Abstract
Heavily advertised as a harmless tobacco alternative, hookah (i.e., waterpipe)-flavored tobacco smoking has contributed to the wider epidemic of smoking, especially amongst marginalized sexual minority (SM) populations. Evidence regarding the concurrent use of substances and other drugs, among SM current hookah smokers, is scarce. We utilized nationally representative data from the Population Assessment of Tobacco and Health (PATH) Study (2016–2019) to examine patterns of the concurrent use of substances (i.e., marijuana, painkillers, sedatives, tranquilizers, cocaine, stimulants (specifically methamphetamines), and others), in SM adult hookah smokers and their heterosexual counterparts. Current hookah smoking is higher among SM adults (Wave 4: 4.22% [95% CI = 2.94–5.94] and Wave 5: 2.65% [95% CI = 1.81–3.48]) than heterosexuals (Wave 4: 1.31% [95% CI = 1.13–1.50] and Wave 5: 1.07% [95% CI = 0.89–1.25]). Among current SM hookah users, the co-use of substances, including alcohol, marijuana, and cocaine, is comparable to heterosexuals (p = ns). Adjusting for gender alone and all covariates, including age, sex, race/ethnicity, education, income, and education, no differences in concurrent substance use were observed between SM and heterosexual hookah users. While the co-use of substances is comparable between SM and heterosexual hookah smoker adults, the prevalence of current hookah use more than doubled among SM individuals than heterosexual individuals during 2018–2019. Our findings highlight the critical value of prevention efforts directed to increase education and awareness about hookah smoking use and known health effects, particularly tailored towards sexual minorities.
1. Introduction
Tobacco use is the leading cause of preventable disease, disability, and death within the United States and globally [1]. With tobacco consumption being popularized, racially targeted products, as well as those marketed as ingestible “stress-relieving” [2], have evolved to include alternative ones such as hookah (i.e., waterpipe) smoking, an evolving flavored tobacco epidemic among youth and young adults [3]. Despite emerging studies challenging the widespread unsubstantiated popular belief that hookah smoking is a harmless tobacco alternative [4], hookah use remains high, particularly among young adults. National representative data from Wave 3 (W3; collected throughout 2015–2016) of the Population Assessment of Tobacco and Health (PATH) Study showed that 9.2% of adults 18–24 years of age reported current (past 30 days) hookah use [5].
While the consumption of hookah-flavored tobacco has primarily affected all gender and ethnic groups, emerging studies highlight increasing use among sexual minority (SM)—lesbian, gay, and bisexual—populations, as compared to heterosexuals [6,7]. Utilizing initial PATH study data (W1 and W2; collected throughout 2013–2015), we previously showed that hookah use among SM adults (ever use W1: 29% and W2: 31%; current use W1: 4% and W2: 3%) was higher than heterosexuals (ever use W1: 16% and W2: 16%; current use W1: 1% and W2: 1%) [8]. Similar trends exist among SM students, where they have reported more days of hookah use than cigarettes, in comparison to their heterosexual counterparts [9].
In addition to higher tobacco use prevalence among SM individuals, sexual minorities demonstrate disparate rates of substance use, including alcohol, marijuana, and other drugs, as compared to heterosexuals [10,11,12]. In fact, studies show that the concurrent use of tobacco and substance use is common among SM individuals [13,14]. SM women have a greater proportion of concurrent drinking and cigarette tobacco smoking days [14], and, more recently, we showed that in W1 and W2 of the PATH study, there was a higher prevalence of the concurrent use of marijuana, stimulants, and sedatives amongst SM hookah smokers [15]. Moreover, SM women and young adults (18–24 years old) had higher odds of concurrent hookah and marijuana use, as compared to heterosexuals [15].
Throughout history, SM communities have experienced disproportionate stresses due to the standardization of heteronormativity, cisgender norms, as well as cultural pressures surrounding the unacceptance of these identities [16]. These stressors have been shown to play a major role in etiologies in tobacco-use-related disparities among SM populations [17]. Notably, as compared to heterosexuals, increased tobacco advertisement and marketing in the form of “direct advertising, indirect advertising, community outreach, and sponsorships” are particularly targeted towards SM populations [18]. The disproportionate number of targeted tobacco product advertisements poses an additional risk factor for SM young adults, leading to a higher prevalence of health adversities.
