
Psychiatrists’ Engagement in Research as a Pathway towards the Expansion of Distributed Medical Education (DME): A Regional Analysis across Two Provinces in Atlantic Canada


 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Procedure and Data Collection
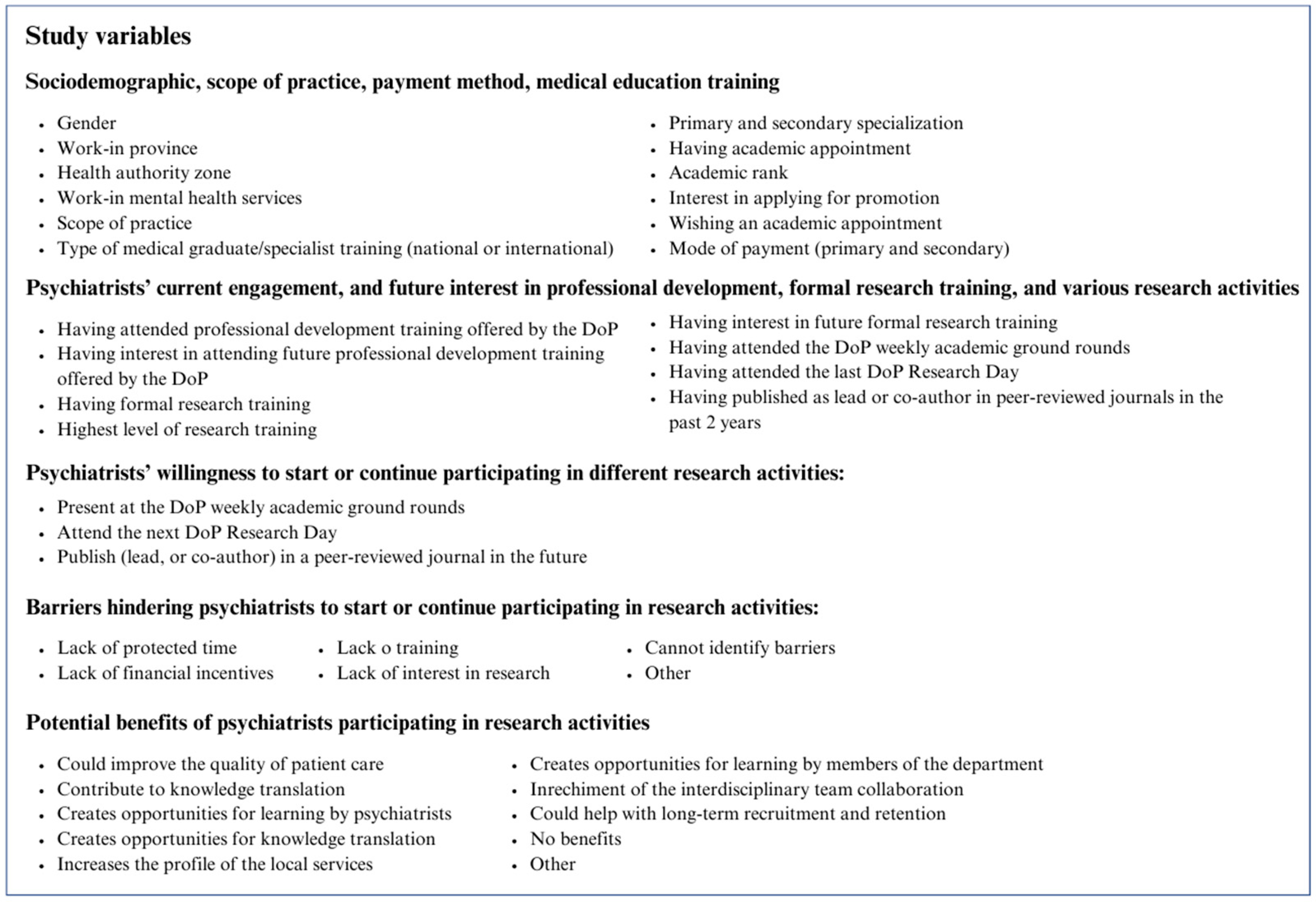
