
Hip Muscle Strength Ratios Predicting Groin Injury in Male Soccer Players Using Machine Learning and Multivariate Analysis—A Prospective Cohort Study

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection and Injury Data Registration
2.3. Testing Protocol
2.4. Injury Data Registration
2.5. Statistical Analysis
2.6. Development of the k-NN Model
2.7. Model Evaluation
3. Results
3.1. Descriptive Characteristics
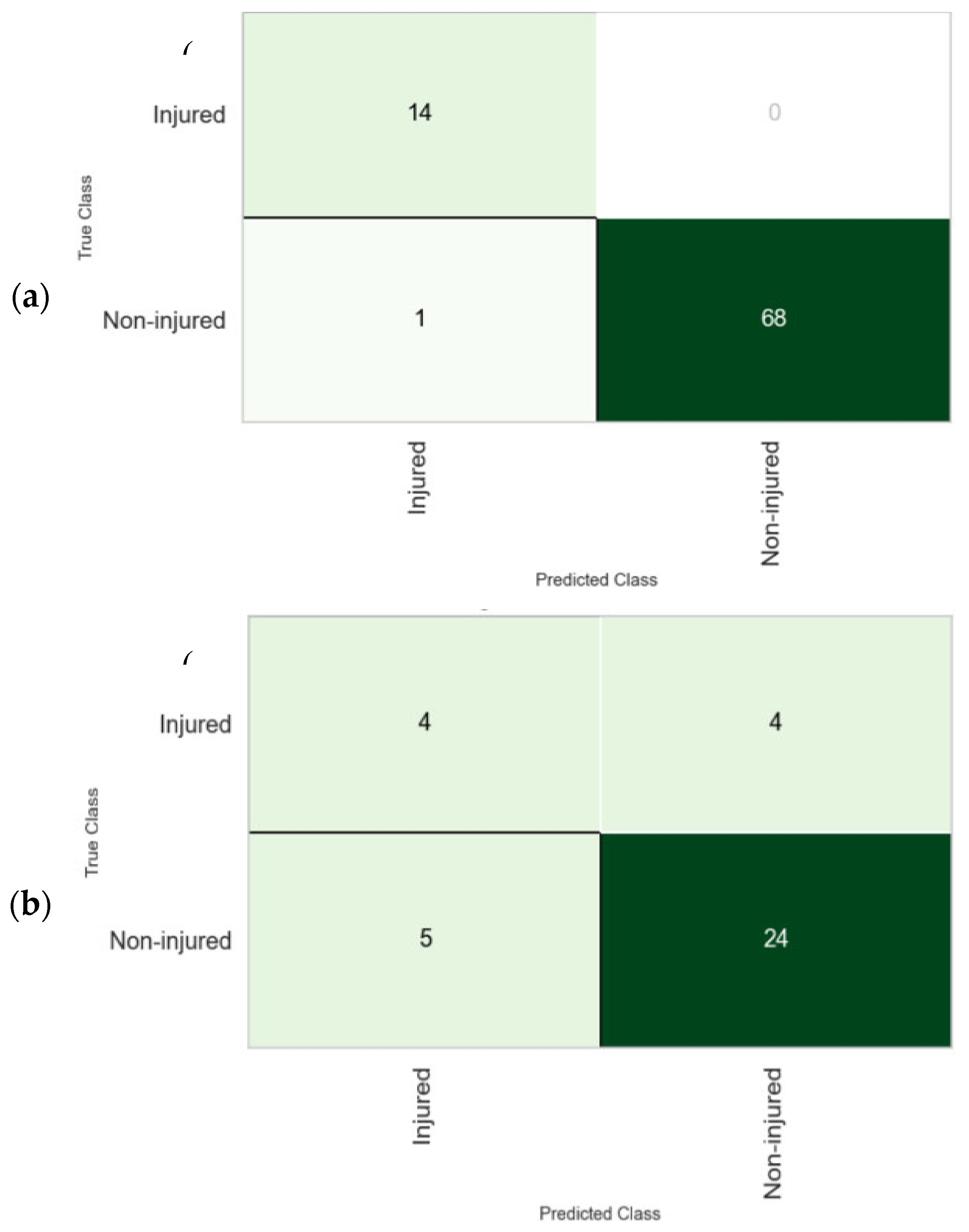
3.2. The k-NN Model
3.3. The Regression Model
4. Discussion
4.1. Hip Muscle Strength Measurements and Ratios as Risk Factors for Groin Injury
4.2. Groin Injury Mechanism
4.3. The Value of Machine Learning in Injury Prediction
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Whittaker, J.L.; Small, C.; Maffey, L.; Emery, C.A. Risk factors for groin injury in sport: An updated systematic review. Br. J. Sports Med. 2015, 49, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Intrinsic Risk Factors for Groin Injuries among Male Soccer Players. Am. J. Sports Med. 2010, 38, 2051–2057. [Google Scholar] [CrossRef] [PubMed]
- Kekelekis, A.; Clemente, F.M.; Kellis, E. Muscle injury characteristics and incidence rates in men’s amateur soccer: A one season prospective study. Res. Sports Med. 2022, 32, 411–424. [Google Scholar] [CrossRef]
- Serner, A.; Mosler, A.B.; Tol, J.L.; Bahr, R.; Weir, A. Mechanisms of acute adductor longus injuries in male football players: A systematic visual video analysis. Br. J. Sports Med. 2019, 53, 158–164. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gomez, J.A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Kekelekis, A.; Kounali, Z.; Kofotolis, N.; Clemente, F.M.; Kellis, E. Epidemiology of Injuries in Amateur Male Soccer Players: A Prospective One-Year Study. Healthcare 2023, 11, 352. [Google Scholar] [CrossRef]
- Mosler, A.B.; Weir, A.; Eirale, C.; Farooq, A.; Thorborg, K.; Whiteley, R.J.; Hölmich, P.; Crossley, K.M. Epidemiology of time loss groin injuries in a men’s professional football league: A 2-year prospective study of 17 clubs and 606 players. Br. J. Sports Med. 2018, 52, 292–297. [Google Scholar] [CrossRef]
- Langhout, R.; Tak, I.; van Beijsterveldt, A.-M.; Ricken, M.; Weir, A.; Barendrecht, M.; Kerkhoffs, G.; Stubbe, J. Risk Factors for Groin Injury and Groin Symptoms in Elite-Level Soccer Players: A Cohort Study in the Dutch Professional Leagues. J. Orthop. Sports Phys. Ther. 2018, 48, 704–712. [Google Scholar] [CrossRef]
- Moreno-Pérez, V.; Travassos, B.; Calado, A.; Gonzalo-Skok, O.; Del Coso, J.; Mendez-Villanueva, A. Adductor squeeze test and groin injuries in elite football players: A prospective study. Phys. Ther. Sport 2019, 37, 54–59. [Google Scholar] [CrossRef]
