
Non-Cardiac Depolarization-Blocking Drugs Are Associated with Increased Risk of Out-of-Hospital Cardiac Arrest in the Community

 ,
,
Abstract
1. Introduction
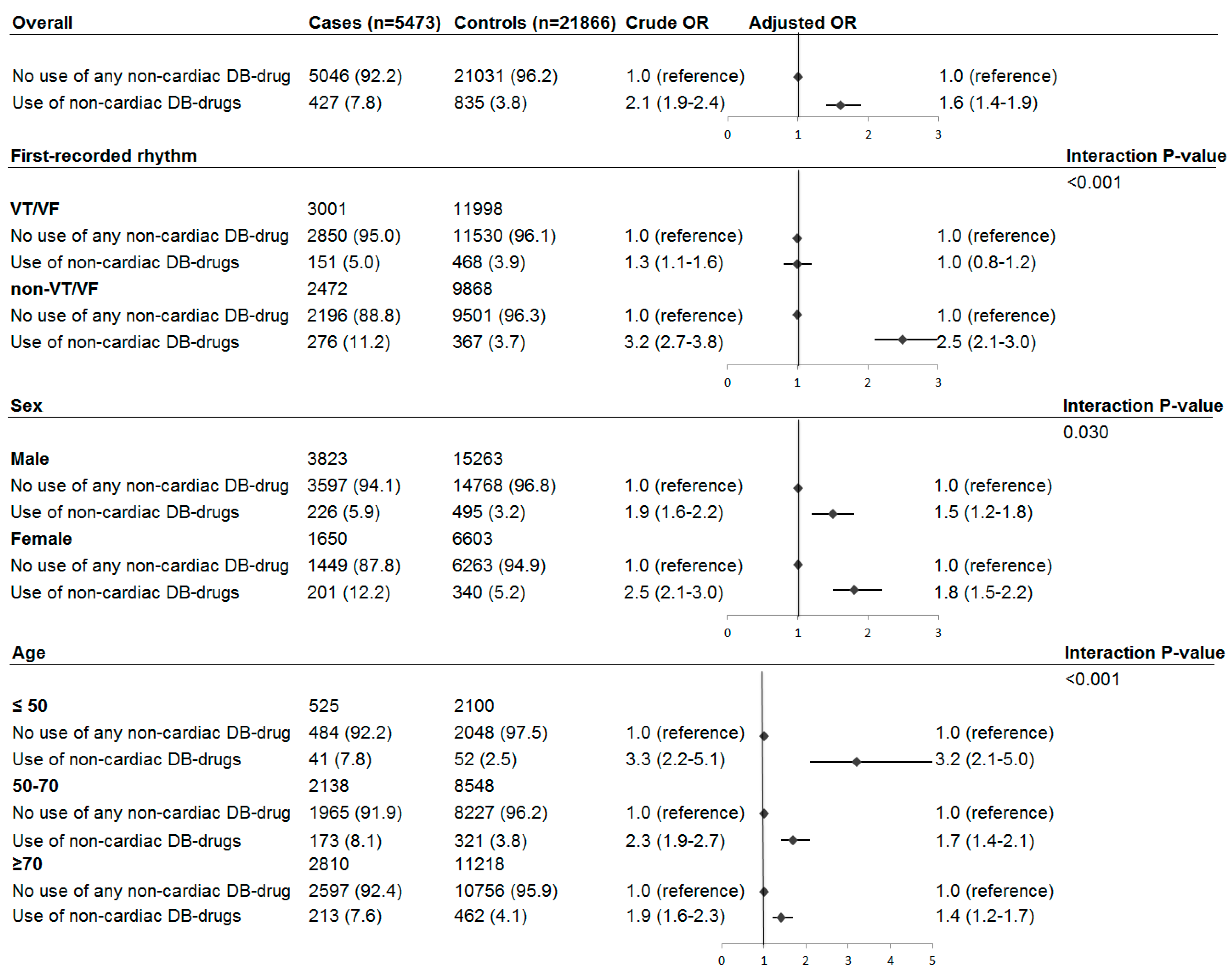
2. Results
3. Discussion
3.1. Previous Studies
3.2. Stratified Analyses
3.3. Strengths and Limitations
4. Materials and Methods
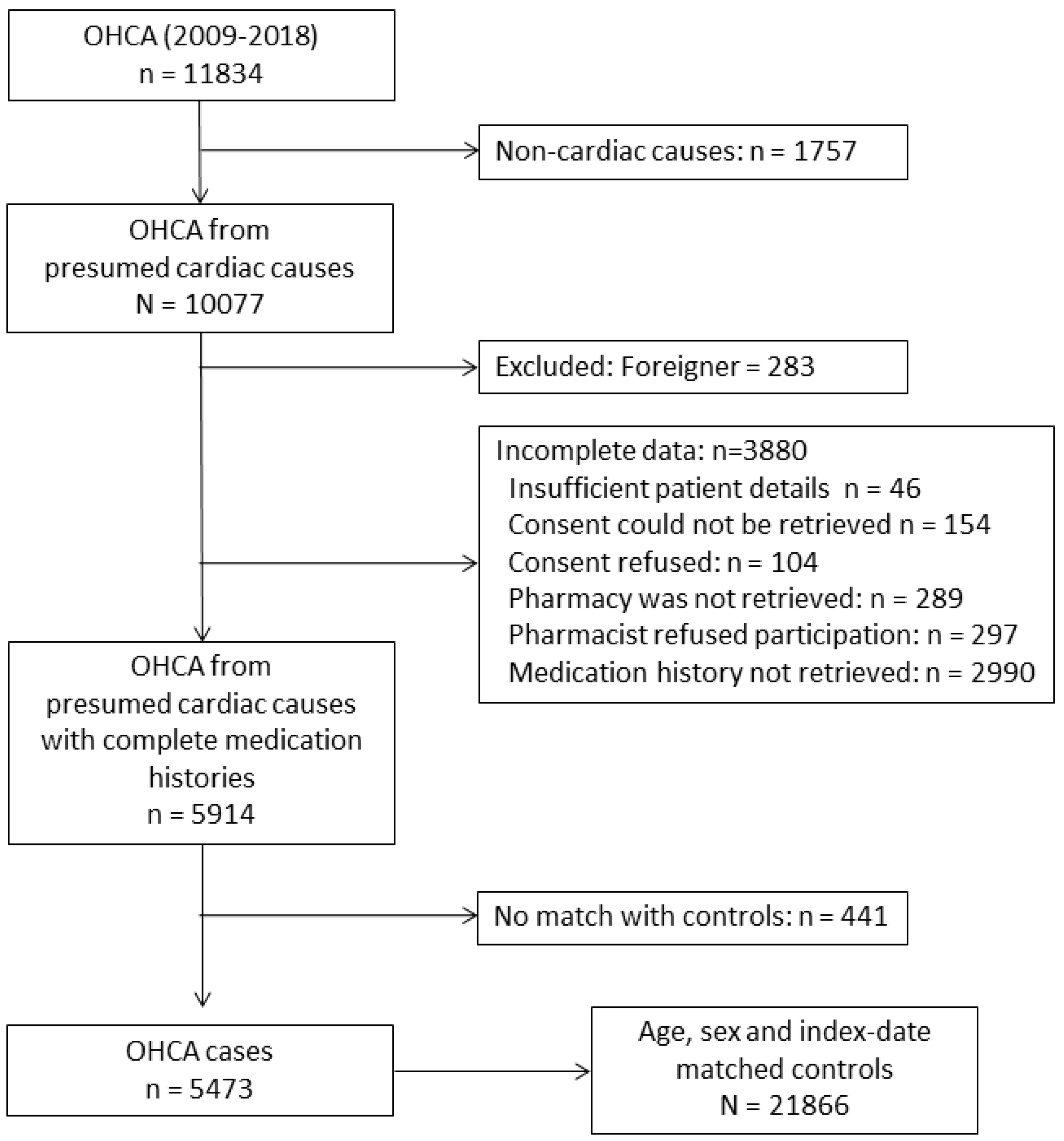
4.1. Study Design and Setting
4.2. Data Collection
4.3. Exposure of Interest and Covariates
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.P.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J.; Castellanos, A. Cardiac arrest and sudden cardiac death. In Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine; Libby, P., Bonow, R.O., Mann, D.L., Zipes, D.P., Eds.; Elsevier: Oxford, UK, 2007; pp. 933–974. [Google Scholar]
- Huikuri, H.V.; Castellanos, A.; Myerburg, R.J. Sudden death due to cardiac arrhythmias. N. Engl. J. Med. 2001, 345, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Tomaselli, G.F.; Zipes, D.P. What causes sudden death in heart failure? Circ. Res. 2004, 95, 754–763. [Google Scholar] [CrossRef]
- Roden, D.M. Drug-induced prolongation of the QT interval. N. Engl. J. Med. 2004, 350, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Waldo, A.L.; Camm, A.J.; Deruyter, H.; Friedman, P.L.; MacNeil, D.J.; Pauls, J.F.; Pitt, B.; Pratt, C.M.; Schwartz, P.J.; Veltri, E.P. Effect of d-sotalol on mortality in patients with left ventricular dysfunction after recent and remote myocardial infarction. Lancet 1996, 348, 7–12. [Google Scholar] [CrossRef]
- Straus, S.M.; Sturkenboom, M.C.; Bleumink, G.S.; Dieleman, J.P.; Van Der Lei, J.; De Graeff, P.A.; Kingma, J.H.; Stricker, B.H. Non-cardiac QTc-prolonging drugs and the risk of sudden cardiac death. Eur. Heart J. 2005, 26, 2007–2012. [Google Scholar] [CrossRef]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Hall, K.; Stein, C.M. Atypical antipsychotic drugs and the risk of sudden cardiac death. N. Engl. J. Med. 2009, 360, 225–235. [Google Scholar] [CrossRef]