2.4. Outcome Measures
2.5. Statistical Analysis
2.6. Ethics Considerations
3. Results
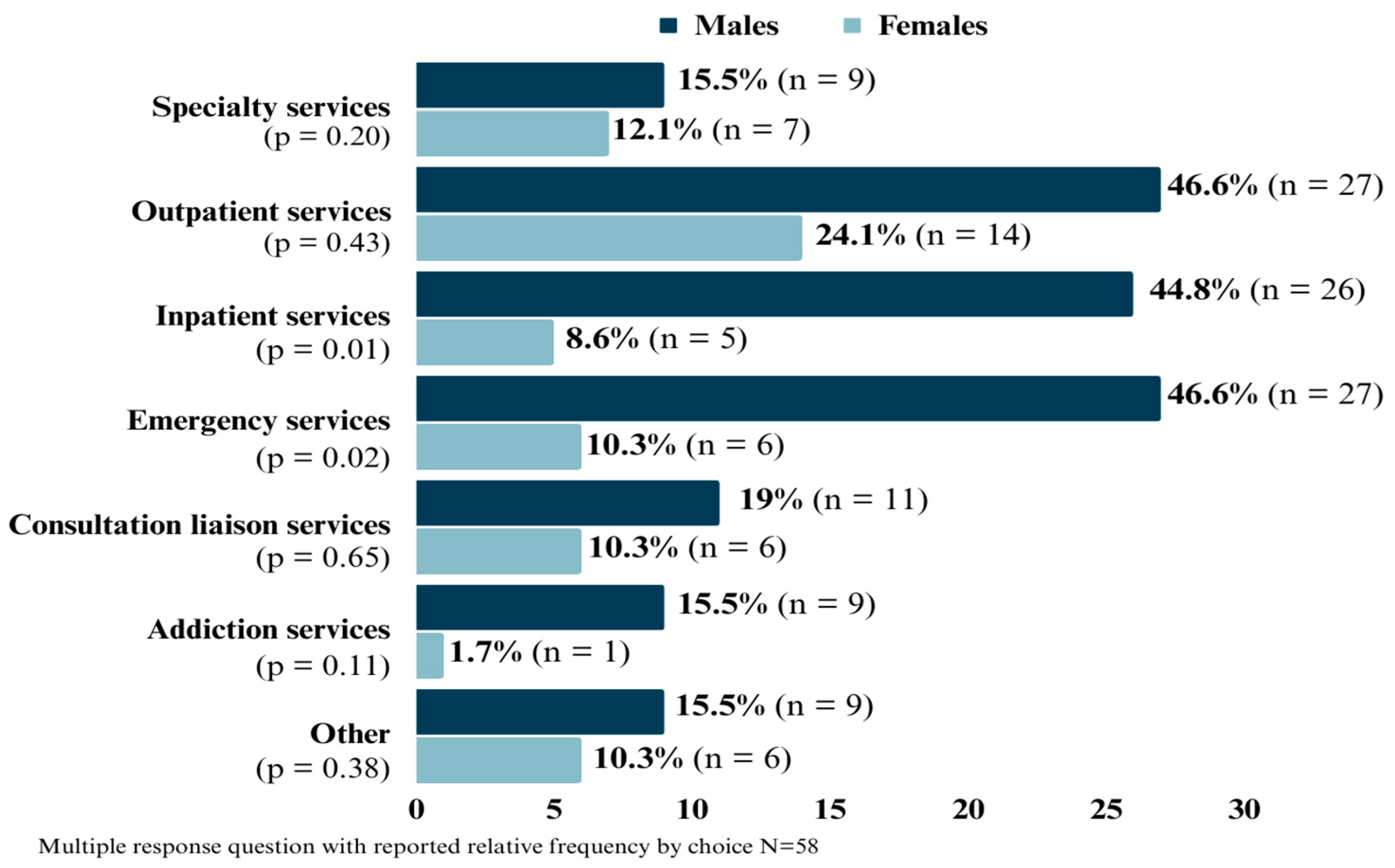
3.1. Sociodemographic Characteristics
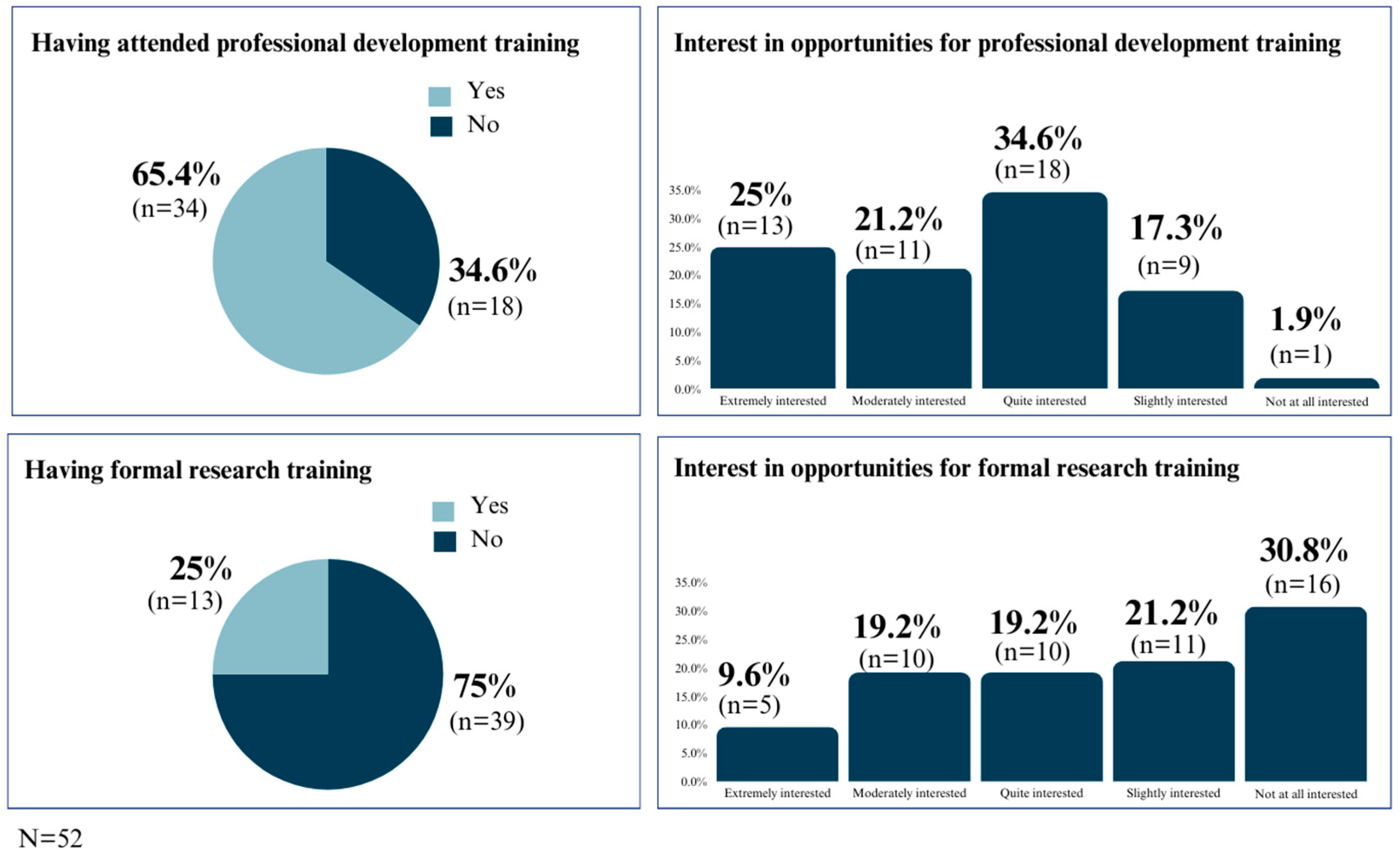
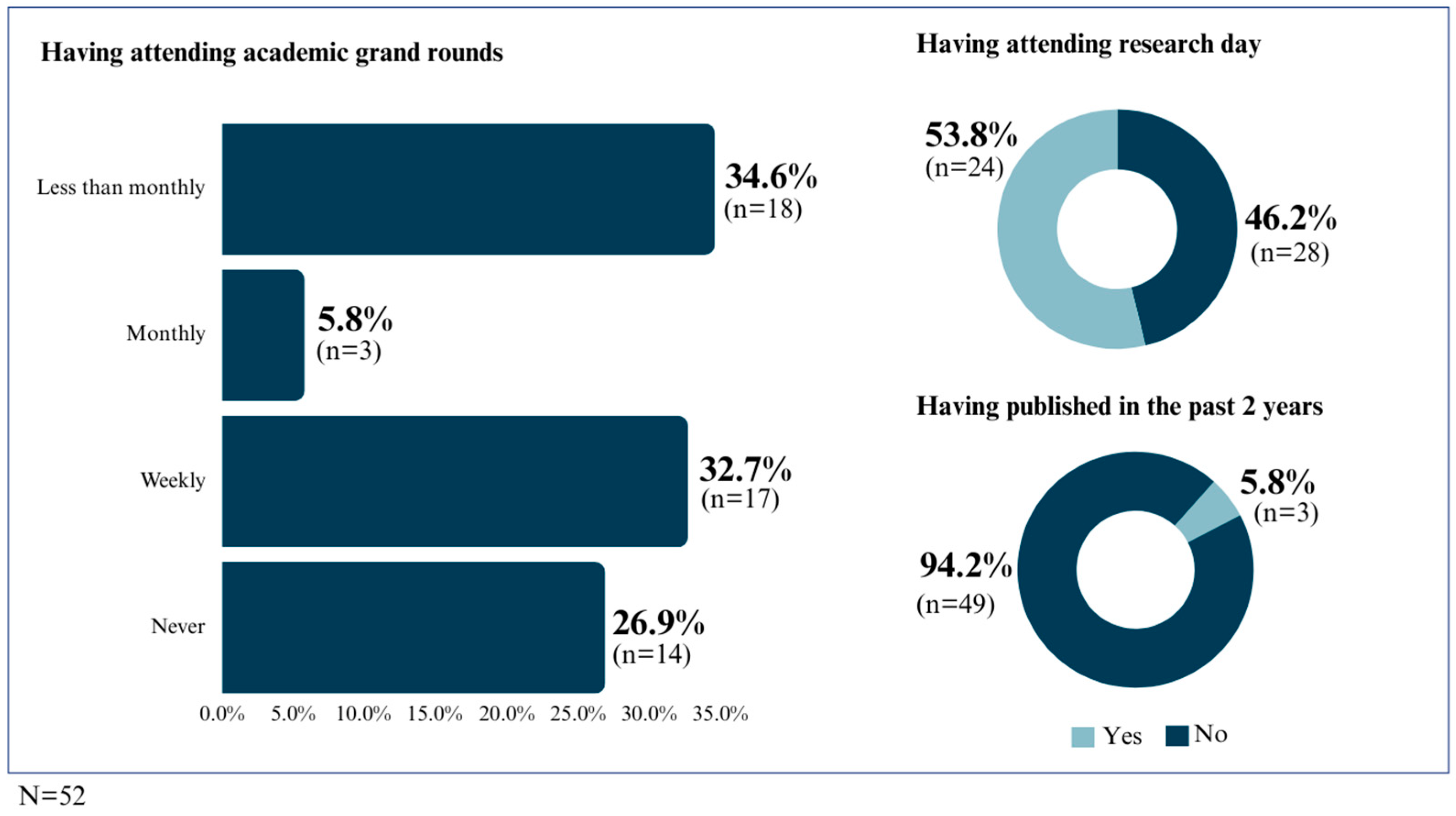