While the use of tobacco and substances alone poses substantial public health concerns [19], the concurrent use of these substances exponentially increases health-related outcomes and disparities [20]. Indeed, hookah-flavored tobacco smoking has been implicated in a number of negative health outcomes, including cardiovascular, pulmonary, and oral diseases [4,21,22]. Contrary to widely held claims, a systematic review and meta-analysis demonstrated the accumulating scientific evidence associating hookah smoking with cancer, including oral cancer (odds ratio (OR) = 4.17; 95% CI = 2.53–6.89) and lung cancer (OR = 2.12; 95% CI = 1.32–3.42), as well as respiratory diseases, including chronic obstructive pulmonary disease (OR = 3.18, 95% CI = 1.25–8.08) and bronchitis (OR = 2.37, 95% CI = 1.49–3.77) [23]. In addition to tobacco combustion products, hookah smoking exposes users to high levels of charcoal combustion products, including carbon monoxide levels, which has been implicated in substantial increases in hookah-associated carbon monoxide poisoning cases [24,25]. A study utilizing smoking machines estimated that a typical one-hour hookah smoking session emits 30 times the carbon monoxide levels of a single cigarette in the side-stream [26].
To date, little is known about the concurrent use of substances among SM hookah smokers, particularly as compared to heterosexuals. Increasing this knowledge base could help inform prevention and cessation efforts specifically targeted to this group vulnerable to tobacco and substance use. Therefore, the primary goal of this study was to extend the findings of Dobrin et al. [15] by examining the concurrent use of substances, including marijuana, painkillers, sedatives, tranquilizers, cocaine, stimulants (i.e., methamphetamines), and other drugs, among SM adult current hookah smokers and their heterosexual counterparts, using the most recent nationally representative PATH study data (W4 (collected throughout 2016–2018) and W5 (collected throughout 2018–2019)).
2. Materials and Methods
2.1. Study Design
This analysis used longitudinal data from W4 (collected from 1 December 2016 to 3 January 2018) and W5 (collected from 1 December 2018 to 30 November 2019) of the PATH Study, which included a nationally representative cohort of U.S. youth and adults. Wave 5 study participants were interviewed approximately 103 weeks after the W4 interview. The design of the PATH Study allowed data to be collected on various outcomes associated with the use of tobacco and alternative tobacco products, including use patterns, risk perceptions, attitudes, and health outcomes [27]. The study was approved by the Westat Institutional Review Board (IRB). The University of California, Los Angeles IRB, approved the secondary analyses of PATH data. Study analyses were strictly performed in accordance with the relevant guidelines and regulations.
2.2. Measures
2.2.1. Socio-Demographic Characteristics
Demographic data included was age, race/ethnicity, sex, sexual orientation, education level, household income level, health insurance status, and mental health self-perceptions. We defined sexual minorities (SMs) as participants who self-reported their sexual orientation as “lesbian or gay”, “bisexual”, or “something else”. Heterosexuals were defined as those who self-reported their sexual orientation as “Straight, that is, not lesbian or gay”. Participants self-reported their race/ethnicity as any of the following: white non-Hispanic, black non-Hispanic, other non-Hispanic, and Hispanic. Other demographic variables were as follows: age, categorized by 18–24, 25–34, 35–44, 45–54, and ≥55 years of age; sex, categorized as male versus female; education level, categorized as college versus no college; and household income level, categorized as <USD 25,000, USD 25,000–49,999, USD 50,000–99,999, and ≥USD 100,000.
2.2.2. Hookah Use and Substance Use
Inclusion criteria included current hookah smokers, who self-reported the current use of other substances. Current hookah use was defined as participants who self-reported smoking hookah every day or some days during the past 30 days. To study the co-use of hookah tobacco with other substances, we analyzed current hookah users who also indicated the current use (past 30 days) of any of the following substances: alcohol, marijuana, Ritalin®/Adderall®, painkillers/sedatives/tranquilizers, cocaine, simulants, and other drugs (heroin, inhalants, solvents, or hallucinogens). The sample study participants were not exclusive hookah users and could have potentially used additional tobacco/nicotine products, such as cigarettes and/or e-cigarettes, cigars, traditional cigars, filtered cigars, cigarillos, pipe, pipe tobacco, snus pouches, dissolvable tobacco, or smokeless tobacco.
2.3. Statistical Analyses
For each substance outlined above, we used replicate survey weights in SAS 9.4 balanced repeated replication method with Fay’s variant. We estimated the weighted percentages of co-use prevalence with 95% confidence intervals (CIs). For both W4 and W5, Rao-Scott chi-square tests were completed on each to compare SM hookah users to heterosexual hookah users (independent variable) on their use of each substance (dependent variable). Within sex and age group categories, SM vs. heterosexual group differences in co-occurring substances were examined via survey-weighted logistic regression.
