. Results
According to
Table 1, P2 had zero MAS scores for shoulder abduction and flexion, which means he had no muscle resistance for the passive execution of these movements [
33]. P1 also had a zero score for shoulder abduction but had score 2 for shoulder flexion, indicating “a marked increase in muscle tone throughout most of the ROM, but still being able to move affected part(s) with ease” [
33]. Finally, P3 had 1+ MAS score for both shoulder abduction and flexion, meaning he had a “slight increase in muscle tone, manifested as a catch, followed by minimal resistance through the remainder (less than half) of the ROM” [
33].
Due to the different degrees of motor impairment of the patients, the only requirements for shoulder exercise during AR were for them to try to raise their arms (in both flexion and abduction movements) as much as they could. All participants underwent all eight NeuroR training sessions. There were no adverse outcomes for any of the patients.
Table 3 summarizes goniometry data for all participants. Data for P2 were equal to zero angles for all sessions since this participant had the most severe degree of hemiplegia. For P3, it is possible to notice that measurements taken after sessions were usually smaller than measures taken before sessions, which is most likely due to participant fatigue.
Table 4 shows the mean functional connectivity values (considering only positive correlations) over the AAL regions listed in
Table 2 at pretest and post-test for all patients. P1 and P2 presented significant differences (
t-test,
p < 0.05) in functional connectivity in motor-related areas between pretest and post-test, but not P3 (
Table 4).
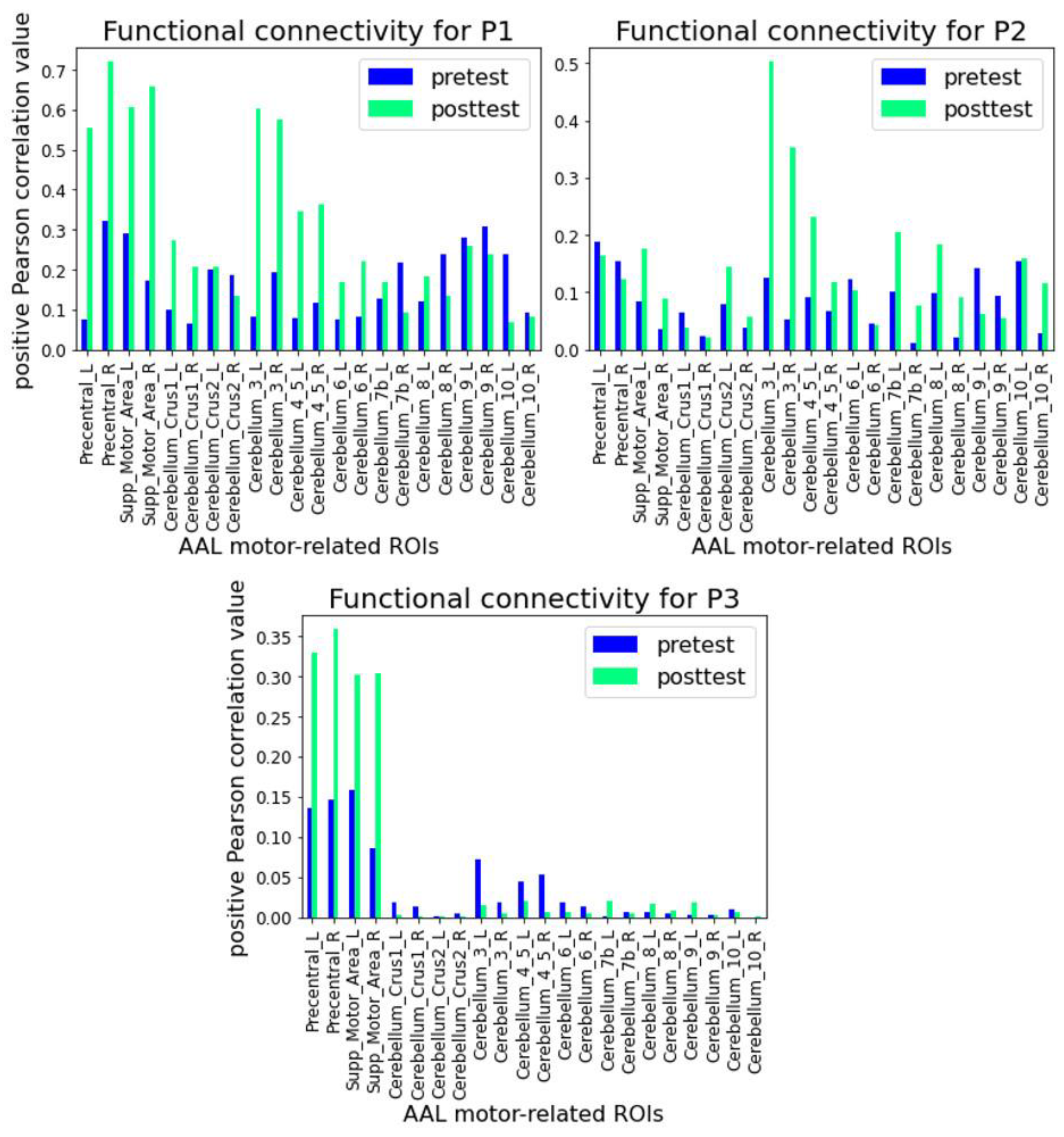
Figure 3 shows plots of mean functional connectivity values for each region of
Table 2 for each participant at both time points. P1 and P3 showed a clear increase in connectivity for the primary motor cortex (precentral gyrus) and supplementary motor area bilaterally after training with NeuroR, but P2 only had an increase in the supplementary motor area (also in both hemispheres). On the other hand, P1 and P2 had functional connectivity increases at post-test in most cerebellum areas, while P3 had very low connectivity values in the cerebellum before and after training.
