Abstract
Reflection facilitates medical education and professional practice by enhancing active and deep learning from experiences. The reflection period is a time for self-awareness and self-assessment of learning events and experiences to improve future experiences (e.g., skill acquisition). Advocates for reflection suggest that reflective practice has the power to enhance professionalism as it provides an opportunity for critical thinking. It can be of variable length and depth; however, the process should be explorative and factual. Critical reflection is a broader and in-depth consideration of historical, cultural and political contexts to challenge and change one’s or a group’s assumptions and actions. Although the process is beneficial to achieving the intended learning objectives, its impact on educational and clinical outcomes remains unclear in anaesthesia. The usefulness of reflection in the learning process or work practices varies depending on personal, professional and organisational factors. Several models and approaches are described to facilitate the reflection process. However, assessment of reflection within the curriculum boundaries and for workplace-based learning activities is complex and challenging due to the lack of validated tools for different types of reflection. PubMed and Google Scholar were searched for articles on reflection and its application in anaesthesia. The anaesthesia literature has minimal information on the theoretical and research aspects of reflective learning and teaching. This review aims to outline the purpose of reflection, discuss the utilisation of commonly used reflection models and underline the intricacy of reflection in anaesthesia learning, teaching and practice. This article highlights crucial factors which may foster or hinder reflection and its effectiveness in achieving meaningful intended outcomes.
Keywords:
anesthesia; anesthesiologists; reflection; professionalism; education; reflective learning 1. Introduction
Anaesthesia providers learn, teach and work in multidisciplinary and complex healthcare environments. We must be skillful and knowledgeable in wide-ranging specialty-related tasks and non-technical skills such as communication, teamwork and leadership. In recent years, reflective learning and practice have been recommended for competency achievement and are mandatory for the relicensing and revalidation of medical professionals, including anaesthetists in the UK [1]. Reflection is a skill composed of a sequential set of steps to describe, analyse, write and improve learning experiences in the classroom or clinical areas. However, the operationalisation and practical aspects of reflection for learners and teachers can be challenging because of several meanings and interpretations of reflection described in the literature. One definition suggests reflection is a metacognition self-regulatory process (controllable and developable), can occur at all stages (before, during and after) of experience, considers self and situational contexts and has a definite purpose [2].
Self-reflection is a recognised component to cultivate professionalism in medical education and practice [3]. It is considered a deliberate process to achieve in-depth meaning and reform professional values [3]. Several reflection methods/models can be applied to enable continuous professional development in anaesthesia education and practice. Supervisors in anaesthesia should be familiar with the reflection process and have mentoring, communication and feedback skills to facilitate critical reflection [2]. Reflection is looking beyond self-learning/the working environment to make real sense of situations and events.
Critical reflection comprises individual learner-/provider-centred interactions with broader contexts to explore and express thoughts, actions, self-assumptions and biases [4]. It demands the ability to inquire, probe and challenge from different perspectives, including ethical, social and political, for a deep understanding of the experience [4]. Formal assessment and evaluation of reflective practice are not a curriculum component during anaesthesia training. It is formidable because no uniform tool can examine all reflective pieces [5]. The nature of reflection and the surrounding confounding variables make its quantitative and qualitative evaluation complex. One systematic review synthesising 29 studies of reflective practice in health professions concluded that rigorous research is required to understand reflective practice’s elements and their impact on the qualities of professional development [6].
This article discusses the purpose of reflection and how to process it and summarises applicable models to enhance learning in anaesthesia. Problems related to reflective education and practice are highlighted, including barriers to practical reflection. Finally, the review outlines values and measures to strengthen reflective learning and training. The PubMed and Google Scholar databases were searched for the literature on the use and application of reflection in anaesthesia education and practice. A detailed search strategy is described in the Supplementary File.
2. Purpose of Reflection
One of the valid reasons to develop reflective learning and practice is that professional and regulatory organisations have integrated it into the curriculum, portfolio, appraisal and professional revalidation [1,7]. Based on the translational evidence from other fields, anaesthesia trainees and providers in the UK must reflect on a wide range of activities, including continuing medical activities, log books, critical incidents, complaints, etc. The Royal College of Anaesthetists (RCOA) advises to follow GMC and Academy of Medical Royal Colleges (AoMRC) guidance. Professional organisations, including the RCOA, widely accept that reflecting on clinical practice is not only important for individual well-being and professional development, but it is also valuable in helping improve the quality of care for patients [1,7]. Reflection theorists illuminate that it is crucial to cultivate and integrate it into professional education, health systems, work and growth as science and evidence-based medicine have limitations in modern complex medical practice [1,2,6,8].
The utilisation of reflection as a medium to learn a wide range of personal and professional values in medicine is a common area of focus for reflection-related research [9,10]. However, unlike in many other humanistic fields (e.g., social care), medical specialties, including anaesthesia, have few investigations to comprehend how reflection can influence the development of professional competencies and patient-level outcomes [11]. A more defined construct of reflection, an intelligible process and trained supervisors/mentors could guide and facilitate reflection and track student progress [12]. The reflection applies to several educational activities during anaesthesia training and improvements in professional enactments (Table 1).

Table 1.
Potential purposes of reflection in anaesthesia education and professional practice.
