
Sport-Related Injuries in Portuguese CrossFit® Practitioners and Their Characteristics

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
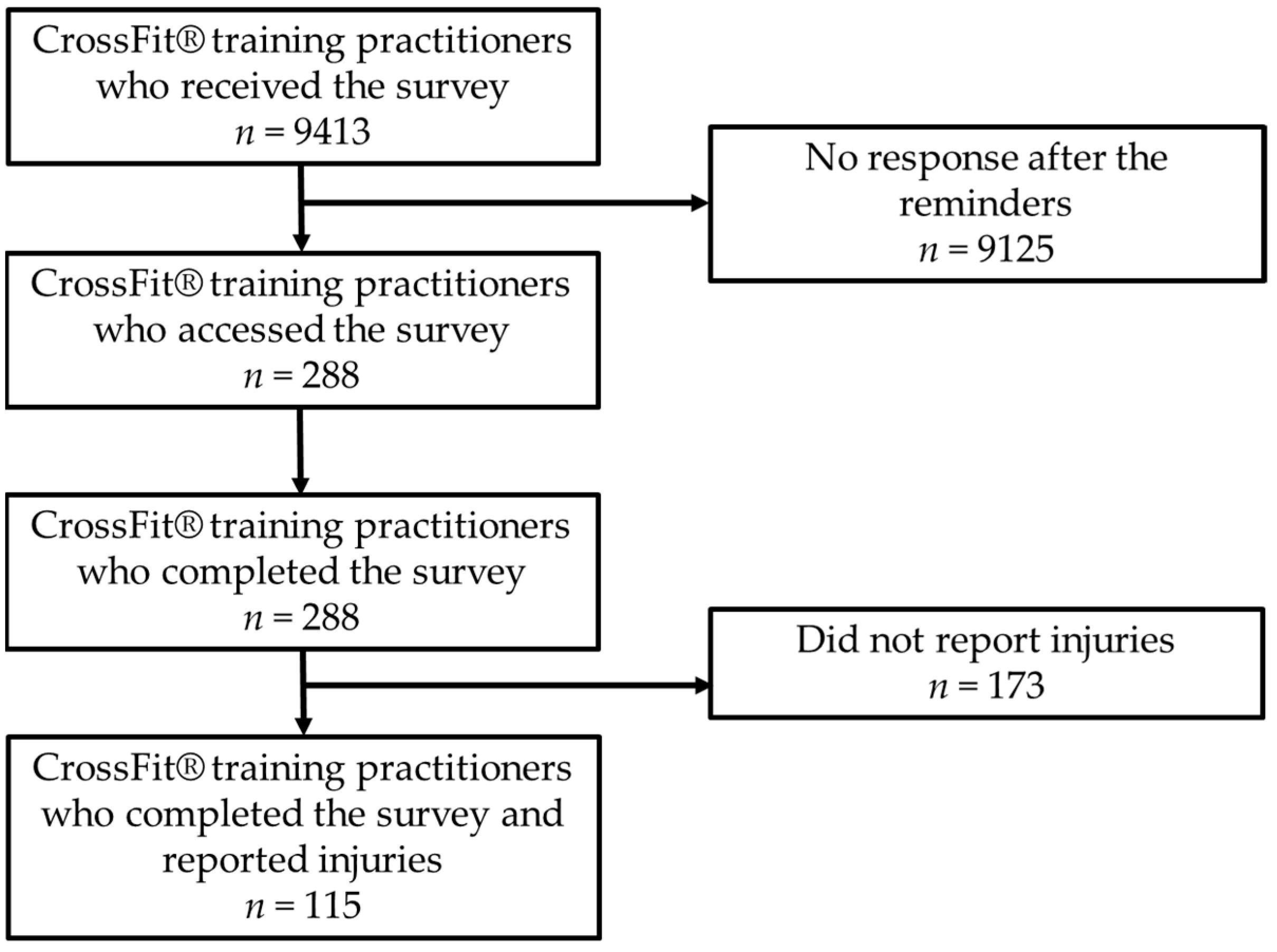
2.1. Participants and Data Collection
2.2. Questionnaire
- Sport and sociodemographic-related items. The items covered information regarding age, sex, height, weight, professional physical level, sports background, years of CrossFit® training, CrossFit® training level, CrossFit® training competition participation, CrossFit® training load, training context, and CrossFit® training warm-up and cool-down.
- Health disorders and injuries-related items. The items covered information regarding health disorders and injuries related to CrossFit® Training, e.g., type, location, frequency, time to return to sport, context, health history, and management. Items in this phase were adapted from a consensus statement on injury registration [46]. It defined injury as any physical damage to a body part, sustained during training or competition, which prevented the participant from training, working, or competing in any way and for any period of time [25,47]. To ensure questionnaires were filled out properly, definitions and examples were given throughout the items, helping to contextualize the readers.
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vassis, K.; Siouras, A.; Kourkoulis, N.; Poulis, I.A.; Meletiou, G.; Iliopoulou, A.-M.; Misiris, I. Epidemiological Profile among Greek CrossFit Practitioners. Int. J. Environ. Res. Public Health 2023, 20, 2538. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Lavallee, M.E.; Balam, T. An overview of strength training injuries: Acute and chronic. Curr. Sports Med. Rep. 2010, 9, 307–313. [Google Scholar] [CrossRef]
- Wahl, P.; Bloch, W.; Proschinger, S. The molecular signature of high-intensity training in the human body. Int. J. Sports Med. 2021, 43, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: Cardiopulmonary emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef]
- American College of Sports Medicine. American College of Sports Medicine Position Stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef] [PubMed]
- Billat, L.V. Interval training for performance: A scientific and empirical practice: Special recommendations for middle- and long-distance running. Part I: Aerobic interval training. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef]
- Rugbeer, N.; Constantinou, D.; Torres, G. Comparison of high-intensity training versus moderate-intensity continuous training on cardiorespiratory fitness and body fat percentage in persons with overweight or obesity: A systematic review and meta-analysis of randomized controlled trials. J. Phys. Act. Health 2021, 18, 610–623. [Google Scholar] [CrossRef]
- Feito, Y.; Heinrich, K.M.; Butcher, S.J.; Poston, W.S.C. High-intensity functional training (HIFT): Definition and research implications for improved fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Burrows, E.K.; Tabb, L.P. A 4-year analysis of the incidence of injuries among CrossFit-trained participants. Orthop. J. Sports Med. 2018, 6, 2325967118803100. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, T.S.; Louzada, C.T.N.; Miyashita, G.K.; da Silva, P.H.J.; Sungaila, H.Y.F.; Lara, P.H.S.; Pochini, A.d.C.; Ejnisman, B.; Cohen, M.; Arliani, G.G. CrossFit®: Injury prevalence and main risk factors. Clinics 2019, 74, e1402. [Google Scholar] [CrossRef] [PubMed]
- Alekseyev, K.; John, A.; Malek, A.; Lakdawala, M.; Verma, N.; Southall, C.; Nikolaidis, A.; Akella, S.; Erosa, S.; Islam, R. Identifying the most common CrossFit injuries in a variety of athletes. Rehabil. Process Outcome 2020, 9, 1179572719897069. [Google Scholar] [CrossRef]
- Claudino, J.G.; Gabbett, T.J.; Bourgeois, F.; Souza, H.d.S.; Miranda, R.C.; Mezêncio, B.; Soncin, R.; Cardoso Filho, C.A.; Bottaro, M.; Hernandez, A.J. CrossFit overview: Systematic review and meta-analysis. Sports Med. Open 2018, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- FinModelsLab. How Much Crossfit Business Owner Make? 2024. Available online: https://finmodelslab.com/blogs/how-much-makes/how-much-business-owner-makes-crossfit (accessed on 31 August 2024).