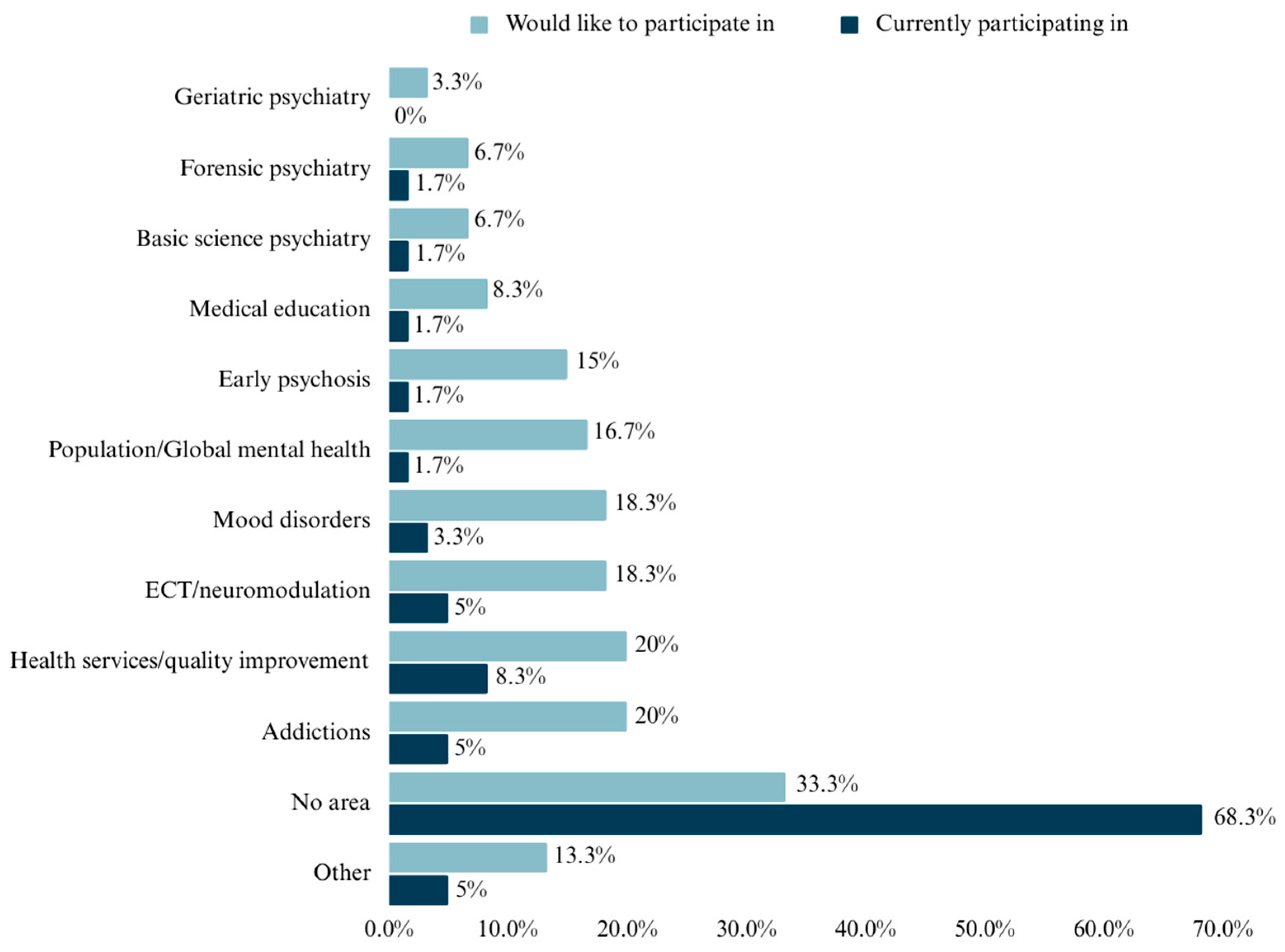
3.2. Current Participation and Future Interest of Psychiatrists in Research Training and Research Activities
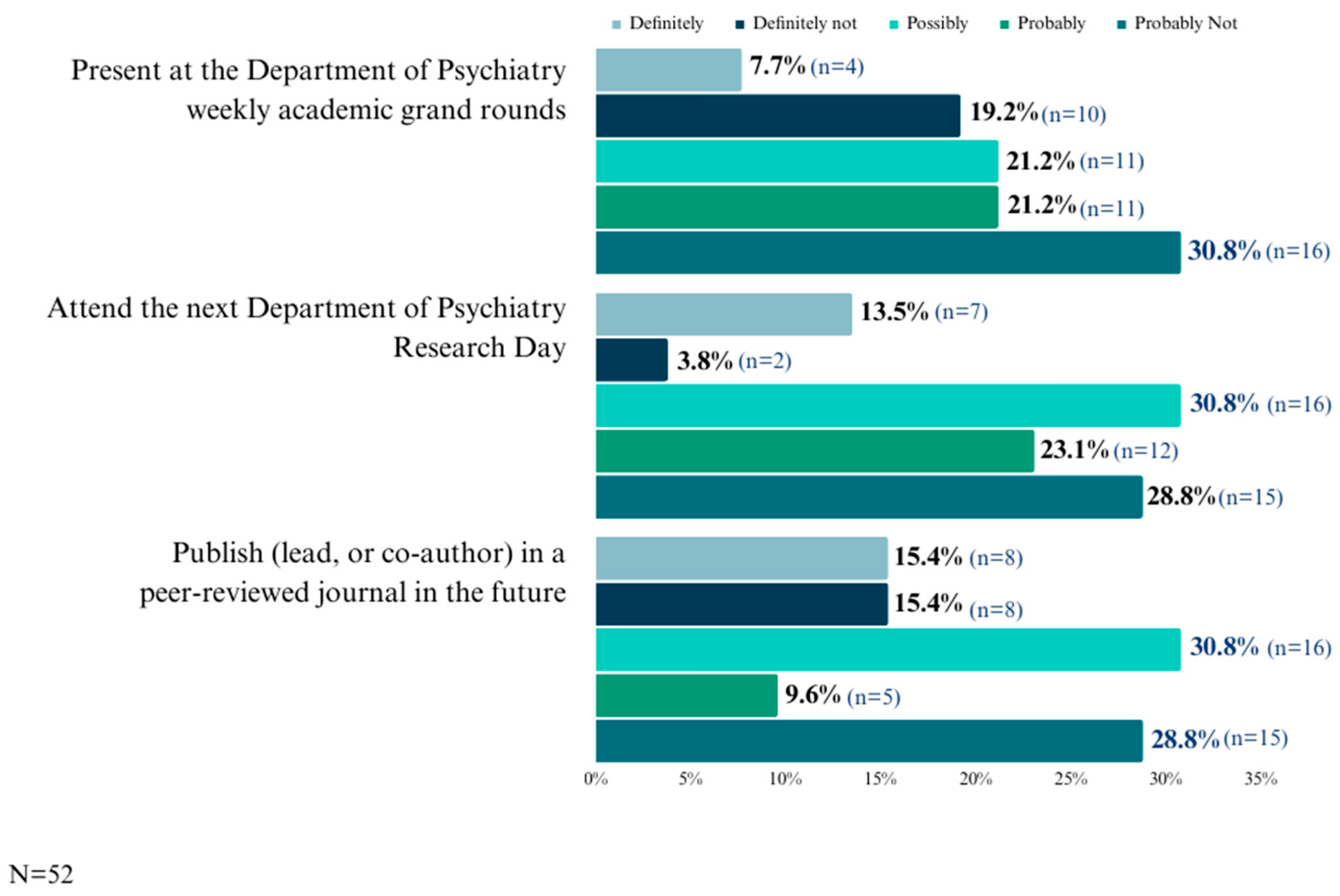
3.3. Psychiatrists’ Willingness to Participate in Research Activities
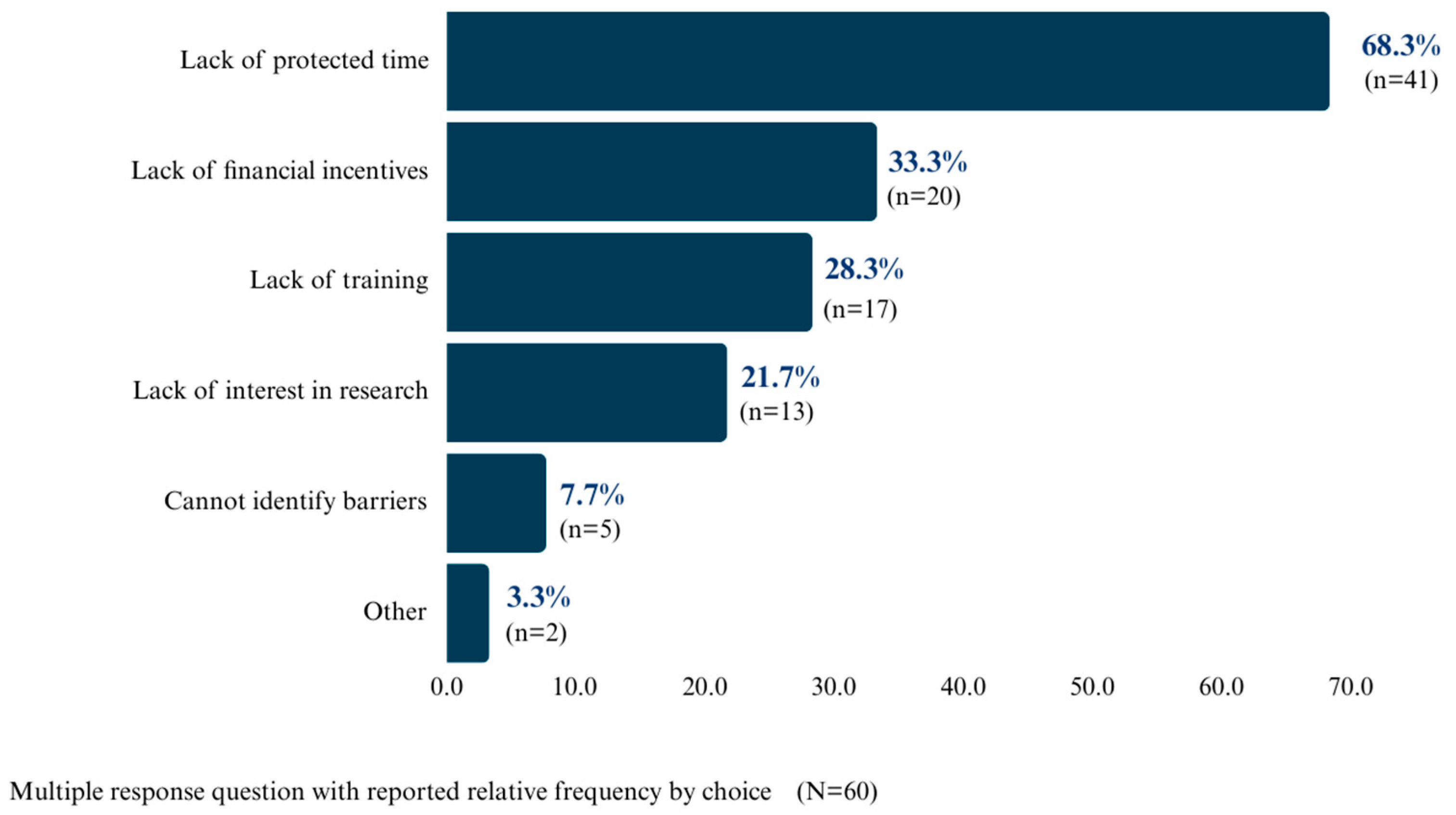