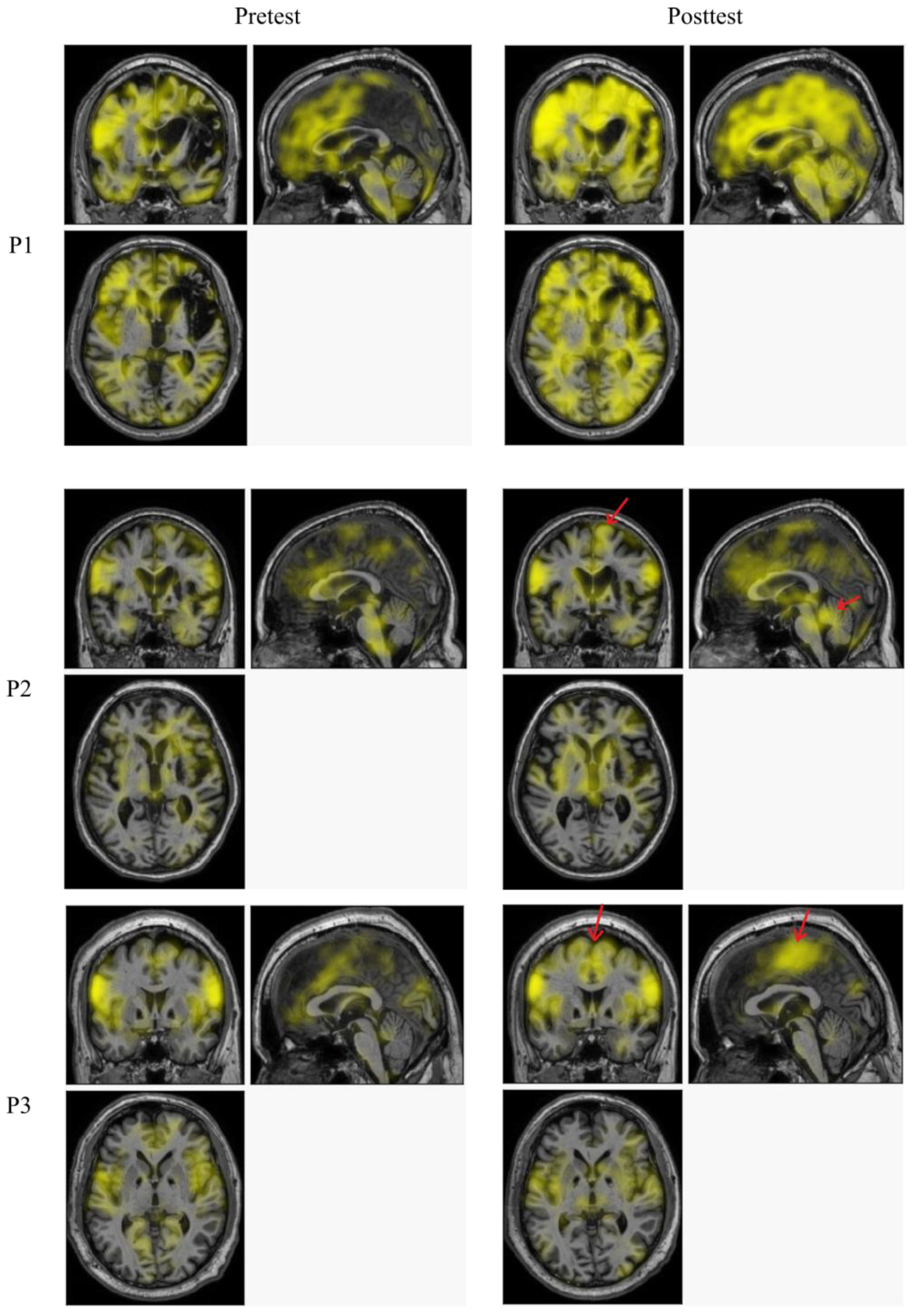
Figure 4 shows positive correlation maps for each patient at pretest (left column) and post-test (right column). The increase in correlation values is evident for P1, for whom even the lesioned area presents higher correlation values at post-test. P2 and P3 had subtler lesions, and although the changes at post-test are not as evident, brighter areas can be seen for P2 at the right motor cortex (red arrow), temporal lobes and cerebellum and at both right and left motor cortices for P3.