- Feito, Y.; Burrows, E.; Tabb, L.; Ciesielka, K.-A. Breaking the myths of competition: A cross-sectional analysis of injuries among CrossFit trained participants. BMJ Open Sport Exerc. Med. 2020, 6, e000750. [Google Scholar] [CrossRef] [PubMed]
- CrossFit. CrossFit Games. Available online: https://games.crossfit.com/ (accessed on 31 August 2024).
- CrossFit. Find a Gym. Available online: https://www.crossfit.com/map (accessed on 31 August 2024).
- CrossFit. Open a Crossfit Gym. Available online: https://www.crossfit.com/open-crossfit-gym (accessed on 31 August 2024).
- Pedragosa, V.; Cardadeiro, E.; Santos, A. Barómetro do Fitness em Portugal; Relatório Final; Centro de Estudos Económicos e Institucionais, Universidade Autónoma de Lisboa: Lisbon, Portugal, 2022. [Google Scholar]
- Mehrab, M.; de Vos, R.-J.; Kraan, G.A.; Mathijssen, N.M. Injury incidence and patterns among Dutch CrossFit athletes. Orthop. J. Sports Med. 2017, 5, 2325967117745263. [Google Scholar] [CrossRef] [PubMed]
- Glassman, G. Understanding crossfit. CrossFit J. 2007, 56, 1–2. [Google Scholar]
- Gianzina, E.A.; Kassotaki, O.A. The benefits and risks of the high-intensity CrossFit training. Sport Sci. Health 2019, 15, 21–33. [Google Scholar] [CrossRef]
- Weisenthal, B.M.; Beck, C.A.; Maloney, M.D.; DeHaven, K.E.; Giordano, B.D. Injury rate and patterns among CrossFit athletes. Orthop. J. Sports Med. 2014, 2, 2325967114531177. [Google Scholar] [CrossRef]
- Sprey, J.W.; Ferreira, T.; de Lima, M.V.; Duarte, A., Jr.; Jorge, P.B.; Santili, C. An epidemiological profile of CrossFit athletes in Brazil. Orthop. J. Sports Med. 2016, 4, 2325967116663706. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.M.; Shaefer, H.; Rodriguez, B.; Li, T.; Epnere, K.; Myer, G.D. Retrospective injury epidemiology and risk factors for injury in CrossFit. J. Sports Sci. Med. 2017, 16, 53. [Google Scholar] [PubMed]
- Moran, S.; Booker, H.; Staines, J.; Williams, S. Rates and risk factors of injury in CrossFit: A prospective cohort study. J Sports Med Phys Fit. 2017, 57, 1147–1153. [Google Scholar]
- Waryasz, G.R.; Suric, V.; Daniels, A.H.; Gil, J.A.; Eberson, C.P. CrossFit® instructor demographics and practice trends. Orthop. Rev. 2016, 8, 6571. [Google Scholar]
- Szajkowski, S.; Dwornik, M.; Pasek, J.; Cieślar, G. Risk Factors for Injury in CrossFit®—A Retrospective Analysis. Int. J. Environ. Res. Public Health 2023, 20, 2211. [Google Scholar] [CrossRef] [PubMed]
- Dawson, M.C. CrossFit: Fitness cult or reinventive institution? Int. Rev. Sociol. Sport 2017, 52, 361–379. [Google Scholar] [CrossRef]
- Whiteman-Sandland, J.; Hawkins, J.; Clayton, D. The role of social capital and community belongingness for exercise adherence: An exploratory study of the CrossFit gym model. J. Health Psychol. 2018, 23, 1545–1556. [Google Scholar] [CrossRef]
- Bycura, D.; Feito, Y.; Prather, C. Motivational factors in CrossFit® training participation. Health Behav. Policy Rev. 2017, 4, 539–550. [Google Scholar] [CrossRef]
- Mangine, G.T.; Tankersley, J.E.; McDougle, J.M.; Velazquez, N.; Roberts, M.D.; Esmat, T.A.; VanDusseldorp, T.A.; Feito, Y. Predictors of CrossFit open performance. Sports 2020, 8, 102. [Google Scholar] [CrossRef] [PubMed]
- Prewitt-White, T.; Connolly, C.P.; Feito, Y.; Bladek, A.; Forsythe, S.; Hamel, L.; McChesney, M.R. Breaking barriers: Women’s experiences of crossfit training during pregnancy. Women Sport Phys. Act. J. 2018, 26, 33–42. [Google Scholar] [CrossRef]
- Mehrab, M.; Wagner, R.K.; Vuurberg, G.; Gouttebarge, V.; De Vos, R.-J.; Mathijssen, N.M.C. Risk factors for musculoskeletal injury in CrossFit: A systematic review. Int. J. Sports Med. 2022, 44, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Barranco-Ruiz, Y.; Villa-González, E.; Martínez-Amat, A.; Da Silva-Grigoletto, M.E. Prevalence of injuries in exercise programs based on Crossfit®, cross training and high-intensity functional training methodologies: A systematic review. J. Hum. Kinet. 2020, 73, 251. [Google Scholar] [CrossRef]
- Glassman, J. Consortium for Health and Military Performance and American College of Sports Medicine Consensus Paper on Extreme Conditioning Programs in Military Personnel: An Answer. CrossFit J. 2012, 1–92. Available online: https://journal.crossfit.com/ (accessed on 31 August 2024).