2.1. Educational
Reflection facilitates identifying learning needs, formulating learning objectives and achieving learning outcomes [2]. The integration of new learning with existing knowledge/skills during reflection results in continuous improvement in learning [6]. Reflective learning has been associated with wide-ranging positive learning outcomes in knowledge, skills and attitudes, essential to achieving competency [7,9,10]. In a systematic review of 16 heterogonous studies of reflection as a learning tool, medical graduates found that being reflective enhanced engagement, improved attitudes and positively impacted learning complex subjects [11].
Using a reflective framework, the learner can sensibly analyse self-experiences and events with improved self-awareness and empowerment [8]. With greater insight, there is an aptitude for identifying deficiencies and opportunities. The reflective process encourages learners to explore the circumstances leading to the problem [11,12]. For example, while learning airway management skills, the student can be challenged to understand the airway problem and its management. The teacher explores reasoning for their thoughts, actions and attitudes. Guided reflection, facilitated by a faculty, is expected to further an active and meaningful learning culture.
2.2. Clinical
Reflection provides a structural approach to describing, analysing and evaluating clinical events to plan future actions [12]. Reflective practice can influence patient care by improving understanding of clinical problems and prompting us to seek solutions [2]. When faced with a clinical dilemma, reflective doctors are less likely to make errors in diagnosis because of the ability to analyse and synthesise new understanding of the problem [13]. Although no evidence exists in anaesthesia, reflection is adopted as a tool for better decision-making and managing broader health issues and problems [1].
Debriefing is widely used in clinical crises and simulated settings to teach various technical and non-technical skills [14]. Reflection during debriefing is intentional, structured and guided in a limited period; however, mainly it is verbal. There is evidence that reflection pauses during focused debriefing enhance individual and team performance, promote communications and limit the negative impact on healthcare providers following critical events [15,16].
During perioperative care, a holistic approach to patient-centred care has gained importance in providing patient-centred care for rehabilitation, enhanced recovery, pain management, etc. Group reflection involving multi-professionals is practical and may be more valuable than self-reflection for multidisciplinary care [6,8]. Also, anaesthetists are valued members of multiple multidisciplinary team (MDT) governance groups within hospitals. Team reflection during MDT activities, including audit meetings, case reviews (e.g., challenging or complicated surgical cases) and related clinical concerns (e.g., complaints and incidents) provide an opportunity to improve patient safety and quality of care. In the national health service in the UK, patient feedback is valuable to provide patient-centred care, gain insight and improve the provision of services. Critical reflection on patients’ feedback or reported outcomes related to patient care will likely improve their interactions and understanding of their treatment perceptions and avoid misinterpretation of their feelings [17].
2.3. Personal
Frustrations and difficulties may arise while learning or managing a complex task. In such circumstances, critical reflection can prompt individuals to fully understand specific aspects of learning and reasons (e.g., personal, social, cultural) affecting learning outcomes. Critical thinking and considering broader contexts and evidence empower individuals to examine and evaluate self-assumptions and biases in a challenging problem [18,19,20]. As a result, the learner can frame and reframe personal or professional experiences/circumstances from different perspectives and improve self-behaviours [19]. Reflection may resolve conflicts by better understanding the underlying causes and factors influencing them, e.g., interpersonal conflict [21].