3. Results
Overall, a total of 200 SM and 720 heterosexual current hookah smokers participated in PATH studies W4 and W5 (Table 1). Out of 393 current hookah smokers who participated in W5, 345 (87.8%) also participated in W4. In W4, among SMs, 4.22% (95% CI: 2.94–5.49) reported current hookah use, whereas among heterosexuals, 1.31% (95% CI: 1.13–1.50) reported current hookah use. In W5, among SMs, 2.65% (95% CI: 1.81–3.48) reported current hookah use, whereas among heterosexuals, 1.07% (95% CI: 0.89–1.25) reported current hookah use. In W4, the majority of hookah smokers were young adults between 18 and 24 years of age (62% SM and 55% heterosexual individuals, p = ns). In W5, while young adults constituted 51% of SM current hookah smokers, they constituted 38% of heterosexuals. While 79% of SM current hookah smokers self-identified as females in W4, 44% of heterosexuals identified as females (p < 0.0001). In W5, sex distribution was not significantly different between SMs and heterosexuals. In both waves, sexual minority current hookah smokers were predominantly White with some college education and comparable to heterosexuals (p = ns).

Table 1.
Characteristics of study participants (current hookah smokers).
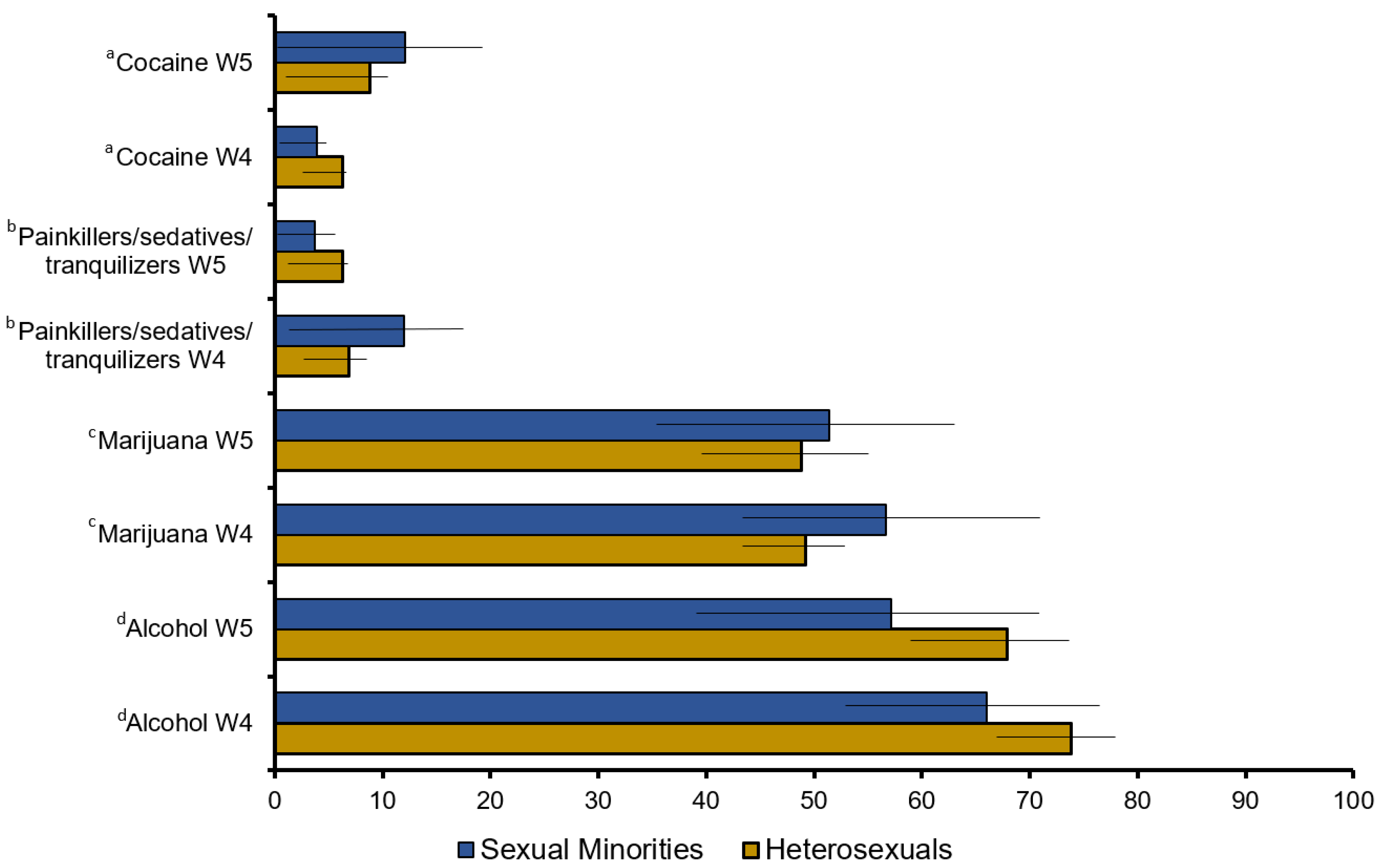
Figure 1 summarizes the prevalence of substance use based on the sexual identity subgroup among hookah smokers. Substances (i.e., Ritalin®/Adderall®, stimulants (i.e., methamphetamines), and other drugs) with fewer than the minimum reportable number of participants were not included in the analysis. The concurrent use of substances, including alcohol, marijuana, and cocaine, was comparable between current SM and heterosexual hookah users (p = ns).