- Bourne, M.N.; Williams, M.; Jackson, J.; Williams, K.L.; Timmins, R.G.; Pizzari, T. Preseason Hip/Groin Strength and HAGOS Scores Are Associated With Subsequent Injury in Professional Male Soccer Players. J. Orthop. Sports Phys. Ther. 2020, 50, 234–242. [Google Scholar] [CrossRef]
- Markovic, G.; Šarabon, N.; Pausic, J.; Hadžić, V. Adductor Muscles Strength and Strength Asymmetry as Risk Factors for Groin Injuries among Professional Soccer Players: A Prospective Study. Int. J. Environ. Res. Public Health 2020, 17, 4946. [Google Scholar] [CrossRef]
- Belhaj, K.; Meftah, S.; Mahir, L.; Lmidmani, F.; Elfatimi, A. Isokinetic imbalance of adductor–abductor hip muscles in professional soccer players with chronic adductor-related groin pain. Eur. J. Sport Sci. 2016, 16, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Schoffl, J.; Dooley, K.; Miller, P.; Miller, J.; Snodgrass, S.J. Factors Associated with Hip and Groin Pain in Elite Youth Football Players: A Cohort Study. Sports Med.-Open 2021, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Tyler, T.F.; Nicholas, S.J.; Campbell, R.J.; McHugh, M.P. The Association of Hip Strength and Flexibility with the Incidence of Adductor Muscle Strains in Professional Ice Hockey Players. Am. J. Sports Med. 2001, 29, 124–128. [Google Scholar] [CrossRef]
- Claudino, J.G.; de Oliveira Capanema, D.; De Souza, T.V.; Serrão, J.C.; Pereira, A.C.M.; Nassis, G.P. Current Approaches to the Use of Artificial Intelligence for Injury Risk Assessment and Performance Prediction in Team Sports: A Systematic Review. Sports Med.-Open 2019, 5, 28. [Google Scholar] [CrossRef]
- Rico-González, M.; Pino-Ortega, J.; Méndez, A.; Clemente, F.; Baca, A. Machine learning application in soccer: A systematic review. Biol. Sport 2023, 40, 249–263. [Google Scholar] [CrossRef]
- Collins, G.S.; Moons, K.G.M. Reporting of artificial intelligence prediction models. Lancet 2019, 393, 1577–1579. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ayala, F.; Puerta, J.M.; Croix, M.B.A.D.S.; Vera-Garcia, F.J.; Hernández-Sánchez, S.; Ruiz-Pérez, I.; Myer, G.D. A Preventive Model for Muscle Injuries. Med. Sci. Sports Exerc. 2018, 50, 915–927. [Google Scholar] [CrossRef]
- Ayala, F.; López-Valenciano, A.; Martín, J.A.G.; Croix, M.D.S.; Vera-Garcia, F.J.; García-Vaquero, M.D.P.; Ruiz-Pérez, I.; Myer, G.D. A Preventive Model for Hamstring Injuries in Professional Soccer: Learning Algorithms. Int. J. Sports Med. 2019, 40, 344–353. [Google Scholar] [CrossRef]
- Rommers, N.; Rössler, R.; Verhagen, E.; Vandecasteele, F.; Verstockt, S.; Vaeyens, R.; Lenoir, M.; D’hondt, E.; Witvrouw, E. A Machine Learning Approach to Assess Injury Risk in Elite Youth Football Players. Med. Sci. Sports Exerc. 2020, 52, 1745–1751. [Google Scholar] [CrossRef]