3. Reflection Process
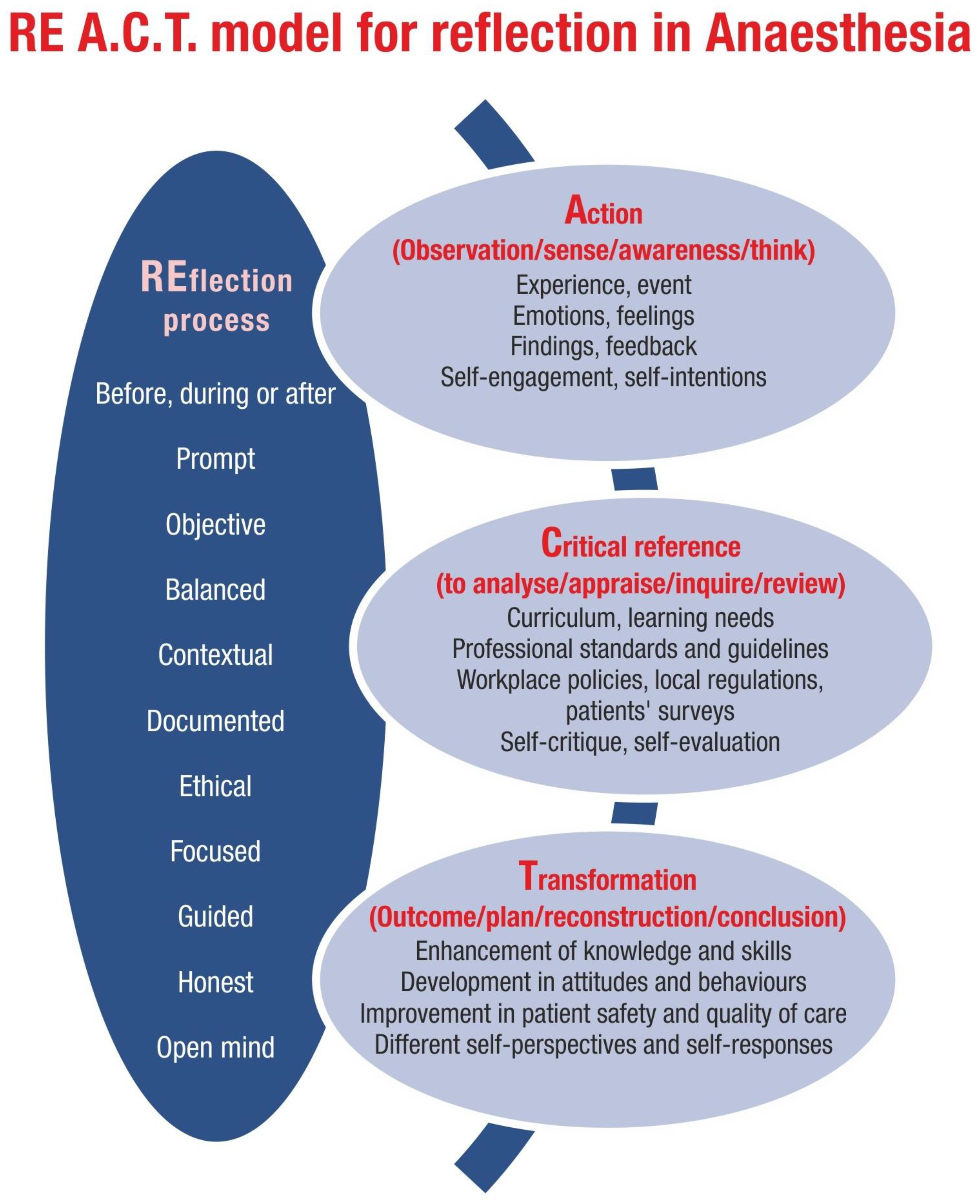
Practising reflection is vital to discovering new knowledge and questions and brainstorming experiences. Reflection is a proactive engagement to gain insights into events/ideas for life-long learning and professional development. Reflection should not be considered a tick-box exercise or a simple description of events. Sander suggests reflection is approached with metacognition and can occur at all encountered stages with a definitive purpose [2]. Whether reflection is necessary while learning all clinical problems has yet to be discovered in anaesthesia. Mamede and colleagues [13] studied internal medicine residents to understand the effects of automatic (non-analytic) and reflective reasoning on diagnosing simple or complex cases. Reflective practice may improve diagnoses in uncertain and unique situations, reducing errors. Therefore, in addition to the individual aptitude to reflect, the utility of reflection may depend on the circumstances being contemplated.
Several elements are essential for reflection to be purposeful during learning and practice in anaesthesia (Figure 1).

Figure 1.
A model for reflection in anaesthesia.
3.1. Models for Reflection
There are several models for applying reflective practice to learning [22,23,24,25,26,27,28,29,30]; Table 2 summarises the main component and their advantages and limitations. Although elements of models and frameworks foster reflection practically, the theoretical features and boundaries of reflection often vary across scholars. The AoMRC has also published a template for reflection and has examples of how to process it [7]. Most reflective practice models are cyclical and retrospective and can be used individually or collaboratively with peers or facilitators/supervisors.
Table 2.
Models for reflection and their strength and limitations.
For example, reflection based on the Gibbs reflection model is included in Box 1.
Box 1. Use of Gibbs’ cycle for reflection.
Anaesthetist A had a problematic tracheal intubation for
an emergency laparotomy during the night shift. After three attempts, he
asked for specialised equipment. However, it was not immediately available
because it was moved to another clinical location in the hospital. He asked
for help from a colleague on call in the intensive care unit who could not
come as he was busy. The patient’s oxygenation remained low for a few
minutes. Finally, a video laryngoscope was located in another clinical area
and bought for use. Tracheal intubation was successful, and surgery was
completed.
Description:
What happened? When? Where? What were the actions taken?
How will other colleagues approach a similarly difficult airway management
scenario? What was the result of actions taken to manage the problem?
Feelings:
Describe emotions/feelings before, during and after difficult tracheal
intubation. What do you think about other colleagues’ feelings who were
present? What did others feel about your actions? Why?
Evaluation:
What were the positive and negative steps? Why? Did the team work
well or not? Why? How other colleagues would have managed the problem? Why?
Analysis:
Was the pre-operative airway assessment adequate? Were all preparations made for
airway management? What are the current difficult airway management
guidelines? Was the patient’s airway management performed according to the
difficult airway management guidelines? What are the learning points?
Conclusion:
What will you approach differently? Are there gaps in the
knowledge, skills and attitude for difficult airway management?
Action plan:
To discuss and review the case with the airway lead of
the department and act on his feedback. To write a critical incident using a
local reporting system. To present the case in the departmental morbidity and
mortality meeting. Review difficult airway management trolley availability in
operating and other areas of anaesthesia services.
