
A Pilot Study on the Influence of Diaphragmatic Function on Iliopsoas Muscle Activity in Individuals with Chronic Ankle Instability

Abstract
1. Introduction
- (i)
- Iliopsoas activity between the affected (sprained) and contralateral (control) sides during maximal isometric hip flexion under three breath-holding conditions: end-expiration, end-inspiration, and intermediate state.
- (ii)
- The activity and torque output of the other hip flexor muscles (rectus femoris, sartorius, and tensor fasciae latae) were measured to determine whether a reduction in iliopsoas activity affected force production.
- (iii)
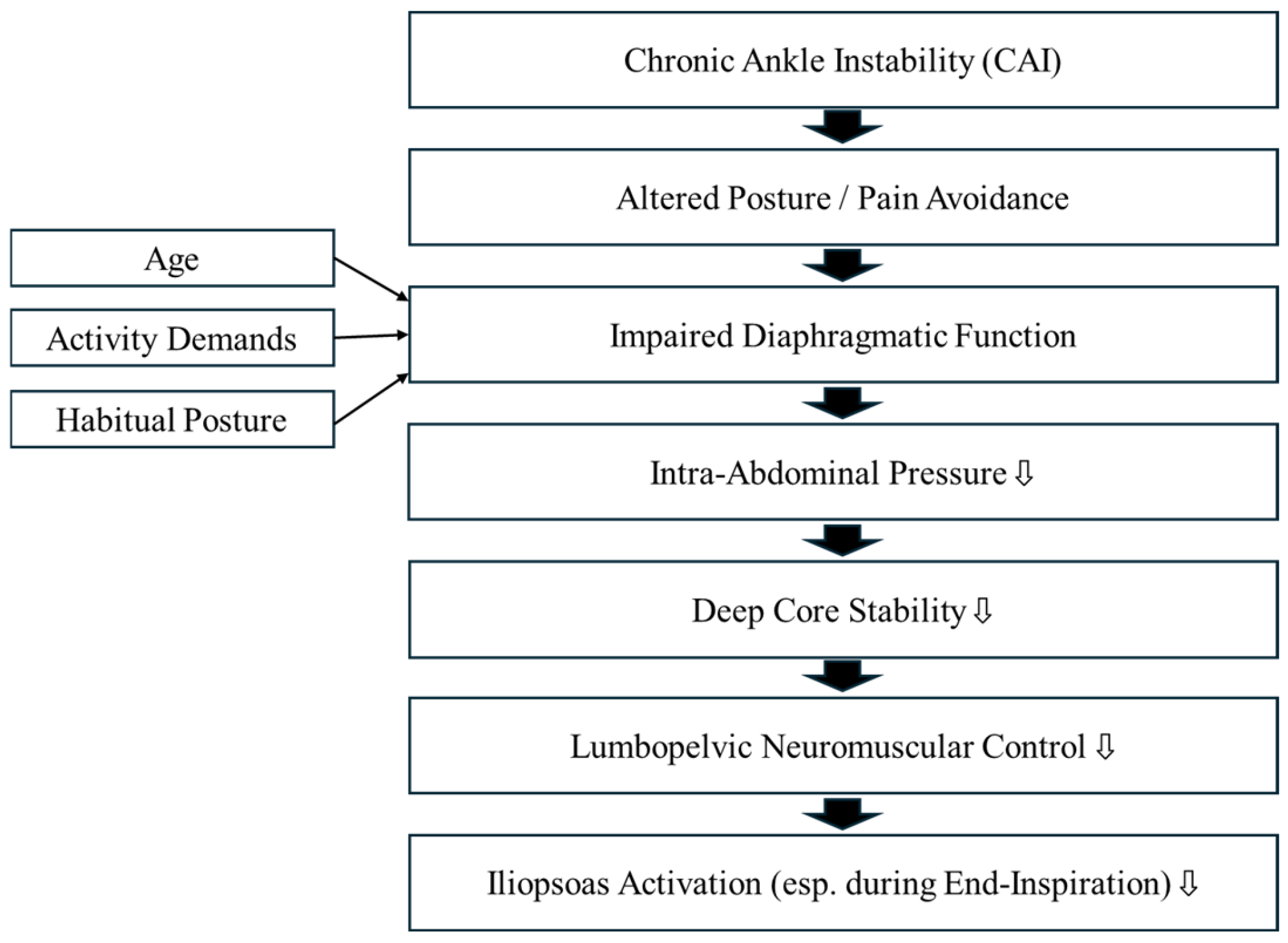
- Propose a comprehensive rehabilitation strategy for individuals with CAI based on these findings.