- Bergeron, M.F.; Nindl, B.C.; Deuster, P.A.; Baumgartner, N.; Kane, S.F.; Kraemer, W.J.; Sexauer, L.R.; Thompson, W.R.; O’Connor, F.G. Consortium for Health and Military Performance and American College of Sports Medicine consensus paper on extreme conditioning programs in military personnel. Curr. Sports Med. Rep. 2011, 10, 383–389. [Google Scholar] [CrossRef]
- Feito, Y.; Brown, C.; Olmos, A. A content analysis of the high-intensity functional training literature: A look at the past and directions for the future. Hum. Mov. 2019, 20, 1–15. [Google Scholar] [CrossRef]
- Ángel Rodríguez, M.; García-Calleja, P.; Terrados, N.; Crespo, I.; Del Valle, M.; Olmedillas, H. Injury in CrossFit®: A systematic review of epidemiology and risk factors. Physician Sportsmed. 2022, 50, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Minghelli, B.; Vicente, P. Musculoskeletal injuries in Portuguese CrossFit practitioners. J. Sports Med. Phys. Fit. 2019, 59, 1213–1220. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Passmore, C.; Dobbie, A.E.; Parchman, M.; Tysinger, J. Guidelines for constructing a survey. Fam. Med. 2002, 34, 281–286. [Google Scholar] [PubMed]
- Sierles, F.S. How to do research with self-administered surveys. Acad. Psychiatry 2003, 27, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Artino, A.R., Jr.; Durning, S.J.; Sklar, D.P. Guidelines for reporting survey-based research submitted to academic medicine. Acad. Med. 2018, 93, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sports 2020 (including the STROBE extension for sports injury and illness surveillance (STROBE-SIIS)). Orthop. J. Sports Med. 2020, 8, 2325967120902908. [Google Scholar] [CrossRef] [PubMed]
- Hak, P.T.; Hodzovic, E.; Hickey, B. The nature and prevalence of injury during CrossFit training. J. Strength Cond. Res. 2022. [Google Scholar] [CrossRef]
- Prion, S.; Haerling, K.A. Making sense of methods and measurement: Spearman-rho ranked-order correlation coefficient. Clin. Simul. Nurs. 2014, 10, 535–536. [Google Scholar] [CrossRef]
- Andrade, C. The P value and statistical significance: Misunderstandings, explanations, challenges, and alternatives. Indian J. Psychol. Med. 2019, 41, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Tafuri, S.; Salatino, G.; Napoletano, P.L.; Monno, A.; Notarnicola, A. The risk of injuries among CrossFit athletes: An Italian observational retrospective survey. J. Sports Med. Phys. Fit. 2018, 59, 1544–1550. [Google Scholar] [CrossRef]
- Lastra-Rodríguez, L.; Llamas-Ramos, I.; Rodríguez-Pérez, V.; Llamas-Ramos, R.; López-Rodríguez, A.F. Musculoskeletal Injuries and Risk Factors in Spanish CrossFit® Practitioners. Healthcare 2023, 11, 1346. [Google Scholar] [CrossRef] [PubMed]
- Lima, P.O.; Souza, M.B.; Sampaio, T.V.; Almeida, G.P.; Oliveira, R.R. Epidemiology and associated factors for CrossFit-related musculoskeletal injuries: A cross-sectional study. J. Sports Med. Phys. Fit. 2020, 60, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Reis, V.A.; Reis, N.A.d.M.A.; Santos, T.R.T. Perfil de lesões em praticantes de CrossFit®: Prevalência e fatores associados durante um ano de prática esportiva. Fisioter. Pesqui. 2022, 29, 88–95. [Google Scholar] [CrossRef]
- Toledo, R.; Dias, M.R.; Souza, D.; Soares, R.; Toledo, R.; Lácio, M.; Vianna, J. Joint and muscle injuries in men and women CrossFit® training participants. Physician Sportsmed. 2022, 50, 205–211. [Google Scholar] [CrossRef]
- Szeles, P.R.d.Q.; Costa, T.S.d.; Cunha, R.A.d.; Hespanhol, L.; Pochini, A.d.C.; Ramos, L.A.; Cohen, M. CrossFit and the epidemiology of musculoskeletal injuries: A prospective 12-week cohort study. Orthop. J. Sports Med. 2020, 8, 2325967120908884. [Google Scholar] [CrossRef]
- Chachula, L.A.; Cameron, K.L.; Svoboda, S.J. Association of prior injury with the report of new injuries sustained during CrossFit training. Athl. Train. Sports Health Care 2016, 8, 28–34. [Google Scholar] [CrossRef]
- Escalante, G.; Gentry, C.R.; Kern, B.D.; Waryasz, G.R. Injury patterns and rates of Costa Rican CrossFit® participants—A retrospective study. Med. Sport. J. Rom. Sports Med. Soc. 2017, 13, 2927–2934. [Google Scholar]
- Brandsema, C.; Mehrab, M.; Mathijssen, N. Most Common Injuries in CrossFit Training: A Systematic Review. Int. J. Sports Exerc. Med. 2022, 8, 228. [Google Scholar] [CrossRef]
- Klimek, C.; Ashbeck, C.; Brook, A.J.; Durall, C. Are injuries more common with CrossFit training than other forms of exercise? J. Sport Rehabil. 2018, 27, 295–299. [Google Scholar] [CrossRef]