3.4. Barriers to Engaging in Research Activities
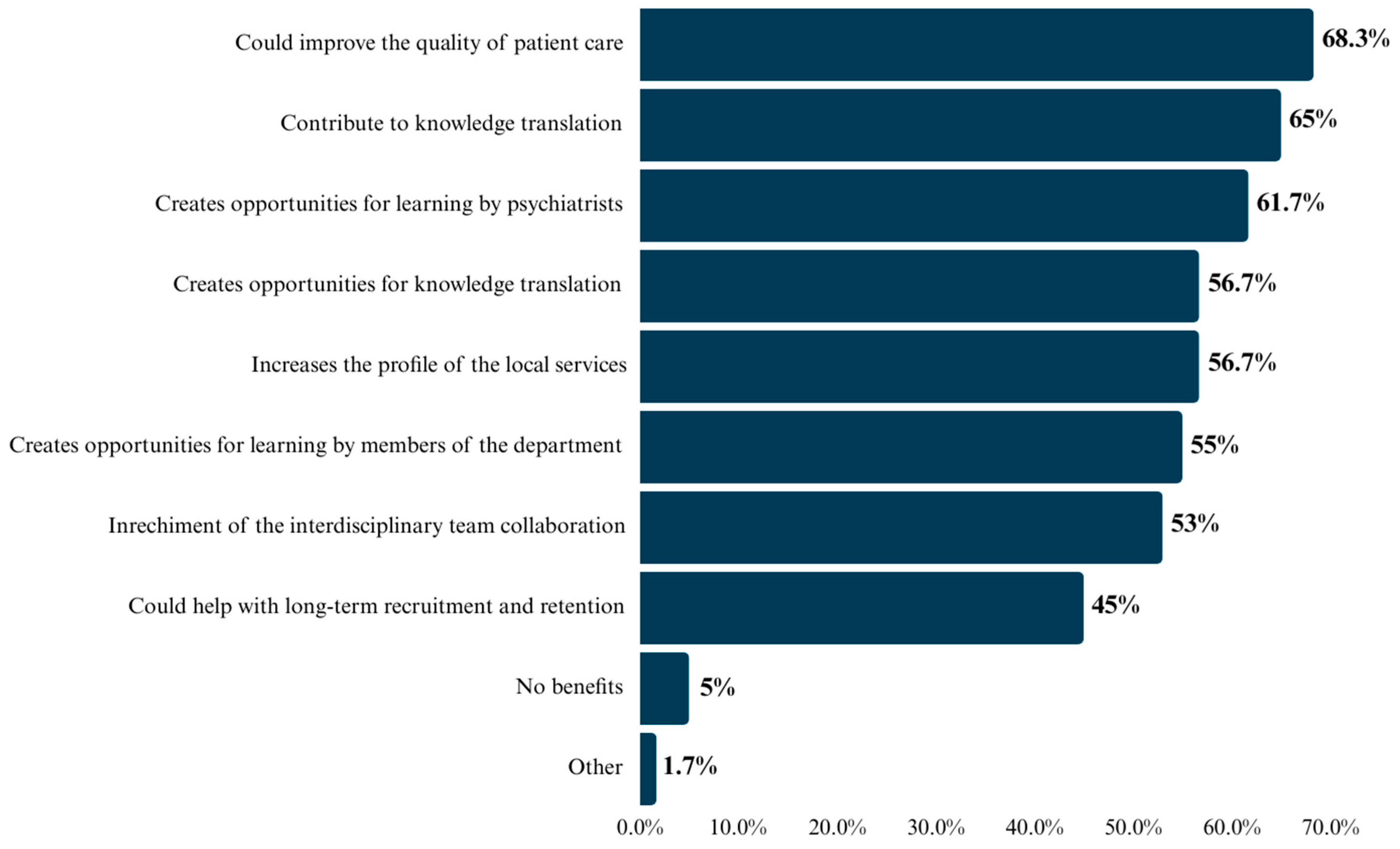
3.5. Potential Benefits of Psychiatrists Participating in Research Activities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ellaway, R.; Bates, J. Distributed medical education in Canada. Can. Med. Educ. J. 2018, 9, e1. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institute for Health Information. A Profile of Physicians in Canada, 2020. Available online: https://www.cihi.ca/en/a-profile-of-physicians-in-canada-2020 (accessed on 24 November 2023).