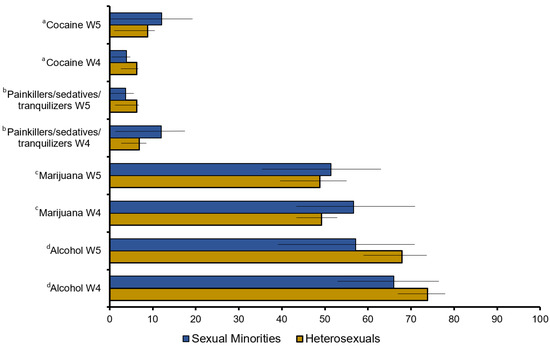
Figure 1.
Substance Use among current hookah users, comparing sexual minorities and heterosexuals. Data represent weighted percentages (95% CI). a Comparison of cocaine use between SM individuals and heterosexuals in W4, p = 0.35 and W5, p = 0.67; b comparison of painkiller/sedative use between SM individuals and heterosexuals in W4, p = 0.25 and W5, p = 0.42; c comparison of marijuana use between SM individuals and heterosexuals in W4, p = 0.36 and W5, p = 0.80; d comparison of alcohol use between SM individuals and heterosexuals in W4, p = 0.22 and W5, p = 0.26. W4 was collected over 2016–2018; W5 was collected over 2018–2019.
Whereas in W4 and compared with heterosexuals, SM hookah smokers reported higher concurrent use of pain killers/sedatives/tranquilizers (6.85% (95% CI = 3.08–10.63) vs. 11.94% (95% CI = 1.85–22.03), reported concurrent use was lower in W5 (6.25% (95% CI = 1.45–11.04) vs. 3.72% (95% CI = 0.00–7.55); Figure 1). For females, 14.54% (95% CI = 1.90–27.17) in W4 and 5.70% (95% CI = 0.00–12.44) in W5 of SM adults, as compared to 8.64% (95% CI = 1.39–15.90) in W4 and 8.94% (95% CI = 2.31–15.56) in W5 heterosexuals, reported the concurrent use of pain killers/sedatives/tranquilizers. For males, 2.03% (95% CI = 0.00–5.57) in W4 and 1.19% (95% CI = 0.00–3.11) in W5 of SM adults, as compared to 5.44% (95% CI = 1.37–9.52) in W4 and 4.01% (95% CI = 0.00–11.41) in W5 heterosexuals, reported the concurrent use of pain killers/sedatives/tranquilizers.
Table 2 summarizes the adjusted odds for concurrent substance use for SM and heterosexual hookah smokers. Adjusted for gender alone as well as all covariates, including age, sex, race/ethnicity, education, income, and education, no differences in concurrent substance use were observed between SM and heterosexual hookah users (Table 2).
Table 2.
Concurrent use of substances among SM and heterosexual hookah smokers.
4. Discussion
Despite the enormous global health burden, studies on tobacco and substance use among SM populations remain understudied. Drawing from a nationally representative U.S. sample of adults 18 years and older, this study provides 2016-to-2019 data on the concurrent use of substances among SM and heterosexual adult hookah smokers. The findings of this study add to the literature focused on alternative tobacco use among SM adults by revealing two noteworthy points. First, study findings indicate a substantially higher prevalence of hookah use among SM individuals, as compared to heterosexual adults. Second, no statistically significant differences were found for concurrent substance use, including cocaine, marijuana, sedatives, and alcohol, between SM and heterosexual hookah smokers, even after adjusting for differences in age, sex, race/ethnicity, education, income, and education.