2. Results
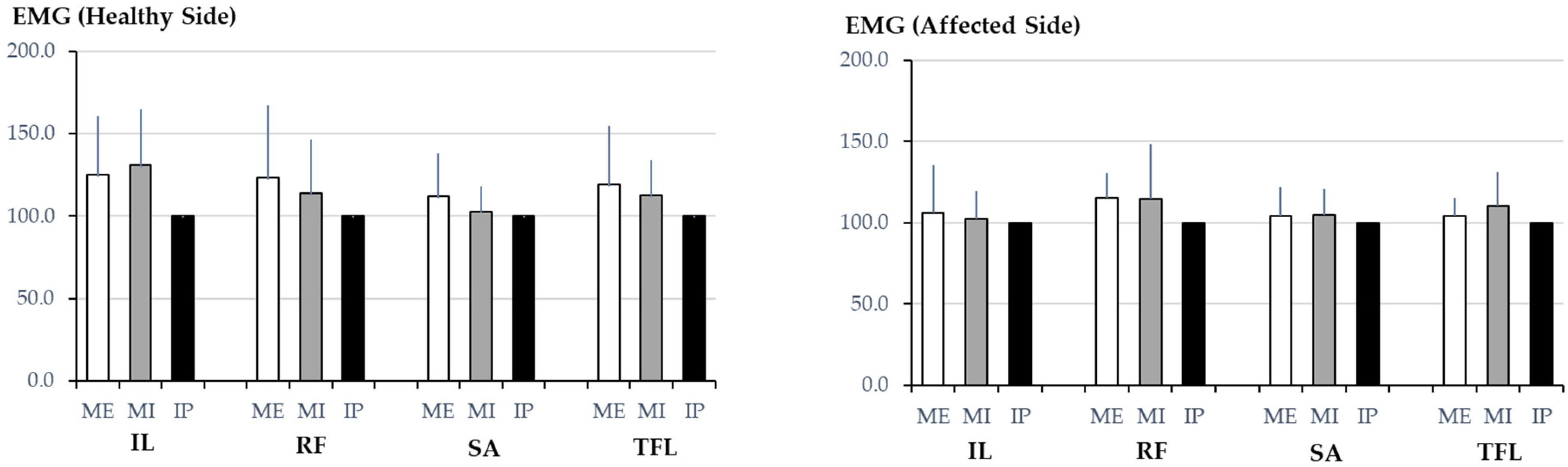
2.1. Hip Flexor Muscle Activity
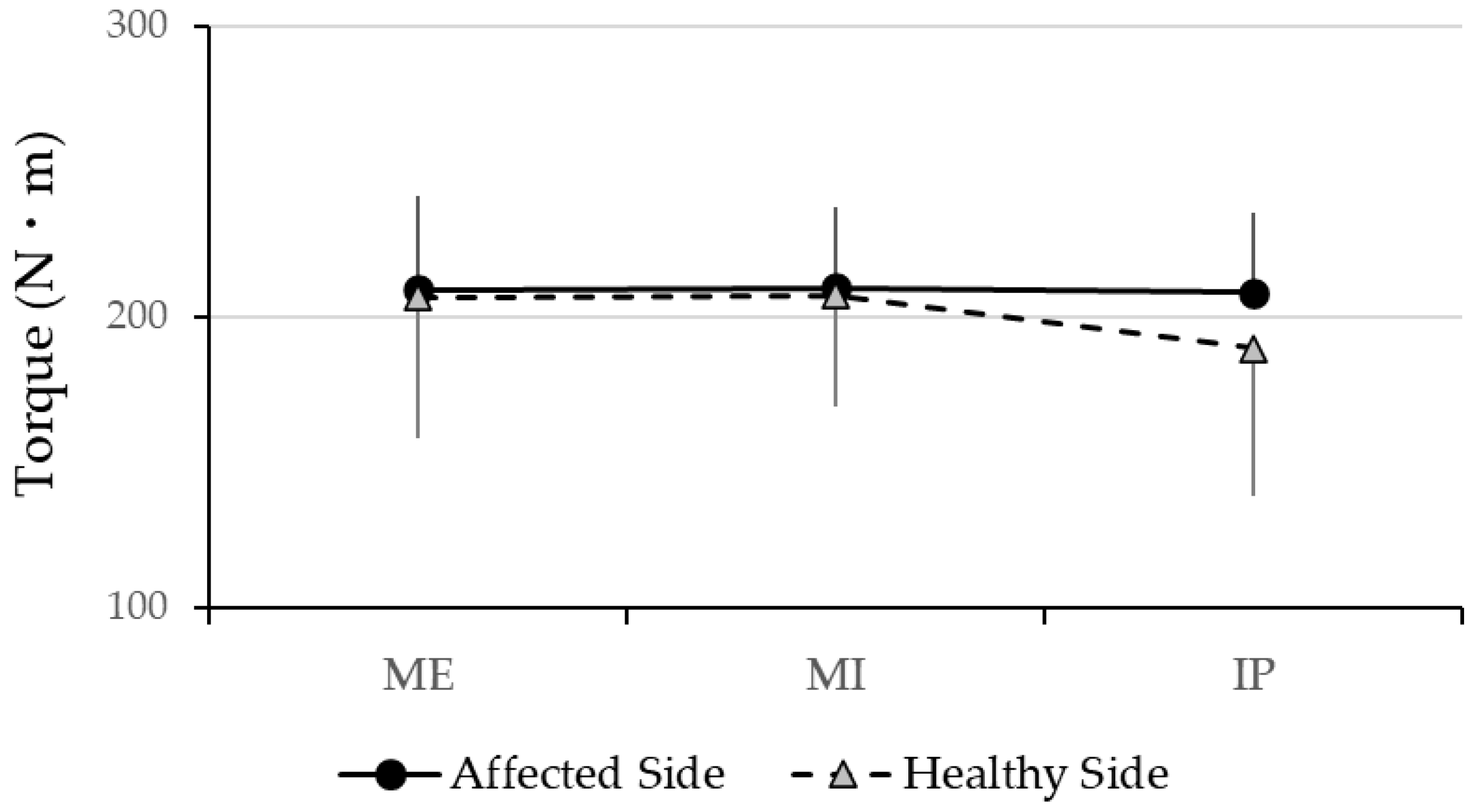
2.2. Torque Measurements
3. Discussion
3.1. Relationship Between Diaphragm Function and Iliopsoas Activity
3.2. Comparison with Other Hip Flexor Muscles and Impact on Force Production
3.3. Comparison with Clinical Implications and Rehabilitation Applications
3.4. Limitations
3.5. Future Directions
4. Materials and Methods
4.1. Relationship Between Diaphragm Study Design and Participants
- A history of CAS with onset at least six months prior to the study.
- Subjective instability reported in one ankle.
- A clear distinction between affected and unaffected limbs, allowing for side-to-side comparisons
- No history of ankle surgery or other major lower-limb interventions in the past year.
- Engagement in moderate or high levels of physical activity was defined as participation in sports or recreational exercise at least once a week.
- No history of other lower-limb musculoskeletal conditions, such as knee or hip disorders.
4.2. Muscle Measurement and Equipment
4.2.1. sEMG
4.2.2. Electrode Placement
- Rectus femoris: midpoint between the anterior inferior iliac spine (AIIS) and upper edge of the patella.
- Sartorius: Along the line connecting the ASIS and medial tibial condyle, approximately 8 cm distal to the ASIS.
- Tensor fasciae latae: Midpoint between the ASIS and apex of the greater trochanter.
4.2.3. Isokinetic Dynamometer
4.2.4. Experimental Conditions (Breath-Holding Conditions)
- End expiration (functional residual capacity state).
- End inspiration (maximum lung inflation state).
- Intermediate state (resting expiration level).