- Cheng, Y.-J.; Nie, X.-Y.; Chen, X.-M.; Lin, X.-X.; Tang, K.; Zeng, W.-T.; Mei, W.-Y.; Liu, L.-J.; Long, M.; Yao, F.-J.; et al. The role of macrolide antibiotics in increasing cardiovascular risk. J. Am. Coll. Cardiol. 2015, 66, 2173–2184. [Google Scholar] [CrossRef]
- Weeke, P.; Jensen, A.; Folke, F.; Gislason, G.; Olesen, J.; Andersson, C.; Fosbøl, E.L.; Larsen, J.K.; Lippert, F.K.; Nielsen, S.L.; et al. Antidepressant Use and Risk of Out-of-Hospital Cardiac Arrest: A Nationwide Case–Time–Control Study. Clin. Pharmacol. Ther. 2012, 92, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Weeke, P.; Jensen, A.; Folke, F.; Gislason, G.H.; Olesen, J.B.; Fosbøl, E.; Wissenberg, M.; Lippert, F.K.; Christensen, E.F.; Nielsen, S.L.; et al. Antipsychotics and Associated Risk of Out-of-Hospital Cardiac Arrest. Clin. Pharmacol. Ther. 2014, 96, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Tsai, Y.T.; Tsai, H.J. Antipsychotic drugs and the risk of ventricular arrhythmia and/or sudden cardiac death: A nation-wide case-crossover study. J. Am. Heart Assoc. 2015, 4, e001568. [Google Scholar] [CrossRef] [PubMed]
- Echt, D.S.; Liebson, P.R.; Mitchell, L.B.; Peters, R.W.; Obias-Manno, D.; Barker, A.H.; Arensberg, D.; Baker, A.; Friedman, L.; Greene, H.L.; et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo: The Cardiac Arrhythmia Suppression Trial. N. Engl. J. Med. 1991, 324, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Bardai, A.; Amin, A.S.; Blom, M.T.; Bezzina, C.R.; Berdowski, J.; Langendijk, P.N.; Beekman, L.; Klemens, C.A.; Souverein, P.C.; Koster, R.W.; et al. Sudden cardiac arrest associated with use of a