Though heavily marketed as a harmless tobacco alternative, hookah smoke yields comparable constituents to cigarette smoke, containing abundant amounts of harmful or potentially harmful substances, including oxidants, particulate matter, polycyclic aromatic hydrocarbons, and heavy metals [4,22]. Research has shown that hookah smoking predisposes users to numerous deleterious health effects, including cardiopulmonary diseases, oral and infectious diseases, and cancer [22,28,29]. Furthermore, because burning charcoal is used to char the flavored hookah tobacco during lengthy smoking sessions, significant increases in carbon monoxide levels result in hookah-related carbon monoxide poisoning [24,30,31]. Our study extends prior research by documenting the increasing tobacco use disparities that continue to exist among SM adults. Critically, our findings underline the importance for educational and advocacy efforts to offset the unsubstantiated claims and correct misperceptions surrounding hookah smoking within the SM community.
In 2016–2019, our nationally representative data documents significantly higher prevalence of current hookah use among SM individuals than heterosexuals. While current hookah use decreased among both SM and heterosexual individuals between 2016 and 2019, as compared to heterosexuals, hookah use more than doubled among SM individuals. The lack of SM-specific hookah tobacco public education and other intervention efforts likely contribute to disparities in prevalence among this population vulnerable to tobacco and substance use. Indeed, sexual identity is strongly associated with tobacco use frequency, and SM individuals have not only faced victimization, psychological stress, and identity suppression due to the lack of unacceptance surrounding those who identify beyond cis-gender, but have also been subjected to aggressively targeted tobacco marketing and advertisements [9,32,33,34]. Future studies are warranted to identify and determine specific mechanisms, such as exposure to hookah tobacco marketing and advertisements, which affect patterns of hookah tobacco use.
As compared to the literature on SM cigarette smokers [14,15], and despite the increasing prevalence of SM hookah smokers [8,35,36], few studies have examined concurrent substance use among SM hookah smokers. For example, as compared to heterosexual women, SM women report a greater proportion of cigarette tobacco smoking days and a greater proportion of concurrent alcohol drinking and smoking days [14]. Using the first two waves of the PATH Study data, Dobrin et al.’s study highlighted that SM individuals who smoke hookah were found to have a greater prevalence of concurrent use of substances (i.e., alcohol, marijuana, and other drugs) in comparison to heterosexuals who smoke hookah [15]. It is noteworthy that our current analysis with subsequent W4 and W5 PATH studies showed no significant difference in concurrent substance use between adult SM and heterosexuals who report hookah smoking. It is plausible that negative attitudes and discrimination about homosexuality, which have continued to decrease over time, resulting in reduced stress, have led to reduced substance use among SM populations [37,38]. For example, data from the General Social Survey showed a continued decline in Americans’ negative perceptions towards homosexuality since the 1970s [39]. Study findings indicate the need for substance use treatment interventions, specifically tailored to the needs of SM populations. This is important considering recent nationally representative findings documenting differences between SM and heterosexual individuals in utilizing substance use treatments [40]. Specifically, according to data from the National Survey on Drug Use and Health, and as compared to heterosexuals, gay and lesbian individuals utilize treatment for substance use disorders at higher rates, while bisexuals utilize treatments at lower rates [40].
Although our findings enhance our limited understanding of concurrent substance use among SM hookah smokers using a large nationally representative dataset, there are several limitations to this study. Because PATH data for W4 and W5 were collected prior to the unprecedented 2019 coronavirus pandemic, our findings may not be translatable to current hookah use or prevalence after the pandemic. Because some substances, including Ritalin®/Adderall®, stimulants (i.e., methamphetamines), and other drugs, had relatively small sample sizes, they were not included in our analyses. Smoking and substance use status amongst SM and heterosexual smokers were not biochemically measured and study findings rely on self-reported data. Sexual minority PATH participants were all grouped together in the study surveys. Though the PATH study datasets are longitudinal, the analysis carried out for this paper was cross-sectional. Future PATH waves should separate lesbian/gay populations from their bisexual counterparts to effectively address the needs of each group.