Limited studies evaluate the effectiveness of reflection models and their impact on learning or clinical performance and outcomes in anaesthesia. In addition, models or reflection processes are often integrated for performance assessment and feedback [31]. Reflection is helpful before (e.g., reflection on the logbook before job planning) or during the experience. Schon’s model includes reflection-in-action (RiA), in which thinking during the task is accomplished for continuous learning and self-monitoring [25]. It allows learners to make adjustments and modifications for meaningful decisions and discussions. In primary care, RiA reduces stress and burnout in primary care by enhancing the clinicians’s ability to self-monitor during practice and improving empathy and psycho-social orientation [32].
Educational and clinical supervisors have a crucial role during various stages of reflection, e.g., analysing the student’s knowledge and supporting an action plan. As a supervisor/mentor, to operationalise reflection, questions, challenges and non-judgemental comments should be framed to engage learners. Guidance from the curriculum, professional standards, evidence-based studies and institutional policies are common references to analyse learning experiences (Figure 1). As a learner or teacher, several skills are salient for reflection to be effective, including communication, active listening, teamwork, framing and the ability to give and receive constructive feedback [33].
Furthermore, context-specific reflection and complex situations may demand the ability to inquire, probe and challenge, e.g., to learn from a life-threatening complication [34]. In contrast to a rigid framework-based reflection, Cronix and Veen [35] emphasised using models pragmatically and according to a personal learning style rather than any specific model implemented by an organisation.
3.2. Depth of Reflection
Terms such as descriptive (provides information of events), dialogic or analytic (includes reason and evaluation of events and change for plan) and critical reflection are often used to underline the level of reflection. In addition to descriptive and dialogic reflection, developing skills for critical reflection is desirable [4,26,34]. Critical reflection encourages critical thinking and framing situations in different ways [34,36]. Therefore, the essential objective of reflection is transformational learning so that future actions are adequate and appropriate [36].
The critical reflection considers questions in broader breadth and depth and adopts a comprehensive approach to meaning [20]. It accomplishes open-minded analysis from multiple perspectives and cognitive and affective responses to the observed reality [8]. Therefore, critical reflection is essential to achieve higher professional competency, develop resilience and promote well-being [33]. During critical reflection, ethical, historical, cultural and political values or beliefs are contemplated in evaluating personal or professional matters [37]. The learner can deconstruct the events and experiences by questioning their assumptions and analysis [34].
3.3. Documentation
Although not necessary, using a model of reflective writing tools can facilitate reflective writing [38]. Reflective writing explores the reasons for what happened, elaborates on the self and the actions of others and evaluates the outcome from various perspectives [39]. The reflector expresses feelings and emotions and critically examines reasons to make sense of the situations. It is vital to elucidate what could have been approached differently, what is required to obtain new knowledge and skills and to act differently for future similar episodes [1,7,39].
Although there is no single way to reflect, reflection documentation should be correct and prompt following learning activities because, with time, memory fades, and critical thinking about crucial aspects of the experience may happen if it is completed on time. Documentation of reflection on learning activities has become mandatory for all medical specialties, including anaesthesia, in the UK [1,7]. In the UK, for anaesthesia, reflection documentation is mainly within the RCOA-managed online portfolio for trainees and the organisation-provided appraisal system for clinical anaesthetists.
Reflective notes, journals, logs, blogs, questionnaires, diaries and essays foster reflective learning [10]. Reflective notes can be assessed as evidence of thinking, judgements and development. A court of law can require reflective notes depending on the local legal rules; accordingly, such notes should focus on learning rather than a whole discussion of the case or situation [40]. If the writing is assessed, the confidentiality of the patients, other individuals and the reflector should be maintained.
3.4. Blending with Other Learning Methods
Structural teaching programs within which reflective learning and process are being encouraged are essential [41]. Conceptually, reflection fundamentally should align with an individual’s learning style, and the climate for learning should be conducive to reflection [34,35]. Reflection is a crucial stage in experiential learning, during which the learner reviews the experience to make sense of and formulate future action plans [23]. During problem-based learning (PBL), the teacher facilitates reflection to focus and deepen the understanding of crucial aspects of the problem being learned. PBL provides space (e.g., classrooms or web-based spaces) to reflect in a comfortable environment and facilitates the development of critical skills valuable for group reflection, such as communication and collaborative working [10]. One frequently suggested approach is self-directed learning for adult education. Reflection nurtures self-directed learning to gain transformative knowledge [11,12,42]. During simulation-based teaching, reflection is essential for learning advanced anaesthesia skills and analysing their performance [14,43], e.g., anaesthesia machine checks, problem-solving and decision-making for a complex airway scenario. However, active participation and engagement from students are necessary to achieve the desired benefits of reflection [14,15].
4. Pitfalls: Practical and Theoretical
4.1. Meaning, Definition and Research
There are several definitions, meanings and models of reflection in the literature, which novice residents and inexperienced teachers may need help to conceptualise [44]. There is no generally accepted definition in the underlying theory and practice differences. Therefore, operationalising reflection is challenging from several aspects, including its integration into the curriculum, its standardisation for its assessment and the evaluation of its impact on learning outcomes [6]. The literature reviewed for this article suggests considerable variability in reflection in education and clinical practice. If reflection is essential, how best can it be implemented and facilitated in anaesthesia for its effectiveness? What are likely barriers to reflective practice in anaesthesia? To what extent does reflective practice impact anaesthesia practice and its related outcomes? These questions largely need to be answered. It is also vital to be aware of barriers and facilitators of reflection to improve its role in daily practice in anaesthesia [45,46].