4. Discussion
The aim of this study was to evaluate brain functional connectivity changes in three chronic stroke patients resulting from AR-based upper limb rehabilitation with the NeuroR system and to compare these changes with shoulder ROM changes in those patients. Patients completed up to eight sessions of the NeuroR intervention.
For two individuals (P1 and P2), there was a statistically significant increase in the functional connectivity of motor-related areas (motor cortex plus cerebellar areas; see
Table 2) with the seed at the noninjured (left) motor area after the NeuroR training sessions (
Table 4). Moreover, four motor areas (left and right primary and supplementary motor areas) had higher correlation values at post-test than at pretest for P1 and P3, while only the supplementary motor areas had higher correlation values for P2 (
Figure 3). Particularly, connectivity in the right (injured) motor cortex increased for all patients, although with different amplitudes: P1 and P3 had a substantial increase in connectivity both in the right precentral gyrus (about two-fold) and the right supplementary motor area (about three-fold), while P2 had a moderate increase only in the right supplementary motor area (about two-fold), with a small decrease in the right precentral gyrus (about 20%) (
Figure 3). This could possibly indicate the occurrence of neuroplasticity on the injured side, as hypothesized. Regarding the results for P2, since this patient had more movement restrictions (all his goniometry data were zero) than the other patients and flaccid hemiplegia affecting the left side, this could indicate that only his movement planning areas were recruited [
34]. The difference for P3 was nonsignificant; however, unlike the others, this participant reported shoulder pain after AR training. Additionally, since this participant had previously received intensive and frequent therapy, he might have been closer to a plateau than the other patients, which could explain the nonsignificant changes observed. Another factor that may explain the outcome is the age of the patients. It has been reported that advanced age is one of the main social factors that can affect stroke recovery [
35]. While P1 and P3 were in their forties, P2 was in their eighties, which could help describe their poorer performance.
Other studies have reported similar findings. In the study by Song et al., nine stroke patients with persistent upper extremity motor impairment completed up to fifteen two-hour sessions of rehabilitation therapy using brain–computer interface (BCI) technology, and cortical motor activity was assessed using motor-task fMRI data [
36]. They found an increase in corticomotor activity (during finger tapping) associated with worse motor rehabilitation outcomes in the patients. Although rs-fMRI investigates synchronous and spontaneous activity between brain regions occurring in the absence of a task or stimulus, these simultaneous activities have shown close correspondence to brain activation dynamics. Therefore, an rs-fMRI experiment is a potential alternative for mapping motor networks that does not require task performance [
36].
In the study by Schuster-Amft and colleagues, two stroke patients with upper limb motor impairments performed nineteen VR training sessions and showed changes in brain activity revealed using fMRI data [
37]. Analysis of their fMRI data showed recruitment of secondary motor areas [
37]. In our study, three stroke participants with persistent upper extremity motor impairment completed up to eight one-hour sessions of NeuroR training. Rs-fMRI measures showed higher values of functional connectivity in motor areas after AR training for all patients, although for P2, these were only for the supplementary motor areas.
Previous studies using fMRI data have pointed out that increased recruitment of ipsilesional motor areas over the course of treatment is associated with improved outcomes [
38,
39]. According to [
40], brain-based rehabilitation to improve motor function for poststroke patients should promote ipsilesional activity during impaired limb movement for optimal improvement. In our study, P1 and P3 showed higher correlation values/area in the ipsilesional primary and supplementary motor cortices at post-test (
Figure 3 and
Figure 4).
Brauchle et al. pointed out that the functional connectivity networks between the contralateral motor imagery motor network and the entire brain can be evaluated by defining a seed electrode in the ipsilesional primary motor cortex [
27]. Similarly, our outcomes indicated that the functional connectivity of stroke participants can be evaluated by defining a seed of voxels in the noninjured (left) primary motor cortex from rs-fMRI exams.