non-cardiac drug that reduces cardiac excitability: Evidence from bench, bedside, and community. Eur. Heart J. 2013, 34, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Bardai, A.; Blom, M.T.; van Noord, C.; Verhamme, K.M.; Sturkenboom, M.C.; Tan, H.L. Sudden cardiac death is associated both with epilepsy and with use of antiepileptic medications. Heart 2015, 101, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Postema, P.G.; Wolpert, C.; Amin, A.S.; Probst, V.; Borggrefe, M.; Roden, D.M.; Priori, S.G.; Tan, H.L.; Hiraoka, M.; Brugada, J.; et al. Drugs and Brugada syndrome patients: Review of the literature, recommendations and an up-to-date website (www.brugadadrugs.org). Heart Rhythm. 2009, 6, 1335–1341. [Google Scholar] [CrossRef]
- Greenberg, H.M.; Dwyer, E.M.; Hochman, J.S.; Steinberg, J.S.; Echt, D.S.; Peters, R.W. Interaction of ischaemia and encainide/flecainide treatment: A proposed mechanism for the increased mortality in CAST I. Br. Heart J. 1995, 74, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Blom, M.T.; van Hoeijen, D.A.; Bardai, A.; Berdowski, J.; Souverein, P.C.; De Bruin, M.L.; Koster, R.W.; de Boer, A.; Tan, H.L. Genetic, clinical and pharmacological determinants of out-of-hospital cardiac arrest: Rationale and outline of the AmsteRdam Resuscitation Studies (ARREST) registry. Open Heart 2014, 1, e000112. [Google Scholar] [CrossRef]
- European Heart Rhythm Association (EHRA); Camm, A.J.; Kirchhof, P.; Lip, G.Y.; Schotten, U.; Savelieva, I.; Ernst, S.; Van Gelder, I.C.; Al-Attar, N.; Hindricks, G.; et al. Guidelines for the management of atrial fibrillation: The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur. Heart J. 2010, 12, 1360–1420. [Google Scholar]
- GIPdatabank. Zorginstituut Nederland. Available online: https://www.gipdatabank.nl (accessed on 2 March 2020).