4.2. Individual and Organisational
Honest speaking, listening and writing of experiences and events are essential for genuine reflective outcomes [34]. Worrying about self-weakness, self-ignorance, self-blame or self-guilt during reflection may prevent true reflection. Empathy, no-blame culture, peer support and mutual respect may avoid such fears and feelings of reflective practitioners [6,47]. These factors are relevant to the complex, competitive, diverse and demanding working conditions encountered by anaesthetists in operating rooms and clinics. If reflection is considered only a tick-box exercise and critical analysis and genuine introspection are not conducted, the value of the reflection learning tool is weakened. It may create a bias towards self-capability and self-confidence [35].
Lack of time may lead to the underutilisation of reflective learning [48]. Meaningful reflection requires time and space to think, understand and reconstruct knowledge. The macro context (political, social, cultural, professional bodies) and micro context (local ‘space’ to reflect in, e.g., teacher and learner power, communication, openness) may inhibit each other while reflecting [34]. Critical reflection may challenge existing practices and question power relations, which may not be acceptable to peers, supervisors or organisations.
Table 3 summarises individual and organizational factors which may hinder the reflection process.
Table 3.
Barriers to reflective learning and practice.
4.3. Assessment
To assess reflection or the lack of it in medical education is controversial. Some scholars argue that reflection is subjective; any categorisation may devalue its purpose and cause strategic ‘pseudo-reflection’ among students to align reflection with the assessment criteria [8,35]. There are risks of rationalising reflection and removing its philosophical underpinnings in pursuit of measurement and assessing its impact on learning or clinical outcomes [25]. However, some authors have expressed concerns that it may be inaccurate and inappropriate if self-reflection is associated with only self-assessment [9].
Reflection assessment is complex and challenging for several reasons, including a need for valid, reliable and reproducible tools [10,49]. No agreed standards or protocols exist for reliable and accurate assessment because of wide-ranging confounding factors, including the number of tools available [50,51]. In one study evaluating 34 reflection assessment tools identified, 11 components of reflection, but none encompassed all elements [52]. The authors suggested that the context surrounding evaluation should be carefully considered when choosing an evaluation tool for reflection. Manual assessment of reflective writing is time-consuming and may affect teacher–student relations [50]. Machine-learning-based tools may be available to assess the contents and depth of reflection, providing a scalable and immediate assessment [53]. However, language indicators for anaesthesia are unavailable for machine-learning-based assessment.
4.4. Teaching Reflection
Although reflective practice is now well founded in the medical discipline, the structural integration of teaching reflection is not prevalent in medical education, possibly due to theoretical vs. practical contradictions [54]. Reflection skills can be developed to evolve oneself from being a passive learner into an intellectual and logical reflective practitioner [55]. Teaching reflection to anaesthesia residents or other healthcare professionals requires theoretical knowledge of models, acquiring the skills needed for effective reflection, highlighting the value of reflection exercises and discussing evidence of reflection in improving the quality and safety of patient care and its impact on the well-being of individuals. However, teaching reflection, especially high-order reflection such as critical reflection, is practically challenging because individual, situational and contextual factors and their interpretations by learners vary [37,52].
5. Promoting Learning Using Reflection
Supervisors are key to the development of reflective practice [56]. Reflective activity should be learner-centred, leading to learning outcomes such as gaining competency and keeping patients at the centre [1,7]. The facilitator and learner should demonstrate the necessary qualities to foster reflective collaboration (Table 4). Interest and enthusiasm from both the teacher and learner are essential for adopting reflection as a medium for education. A step-wise introduction (e.g., superficial to deep) may increase the success of the reflective process [41]. Chaffey et al., found limited empirical evidence of effective facilitation methods for reflection [12]. One meta-analysis highlighted sustained reflection for specific learning situations, collective reflection (e.g., role play in classrooms, expressing self-positioning during online discussions) and a diverse approach rather than rigid adherence to one format as cornerstones of reflection to gain positive effects and be productive [57].
Table 4.
Characteristics of an ideal reflective learner and practitioner.
Rudolph and colleagues highlighted the importance of various debriefing methods (judgemental, non-judgemental and debriefing with good judgment) to improve reflective practice and performance during high-fidelity simulation-based learning [58]. Feedback and reflection have the potential to complement each other [31]. Feedback also promotes reflecting from multiple perspectives. However, in-depth qualitative studies are necessary to analyse the effects of various types of feedback (e.g., affective, suggestive or corrective) on the outcome of reflection [57].
5.1. Individual Support
Observation of practical peer reflective group discussions may motivate, improve engagement and provide developmental opportunities at an individual level [21]. Workshops to enhance awareness and the application of reflective skills may overcome some obstacles. Videos have been found to enhance reflection and aid student-led and critical reflection, which can be viewed on easy-to-use portable devices for analysis [59]. Watching your own videos may provide a different perspective to reflect on your behaviour, communication skills and interactions with others, e.g., students and colleagues. Collaborative approaches (e.g., group reflection) within a professional team may link individual concerns to team concerns and provide psychological safety [60].