- Parkkari, J.; Kannus, P.; Natri, A.; Lapinleimu, I.; Palvanen, M.; Heiskanen, M.; Vuori, I.; Järvinen, M. Active living and injury risk. Int. J. Sports Med. 2004, 25, 209–216. [Google Scholar] [PubMed]
- Campbell, R.A.; Bradshaw, E.J.; Ball, N.B.; Pease, D.L.; Spratford, W. Injury epidemiology and risk factors in competitive artistic gymnasts: A systematic review. Br. J. Sports Med. 2019, 53, 1056–1069. [Google Scholar] [CrossRef]
- Keogh, J.W.; Winwood, P.W. The epidemiology of injuries across the weight-training sports. Sports Med. 2017, 47, 479–501. [Google Scholar] [CrossRef]
- Aasa, U.; Svartholm, I.; Andersson, F.; Berglund, L. Injuries among weightlifters and powerlifters: A systematic review. Br. J. Sports Med. 2017, 51, 211–219. [Google Scholar] [CrossRef]
- Summitt, R.J.; Cotton, R.A.; Kays, A.C.; Slaven, E.J. Shoulder injuries in individuals who participate in CrossFit training. Sports Health 2016, 8, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Nicolay, R.W.; Moore, L.K.; DeSena, T.D.; Dines, J.S. Upper extremity injuries in CrossFit athletes—A review of the current literature. Curr. Rev. Musculoskelet. Med. 2022, 15, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.R.; Maffulli, N.; Migliorini, F.; Santos, G.M.; de Menezes, F.S.; Okubo, R. Function, strength, and muscle activation of the shoulder complex in Crossfit practitioners with and without pain: A cross-sectional observational study. J. Orthop. Surg. Res. 2022, 17, 24. [Google Scholar] [CrossRef]
- Sugimoto, D.; Zwicker, R.L.; Quinn, B.J.; Myer, G.D.; Stracciolini, A. Part II: Comparison of CrossFit-related injury presenting to sports medicine clinic by sex and age. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2020, 30, 251. [Google Scholar] [CrossRef] [PubMed]
- Torres-Banduc, M.A.; Jerez-Mayorga, D.; Moran, J.; Keogh, J.W.; Ramírez-Campillo, R. Isokinetic force-power profile of the shoulder joint in males participating in CrossFit training and competing at different levels. PeerJ 2021, 9, e11643. [Google Scholar] [CrossRef] [PubMed]
- Berckmans, K.; Maenhout, A.G.; Matthijs, L.; Pieters, L.; Castelein, B.; Cools, A.M. The isokinetic rotator cuff strength ratios in overhead athletes: Assessment and exercise effect. Phys. Ther. Sport 2017, 27, 65–75. [Google Scholar] [CrossRef]
- Wagener, S.; Hoppe, M.W.; Hotfiel, T.; Engelhardt, M.; Javanmardi, S.; Baumgart, C.; Freiwald, J. CrossFit®—Development, Benefits and Risks. Sports Orthop. Traumatol. 2020, 36, 241–249. [Google Scholar] [CrossRef]
- Kaczorowska, A.; Noworyta, K.; Mroczek, A.; Lepsy, E. Effect of the MobilityWOD training program on functional movement patterns related to the risk of injury in CrossFit practitioners. Acta Gymnica 2020, 50, 3–8. [Google Scholar] [CrossRef]
- Gardiner, B.; Devereux, G.; Beato, M. Injury risk and injury incidence rates in CrossFit. J. Sports Med. Phys. Fit. 2020, 60, 1005–1013. [Google Scholar] [CrossRef]
- Mangine, G.T.; Stratton, M.T.; Almeda, C.G.; Roberts, M.D.; Esmat, T.A.; VanDusseldorp, T.A.; Feito, Y. Physiological differences between advanced CrossFit athletes, recreational CrossFit participants, and physically-active adults. PLoS ONE 2020, 15, e0223548. [Google Scholar] [CrossRef]
- Gabbett, T.J. The training—Injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sports Med. 2016, 50, 273–280. [Google Scholar] [CrossRef]

{kind=link}
| Static Stretching | Dynamic Stretching | Sport-Specific | Core | Running | Mobility | Running Drills | Strengthening | Balance | Self-Massage | n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
 | 14 (6.1) | |||||||||
| | 13 (5.7) | ||||||||
| | | 11 (4.8) | |||||||
| | | 9 (4.0) | |||||||
| | 8 (3.5) | ||||||||
| | | | | 7 (3.1) | |||||
| | | | 7 (3.1) | ||||||
| | | | | 6 (2.6) | |||||
| | 5 (2.2) | ||||||||
| | 5 (2.2) | ||||||||
| 4 (1.8) | |||||||||
| | 4 (1.8) | ||||||||
| | 4 (1.8) | ||||||||
| | | | 4 (1.8) | ||||||
| 4 (1.8) | |||||||||
| | 3 (1.3) | ||||||||
| | | | 3 (1.3) | ||||||
| | | 3 (1.3) | |||||||
| | | 3 (1.3) | |||||||
| | | 3 (1.3) | |||||||
| | | 2 (0.9) | |||||||
| | | 2 (0.9) | |||||||
| | | | 2 (0.9) | ||||||
| | | | 2 (0.9) | ||||||
| 2 (0.9) | |||||||||
| | | | 2 (0.9) | ||||||
| | | | | | 2 (0.9) | ||||
| | | | | | | 2 (0.9) | |||
| | | | | | 2 (0.9) | ||||
| | | 2 (0.9) | |||||||
| | | 2 (0.9) | |||||||
| | | | 2 (0.9) | ||||||
| | | 2 (0.9) |
| Variable | Total (n = 288 (100%)) n(%) | Unreported Injury (n = 173 (60.1%)) n(%) | Reported Injury (n = 115 (39.9%)) n(%) | p Injury vs. No Injury |
|---|---|---|---|---|
| Age group (years) | 0.727 * | |||
| 18–24 | 15 (5.2) | 10 (5.8) | 5 (4.3) | |
| 25–29 | 52 (18.1) | 30 (17.3) | 22 (19.1) | |