- Lewer, D.; O’Reilly, C.; Mojtabai, R.; Evans-Lacko, S. Antidepressant use in 27 European countries: Associations with sociodemographic, cultural and economic factors. Br. J. Psychiatry 2015, 207, 221–226. [Google Scholar] [CrossRef]
- Yap, Y.G.; Behr, E.R.; Camm, A.J. Drug-induced Brugada syndrome. Europace 2009, 11, 989–994. [Google Scholar] [CrossRef]
- Risgaard, B.; Winkel, B.G.; Jabbari, R.; Lynge, T.H.; Wissenberg, M.; Glinge, C.; Haunsø, S.; Behr, E.R.; Fink-Jensen, A.; Gislason, G.H.; et al. Sudden Cardiac Death: Pharmacotherapy and Proarrhythmic Drugs: A Nationwide Cohort Study in Denmark. JACC Clin. Electrophysiol. 2017, 3, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Granfeldt, A.; Wissenberg, M.; Hansen, S.M.; Lippert, F.; Lang-Jensen, T.; Hendriksen, O.M.; Torp-Pedersen, C.; Christensen, E.F.; Christiansen, C. Clinical predictors of shockable versus non-shockable rhythms in patients with out-of-hospital cardiac arrest. Resuscitation 2016, 108, 40–47. [Google Scholar] [CrossRef]
- Bezzina, C.; Veldkamp, M.W.; Berg, M.P.V.D.; Postma, A.V.; Rook, M.B.; Viersma, J.-W.; van Langen, I.M.; Tan-Sindhunata, G.; Bink-Boelkens, M.T.E.; van der Hout, A.H.; et al. A single Na+ channel mutation causing both long-QT and Brugada syndromes. Circ. Res. 1999, 85, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.L.; Bink-Boelkens, M.T.; Bezzina, C.R.; Viswanathan, P.C.; Beaufort-Krol, G.C.; van Tintelen, P.J.; van den Berg, M.P.; Wilde, A.A.; Balser, J.R. A sodium-channel mutation causes isolated cardiac conduction disease. Nature 2001, 409, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Amin, A.S.; Tan, H.L.; Wilde, A.A. Cardiac ion channels in health and disease. Heart Rhythm 2010, 7, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Nademanee, K.; Veerakul, G.; Nimmannit, S.; Chaowakul, V.; Bhuripanyo, K.; Likittanasombat, K.; Tunsanga, K.; Kuasirikul, S.; Malasit, P.; Tansupasawadikul, S.; et al. Arrhythmogenic marker for the sudden unexplained death syndrome in Thai men. Circulation 1997, 96, 2595–2600. [Google Scholar] [CrossRef] [PubMed]
- Hermida, J.-S.; Lemoine, J.-L.; Aoun, F.B.; Jarry, G.; Rey, J.-L.; Quiret, J.-C. Prevalence of the Brugada syndrome in an apparently healthy population. Am. J. Cardiol. 2000, 86, 91–94. [Google Scholar] [CrossRef]
- Pham, T.V.; Robinson, R.B.; Danilo, P., Jr.; Rosen, M.R. Effects of gonadal steroids on gender-related differences in transmural dispersion of L-type calcium current. Cardiovasc. Res. 2002, 53, 752–762. [Google Scholar] [CrossRef][Green Version]
- Meregalli, P.G.; Wilde, A.A.; Tan, H.L. Pathophysiological mechanisms of Brugada syndrome: Depolarization disorder, repolarization disorder, or more? Cardiovasc. Res. 2005, 67, 367–378. [Google Scholar] [CrossRef]
- Nattel, S.; Maguy, A.; Le Bouter, S.; Yeh, Y.-H. Arrhythmogenic ion-channel remodeling in the heart: Heart failure, myocardial infarction, and atrial fibrillation. Physiol. Rev. 2007, 87, 425–456. [Google Scholar] [CrossRef]