5.2. Role of Organisation
Ground rules, boundaries of practice, ethical considerations, awareness of learners’ and teachers’ power and limitations, trust and framing as per the discipline are likely to promote context-specific reflection [34]. Guidelines, coaching of students/staff and mechanisms for accurate feedback are also expected to improve reflective skills [41]. The reflective process should be integrated into routine workplace-based assessments and broader educational and professional portfolios [1,7].
5.3. Role of Supervisor and Mentor
A facilitator (e.g., an educational or clinical supervisor in anaesthesia) can provide the necessary supportive environment to enable an individual to notice and make sense of their experiences [57]. Supervisors should stress the value of true reflection rather than superficial or strategic exercises to satisfy periodic review and appraisal requirements [56]. Depending on sensitivity, attention to the physical environment is also important, ensuring the that the discussion can occur in privacy and is free from interruption.
The facilitator should clarify the learning objectives, embrace different perspectives (e.g., variation in learning methods of residents), encourage constructive dialogue and help learners understand reflection [6,10,21,46,48,57]. Experienced teachers or supervisors identify performance gaps, provide constructive feedback to their trainees or supervisees and balance their reflection to achieve competency [61]. The facilitator can provide support through key counselling and mentoring skills, such as non-judgmental questioning and accepting divergent views. The facilitator has an important role in group teaching, including moderating conversations rationally, cultivating a blame-free and fear-free environment, addressing disagreements sensitively and maintaining an open and empathetic approach towards learners [21]. While a supervisor should consider multiple perspectives of learners, it is also essential to guide reflection and encourage conversations by probing assumptions and challenging biases for critical reflection.
6. Limitations
The primary limitation is the scant literature on reflection and its applicability to various domains of anaesthesia, including training, teaching and practice. Reflective literature is primarily qualitative and therefore includes inherent limitations such as difficulty in its duplication, evaluation and generalisation. Further high-quality research is essential for reflection and its impact on various aspects of anaesthesia education and professional practice. Meanwhile, in anaesthesia, using reflection for teaching and clinical activities depends on understanding the concepts and findings from other relevant literature.
7. Conclusions
Reflection is mandatory for lifelong learning and professional development in anaesthesia education and practice. Although there is no robust evidence of it in anaesthesia, it will likely facilitate objective and outcome-oriented learning and guide purposeful planning for future learning experiences. It should be incorporated with other learning and teaching methods for individual or group reflection. Critical reflection considers wider contexts for deep self-assessment and situational assessment. It has the power and potential to change attitudes, beliefs and behaviours and find psychosocial solutions to complex problems. Understanding the factors influencing the reflection process and knowledge of models for reflection is important for its purposeful application. Mentoring, communication and feedback facilitate reflection. Objective assessment of reflective learning is complex due to several personal and professional confounding factors.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ime2040025/s1.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The author declares no conflict of interest.
References
- General Medical Council. Available online: https://www.gmc-uk.org/education/standards-guidance-and-curricula/guidance/reflective-practice (accessed on 1 May 2023).
- Sandars, J. The use of reflection in medical education: AMEE Guide No. 44. Med. Teach. 2009, 31, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Branch, W.T., Jr. The road to professionalism: Reflective practice and reflective learning. Patient Educ. Couns. 2010, 80, 327–332. [Google Scholar] [CrossRef]
- Smith, E. Teaching critical reflection. Teach. High. Edu. 2011, 16, 211–223. [Google Scholar] [CrossRef]
- Bjerkvik, L.K.; Hilli, Y. Reflective writing in undergraduate clinical nursing education: A literature review. Nurse Educ. Pract. 2019, 35, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.V.; Jill, G.; MacLeod, A. Reflection and reflective practice in health professions education: A systematic review. Adv. Health Sci. Educ. 2009, 14, 595–621. [Google Scholar] [CrossRef]
- Academy of Medical Royal Colleges. Available online: www.aomrc.org.uk/wp-content/uploads/2018/09/Reflective_Practice_Toolkit_AoMRC_CoPMED_0818.pdf (accessed on 1 May 2023).