| 30–34 | 55 (19.1) | 45 (26) | 24 (20.9) | |
| 35–39 | 69 (24.0) | 36 (20.8) | 26 (22.6) | |
| 40–44 | 26 (9.0) | 15 (8.7) | 11 (9.6) | |
| 45–50 | 9 (3.1) | 7 (4.0) | 2 (1.7) | |
| +50 | ||||
| Sex | 0.614 ** | |||
| Female | 140 (48.6) | 82 (47.4) | 58 (50.4) | |
| Male | 148 (51.4) | 91 (52.6) | 57 (49.6) | |
| Body weight (kilograms) | 0.612 * | |||
| −50 | 6 (2.1) | 4 (2.3) | 2 (1.7) | |
| 50–74 | 158 (54.9) | 97 (56.1) | 61 (53.0) | |
| 75–100 | 114 (39.6) | 65 (37.6) | 49 (42.6) | |
| +100 | 10 (3.5) | 7 (4.0) | 3 (2.6) | |
| Body height (meters) | 0.618 * | |||
| −1.50 | 2 (0.7) | 2 (1.2) | 0 (0.0) | |
| 1.50–1.74 | 180 (62.5) | 109 (63) | 71 (61.7) | |
| 1.75–2.00 | 105 (36.5) | 61 (35.3) | 44 (38.3) | |
| +2.00 | 1 (0.3) | 1 (0.6) | 0 (0.0) | |
| Profession physical activity level | 0.505 * | |||
| Sedentary | 64 (22.2) | 35 (20.2) | 29 (25.2) | |
| Sitting and walking, without physical efforts | 113 (39.2) | 70 (40.5) | 43 (37.4) | |
| Sitting and walking, with moderate physical efforts | 32 (11.1) | 17 (9.8) | 15 (13) | |
| Sitting and walking, with heavy physical efforts | 5 (1.7) | 4 (2.3) | 1 (0.9) | |
| Standing and walking, without physical efforts | 18 (6.3) | 13 (7.5) | 5 (4.3) | |
| Standing and walking, with moderate physical efforts | 39 (13.5) | 26 (15.0) | 13 (11.3) | |
| Standing and walking, with heavy physical efforts | 17 (5.9) | 8 (4.6) | 9 (7.8) | |
| Sport or physical activity background | 0.199 ** | |||
| Yes | 219 (76.0) | 127 (73.4) | 92 (80.0) | |
| No | 69 (24.0) | 46 (26.6) | 23 (20.0) | |
| Years practicing CrossFit® training | 0.006 * | |||
| −1 | 65 (22.6) | 49 (28.3) | 16 (13.9) | |
| 1–3 | 94 (32.6) | 55 (31.8) | 39 (33.9) | |
| 4–6 | 73 (25.3) | 41 (23.7) | 32 (27.8) | |
| 7–10 | 48 (16.7) | 23 (13.3) | 25 (21.7) | |
| +10 | 8 (2.8) | 5 (2.9) | 3 (2.6) | |
| CrossFit® training competitive level | 0.051 * | |||
| Non-competitive | 197 (68.4) | 125 (72.3) | 72 (62.6) | |
| Competitive, recreational | 45 (15.6) | 26 (15) | 19 (16.5) | |
| Competitive, beginner | 25 (8.7) | 14 (8.1) | 11 (9.6) | |
| Competitive, advanced | 21 (7.3) | 8 (4.6) | 13 (11.3) | |
| CrossFit® training weekly practice | 0.003 * | |||
| Once per week | 8 (2.8) | 8 (4.6) | 0 (0.0) | |
| 2–3 times per week | 90 (31.3) | 62 (35.8) | 28 (24.3) | |
| 4–6 times per week | 180 (62.5) | 98 (56.6) | 82 (71.3) | |
| 7 or more times a week | 10 (3.5) | 5 (2.9) | 5 (4.3) | |
| CrossFit® training practice duration (minutes) | 0.615 * | |||
| 30–59 | 178 (61.8) | 104 (60.1) | 74 (64.3) | |
| 60–89 | 100 (34.7) | 65 (37.6) | 35 (30.4) | |
| 90–120 | 10 (3.5) | 4 (2.3) | 6 (5.2) | |
| Annual CrossFit® training competitions participations | 0.076 * | |||
| Do not compete | 197 (68.4) | 125 (72.3) | 72 (62.6) | |
| 1 | 27 (9.4) | 15 (8.7) | 12 (10.4) | |
| 2 | 37 (12.8) | 20 (11.6) | 17 (14.8) | |
| 3 | 17 (5.9) | 7 (4.0) | 10 (8.7) | |
| 4 | 7 (2.4) | 5 (2.9) | 2 (1.7) | |
| 5 | 1 (0.3) | 0 (0.0) | 1 (0.9) | |
| +5 | 2 (0.7) | 1 (0.6) | 1 (0.9) | |
| Warm-up before training/competitions? | 0.808 * | |||
| No | 56 (19.4) | 33 (19.1) | 23 (20.0) | |
| Yes, −10 min | 140 (48.6) | 83 (48.0) | 57 (49.6) | |
| Yes, 10–20 min | 85 (29.5) | 55 (31.8) | 30 (26.1) | |
| Yes, 21–30 min | 6 (2.1) | 2 (1.2) | 4 (3.5) | |
| Yes, +30 min | 1 (0.3) | 0 (0.0) | 1 (0.9) | |
| Warm-up exercises used | ||||
| Running | 32 (3.9) | 20 (4.1) | 12 (3.5) | 0.766 ** |
| Sprint | 8 (1.0) | 6 (1.2) | 2 (0.6) | 0.382 ** |
| Running drills | 56 (6.8) | 34 (7.0) | 22 (6.4) | 0.913 ** |
| Mobility exercises | 198 (23.9) | 117 (24.2) | 81 (23.5) | 0.615 ** |
| Dynamic stretching | 152 (18.4) | 86 (17.8) | 66 (19.1) | 0.201 ** |
| Static stretching | 90 (10.9) | 51 (10.6) | 39 (11.3) | 0.427 ** |
| Strengthening exercises | 47 (5.7) | 26 (5.4) | 21 (6.1) | 0.467 ** |
| Core exercises | 90 (10.9) | 50 (10.4) | 40 (11.6) | 0.292 ** |
| Balance exercises | 28 (3.4) | 15 (3.1) | 13 (3.8) | 0.460 ** |
| Sport-specific exercises | 102 (12.3) | 60 (12.4) | 42 (12.2) | 0.749 ** |
| Plyometrics | 11 (1.3) | 9 (1.9) | 2 (0.6) | 0.133 ** |
| Self-massage | 8 (1.0) | 4 (0.8) | 4 (1.2) | 0.555 ** |
| Other | 6 (0.7) | 5 (1.0) | 1 (0.3) | 0.240 ** |
| Cool-down after training/competitions? | 0.456 * | |||
| No | 99 (34.4) | 57 (32.9) | 42 (36.5) | |
| Yes, −10 min | 163 (56.6) | 99 (57.2) | 64 (55.7) | |
| Yes, 10–20 min | 23 (8.0) | 15 (8.7) | 8 (7.0) | |
| Yes, 21–30 min | 1 (0.3) | 0 (0.0) | 1 (0.9) | |
| Yes, +30 min | 2 (0.7) | 2 (1.2) | 0 (0.0) | |
| Cool-down strategies used | 0.305 ** | |||
| Stretching | 122 (64.6) | 80 (69.0) | 42 (57.5) | |
| Electric stimulation | 2 (1.1) | 0 (0.0) | 2 (2.7) | |