4.3. Data Analysis
4.3.1. EMG Analysis
4.3.2. Torque Analysis
4.3.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAI | chronic ankle instability |
| sEMG | surface electromyography |
| EMG | electromyography |
| MRI | magnetic resonance imaging |
| RMS | root mean square |
| IL | iliopsoas |
| RF | rectus femoris |
| SA | sartorius |
| TFL | tensor fasciae latae |
| ASIS | anterior superior iliac spine |
| ME | maximum expiration |
| MI | maximum inspiration |
| IP | intermediate position |
| ANOVA | analysis of variance |
References
- Anatomy, H.J.F. Pathomechanics, and Pathophysiology of Lateral Ankle Instability. J. Athl. Train. 2002, 37, 364–375. [Google Scholar]
- Fong, D.T.-P.; Hong, Y.; Chan, L.-K.; Yung, P.S.-H.; Chan, K.-M. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007, 37, 73–94. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.L.; Fourchet, F.; Fong, D.; Hertel, J.; Hiller, C.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J. Athl. Train. 2014, 49, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Miklovic, T.M.; Donovan, L.; Protzuk, O.A.; Kang, M.S.; Feger, M.A. Acute lateral ankle sprain to chronic ankle instability: A pathway of dysfunction. Phys. Sportsmed. 2018, 46, 116–122. [Google Scholar] [CrossRef]
- Kim, K.-M.; Best, T.M.; Aiyer, A. How Do Athletes with Chronic Ankle Instability Suffer from Impaired Balance? An Update on Neurophysiological Mechanisms. Curr. Sports Med. Rep. 2017, 16, 309–311. [Google Scholar] [CrossRef]
- Levin, O.; Vanwanseele, B.; Thijsen, J.R.J.; Helsen, W.F.; Staes, F.F.; Duysens, J. Proactive and reactive neuromuscular control in subjects with chronic ankle instability: Evidence from a pilot study on landing. Gait Posture 2015, 41, 106–111. [Google Scholar] [CrossRef]
- Kim, K.-M.; Estepa-Gallego, A.; Estudillo-Martínez, M.D.; Castellote-Caballero, Y.; Cruz-Díaz, D. Comparative Effects of Neuromuscular- and Strength-Training Protocols on Pathomechanical, Sensory-Perceptual, and Motor-Behavioral Impairments in Patients with Chronic Ankle Instability: Randomized Controlled Trial. Healthcare 2022, 10, 1364. [Google Scholar] [CrossRef]
- Hall, E.A.; Chomistek, A.K.; Kingma, J.J.; Docherty, C.L. Balance- and Strength-Training Protocols to Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome Measures. J. Athl. Train. 2018, 53, 568–577. [Google Scholar] [CrossRef]
- Han, J.; Luan, L.; Adams, R.; Witchalls, J.; Newman, P.; Tirosh, O.; Waddington, G. Can Therapeutic Exercises Improve Proprioception in Chronic Ankle Instability? A Systematic Review and Network Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 2232–2244. [Google Scholar] [CrossRef]
- Ardakani, M.K.; Wikstrom, E.A.; Minoonejad, H.; Rajabi, R.; Sharifnezhad, A. Hop-Stabilization Training and Landing Biomechanics in Athletes with Chronic Ankle Instability: A Randomized Controlled Trial. J. Athl. Train. 2019, 54, 1296–1303. [Google Scholar] [CrossRef]
- Cain, M.S.; Ban, R.J.; Chen, Y.-P.; Geil, M.D.; Goerger, B.M.; Linens, S.W. Four-Week Ankle-Rehabilitation Programs in Adolescent Athletes with Chronic Ankle Instability. J. Athl. Train. 2020, 55, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Foss, K.D.B.; Thomas, S.; Khoury, J.C.; Myer, G.D.; Hewett, T.E. A School-Based Neuromuscular Training Program and Sport-Related Injury Incidence: A Prospective Randomized Controlled Clinical Trial. J. Athl. Train. 2018, 53, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Recovery From a First-Time Lateral Ankle Sprain and the Predictors of Chronic Ankle Instability: A Prospective Cohort Analysis. Am. J. Sports Med. 2016, 44, 995–1003. [Google Scholar] [CrossRef]