5. Conclusions
Our findings are among the first to document differences in hookah use among SM adults utilizing the most recent PATH study waves, and they reveal that SMs have a significantly higher rate of smoking hookah as compared to their heterosexual counterparts. These results illustrate the need to implement hookah smoking prevention programs, specific to SM populations, through education on causative socioeconomic/cultural agents that may be tied to hookah smoking. Future work should focus on examining the drivers behind hookah use among SM communities, including, but not limited to, social determinants of health, underlying health conditions, as well as the internalization of stress/stigmas. Ultimately, these correlations, as well as detrimental effects of hookah use, should not only reach SM communities, but also marginalized communities that are susceptible to hookah marketing and advertisements.
Author Contributions
Conceptualization and methodology, M.R.-H., U.S.W. and M.-L.B.; investigation, C.S., A.A., A.K., U.S.W., M.-L.B. and M.R.-H.; software, M.-L.B. and U.S.W.; formal analysis, M.R.-H., U.S.W. and M.-L.B.; supervision, M.R.-H.; writing—original draft preparation, C.S. and A.A.; writing—review and editing, C.S., A.A., A.K., U.S.W., M.-L.B. and M.R.-H. All authors have read and agreed to the published version of the manuscript.
Funding
M.R.H. was supported by the National Institute of Health; the National Heart, Lung, and Blood Institute (1R01HL152435-01A1); and the University of California, Tobacco-Related Disease Research Program (T30IP1013).
Institutional Review Board Statement
Ethical approval was obtained from the University of California, Los Angeles Institutional Review Board (protocol code 17-001484) in order to access and analyze the study data.
Informed Consent Statement
Not applicable because this study offers a secondary analysis of publicly available data.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the Population Assessment of Tobacco and Health Study Public-Use Files, https://www.icpsr.umich.edu/icpsrweb/NAHDAP/studies/36498 (accessed on 20 September 2022).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Centers for Diease Control and Prevention. Smoking and Tobaco Use: Tobacco-Related Mortality. 2020. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/tobacco_related_mortality/index.htm (accessed on 10 November 2022).
- Cook, B.L.; Wayne, G.F.; Keithly, L.; Connolly, G. One size does not fit all: How the tobacco industry has altered cigarette design to target consumer groups with specific psychological and psychosocial needs. Addiction 2003, 98, 1547–1561. [Google Scholar] [CrossRef] [PubMed]
- Maziak, W.; Taleb, Z.B.; Bahelah, R.; Islam, F.; Jaber, R.; Auf, R.; Salloum, R.G. The global epidemiology of waterpipe smoking. Tob. Control 2015, 24 (Suppl. 1), i3–i12. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, A.; Maziak, W.; Eissenberg, T.; Ward, K.D.; Thurston, G.; King, B.A.; Sutfin, E.L.; Cobb, C.O.; Griffiths, M.; Goldstein, L.B.; et al. Water Pipe (Hookah) Smoking and Cardiovascular Disease Risk: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e917–e936. [Google Scholar] [CrossRef] [PubMed]
- Sharma, E.; Bansal-Travers, M.; Edwards, K.C.; Halenar, M.J.; Taylor, K.A.; Kasza, K.A.; Day, H.; Hammad, H.T.; Anic, G.; Limpert, J.; et al. Longitudinal pathways of exclusive and polytobacco hookah use among youth, young adults and adults in the USA: Findings from the PATH Study Waves 1–3 (2013–2016). Tob. Control 2020, 29 (Suppl. 3), s155–s162. [Google Scholar] [CrossRef]
- Fallin-Bennett, A.; Lisha, N.E.; Ling, P.M. Other Tobacco Product Use Among Sexual Minority Young Adult Bar Patrons. Am. J. Prev. Med. 2017, 53, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Haardörfer, R.; Vu, M.; Windle, M.; Berg, C.J. Sex and sexual orientation in relation to tobacco use among young adult college students in the US: A cross-sectional study. BMC Public Health 2018, 18, 1244. [Google Scholar] [CrossRef] [PubMed]