ROM measures suggested an improvement tendency for two of the participants (P1 and P3), and although the participant with the most severe degree of hemiplegia remained at zero angles (P2), a hint of muscle contraction was observed. Based on this observation, we propose that, in the next study, the muscle strength scale should be used as an evaluation tool rather than goniometry. On the other hand, P3 showed an angle decrease for both shoulder abduction and flexion after sessions compared to before sessions, possibly due to participant fatigue. According to [
41], in the presence of an event of fatigue during a rehabilitation session, either the goals are not achieved or the rehabilitation session is abandoned. Therefore, a control scheme to reduce the effects of muscle fatigue must be planned. In our study, we adopted adequate rest between repetition sessions to reduce fatigue during AR training, but it may not have been sufficient for this patient.
Regarding ROM results for P2, it is interesting to note that according to Su and Xu [
42], various poststroke interventions seek to promote the plasticity of the remaining neural circuit. Notwithstanding, factors such as a long time since stroke, location and size of the lesion and biological factors such as aging can reduce the neuroplasticity effects. In our study, clinical measures showed that P2 (84 years old), who was much older than P1 (49 years old) and P3 (45 years old), remained without gain in flexion and extension in the injured limb after AR training with NeuroR. Although P2 presented an increase in functional connectivity with motor-related areas from 0.082 (pretest) to 0.141 (post-test) (
Table 4), this did not translate into motor improvement for this patient.
Although valuable outcomes were reported in our study, the case series design prevents us from drawing robust conclusions about the impact of augmented reality training exercises on brain connectivity. The design of case series has several limitations and needs further validation from stroke cases with different brain damage features and postonset periods. On the other hand, it is important to draw attention to the difficulties concerning this type of multidisciplinary study, which requires compliance with the subtleties of many different expertise areas, including motor rehabilitation, brain imaging and AR. The main one is that participants are required to come several times to the research facility (be it a clinic, hospital or university) for exams and therapy sessions, but most are impaired and have locomotion problems and thus depend on caregivers to bring them to the sessions. Polese and coworkers [
43] reported that individuals with chronic stroke had low rates of recruitment and retention. In our country, research subjects are not paid. A previous study [
44] revealed a problem of slow recruitment for Brazilian clinical trials with stroke survivors, in which 150 stroke survivors were screened for eligibility and only 10 agreed to participate. According to these authors, the lack of transport was reported as the main obstacle to participating in and attending the training sessions. We also faced those same recruitment challenges, with the addition of funding and schedule limitations. All this results in a high dropout rate. Another limitation was the fact that the participants were all male. Stroke subjects of both sexes, male and female, were invited to participate in the study. We are aware that the underrepresentation of women in cardiovascular disease research has been a long-standing problem [
45]. However, due to schedule constraints, we could not delay the recruitment period to balance the participants’ genders in the study.
Yet another problem with our study could be attributed to the fact that the virtual arm in the AR environment does not appear realistic. Nevertheless, in a previous study with the NeuroR system with four participants, three demonstrated perceiving a “matching” of the NeuroR’s virtual arm with their actual arm [
24]. Only a participant who had suffered an injury in the nucleus of the thalamus and base neglected the relationship between his physical arm and the virtual arm. The authors argued that there is evidence that participants with lesions in the reticular formation or elsewhere in the brain stem may have difficulties in stimulating motor neurons from visual stimuli, affecting their performance in AR-based training [
24], but this was not the case for the patients in the present study. Notwithstanding, improvements in the realistic aspect of the virtual arm of the NeuroR system are already underway. Real disembodiment and re-embodiment are important for the participants to feel a sense of attachment to their avatar self, extending their version of selves in the AR world [
46,
47]. According to [
48], in telepresence scenarios, equal-sized avatars are more influential than small-sized avatars. Therefore, a new version of the NeuroR system will detect the skin pixels in a given initial image [
49] and will provide an equal-sized virtual arm.
Participants reported that they were mostly sedentary for the last 30 days prior to the study. These reported data agree with the outcomes of the study by Fini and colleagues [
50], in which physical activity levels were low at 24 months after rehabilitation discharge for 79 stroke survivors, with no changes over time observed. Further research could investigate the relation between different levels of physical activity and brain connectivity for stroke survivors.
The feasibility of the proposed protocol for AR training was based on the review by Aramaki et al. [
51]. The studies reviewed by these authors performed training sessions two or three times a week, with each session lasting from 30 to 60 min, over 2–12 weeks. In our study, AR sessions happened two times a week for four weeks, and the number of repetitions of AR shoulder flexion and abduction was equally sized to be performed in 30 min, including rest periods and AR stretching at the end. ROM and brain connectivity outcomes suggested that the frequency and number of sessions were feasible.
Finally, functional evaluation scales, such as the Fugl-Meyer assessment, should have been included in the study. This was not executed due to time restrictions during the sessions, but the assessment will be included in a future study.










{kind=link}
{kind=link}
{kind=link}
{kind=link}