- Delahunt, E.; Bleakley, C.M.; Bossard, D.S.; Caulfield, B.M.; Docherty, C.L.; Doherty, C.; Fourchet, F.; Fong, D.T.; Hertel, J.; Hiller, C.E.; et al. Clinical assessment of acute lateral ankle sprain injuries (ROAST): 2019 consensus statement and recommendations of the International Ankle Consortium. Br. J. Sports Med. 2018, 52, 1304–1310. [Google Scholar] [CrossRef]
- Wagemans, J.; Taeymans, J.; Kuppens, K.; Baur, H.; Bleakley, C.; Vissers, D. Determining key clinical predictors for chronic ankle instability and return to sports with cost of illness analysis: Protocol of a prospective cohort study. BMJ Open 2023, 13, e069867. [Google Scholar] [CrossRef]
- McCann, R.S.; Johnson, K.; Suttmiller, A.M.B. Lumbopelvic Stability and Trunk Muscle Contractility of Individuals with Chronic Ankle Instability. Int. J. Sports Phys. Ther. 2021, 16, 741–748. [Google Scholar] [CrossRef]
- DeJong, A.F.; Mangum, L.C.; Hertel, J. Ultrasound Imaging of the Gluteal Muscles During the Y-Balance Test in Individuals with or Without Chronic Ankle Instability. J. Athl. Train. 2020, 55, 49–57. [Google Scholar] [CrossRef]
- Hodges, P.W.; Heijnen, I.; Gandevia, S.C. Postural activity of the diaphragm is reduced in humans when respiratory demand increases. J. Physiol. 2001, 537 Pt 3, 999–1008. [Google Scholar] [CrossRef]
- Gandevia, S.C.; Butler, J.E.; Hodges, P.W.; Taylor, J.L. Motor control and the skeleton. Clin. Exp. Pharmacol. Physiol. 2002, 29, 118–121. [Google Scholar] [CrossRef]
- Finta, R.; Nagy, E.; Bender, T. The effect of diaphragm training on lumbar stabilizer muscles: A new concept for improving segmental stability in the case of low back pain. J. Pain. Res. 2018, 11, 3031–3045. [Google Scholar] [CrossRef]
- Eliks, M.; Zgorzalewicz-Stachowiak, M.; Zeńczak-Praga, K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: State of the art. Postgrad. Med. J. 2019, 95, 41–45. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J. Appl. Physiol. 2000, 89, 967–976. [Google Scholar] [CrossRef]
- Hodges, P.W.; Cresswell, A.G.; Daggfeldt, K.; Thorstensson, A. In vivo measurement of the effect of intra-abdominal pressure on the human spine. J. Biomech. 2001, 34, 347–353. [Google Scholar] [CrossRef]
- Terada, M.; Kosik, K.B.; McCann, R.S.; Gribble, P.A. Diaphragm Contractility in Individuals with Chronic Ankle Instability. Med. Sci. Sports Exerc. 2016, 48, 2040–2045. [Google Scholar] [CrossRef]
- Terada, M.; Kosik, K.B.; Gribble, P.A. Association of Diaphragm Contractility and Postural Control in a Chronic Ankle Instability Population: A Preliminary Study. Sports Health 2024, 16, 19–25. [Google Scholar] [CrossRef]
- Lee, D.G. The Pelvic Girdle: An Integration of Clinical Expertise and Research, 4th ed.; Churchill Livingstone: Philadelphia, PA, USA, 2010. [Google Scholar]
- Sajko, S.; Stuber, K. Psoas Major: A case report and review of its anatomy, biomechanics, and clinical implications. J. Can. Chiropr. Assoc. 2009, 53, 311–318. [Google Scholar]
- Regev, G.J.; Kim, C.W.; Tomiya, A.; Lee, Y.P.; Ghofrani, H.; Garfin, S.R.; Lieber, R.L.; Ward, S.R. Psoas muscle architectural design, in vivo sarcomere length range, and passive tensile properties support its role as a lumbar spine stabilizer. Spine 2011, 36, E1666–E1674. [Google Scholar] [CrossRef]