- Ellaway, R.H.; O’Gorman, L.; Strasser, R.; Marsh, D.C.; Graves, L.; Fink, P.; Cervin, C. A critical hybrid realist-outcomes systematic review of relationships between medical education programmes and communities: BEME Guide No. 35. Med. Teach. 2016, 38, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Bates, J.; Schrewe, B.; Ellaway, R.H.; Teunissen, P.W.; Watling, C. Embracing standardisation and contextualization in medical education. Med. Educ. 2019, 53, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Burrows, A.M.; Laupland, K.B. Comprehensiveness of distributed medical education systems: A regional population-based perspective. BMC Med. Educ. 2021, 21, 42. [Google Scholar] [CrossRef]
- Canadian Medical Association. Number of Physicians by Province/Territory and Specialty, Canada; Canadian Medical Association: Ottawa, ON, Canada, 2019. [Google Scholar]
- Friesen, E. The Landscape of Mental Health Services in Rural Canada. Univ. Tor. Med. J. 2019, 96, 47–52. [Google Scholar]
- Hippe, J.; Maddalena, V.; Heath, S.; Jesso, B.; McCahon, M.; Olson, K. Access to health services in Western Newfoundland, Canada: Issues, barriers and recommendations emerging from a community-engaged research project. Gatew. Int. J. Community Res. Engagem. 2014, 7, 67–84. [Google Scholar] [CrossRef][Green Version]
- The Association of Faculties of Medicine of Canada. Mapping Undergraduate Distributed Medical Education in Canada; AFMC: Ottawa, ON, Canada, 2010. [Google Scholar]
- Lee, J.; Walus, A.; Billing, R.; Hillier, L.M. The role of distributed education in recruitment and retention of family physicians. Postgrad. Med. J. 2016, 92, 436–440. [Google Scholar] [CrossRef]
- Myhre, D.L.; Hohman, S. Going the distance: Early results of a distributed medical education initiative for Royal College residencies in Canada. Rural. Remote Health 2012, 12, 2151. [Google Scholar] [CrossRef]
- Toomey, P.; Lovato, C.Y.; Hanlon, N.; Poole, G.; Bates, J. Impact of a regional distributed medical education program on an underserved community: Perceptions of community leaders. Acad. Med. 2013, 88, 811–818. [Google Scholar] [CrossRef]
- da Costa, M.P. Early career psychiatrists–history, 2020 and beyond. World Psychiatry 2020, 19, 127. [Google Scholar] [CrossRef]
- Burford, C. Attitudes to research among Royal Free psychiatric trainees and consultants. Bull. R. Coll. Psychiatr. 1987, 11, 254–257. [Google Scholar] [CrossRef]
- Burke, J.D.; Pincus, H.A.; Pardes, H. The clinician-researcher in psychiatry. Am. J. Psychiatry 1986, 143, 968–975. [Google Scholar] [PubMed]
- Hanney, S.; Boaz, A.; Soper, B.; Jones, T. Engagement in research: An innovative three-stage review of the benefits for health-care performance. Health Serv. Deliv. Res. 2013, 1. [Google Scholar] [CrossRef]
- Harding, K.; Lynch, L.; Porter, J.; Taylor, N.F. Organisational benefits of a strong research culture in a health service: A systematic review. Aust. Health Rev. 2016, 41, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Blevins, D.; Farmer, M.S.; Edlund, C.; Sullivan, G.; Kirchner, J.E. Collaborative research between clinicians and researchers: A multiple case study of implementation. Implement. Sci. 2010, 5, 76. [Google Scholar] [CrossRef] [PubMed]
- McNair, R.; Taft, A.; Hegarty, K. Using reflexivity to enhance in-depth interviewing skills for the clinician-researcher. BMC Med. Res. Methodol. 2008, 8, 73. [Google Scholar] [CrossRef] [PubMed]
- Foerster, A.; Meadows, G. How useful is a six-month research option for trainee psychiatrists? Psychiatr. Bull. 1989, 13, 301–302. [Google Scholar] [CrossRef]
- Strydom, A.; Higgins, N. Are dedicated research posts of value to psychiatry trainees? Psychiatr. Bull. 2004, 28, 260–263. [Google Scholar] [CrossRef]
- Hazelton, L.; da Luz Dias, R.; Esliger, M.; Tibbo, P.; Sinha, N.; Njoku, A.; Satyanarayana, S.; Siddhartha, S.; Alexiadis-Brown, P.; Rahman, F.; et al. Exploring Current Practices, Needs, and Barriers for Expanding Distributed Medical Education and Scholarship in Psychiatry: Protocol for an Environmental Scan Using a Formal Information Search Approach and Explanatory Design. JMIR Res. Protoc. 2023, 12, e46835. [Google Scholar] [CrossRef]
- Object Planet. Opinio 7.20; Computer Software. 2023. Available online: https://www.objectplanet.com/opinio/ (accessed on 18 February 2023).
- IBM Corp. IBM SPSS Statistics for Windows, version 28.0. Computer Software. IBM Corp.: Armonk, NY, USA, 2020.
- Canadian Institutes of Health Research; Natural Sciences and Engineering Research Council of Canada; Social Sciences and Humanities Research Council of Canada. TCPS-2. Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans; Medical Research Council of Canada: Ottawa, ON, Canada, 2014.
- Mok, P.S.; Baerlocher, M.O.; Abrahams, C.; Tan, E.Y.; Slade, S.; Verma, S. Comparison of Canadian medical graduates and international medical graduates in Canada: 1989–2007. Acad. Med. 2011, 86, 962–967. [Google Scholar] [CrossRef]
- Vasile, V.; Bunduchi, E.; Stefan, D.; Comes, A.; Vasile, R.; Stefan, B. Are We Facing a Radical Change in the Migration Behavior of Medical Graduates from Less Developed Countries? Demographic Profile vs. Social Push Factors. Int. J. Environ. Res. Public Health 2023, 20, 4894. [Google Scholar] [CrossRef] [PubMed]
- Toyin-Thomas, P.; Ikhurionan, P.; Omoyibo, E.E.; Iwegim, C.; Ukueku, A.O.; Okpere, J.; Nnawuihe, U.C.; Atat, J.; Otakhoigbogie, U.; Orikpete, E.V.; et al. Drivers of health workers’ migration, intention to migrate and non-migration from low/middle-income countries, 1970–2022: A systematic review. BMJ Glob. Health 2023, 8, e012338. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.; Boone, A.; Godderis, L.; Bouman, J.; Szemik, S.; Matranga, D.; de Winter, P. The Race to Retain Healthcare Workers: A Systematic Review on Factors that Impact Retention of Nurses and Physicians in Hospitals. J. Health Care Organ. Provis. Financ. 2023, 60, 469580231159318. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Saboor, S.; Naveed, S.; Chaudhary, A.M.D.; Ullah, I.; Ashraf, N.; Khosa, F. Gender and Racial Trends among Geriatric Psychiatry Fellows in the USA: A Call to Action. Psychiatr. Q. 2022, 93, 559–570. [Google Scholar] [CrossRef]
- American Association of Geriatric Psychiatry (AAGP). Available online: https://www.aagponline.org/index.php?src=gendocs&ref=CareersGeriatricPsychiatry&category=Main%20 (accessed on 20 December 2023).
- Koelkebeck, K.; Andlauer, O.; Asztalos, M.; Jovanovic, N.; Kazakova, O.; Naughton, S.; Pantovic-Stefanovic, M.; Riese, F.; da Costa, M.P. Research by Psychiatric Trainees and Early Career Psychiatrists—Results of a Survey from 34 Countries in Europe. Front. Psychiatry 2021, 12, 718669. [Google Scholar] [CrossRef] [PubMed]
- Statistics of Canada. Population Projections for Canada (2021 to 2068), Provinces and Territories (2021 to 2043). Available online: https://www150.statcan.gc.ca/n1/pub/91-520-x/91-520-x2022001-eng.htm (accessed on 20 December 2023).