- Tadros, R.; Tan, H.L.; ESCAPE-NET Investigators; El Mathari, S.; Kors, J.A.; Postema, P.G.; Lahrouchi, N.; Beekman, L.; Radivojkov-Blagojevic, M.; Amin, A.S.; et al. Predicting cardiac electrical response to sodium-channel blockade and Brugada syndrome using polygenic risk scores. Eur. Heart J. 2019, 40, 3097–3107. [Google Scholar] [CrossRef]
- Behzadi, M.; Joukar, S.; Beik, A. Opioids and Cardiac Arrhythmia: A Literature Review. Med. Princ. Pract. 2018, 27, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Keller, G.A.; Etchegoyen, M.C.V.; Fernandez, N.; Olivera, N.M.; Quiroga, P.N.; Belloso, W.H.; Diez, R.A.; Girolamo, G.D. Trmadol induced QTc-interval prolongation: Prevalence, clinical factors and correlation to plasma concentrations. Curr. Drug Saf. 2016, 11, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.B.; Sattiraju, S.; Bilden, E.F.; Asinger, R.W.; Bertog, S.C. Isolated tramadol overdose associated with Brugada ECG pattern. Pacing Clin. Electrophysiol. 2012, 35, e219–e221. [Google Scholar] [CrossRef]
- Izrailtyan, I.; Qiu, J.; Overdyk, F.J.; Erslon, M.; Gan, T.J. Risk factors for cardiopulmonary and respiratory arrest in medical and surgical hospital patients on opioid analgesics and sedatives. PLoS ONE 2018, 13, e0194553. [Google Scholar] [CrossRef]
- Eroglu, T.E.; Mohr, G.H.; Blom, M.T.; Verkerk, A.; Souverein, P.C.; Torp-Pedersen, C.; Folke, F.; Wissenberg, M.; Brink, L.V.D.; Davis, R.; et al. Differential effects on out-of-hospital cardiac arrest of dihydropyridines: Real-world data from population-based cohorts across two European countries. Eur. Heart J. Cardiovasc. Pharm. 2019, 6, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Herings, R.; Pedersen, L. Pharmacy-based Medical Record Linkage Systems. In Pharmacoepidemiology, 5th ed.; Strom, B., Kimmel, S., Eds.; John Wiley & Sons, Ltd.: Chichester, UK, 2012; pp. 270–286. [Google Scholar]
- Buurma, H.; Bouvy, M.L.; De Smet, P.A.G.M.; Floor-Schreudering, A.; Leufkens, H.G.M.; Egberts, A.C.G. Prevalence and determinants of pharmacy shopping behaviour. J. Clin. Pharm. 2008, 33, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Woosley, R.L.; Heise, C.W.; Gallo, T.; Tate, J.; Woosley, D.; Romero, K.A. QTdrugs List, AZCERT, Inc. Oro Valley, AZ, USA. Available online: https://www.CredibleMeds.org (accessed on 16 July 2020).



{kind=link}
{kind=link}
| OHCA Cases | Non-OHCA Controls | |
|---|---|---|
| Total | 5473 | 21,866 |
| Mean age, years (standard deviation) | 68.8 (14.0) | 68.8 (14.0) |
| Male sex | 3823 (69.9) | 15,263 (69.8) |
| Cardiovascular drugs | ||
| Beta blockers | 1998 (36.5) | 3839 (17.6) |
| Calcium channel blockers | 902 (16.5) | 2016 (9.2) |
| Antithrombotics | 2299 (42.0) | 4853 (22.2) |
| Diuretics | 1590 (29.1) | 2712 (12.4) |
| Renin-angiotensin system inhibitors | 2073 (37.9) | 4802 (22.0) |
| Nitrates | 574 (10.5) | 841 (3.9) |
| Statins | 1843 (33.7) | 4609 (21.1) |
| Antidiabetics | 936 (17.1) | 2145 (9.8) |
| Antiarrhythmic drugs Vaughan-Williams class I or III | 114 (2.1) | 183 (0.8) |
| OHCA Cases (n = 5473) | Non-OHCA Controls (n = 21,866) | Crude OR (95% CI) | Adjusted OR * (95% CI) | |