- Andersson, E.; Oddsson, L.; Grundström, H.; Thorstensson, A. The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scand. J. Med. Sci. Sports 1995, 5, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Ikezoe, T.; Mori, N.; Nakamura, M.; Ichihashi, N. Age-related muscle atrophy in the lower extremities and daily physical activity in elderly women. Arch. Gerontol. Geriatr. 2011, 53, e153–e157. [Google Scholar] [CrossRef]
- Andersson, E.A.; Nilsson, J.; Thorstensson, A. Intramuscular EMG from the hip flexor muscles during human locomotion. Acta Physiol. Scand. 1997, 161, 361–370. [Google Scholar] [CrossRef]
- Dorn, T.W.; Schache, A.G.; Pandy, M.G. Muscular strategy shift in human running: Dependence of running speed on hip and ankle muscle performance. J. Exp. Biol. 2012, 215 Pt 11, 1944–1956. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Activation of the human diaphragm during a repetitive postural task. J. Physiol. 2000, 522 Pt 1, 165–175. [Google Scholar] [CrossRef]
- Sinderby, C.; Beck, J.; Spahija, J.; Weinberg, J.; Grassino, A. Voluntary activation of the human diaphragm in health and disease. J. Appl. Physiol. 1998, 85, 2146–2158. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.H.; Khorramroo, F.; Minoonejad, H.; Zwerver, J. Effects of biofeedback on biomechanical factors associated with chronic ankle instability: A systematic review with meta-analysis. BMC Sports Sci. Med. Rehabil. 2023, 15, 168. [Google Scholar] [CrossRef] [PubMed]
- Urhun, E.; Develi, E. Investigation of the effect of chronic ankle instability on core stabilization, dynamic balance and agility among basketball players of a university. J. Bodyw. Mov. Ther. 2024, 40, 332–338. [Google Scholar] [CrossRef]
- Alizamani, S.; Ghasemi, G.; Nejadian, S.L. Effects of eight week core stability training on stable- and unstable-surface on ankle muscular strength, proprioception, and dorsiflexion in athletes with chronic ankle instability. J. Bodyw. Mov. Ther. 2023, 34, 6–12. [Google Scholar] [CrossRef]
- Carr, J.C.; Stock, M.S.; Hernandez, J.M.; Ortegon, J.R., Jr.; Mota, J.A. Additional insight into biarticular muscle function: The influence of hip flexor fatigue on rectus femoris activity at the knee. J. Electromyogr. Kinesiol. 2018, 42, 36–43. [Google Scholar] [CrossRef]
- Stutzig, N.; Siebert, T. Muscle force compensation among synergistic muscles after fatigue of a single muscle. Hum. Mov. Sci. 2015, 42, 273–287. [Google Scholar] [CrossRef]
- Masuda, K.; Kim, J.; Kinugasa, R.; Tanabe, K.; Kuno, S.-Y. Determinants for stair climbing by elderly from muscle morphology. Percept. Mot. Skills 2002, 94 Pt 1, 814–816. [Google Scholar] [CrossRef]
- Tottori, N.; Suga, T.; Miyake, Y.; Tsuchikane, R.; Otsuka, M.; Nagano, A.; Fujita, S.; Isaka, T. Hip Flexor and Knee Extensor Muscularity Are Associated with Sprint Performance in Sprint-Trained Preadolescent Boys. Pediatr. Exerc. Sci. 2018, 30, 115–123. [Google Scholar] [CrossRef]
- Wakahara, T.; Chiba, M. Relation Between Iliopsoas Cross-sectional Area and Kicked Ball Speed in Soccer Players. Int. J. Sports Med. 2018, 39, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Mattacola, C.G.; Dwyer, M.K. Rehabilitation of the Ankle After Acute Sprain or Chronic Instability. J. Athl. Train. 2002, 37, 413–429. [Google Scholar] [PubMed]