- Yin, C.; Steadman, P.E.; Apramian, T.; Zhou, T.E.; Ishaque, A.; Wang, X.; Kuzyk, A.; Warsi, N. Training the next generation of Canadian Clinician-Scientists: Charting a path to success. Clin. Investig. Med. 2017, 40, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Donowitz, M.; Anderson, J.; Cominelli, F.; Germino, G. The attrition of young physician-scientists: Problems and potential solutions. In The Vanishing Physician-Scientist? Schafer, A.I., Ed.; Cornell University Press: Ithaca, NY, USA, 2009. [Google Scholar]
- Lockyer, J.M.; Brezina, S.; Thanke, J.; Beck, P.L.; Hollenberg, M.D.; Hemmelgran, B.R.; Taber, S.; Harris, K.A.; Gorman, L.; Strong, M. Clinician Scientists in Canada: Supporting Innovations in Patient Care through Research; Royal College of Physicians and Surgeons of Canada: Ottawa, ON, Canada, 2016. [Google Scholar]
- Lander, B.; Hanley, G.E.; Atkinson-Grosjean, J. Clinician-scientists in Canada: Barriers to career entry and progress. PLoS ONE 2010, 5, e13168. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Azim Majumder, M.A.; Shaban, S.F.; Rahman, N.; Ahmed, M.; Abdulrahman, K.B. Physician participation in clinical research and trials: Issues and approaches. Adv. Med. Educ. Pract. 2011, 2, 85–93. [Google Scholar] [CrossRef]
- Beckett, M.; Quiter, E.; Ryan, G.; Berrebi, C.; Taylor, S.; Cho, M.; Pincus, H.; Kahn, K. Bridging the gap between basic science and clinical practice: The role of organizations in addressing clinician barriers. Implement. Sci. 2011, 6, 35. [Google Scholar] [CrossRef]
- Ariail, J.; Thomas, S.; Smith, T.; Kerr, L.; Richards-Slaughter, S.; Shaw, D. The value of a writing center at a medical university. Teach. Learn. Med. 2013, 25, 129–133. [Google Scholar] [CrossRef]
- Scherer, R.W.; Ugarte-Gil, C.; Schmucker, C.; Meerpohl, J.J. Authors report lack of time as main reason for unpublished research presented at biomedical conferences: A systematic review. J. Clin. Epidemiol. 2015, 68, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Ajjawi, R.; Crampton, P.E.S.; Rees, C.E. What really matters for successful research environments? A realist synthesis. Med. Educ. 2018, 52, 936–950. [Google Scholar] [CrossRef] [PubMed]
- Oshiro, J.; Caubet, S.L.; Viola, K.E.; Huber, J.M. Going Beyond “Not Enough Time”: Barriers to Preparing Manuscripts for Academic Medical Journals. Teach. Learn. Med. 2020, 32, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Zallman, L.; Tendulkar, S.; Bhuyia, N.; Dube, B.; Early, S.; Arredondo, M.; Puleo, R.; Sengupta, N.; Alsan, B.; Hacker, K. Provider’s perspectives on building research and quality improvement capacity in primary care: A strategy to improve workforce satisfaction. Clin. Transl. Sci. 2013, 6, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Michelson, K.A.; Nigrovic, L.E.; Nagler, J.; McAneney, C.M.; Mistry, R.D. Research interest in pediatric emergency medicine fellows. Pediatr. Emerg. Care 2017, 36, e38–e42. [Google Scholar] [CrossRef] [PubMed]
- Koelkebeck, K.; Stefanovic, M.P.; Frydecka, D.; Palumbo, C.; Andlauer, O.; Riese, F.; Jovanovic, N.; da Costa, M.P. Barriers and facilitators to conducting research by early career psychiatrists: A literature review. Glob. Psychiatry 2019, 2, 135–154. [Google Scholar] [CrossRef]
- Ciemins, E.L.; Mollis, B.L.; Brant, J.M.; Hassell, L.A.; Albritton, S.; Amoroso, P.; Baldwin, L.M. Clinician engagement in research as a path toward the learning health system: A regional survey across the northwestern United States. Health Serv. Manag. Res. 2020, 33, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.L.; Cation, L.J. Developments: Impact of a residency research program on research activity, faculty involvement, and institutional cost. Teach. Learn. Med. 2005, 17, 159–165. [Google Scholar] [CrossRef]
- Wenke, R.J.; Mickan, S.; Bisset, L. A cross-sectional observational study of research activity of allied health teams: Is there a link with self-reported success, motivators and barriers to undertaking research? BMC Health Serv. Res. 2017, 17, 114. [Google Scholar] [CrossRef]
- Pink, D.H. Drive: The Surprising Truth about What Motivates Us; Penguin: London, UK, 2011. [Google Scholar]
- Elma, A.; Nasser, M.; Yang, L.; Chang, I.; Bakker, D.; Grierson, L. Medical education interventions influencing physician distribution into underserved communities: A scoping review. Hum. Resour. Health 2022, 20, 31. [Google Scholar] [CrossRef]
- Johnston, A.; Malhi, R.; Cofie, N.; Jokic, R.; Goertzen, J.; Smith-Windsor, T.; Makwarimba, E.; Girouard, M.H.; Badcock, S.; Bell, A. Currencies of recognition: What rewards and recognition do canadian distributed medical education preceptors value? MedEdPublish 2022, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Christner, J.G.; Dallaghan, G.B.; Briscoe, G.; Casey, P.; Fincher, R.M.E.; Manfred, L.M.; Margo, K.I.; Muscarella, P.; Richardson, J.E.; Safdieh, J.; et al. The community preceptor crisis: Recruiting and retaining community-based faculty to teach medical students—A shared perspective from the Alliance for Clinical Education. Teach. Learn. Med. 2016, 28, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Silberman, E.K.; Belitsky, R.; Bernstein, C.A.; Cabaniss, D.L.; Crisp-Han, H.; Dickstein, L.J.; Kaplan, A.S.; Hilty, D.M.; Nadelson, C.C.; Scheiber, S.C. Recruiting researchers in psychiatry: The influence of residency vs. early motivation. Acad. Psychiatry 2012, 36, 85–90. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Female | Male | Total | Chi2 (df) | p Value |
|---|---|---|---|---|---|
| (1) Participant characteristics | |||||
| Works in-province | |||||