- Rezk-Hanna, M.; Holloway, I.W.; Toyama, J.; Warda, U.S.; Berteau, L.C.; Brecht, M.L.; Sarna, L. Transitions in hookah (Waterpipe) smoking by U.S. sexual minority adults between 2013 and 2015: The population assessment of tobacco and health study wave 1 and wave 2. BMC Public Health 2021, 21, 445. [Google Scholar] [CrossRef] [PubMed]
- Azagba, S.; Shan, L. Disparities in the frequency of tobacco products use by sexual identity status. Addict. Behav. 2021, 122, 107032. [Google Scholar] [CrossRef]
- Sönmez, İ.; Palamar, J.J. Sexual Orientation and Age of First Drug Use Among Adults in the United States. Subst. Use Misuse 2022, 57, 1313–1321. [Google Scholar] [CrossRef]
- Ehlke, S.J.; Kendzor, D.E.; Smith, M.A.; Sifat, M.S.; Boozary, L.K.; Cohn, A.M. Single-use, co-use, and polysubstance use of alcohol, tobacco, and cannabis in sexual minority and heterosexual females. Am. J. Addict. 2022, 32, 66–75. [Google Scholar] [CrossRef]
- Rodríguez-Bolaños, R.; Arillo-Santillán, E.; Guzmán-Rodríguez, C.; Barrientos-Gutiérrez, I.; Gallegos-Carrillo, K.; Titus, A.; Cruz-Jiménez, L.; Thrasher, J.F. Similarities and Differences in Substance Use Patterns Among Lesbian, Gay, Bisexual, and Heterosexual Mexican Adult Smokers. LGBT Health 2021, 8, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.M.; Gilmore, A.K.; Rhew, I.C.; Hodge, K.A.; Kaysen, D.L. Minority stress is longitudinally associated with alcohol-related problems among sexual minority women. Addict. Behav. 2016, 61, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Hequembourg, A.L.; Blayney, J.A.; Bostwick, W.; Van Ryzin, M. Concurrent Daily Alcohol and Tobacco Use among Sexual Minority and Heterosexual Women. Subst. Use Misuse 2020, 55, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Dobrin, D.; Means, A.; Cheng, C.W.; Adolfo, A.; Anderson, S.; Warda, U.W.; Brecht, M.L.; Rezk-Hanna, M. Concurrent Hookah (Waterpipe) and Substance Use among Sexual Minority Adults in the United States: Findings from the Population Assessment of Tobacco and Health Study. Psychoactives 2022, 1, 89–101. [Google Scholar] [CrossRef]
- Medina-Martínez, J.; Saus-Ortega, C.; Sánchez-Lorente, M.M.; Sosa-Palanca, E.M.; García-Martínez, P.; Mármol-López, M.I. Health Inequities in LGBT People and Nursing Interventions to Reduce Them: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11801. [Google Scholar] [CrossRef] [PubMed]
- Frost, D.M.; Fingerhut, A.W.; Meyer, I.H. Social change and relationship quality among sexual minority individuals: Does minority stress still matter? J. Marriage Fam. 2022, 84, 920–933. [Google Scholar] [CrossRef] [PubMed]
- Stevens, P.; Carlson, L.M.; Hinman, J.M. An analysis of tobacco industry marketing to lesbian, gay, bisexual, and transgender (LGBT) populations: Strategies for mainstream tobacco control and prevention. Health Promot. Pract. 2004, 5 (Suppl. 3), 129s–134s. [Google Scholar] [CrossRef]
- Omare, M.O.; Kibet, J.K.; Cherutoi, J.K.; Kengara, F.O. A review of tobacco abuse and its epidemiological consequences. Z. Gesundh. Wiss 2022, 30, 1485–1500. [Google Scholar] [CrossRef]
- Linden-Carmichael, A.N.; Stamates, A.L.; Lau-Barraco, C. Simultaneous Use of Alcohol and Marijuana: Patterns and Individual Differences. Subst. Use Misuse 2019, 54, 2156–2166. [Google Scholar] [CrossRef]
- Hawari, F.I.; Obeidat, N.A.; Ayub, H.; Ghonimat, I.; Eissenberg, T.; Dawahrah, S.; Beano, H. The acute effects of waterpipe smoking on lung function and exercise capacity in a pilot study of healthy participants. Inhal. Toxicol. 2013, 25, 492–497. [Google Scholar] [CrossRef]
- Rezk-Hanna, M.; Benowitz, N.L. Cardiovascular Effects of Hookah Smoking: Potential Implications for Cardiovascular Risk. Nicotine Tob. Res. 2019, 21, 1151–1161. [Google Scholar] [CrossRef] [PubMed]
- Waziry, R.; Jawad, M.; Ballout, R.A.; Al Akel, M.; Akl, E.A. The effects of waterpipe tobacco smoking on health outcomes: An updated systematic review and meta-analysis. Int. J. Epidemiol. 2017, 46, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Ashurst, J.V.; Urquhart, M.; Cook, M.D. Carbon monoxide poisoning secondary to hookah smoking. J. Am. Osteopath. Assoc. 2012, 112, 686–688. [Google Scholar] [PubMed]