- Al Attar, W.S.A.; Khaledi, E.H.; Bakhsh, J.M.; Faude, O.; Ghulam, H.; Sanders, R.H. Injury prevention programs that include balance training exercises reduce ankle injury rates among soccer players: A systematic review. J. Physiother. 2022, 68, 165–173. [Google Scholar] [CrossRef]
- Yeum, W.-J.; Lee, M.-Y.; Lee, B.-H. The Influence of Hip-Strengthening Program on Patients with Chronic Ankle Instability. Medicina 2024, 60, 1199. [Google Scholar] [CrossRef]
- Feger, M.A.; Donovan, L.; Hart, J.M.; Hertel, J. Lower extremity muscle activation during functional exercises in patients with and without chronic ankle instability. PM R. 2014, 6, 602–611, quiz 611. [Google Scholar] [CrossRef]
- Labanca, L.; Mosca, M.; Ghislieri, M.; Agostini, V.; Knaflitz, M.; Benedetti, M.G. Muscle activations during functional tasks in individuals with chronic ankle instability: A systematic review of electromyographical studies. Gait Posture 2021, 90, 340–373. [Google Scholar] [CrossRef]
- Jiroumaru, T.; Kurihara, T.; Isaka, T. Establishment of a recording method for surface electromyography in the iliopsoas muscle. J. Electromyogr. Kinesiol. 2014, 24, 445–451. [Google Scholar] [CrossRef]
- Jiroumaru, T.; Kurihara, T.; Isaka, T. Measurement of muscle length-related electromyography activity of the hip flexor muscles to determine individual muscle contributions to the hip flexion torque. Springerplus 2014, 22, 624. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Muscle | Condition | Healthy Side (n = 11) | Affected Side (n = 11) | p-Value |
|---|---|---|---|---|
| Iliopsoas | Maximum inspiration | 131 ± 34 | 103 ± 17 | 0.014 * |
| Maximum expiration | 125 ± 36 | 106 ± 29 | 0.129 | |
| Intermediate position | 100 ± 0 | 100 ± 0 | — | |
| Rectus Femoris | Maximum inspiration | 114 ± 33 | 115 ± 16 | 0.939 |
| Maximum expiration | 132 ± 67 | 115 ± 33 | 0.372 | |
| Intermediate position | 100 ± 0 | 100 ± 0 | — | |
| Sartorius | Maximum inspiration | 103 ± 15 | 105 ± 16 | 0.792 |
| Maximum expiration | 112 ± 26 | 104 ± 18 | 0.361 | |
| Intermediate position | 100 ± 0 | 100 ± 0 | — | |
| Tensor Fasciae Latae | Maximum inspiration | 113 ± 21 | 110 ± 21 | 0.673 |
| Maximum expiration | 119 ± 36 | 104 ± 11 | 0.212 | |
| Intermediate position | 100 ± 0 | 100 ± 0 | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiroumaru, T.; Nomura, S.; Hyodo, Y.; Wachi, M.; Ochi, J.; Shichiri, N.; Fujikawa, T. A Pilot Study on the Influence of Diaphragmatic Function on Iliopsoas Muscle Activity in Individuals with Chronic Ankle Instability. Muscles 2025, 4, 16. https://doi.org/10.3390/muscles4020016
Jiroumaru T, Nomura S, Hyodo Y, Wachi M, Ochi J, Shichiri N, Fujikawa T. A Pilot Study on the Influence of Diaphragmatic Function on Iliopsoas Muscle Activity in Individuals with Chronic Ankle Instability. Muscles. 2025; 4(2):16. https://doi.org/10.3390/muscles4020016
Chicago/Turabian StyleJiroumaru, Takumi, Shun Nomura, Yutaro Hyodo, Michio Wachi, Junko Ochi, Nobuko Shichiri, and Takamitsu Fujikawa. 2025. "A Pilot Study on the Influence of Diaphragmatic Function on Iliopsoas Muscle Activity in Individuals with Chronic Ankle Instability" Muscles 4, no. 2: 16. https://doi.org/10.3390/muscles4020016
APA StyleJiroumaru, T., Nomura, S., Hyodo, Y., Wachi, M., Ochi, J., Shichiri, N., & Fujikawa, T. (2025). A Pilot Study on the Influence of Diaphragmatic Function on Iliopsoas Muscle Activity in Individuals with Chronic Ankle Instability. Muscles, 4(2), 16. https://doi.org/10.3390/muscles4020016