| New Brunswick | 8 (44.4) | 19 (47.5) | 27 (46.6) | 0.05 (1) | 0.81 |
| Nova Scotia | 10 (55.6) | 21 (52.5) | 31 (53.4) | ||
| Works in horizon health zone | |||||
| HZ1 NB: Moncton/SE area | 2 (11.1) | 6 (15.0) | 8 (13.8) | * | 0.31 |
| HZ2 NB: Fundy Shore and Saint John Area | 2 (11.1) | 10 (25.0) | 12 (20.7) | ||
| HZ3 NB: Fredericton and River Valley Area | 4 (22.2) | 3 (7.5) | 7 (12.1) | ||
| Eastern Zone NS | 1 (5.6) | 5 (12.5) | 6 (10.3) | ||
| Northern Zone NS | 4 (22.2) | 3 (7.5) | 7 (12.1) | ||
| Western Zone NS | 5 (27.8) | 13 (32.5) | 18 (31.0) | ||
| Type of medical graduates | |||||
| IMG | 8 (44.4) | 30 (75.0) | 38 (65.5) | 5.13 (1) | 0.02 |
| CMG | 10 (55.6) | 10 (25.0) | 20 (34.5) | ||
| Type of completed specialist training | |||||
| International specialist training | 5 (27.8) | 23 (57.5) | 28 (48.3) | 4.39 (1) | 0.04 |
| Canadian specialist training | 13 (72.2) | 17 (42.5) | 30 (51.7) | ||
| Having an academic appointment | |||||
| Yes | 13 (72.2) | 29 (72.5) | 42 (72.4) | 0.00 (1) | 0.98 |
| No | 5 (27.8) | 11 (27.5) | 16 (27.6) | ||
| Academic rank | |||||
| Adjunct | 1 (7.7) | 0 (0.0) | 1 (2.4) | * | 0.34 |
| Assistant Professor | 10 (76.9) | 23 (79.3) | 33 (78.6) | ||
| Associate Professor | 0 (0.0) | 3 (10.3) | 3 (7.1) | ||
| Lecturer | 0 (0.0) | 1 (3.4) | 1 (2.4) | ||
| Unsure | 2 (15.4) | 2 (6.9) | 4 (9.5) | ||
| Interest in applying for promotion to a higher academic rank | |||||
| Extremely interested | 1 (7.7) | 4 (13.8) | 5 (11.9) | * | 0.74 |
| Moderately interested | 3 (23.1) | 4 (13.8) | 7 (16.7) | ||
| Not at all interested | 2 (15.4) | 8 (27.6) | 10 (23.8) | ||
| Quite interested | 3 (23.1) | 8 (27.6) | 11 (26.2) | ||
| Slightly interested | 4 (30.8) | 5 (17.2) | 9 (21.4) | ||
| Would like an academic appointment | |||||
| Definitely | 3 (60.0) | 4 (36.4) | 7 (43.8) | * | 0.71 |
| Possibly | 0 (0.0) | 2 (18.2) | 2 (12.5) | ||
| Probably | 1 (20.0) | 4 (36.4) | 5 (31.3) | ||
| Probably Not | 1 (20.0) | 1 (9.1) | 2 (12.5) | ||
| (2) Practice related variables | |||||
| Primary specialization or scope of practice | |||||
| General adult Psychiatry | 8 (44.4) | 29 (72.5) | 37 (63.8) | * | 0.03 |
| Child and adolescent psychiatry | 6 (33.3) | 9 (22.5) | 15 (25.9) | ||
| Geriatric Psychiatry | 3 (16.7) | 0 (0.0) | 3 (5.2) | ||
| Other | 1 (5.6) | 2 (5.0) | 3 (5.2) | ||
| Secondary specialization or scope of practice | |||||
| Addiction Psychiatry | 0 (0.0) | 5 (12.5) | 5 (8.6) | * | 0.57 |
| Child and Adolescent Psychiatry | 1 (5.6) | 2 (5.0) | 3 (5.2) | ||
| Consultation Liaison Psychiatry | 1 (5.6) | 1 (2.5) | 2 (3.4) | ||
| Emergency Psychiatry | 0 (0.0) | 4 (10.0) | 4 (6.9) | ||
| General Adult Psychiatry | 3 (16.7) | 6 (15.0) | 9 (15.5) | ||
| Geriatric Psychiatry | 2 (11.1) | 3 (7.5) | 5 (8.6) | ||
| I do not have a secondary specialization | 6 (33.3) | 13 (32.5) | 19 (32.8) | ||
| Other | 5 (27.8) | 6 (15.0) | 11 (19.0) | ||
| (3) Payment related variables | |||||
| Primary mode of payment for the delivered psychiatric services | |||||
| Salary with benefits (e.g., pension) | 6 (33.3) | 13 (32.5) | 19 (32.8) | * | 0.08 |
| Fee for service | 1 (5.6) | 9 (22.5) | 10 (17.2) | ||
| Sessional fees | 5 (27.8) | 3 (7.5) | 8 (13.8) | ||
| Alternate Funding Plan | 2 (11.1) | 11 (27.5) | 13 (22.4) | ||
| Other | 4 (22.2) | 4 (10.0) | 8 (13.8) | ||
| Secondary mode of payment for the delivered psychiatric services | |||||
| Alternate Funding Plan | 0 (0.0) | 1 (2.5) | 1 (1.7) | * | 0.8 |
| Fee for service | 6 (33.3) | 15 (37.5) | 21 (36.2) | ||
| Other, please specify: | 1 (5.6) | 2 (5.0) | 3 (5.2) | ||
| Salary with benefits (e.g., pension) | 0 (0.0) | 3 (7.5) | 3 (5.2) | ||
| Sessional fees | 0 (0.0) | 2 (5.0) | 2 (3.4) | ||
| There is no secondary mode of payment | 11 (61.1) | 17 (42.5) | 28 (48.3) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obeng Nkrumah, S.; Dias, R.d.L.; Hazelton, L.; Esliger, M.; Brown, P.A.; Tibbo, P.G.; Sinha, N.; Njoku, A.; Satyendra, S.; Siddhartha, S.; et al. Psychiatrists’ Engagement in Research as a Pathway towards the Expansion of Distributed Medical Education (DME): A Regional Analysis across Two Provinces in Atlantic Canada. Int. Med. Educ. 2024, 3, 62-77. https://doi.org/10.3390/ime3010006
Obeng Nkrumah S, Dias RdL, Hazelton L, Esliger M, Brown PA, Tibbo PG, Sinha N, Njoku A, Satyendra S, Siddhartha S, et al. Psychiatrists’ Engagement in Research as a Pathway towards the Expansion of Distributed Medical Education (DME): A Regional Analysis across Two Provinces in Atlantic Canada. International Medical Education. 2024; 3(1):62-77. https://doi.org/10.3390/ime3010006
Chicago/Turabian StyleObeng Nkrumah, Samuel, Raquel da Luz Dias, Lara Hazelton, Mandy Esliger, Peggy Alexiadis Brown, Philip G. Tibbo, Nachiketa Sinha, Anthony Njoku, Satyanarayana Satyendra, Sanjay Siddhartha, and et al. 2024. "Psychiatrists’ Engagement in Research as a Pathway towards the Expansion of Distributed Medical Education (DME): A Regional Analysis across Two Provinces in Atlantic Canada" International Medical Education 3, no. 1: 62-77. https://doi.org/10.3390/ime3010006
APA StyleObeng Nkrumah, S., Dias, R. d. L., Hazelton, L., Esliger, M., Brown, P. A., Tibbo, P. G., Sinha, N., Njoku, A., Satyendra, S., Siddhartha, S., Rahman, F., Maguire, H., Gray, G., Bosma, M., Parker, D., Raji, A., Manning, A., Bagnell, A., Shalaby, R., & Agyapong, V. I. O. (2024). Psychiatrists’ Engagement in Research as a Pathway towards the Expansion of Distributed Medical Education (DME): A Regional Analysis across Two Provinces in Atlantic Canada. International Medical Education, 3(1), 62-77. https://doi.org/10.3390/ime3010006