| Manual massage | 5 (2.6) | 3 (2.6) | 2 (2.7) | |
| Massage guns | 8 (4.2) | 4 (3.4) | 4 (5.5) | |
| Active recovery | 25 (13.2) | 13 (11.2) | 12 (16.4) | |
| Passive recovery/Rest | 6 (3.2) | 4 (3.4) | 2 (2.7) | |
| Foam roller | 11 (5.8) | 4 (3.4) | 7 (9.6) | |
| Nutrition/Supplementation | 8 (4.2) | 6 (5.2) | 2 (2.7) | |
| Other | 2 (1.1) | 2 (1.7) | 0 (0.0) | |
| Presence and being monitored by a CrossFit® training instructor | 0.226 ** | |||
| No | 7 (2.4) | 2 (1.2) | 5 (4.3) | |
| Yes, and non-monitored | 26 (9.0) | 16 (9.2) | 10 (8.7) | |
| Yes, and monitored | 255 (88.5) | 155 (89.6) | 100 (87.0) | |
| Monitored by a health professional | 0.903 ** | |||
| No | 154 (53.5) | 92 (53.2) | 62 (53.9) | |
| Yes | 134 (46.5) | 81 (46.8) | 53 (46.1) | |
| Practice other sports or physical activity? | 0.891 * | |||
| No | 170 (59.0) | 102 (59.0) | 68 (59.1) | |
| Yes, once per week | 68 (23.6) | 40 (23.1) | 28 (24.3) | |
| Yes, 2 times per week | 27 (9.4) | 16 (9.2) | 11 (9.6) | |
| Yes, 3 times per week | 10 (3.5) | 7 (4.0) | 3 (2.6) | |
| Yes, more than 3 times per week | 13 (4.5) | 8 (4.6) | 5 (4.3) |
| Variable | n (%) |
|---|---|
| N° of injuries | |
| 1 | 56 (48.7) |
| 2 | 40 (34.8) |
| 3 | 12 (10.4) |
| 4 | 3 (2.6) |
| 5 | 0 (0.0) |
| +5 | 4 (3.5) |
| Injury localization | |
| Head | 2 (1.7) |
| Cervical Spine | 2 (1.7) |
| Upper Back | 1 (0.9) |
| Thoracic Spine | 1 (0.9) |
| Middle Back | 2 (1.7) |
| Chest/Ribs | 2 (1.7) |
| Lower Back | 10 (8.7) |
| Lumbar Spine | 3 (2.6) |
| Shoulder | 53 (46.1) |
| Elbow | 9 (7.8) |
| Forearm (posterior) | 1 (0.9) |
| Wrist | 2 (1.7) |
| Hand/Fingers | 1 (0.9) |
| Pelvis/Groin | 1 (0.9) |
| Thigh (anterior) | 2 (1.7) |
| Thigh (posterior) | 1 (1.7) |
| Knee | 13 (11.3) |
| Leg (anterior) | 2 (1.7) |
| Leg (posterior) | 1 (0.9) |
| Ankle | 1 (0.9) |
| Foot/Fingers | 4 (3.5) |
| Other | 1 (0.9) |
| Injury type | |
| Bursitis | 3 (2.6) |
| Concussion | 1 (0.9) |
| Organ Trauma | 1 (0.9) |
| Laceration/Abrasion/Bleeding | 3 (2.6) |
| Joint Injury | 9 (7.8) |
| Fascial Injury | 4 (3.5) |
| Ligamentous Injury | 5 (4.3) |
| Meniscal Injury | 2 (1.7) |
| Muscular Injury | 32 (27.8) |
| Bone Injury | 4 (3.5) |
| Tendon Injury | 47 (40.9) |
| Pain | 1 (0.9) |
| Other | 3 (2.6) |
| Injury occurrence situation | |
| Warm-up (training) | 5 (4.3) |
| Cool-down (training) | 6 (5.2) |
| During training | 96 (83.5) |
| During competition | 8 (7.0) |
| Injury CrossFit® Training exercise | |
| Endurance | 4 (3.5) |
| Gymnastics | 35 (30.4) |
| Olympic Lifting | 24 (20.9) |
| Power Lifting | 32 (27.8) |
| Other | 20 (17.4) |
| Return-to-sport duration | |
| −1 week | 28 (24.3) |
| 1–2 weeks | 22 (19.1) |
| 3–4 weeks | 21 (18.3) |
| 1–3 months | 25 (21.7) |
| 4–6 months | 10 (8.7) |
| 7–12 months | 7 (6.1) |
| +1 year | 2 (1.7) |
| Injury history | |
| Recurrence | 23 (20.0) |
| First time | 92 (80.0) |
| Injury management | |
| No intervention | 5 (4.3) |
| Active self-management | 11 (9.6) |
| Self-Medication/Supplementation | 4 (3.5) |
| Physiotherapist | 52 (45.2) |
| Physician (surgery) | 5 (4.3) |
| Physician (injection) | 1 (0.9) |
| Physician (medication) | 15 (13.0) |
| Non-conventional medicine | 10 (8.7) |
| Rest | 12 (10.4) |
| Injury Type; Localization | n (%) |
|---|---|
| Bursitis | |
| Shoulder | 3 (100) |
| Concussion | |
| Head | 1 (100) |
| Organ Trauma | |
| Other | 1 (100) |
| Laceration/Abrasion/Bleeding | |
| Head | 1 (33.3) |
| Shoulder | 1 (33.3) |
| Leg (posterior) | 1 (33.3) |
| Joint | |
| Cervical Spine | 1 (11.1) |
| Lumbar Spine | 1 (11.1) |
| Shoulder | 3 (33.3) |
| Elbow | 3 (33.3) |
| Wrist | 1 (11.1) |
| Fascial | |
| Shoulder | 1 (25) |
| Knee | 1 (25) |
| Foot/Fingers | 2 (50) |
| Ligamentous | |
| Shoulder | 2 (40) |
| Hand/Fingers | 1 (20) |
| Knee | 2 (40) |
| Meniscal | |
| Knee | 2 (100) |
| Muscular | |
| Upper Back | 1 (3.1) |
| Middle Back | 2 (6.3) |
| Chest/Ribs | 1 (3.1) |
| Lower Back | 9 (28.1) |
| Shoulder | 13 (40.6) |
| Forearm (posterior) | 1 (3.1) |
| Thigh (anterior) | 1 (3.1) |
| Thigh (posterior) | 1 (3.1) |
| Leg (anterior) | 2 (6.3) |
| Foot/Fingers | 1 (3.1) |
| Bone | |
| Chest/Ribs | 1 (20) |
| Lumbar Spine | 1 (20) |
| Thigh (anterior) | 1 (20) |
| Knee | 1 (20) |
| Tendon | |
| Lower Back | 1 (2.1) |
| Shoulder | 29 (61.7) |
| Elbow | 6 (12.8) |
| Wrist | 1 (2.1) |
| Pelvis/Groin | 1 (2.1) |
| Knee | 7 (14.9) |
| Ankle | 1 (2.1) |
| Foot/Fingers | 1 (2.1) |
| Pain | |
| Cervical Spine | 1 (100) |
| Other | |
| Thoracic Spine | 1 (33.3) |
| Lumbar Spine | 1 (33.3) |
| Shoulder | 1 (33.3) |