|---|---|---|---|---|
| No use of any non-cardiac, DB drugs | 5046 (92.2) | 21,031 (96.2) | 1.0 (reference) | 1.0 (reference) |
| Tramadol | 103 (1.9) | 172 (0.8) | 2.5 (1.9–3.2) | 1.7 (1.3–2.2) |
| Paroxetine | 63 (1.2) | 152 (0.7) | 1.7 (1.3–2.4) | 1.5 (1.1–2.1) |
| Amitriptyline | 59 (1.1) | 154 (0.7) | 1.6 (1.2–2.2) | 1.1 (0.8–1.6) |
| Metoclopramide | 63 (1.2) | 35 (0.2) | 7.4 (4.9–11.1) | 6.4 (4.2–10.0) |
| Carbamazepine | 28 (0.5) | 46 (0.2) | 2.5 (1.5–4.0) | 2.1 (1.3–3.4) |
| Nortryptiline | 16 (0.3) | 33 (0.2) | 2.1 (1.1–3.8) | 1.5 (0.8–2.8) |
| Clomipramine | 9 (0.2) | 33 (0.2) | 1.1 (0.5–2.3) | 0.8 (0.4–2.0) |
| Lithium | 7 (0.1) | 16 (0.1) | 1.8 (0.7–4.4) | 1.6 (0.7–4.1) |
| Fluoxetine | 6 (0.1) | 23 (0.1) | 1.1 (0.5–2.8) | 0.8 (0.3–2.0) |
| Fluvoxamine | 10 (0.2) | 18 (0.1) | 2.3 (1.0–5.0) | 1.6 (0.7–3.8) |
| Lamotrigine | 5 (0.1) | 10 (0.1) | 2.1 (0.7–6.0) | 2.1 (0.7–6.4) |
| Phenytoin | 9 (0.2) | 15 (0.1) | 2.5 (1.1–5.8) | 1.9 (0.8–4.6) |
| Use of Non-Cardiac DB Drugs (n = 427) | No Use of Any Non-Cardiac DB Drugs (n = 5046) | p-Value | Unknown | |
|---|---|---|---|---|
| OHCA at public place | 61 (14.3) | 1310 (26.0) | <0.001 | 9 (0.2) |
| Witnessed status | 0.009 | 47 (0.9) | ||
| Bystander-witnessed or emergency-medical-services-witnessed OHCA | 286 (68.1) | 3704 (74.0) | ||
| Unwitnessed OHCA | 134 (31.9) | 1302 (26.0) | ||
| Cardiopulmonary resuscitation status | 0.384 | 66 (1.2) | ||
| Cardiopulmonary resuscitation before arrival of emergency medical services | 297 (70.7) | 3625 (72.7) | ||
| No cardiopulmonary resuscitation performed | 123 (29.3) | 1362 (27.3) | ||
| Automated external defibrillator used | 200 (46.8) | 2557 (50.7) | 0.126 | 2 (<0.1) |
| Median call-to-defibrillator-connection time, min (IQR) | 9.5 (7.4–12.4) | 8.6 (6.6–11.2) | 0.001 | 409 (7.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eroglu, T.E.; Blom, M.T.; Souverein, P.C.; de Boer, A.; Tan, H.L. Non-Cardiac Depolarization-Blocking Drugs Are Associated with Increased Risk of Out-of-Hospital Cardiac Arrest in the Community. Pharmacoepidemiology 2022, 1, 64-75. https://doi.org/10.3390/pharma1020007
Eroglu TE, Blom MT, Souverein PC, de Boer A, Tan HL. Non-Cardiac Depolarization-Blocking Drugs Are Associated with Increased Risk of Out-of-Hospital Cardiac Arrest in the Community. Pharmacoepidemiology. 2022; 1(2):64-75. https://doi.org/10.3390/pharma1020007
Chicago/Turabian StyleEroglu, Talip E., Marieke T. Blom, Patrick C. Souverein, Anthonius de Boer, and Hanno L. Tan. 2022. "Non-Cardiac Depolarization-Blocking Drugs Are Associated with Increased Risk of Out-of-Hospital Cardiac Arrest in the Community" Pharmacoepidemiology 1, no. 2: 64-75. https://doi.org/10.3390/pharma1020007
APA StyleEroglu, T. E., Blom, M. T., Souverein, P. C., de Boer, A., & Tan, H. L. (2022). Non-Cardiac Depolarization-Blocking Drugs Are Associated with Increased Risk of Out-of-Hospital Cardiac Arrest in the Community. Pharmacoepidemiology, 1(2), 64-75. https://doi.org/10.3390/pharma1020007