- Nguyen, V.; Salama, M.; Fernandez, D.; Sperling, J.D.; Regina, A.; Rivera, R.; Wang, J.; Friedman, B.W.; Smith, S.W. Comparison between carbon monoxide poisoning from hookah smoking versus other sources. Clin. Toxicol. 2020, 58, 1320–1325. [Google Scholar] [CrossRef] [PubMed]
- Daher, N.; Saleh, R.; Jaroudi, E.; Sheheitli, H.; Badr, T.; Sepetdjian, E.; Al Rashidi, M.; Saliba, N.; Shihadeh, A. Comparison of carcinogen, carbon monoxide, and ultrafine particle emissions from narghile waterpipe and cigarette smoking: Sidestream smoke measurements and assessment of second-hand smoke emission factors. Atmos Environ. 2010, 44, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Hyland, A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Lambert, E.; Carusi, C.; Taylor, K.; Crosse, S.; Fong, G.T.; Cummings, K.M.; et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob. Control 2017, 26, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Hassane, M.; Rahal, Z.; Karaoghlanian, N.; Zhang, J.; Sinjab, A.; Wong, J.W.; Lu, W.; Scheet, P.; Lee, J.J.; Raso, M.G.; et al. Chronic Exposure to Waterpipe Smoke Elicits Immunomodulatory and Carcinogenic Effects in the Lung. Cancer Prev. Res. 2022, 15, 423–434. [Google Scholar] [CrossRef]
- Qasim, H.; Alarabi, A.B.; Alzoubi, K.H.; Karim, Z.A.; Alshbool, F.Z.; Khasawneh, F.T. The effects of hookah/waterpipe smoking on general health and the cardiovascular system. Environ. Health Prev. Med. 2019, 24, 58. [Google Scholar] [CrossRef]
- Underner, M.; Perriot, J.; Peiffer, G.; Dewitte, J.D.; Jaafari, N. Carbon monoxide poisoning in active or passive shisha smokers. Rev. Mal. Respir. 2020, 37, 376–388. [Google Scholar] [CrossRef]
- Misek, R.; Patte, C. Carbon monoxide toxicity after lighting coals at a hookah bar. J. Med. Toxicol. 2014, 10, 295–298. [Google Scholar] [CrossRef]
- Goldbach, J.T.; Tanner-Smith, E.E.; Bagwell, M.; Dunlap, S. Minority stress and substance use in sexual minority adolescents: A meta-analysis. Prev. Sci. 2014, 15, 350–363. [Google Scholar] [CrossRef] [PubMed]
- Dilley, J.A.; Spigner, C.; Boysun, M.J.; Dent, C.W.; Pizacani, B.A. Does tobacco industry marketing excessively impact lesbian, gay and bisexual communities? Tob. Control 2008, 17, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.A.; Thomson, K.; Offen, N.; Malone, R.E. “If you know you exist, it’s just marketing poison”: Meanings of tobacco industry targeting in the lesbian, gay, bisexual, and transgender community. Am. J. Public Health 2008, 98, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- King, B.A.; Dube, S.R.; Tynan, M.A. Current tobacco use among adults in the United States: Findings from the National Adult Tobacco Survey. Am. J. Public Health 2012, 102, e93–e100. [Google Scholar] [CrossRef] [PubMed]
- Agaku, I.T.; King, B.A.; Dube, S.R. Current cigarette smoking among adults—United States, 2005–2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 29–34. [Google Scholar] [PubMed]
- Smith, T.W. Public Attitudes toward Homosexuality. NORC/University of Chicago. 2011. Available online: https://www.norc.org/PDFs/2011%20GSS%20Reports/GSS_Public%20Attitudes%20Toward%20Homosexuality_Sept2011.pdf (accessed on 8 December 2020).
- Glick, S.N.; Cleary, S.D.; Golden, M.R. Brief Report: Increasing Acceptance of Homosexuality in the United States Across Racial and Ethnic Subgroups. J. Acquir. Immune Defic. Syndr. 2015, 70, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Rijst, V.; Garfield, J.L. Adverse Effects of Tobacco Products (Cigarettes, E-Cigarettes, Hookah, Smokeless Tobacco) Use on Health. In Tobacco Dependence. Respiratory Medicine; Eakin, M.N., Kathuria, H., Eds.; Humana: Cham, Switzerland, 2023; pp. 23–24. [Google Scholar] [CrossRef]
- Hodges, J.C.; Goings, T.C.; Vaughn, M.G.; Oh, S.; Salas-Wright, C.P. Sexual minorities and substance use treatment utilization: New evidence from a national sample. J. Subst. Use Addict. Treat. 2023, 150, 209060. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).