| Injury Localization | Situation | Exercise | Return-to-Sport | Clinical History | Management | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Warm-Up (Training) | Cool-Down (Training) | During Training | During Competition | Endurance | Gymnastic | Olympic Lifting | Power Lifting | Other | −1 Week | 1–2 Weeks | 3–4 Weeks | 1–3 Months | 4–6 Months | 7–12 Months | + 1 Year | Recurrence | First Time | No Intervention | Self-Management | Self-Medication | Physio therapist | Physician (Surgery) | Physician (Injection) | Physician (Medication) | Non-Conventional Medicine | Rest | |
| Head | - | - | 2 | - | - | 1 | - | 1 | - | - | - | 1 | 1 | - | - | - | - | 2 | - | - | - | - | - | - | 1 | - | 1 |
| Cervical Spine | - | - | 2 | - | - | - | 1 | - | 1 | - | - | 1 | 1 | - | - | - | - | 2 | - | - | - | 1 | - | - | - | - | 1 |
| Upper Back | - | - | 1 | - | - | - | - | 1 | - | - | 1 | - | - | - | - | - | 1 | - | - | - | - | 1 | - | - | - | - | - |
| Thoracic Spine | - | - | 1 | - | - | - | - | 1 | - | - | - | - | 1 | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | - |
| Middle Back | - | 1 | 1 | - | - | 1 | - | 1 | - | 1 | 1 | - | - | - | - | - | 1 | 1 | - | - | 1 | - | - | - | - | 1 | - |
| Chest/Ribs | - | - | 2 | - | - | 2 | - | - | - | - | 1 | - | 1 | - | - | - | - | 2 | - | - | 1 | 1 | - | - | - | - | - |
| Lower Back | - | - | 10 | - | - | - | 2 | 8 | - | 3 | 4 | 2 | 1 | - | - | - | 1 | 9 | - | 4 | - | 1 | - | - | 3 | - | 2 |
| Lumbar Spine | 1 | - | 2 | - | - | - | 2 | - | 1 | - | - | 1 | 1 | - | 1 | - | - | 3 | - | - | - | 1 | - | - | 2 | - | - |
| Shoulder | 2 | 1 | 43 | 7 | - | 26 | 11 | 9 | 7 | 16 | 9 | 12 | 6 | 6 | 3 | 1 | 17 | 36 | 3 | 3 | 2 | 25 | 3 | 1 | 4 | 8 | 4 |
| Elbow | - | - | 8 | 1 | - | 1 | 6 | 1 | 1 | 1 | 2 | 2 | 3 | 1 | - | - | 1 | 8 | - | 2 | - | 6 | - | - | 1 | - | - |
| Forearm (posterior) | - | 1 | - | - | - | - | - | 1 | - | 1 | - | - | - | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | - |
| Wrist | - | - | 2 | - | - | 1 | - | 1 | - | - | - | - | 2 | - | - | - | - | 2 | - | - | - | 2 | - | - | - | - | - |
| Hand/Fingers | - | - | 1 | - | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | 1 | - | - | - | - | - | - | - | - | 1 |
| Pelvis/Groin | - | - | 1 | - | - | - | - | 1 | - | - | - | - | - | - | 1 | - | - | 1 | - | - | - | 1 | - | - | - | - | - |
| Thigh (anterior) | - | - | 2 | - | 1 | 1 | - | - | - | - | - | - | 1 | - | 1 | - | - | 2 | - | - | - | 1 | - | - | - | - | 1 |
| Thigh (posterior) | - | - | 1 | - | 1 | - | - | - | - | - | - | - | 1 | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | - |
| Knee | 2 | - | 11 | - | 2 | - | 2 | 5 | 4 | 2 | 3 | 1 | 4 | 1 | 1 | 1 | 1 | 12 | - | 1 | - | 6 | 2 | - | 2 | - | 2 |
| Lower Leg (anterior) | - | - | 2 | - | - | - | - | 1 | 1 | 1 | - | - | 1 | - | - | - | 1 | 1 | 2 | - | - | - | - | - | - | - | - |
| Lower Leg (posterior) | - | 1 | - | - | - | - | - | 1 | - | 1 | - | - | - | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | - |
| Ankle | - | - | 1 | - | - | - | - | - | 1 | 1 | - | - | - | - | - | - | - | 1 | - | 1 | - | - | - | - | - | - | - |
| Foot/Fingers | - | 2 | 2 | - | - | 2 | - | - | 2 | 1 | 1 | - | - | 2 | - | - | - | 4 | - | - | - | 2 | - | - | 1 | 1 | - |
| Other | - | - | 1 | - | - | - | - | - | 1 | - | - | 1 | - | - | - | - | - | 1 | - | - | - | - | - | - | 1 | - | - |
| Injury Type | |||||||||||||||||||||||||||
| Bursitis | 1 | - | 2 | - | - | 2 | - | 1 | - | 1 | - | - | - | 1 | - | 1 | - | 3 | - | - | - | 3 | - | - | - | - | - |
| Concussion | - | - | 1 | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | - | 1 | - | - | - | - | - | - | 1 | - | - |
| Organ | - | - | 1 | - | - | - | - | - | 1 | - | - | 1 | - | - | - | - | - | 1 | - | - | - | - | - | - | 1 | - | - |
| Laceration | - | 1 | 2 | - | - | 1 | - | 1 | 1 | 2 | - | - | 1 | - | - | - | - | 3 | 1 | - | - | 1 | - | - | - | - | 1 |
| Joint | 1 | - | 6 | 2 | - | 1 | 3 | 2 | 3 | 1 | 2 | 2 | 3 | 1 | - | - | - | 9 | - | 1 | - | 3 | - | 1 | 2 | 1 | 1 |
| Fascial | - | 1 | 3 | - | - | 1 | - | 2 | 1 | 2 | 1 | - | 1 | - | - | - | - | 4 | - | - | - | 1 | 1 | - | 2 | - | - |
| Ligamentous | 2 | - | 2 | 1 | 1 | 2 | - | - | 2 | - | 1 | - | 3 | - | 1 | - | - | 5 | - | 1 | - | 2 | 1 | - | - | - | 1 |
| Meniscal | - | - | 2 | - | 1 | - | - | 1 | - | - | - | - | 2 | - | - | - | - | 2 | - | - | - | - | 2 | - | - | - | - |
| Muscular | - | 3 | 28 | 1 | 1 | 9 | 5 | 15 | 2 | 12 | 9 | 2 | 5 | 4 | - | - | 11 | 21 | 3 | 3 | 1 | 15 | - | - | 3 | 4 | 3 |
| Bone | - | - | 4 | - | 1 | 1 | 1 | 1 | - | - | - | 1 | 2 | - | 1 | - | - | 4 | - | - | 1 | 1 | - | - | 1 | - | 1 |
| Tendon | 1 | - | 42 | 4 | - | 18 | 14 | 7 | 8 | 10 | 9 | 12 | 7 | 4 | 4 | 1 | 11 | 36 | 1 | 6 | 2 | 23 | 1 | - | 5 | 5 | 4 |