- Aronson, L. Twelve tips for teaching reflection at all levels of medical education. Med. Teach. 2011, 33, 200–205. [Google Scholar] [CrossRef]
- Ng, S.L.; Kinsella, E.A.; Friesen, F.; Hodges, B. Reclaiming a theoretical orientation to reflection in medical education research: A critical narrative review. Med. Educ. 2015, 49, 461–475. [Google Scholar] [CrossRef]
- Fragkos, K.C. Reflective Practice in Healthcare Education: An Umbrella Review. Educ. Sci. 2016, 6, 27. [Google Scholar] [CrossRef]
- Winkel, A.F.; Yingling, S.; Jones, A.A.; Nicholson, J. Reflection as a learning tool in graduate medical education: A systematic review. J. Grad. Med. Educ. 2017, 4, 430–439. [Google Scholar] [CrossRef]
- Chaffey, L.J.; de Leeuw, E.J.; Finnigan, G.A. Facilitating Students’ Reflective Practice in a Medical Course: Literature Review. Edu. Health 2012, 25, 198–203. [Google Scholar] [CrossRef]
- Mamede, S.; Schmidt, H.G.; Penaforte, J.C. Effects of reflective practice on the accuracy of medical diagnoses. Med. Educ. 2008, 42, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Fanning, R.M.; Gaba, D.M. The role of debriefing in simulation-based learning. Simul. Healthc. 2007, 2, 115–125. [Google Scholar] [CrossRef]
- Lee, J.Y.; Donkers, J.; Jarodzka, H.; Sellenraad, G.; Faber, T.J.; van Merriënboer, J.J. The Effects of reflective pauses on performance in simulation training. Simul. Healthc. 2023; published ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Arriaga, A.F.; Sweeney, R.E.; Clapp, J.T.; Clapp, J.T.; Muralidharan, M.; Burson, R.C.; Gordon, E.K.; Falk, S.A.; Baranov, D.Y.; Fleisher, L.A. Failure to debrief after critical events in anesthesia is associated with failures in communication during the event. Anesthesiology 2019, 130, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Knapp, S.; Gottlieb, M.C.; Handelsman, M.M. Enhancing professionalism through self-reflection. Prof. Psychol. Res. Pract. 2017, 48, 167. [Google Scholar] [CrossRef]
- Koole, S.; Dornan, T.; Aper, L.; Scherpbier, A.; Valcke, M.; Cohen-Schotanus, J.; Derese, A. Factors confounding the assessment of reflection: A critical review. BMC Med. Educ. 2011, 11, 104. [Google Scholar] [CrossRef]
- Hargreaves, K. Reflection in medical education. J. Univ. Teach. Learn. Pract. 2016, 13, 6. [Google Scholar] [CrossRef]
- Schei, E.; Fuks, A.; Boudreau, J.D. Reflection in medical education: Intellectual humility, discovery, and know-how. Med. Health Care Philos 2019, 22, 167–178. [Google Scholar] [CrossRef]
- Marshall, T.; Keville, S.; Cain, A.; Adler, J.R. Facilitating reflection: A review and synthesis of the factors enabling effective facilitation of reflective practice. Reflective Pract. 2022, 23, 483–496. [Google Scholar] [CrossRef]
- Ménard, L.; Ratnapalan, S. Reflection in medicine: Models and application. Can. Family Phy. 2013, 59, 105–107. [Google Scholar]
- Thomas, H.M. Experiential learning—A systematic review and revision of Kolb’s model. Interact. Learn. Environ. 2020, 28, 1064–1077. [Google Scholar]
- Gibbs, G. Case studies of the application of experiential learning methods. In Gibbes G Learning by Doing; Oxford Brooks University: Oxford, UK, 2013; pp. 66–111. [Google Scholar]
- Schon, D.A. The Reflective Practitioner: How Professionals Think in Action; Basic Books: New York, NY, USA, 1983. [Google Scholar]
- Hatton, N.; Smith, D. Reflection in teacher education: Towards definition and implementation. Teach. Teach. Educ. 1995, 11, 33–49. [Google Scholar] [CrossRef]
- Bain, J.D.; Ballantyne, R.; Packer, J.; Mills, C. Using journal writing to enhance student teachers’ reflectivity during field experience placements. Teach. Teach. 1999, 5, 51–73. [Google Scholar] [CrossRef]
- Moon, J. A Handbook of Reflective and Experiential Learning; Routledge: London, UK, 1999. [Google Scholar]
- Johns, C. Engaging Reflection in Practice: A Narrative Approach; Wiley-Blackwell: West Sussex, UK, 2006. [Google Scholar]
- Driscoll, J.; Teh, B. The potential of reflective practice to develop individual orthopaedic nurse practitioners and their practice. J. Ortho Nurse. 2001, 5, 95–103. [Google Scholar] [CrossRef]
- Sargeant, J.; Mann, K.V.; Van der Vleuten, C.P.; Metsemakers, J.F. Reflection: A link between receiving and using assessment feedback. Adv. Health Sci. Educ. 2009, 14, 399–410. [Google Scholar] [CrossRef]
- Epstein, R.M.; Siegel, D.; Silberman, J. Self-monitoring in clinical practice: A challenge for medical educators. J. Contin. Educ. Health Prof. 2008, 28, 5–13. [Google Scholar] [CrossRef]
- Raelin, J. “I don’t have time to think!” versus the art of reflective practice. Reflections 2002, 4, 66–79. [Google Scholar] [CrossRef]
- Boud, D.; Walker, D. Promoting reflection in professional courses: The challenge of context. Studies High. Educ. 1998, 23, 191–206. [Google Scholar] [CrossRef]
- De la Croix, A.; Veen, M. The reflective zombie: Problematizing the conceptual framework of reflection in medical education. Perspect. Med. Educ. 2018, 7, 394–400. [Google Scholar] [CrossRef]