| Pain | - | - | 1 | - | - | - | - | - | 1 | - | - | 1 | - | - | - | - | - | 1 | - | - | - | 1 | - | - | - | - | - |
| Other | - | 1 | 2 | - | - | - | 1 | 1 | 1 | - | - | 1 | 1 | - | 1 | - | 1 | 2 | - | - | - | 2 | - | - | - | - | 1 |
| Variables | Age | Sex | Body Weight | Body Height | Professional Physical Activity Level | Sport Background | Years Practicing Cross | Cross Level | Weekly Cross Practice | Cross Practice Duration | Annual Cross Competitions | Perform Warm-Up | Perform Cool-Down | Cool-Down Strategies | Presence and Monitored by an Instructor | N° Injuries Cross-Related | Injury Localization | Injury Cross Activity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Body weight | - | 0.558 ** | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Body height | - | 0.723 ** | 0.605 ** | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Years practicing CrossFit® | 0.332 ** | - | - | - | 0.256 ** | - | - | - | - | - | - | - | - | - | - | - | - | - |
| CrossFit® Level | - | - | - | - | 0.379 ** | 0.274 ** | 0.194 * | - | - | - | - | - | - | - | - | - | - | - |
| Weekly CrossFit® practice | - | - | - | - | - | - | - | 0.348 ** | - | - | - | - | - | - | - | - | - | - |
| CrossFit® practice duration | - | - | - | - | - | - | 0.196 * | 0.284 ** | 0.257 ** | - | - | - | - | - | - | - | - | - |
| Annual CrossFit® competitions | - | - | - | - | 0.365 ** | 0.289 ** | 0.207 * | 0.955 ** | 0.314 ** | 0.295 ** | - | - | - | - | - | - | - | - |
| Perform warm-up | - | - | - | - | 0.205 * | - | - | - | 0.187 * | 0.333 ** | - | - | - | - | - | - | - | - |
| Perform cool-down | 0.227 * | - | - | - | 0.198 * | - | - | - | - | - | - | 0.368 ** | - | - | - | - | - | - |
| Cool-down strategies | - | - | - | - | - | - | - | 0.229 * | - | - | 0.260 ** | 0.269 ** | 0.857 ** | - | - | - | - | - |
| Presence and monitored by an instructor | - | - | - | - | - | −0.193 * | - | - | - | - | - | - | - | - | - | - | - | - |
| Monitored by a health professional | - | −0.219 * | - | −0.225 * | - | - | - | - | - | - | - | - | 0.210 * | 0.209 * | - | - | - | - |
| Practice other sports plus CrossFit® | - | 0.191 * | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| N° injuries CrossFit®-related | 0.202 * | - | 0.221 * | - | 0.274 ** | - | 0.454 ** | - | - | - | - | - | - | - | −0.190 * | - | - | - |
| Injury type | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Injury occurrence situation | - | - | - | - | 0.186 * | - | - | 0.323 ** | - | - | 0.337 ** | - | - | - | - | - | −0.208 * | - |
| Injury CrossFit® activity | - | - | - | - | −0.249 ** | - | −0.246 ** | - | - | - | - | - | - | - | - | −0.203 * | 0.248 ** | - |
| Return-to-sport duration | - | - | - | - | - | - | 0.190 * | - | - | - | - | - | - | - | - | - | - | −0.191 * |
| Injury (Present) | Factor—Level | Odds Ratio (95% CI) | p | R2 a |
|---|---|---|---|---|
| Tendon | ||||
| Sex | 0.012 | 0.075 | ||
| Male | 2.680 [1.243; 5.777] | |||
| Female | Reference | |||
| Sport Background | 0.043 | 0.053 | ||
| Yes | 3.024 [1.035; 8.837] | |||
| No | Reference | |||
| Muscular | ||||
| Sport Background | 0.001 | 0.129 | ||
| No | 4.995 [1.900; 13.132] | |||
| Yes | Reference | |||
| Shoulder | ||||
| Years Practicing Cross | 0.045 | 0.104 | ||
| 1–3 | 3.014 [0.737; 12.325] | 0.125 | ||
| 4–6 | 7.222 [1.703; 30.637] | 0.007 | ||
| 7–≥10 | 4.333 [1.009; 18.615] | 0.049 | ||
| −1 | Reference | |||
| Knee | ||||
| Body Weight (Kg) | 0.023 | 0.102 | ||
| 75–≥100 | 4.762 [1.236; 18.353] | |||
| ≤50–74 | Reference |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, R.M.; Fernandes, L.G.; Minghelli, B.; Feito, Y.; Sampaio, A.R.; Pimenta, N. Sport-Related Injuries in Portuguese CrossFit® Practitioners and Their Characteristics. Muscles 2025, 4, 2. https://doi.org/10.3390/muscles4010002
Ferreira RM, Fernandes LG, Minghelli B, Feito Y, Sampaio AR, Pimenta N. Sport-Related Injuries in Portuguese CrossFit® Practitioners and Their Characteristics. Muscles. 2025; 4(1):2. https://doi.org/10.3390/muscles4010002
Chicago/Turabian StyleFerreira, Ricardo Maia, Luís Gonçalves Fernandes, Beatriz Minghelli, Yuri Feito, António Rodrigues Sampaio, and Nuno Pimenta. 2025. "Sport-Related Injuries in Portuguese CrossFit® Practitioners and Their Characteristics" Muscles 4, no. 1: 2. https://doi.org/10.3390/muscles4010002
APA StyleFerreira, R. M., Fernandes, L. G., Minghelli, B., Feito, Y., Sampaio, A. R., & Pimenta, N. (2025). Sport-Related Injuries in Portuguese CrossFit® Practitioners and Their Characteristics. Muscles, 4(1), 2. https://doi.org/10.3390/muscles4010002