- DunnGalvin, A.; Cooper, J.B.; Shorten, G.; Blum, R.H. Applied reflective practice in medicine and anaesthesiology. Bri. J. Anaesth. 2019, 122, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Smyth, J. Developing and sustaining critical reflection in teacher education. J. Teachr. Educ. 1989, 40, 2–9. [Google Scholar] [CrossRef]
- Lim, J.Y.; Ong, S.Y.; Ng, C.Y.; Chan, K.L.; Wu, S.Y.; So, W.Z.; Tey, G.J.; Lam, Y.X.; Gao, N.L.; Lim, Y.X.; et al. A systematic scoping review of reflective writing in medical education. BMC Med. Educ. 2023, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Koshy, K.; Limb, C.; Gundogan, B.; Whitehurst, K.; Jafree, D.J. Reflective practice in health care and how to reflect effectively. Int. J. Sur. Oncol. 2017, 2, e2037. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.; Kumar, B. Clinical reflective practice. Obstet. Gynaecol. 2020, 22, 75–82. [Google Scholar] [CrossRef]
- Uygur, J.; Stuart, E.; De Paor, M.; Wallace, E.; Duffy, S.; O’Shea, M.; Smith, S.; Pawlikowska, T. Best Evidence in Medical Education systematic review to determine the most effective teaching methods that develop reflection in medical students: BEME Guide No. 51. Med. Teach. 2019, 41, 3–16. [Google Scholar] [CrossRef]
- Loeng, S. Self-directed learning: A core concept in adult education. Educ. Res. Int. 2020, 2020, 3816132. [Google Scholar] [CrossRef]
- Chernikova, O.; Heitzmann, N.; Stadler, M.; Holzberger, D.; Seidel, T.; Fischer, F. Simulation-based learning in higher education: A meta-analysis. Rev. Educ. Res. 2020, 90, 499–541. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Fernandez, N.; Karsenti, T.; Charlin, B. What is reflection? A conceptual analysis of major definitions and a proposal of a five-component model. Med. Educ. 2014, 48, 1176–1189. [Google Scholar] [CrossRef]
- Goy, R.W.; Lee, J.S.; Ithnin, F.; Sng, B.L. Current state of reflective learning in anaesthesiology residents: A call for ‘reflection-on-action’ training in Singapore. Sing Med. J. 2022, 63, 319–324. [Google Scholar] [CrossRef]
- Gathu, C. Facilitators and barriers of reflective learning in postgraduate medical education: A narrative review. J. Med. Educ. Curric. Dev. 2022, 9, 23821205221096106. [Google Scholar] [CrossRef]
- Bolton, G.; Delderfield, R. Reflective Practice: Writing and Professional Development, 5th ed.; SAGE Publications Ltd.: London, UK, 2018. [Google Scholar]
- Caldwell, L.; Grobbel, C. Importance of reflection in nursing practice. Int. J. Caring Nurses 2013, 6, 319–326. [Google Scholar]
- Chan, C.K.; Lee, K.K. Reflection literacy: A multilevel perspective on the challenges of using reflections in higher education through a comprehensive literature review. Educ. Res. Rev. 2021, 32, 100376. [Google Scholar] [CrossRef]
- Hays, R.; Gay, S. Reflection or ‘pre-reflection’: What are we actually measuring in reflective practice? Med. Educ. 2011, 45, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Ooi, S.M.; Fisher, P.; Coker, S. A systematic review of reflective practice questionnaires and scales for healthcare professionals: A narrative synthesis. Reflect. Pract. 2021, 22, 1–5. [Google Scholar] [CrossRef]
- Préfontaine, C.; Gaboury, I.; Corriveau, H.; Beauchamp, J.; Lemire, C.; April, M.J. Assessment tools for reflection in healthcare learners: A scoping review. Med. Teach. 2022, 44, 394–400. [Google Scholar] [CrossRef]
- Ullmann, T.D. Automated analysis of reflection in writing: Validating machine learning approaches. Int. J. Artif. Intelli Educ. 2019, 29, 217–257. [Google Scholar] [CrossRef]
- Schaepkens, S.P.; Veen, M.; de la Croix, A. Is reflection like soap? a critical narrative umbrella review of approaches to reflection in medical education research. Adv. Health Sci. Educ. 2022, 27, 537–551. [Google Scholar] [CrossRef]
- Husu, J.; Toom, A.; Patrikainen, S. Guided reflection as a means to demonstrate and develop student teachers’ reflective competencies. Reflect. Pract. 2008, 9, 37–51. [Google Scholar] [CrossRef]
- Academy of Medical Royal Colleges. Available online: www.aomrc.org.uk/wp-content/uploads/2019/06/Facilitating_reflection_0619.pdf (accessed on 1 May 2023).
- Guo, L. How should reflection be supported in higher education?—A meta-analysis of reflection interventions. Reflect. Pract. 2022, 23, 118–146. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Simon, R.; Rivard, P.; Dufresne, R.L.; Raemer, D.B. Debriefing with good judgment: Combining rigorous feedback with genuine inquiry. Anesthesiol. Clin. 2007, 25, 361–376. [Google Scholar] [CrossRef]
- Körkkö, M. Towards meaningful reflection and a holistic approach: Creating a reflection framework in teacher education. Scand. J. Educ. Res. 2021, 65, 258–275. [Google Scholar]
- Bindels, E.; Verberg, C.; Scherpbier, A.; Heeneman, S.; Lombarts, K. Reflection revisited: How physicians conceptualize and experience reflection in professional practice—A qualitative study. BMC Med. Edu. 2018, 18, 105. [Google Scholar] [CrossRef] [PubMed]
- Weller, J.; Gotian, R. Evolution of the feedback conversation in anaesthesia education: A narrative review. Br. J. Anaesth. 2023, 131, 503–509. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).