- Luu, B.C.; Wright, A.L.; Haeberle, H.S.; Karnuta, J.M.; Schickendantz, M.S.; Makhni, E.C.; Nwachukwu, B.U.; Williams, R.J.; Ramkumar, P.N. Machine Learning Outperforms Logistic Regression Analysis to Predict Next-Season NHL Player Injury: An Analysis of 2322 Players from 2007 to 2017. Orthop. J. Sports Med. 2020, 8, 1–2. [Google Scholar] [CrossRef]
- Oliver, J.L.; Ayala, F.; Croix, M.B.D.S.; Lloyd, R.S.; Myer, G.D.; Read, P.J. Using machine learning to improve our understanding of injury risk and prediction in elite male youth football players. J. Sci. Med. Sport 2020, 23, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, J.D.; Cormack, S.J.; Whiteley, R.; Williams, M.D.; Timmins, R.G.; Opar, D.A. Modeling the Risk of Team Sport Injuries: A Narrative Review of Different Statistical Approaches. Front. Physiol. 2019, 10, 829. [Google Scholar] [CrossRef]
- Jauhiainen, S.; Kauppi, J.-P.; Krosshaug, T.; Bahr, R.; Bartsch, J.; Äyrämö, S. Predicting ACL Injury Using Machine Learning on Data From an Extensive Screening Test Battery of 880 Female Elite Athletes. Am. J. Sports Med. 2022, 50, 2917–2924. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.-L.; Chaouachi, A.; Chamari, K.; Dellal, A.; Wisloff, U. Effect of Preseason Concurrent Muscular Strength and High-Intensity Interval Training in Professional Soccer Players. J. Strength Cond. Res. 2010, 24, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef] [PubMed]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Nielsen, M.F.; Thorborg, K.; Krommes, K.; Thornton, K.B.; Hölmich, P.; Peñalver, J.J.; Ishøi, L. Hip adduction strength and provoked groin pain: A comparison of long-lever squeeze testing using the ForceFrame and the Copenhagen 5-Second-Squeeze test. Phys. Ther. Sport 2022, 55, 28–36. [Google Scholar] [CrossRef]
- Thorborg, K.; Couppé, C.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Eccentric hip adduction and abduction strength in elite soccer players and matched controls: A cross-sectional study. Br. J. Sports Med. 2011, 45, 10–13. [Google Scholar] [CrossRef]
- Thorborg, K.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand. J. Med. Sci. Sports 2010, 20, 493–501. [Google Scholar] [CrossRef]
- Reurink, G.; Goudswaard, G.J.; Moen, M.H.; Tol, J.L.; Verhaar, J.A.; Weir, A. Strength Measurements in Acute Hamstring Injuries: Intertester Reliability and Prognostic Value of Handheld Dynamometry. J. Orthop. Sports Phys. Ther. 2016, 46, 689–696. [Google Scholar] [CrossRef]
- de Almeida, M.B.; Oliveira, C.; Ornelas, G.; Soares, T.; Souto, J.; Póvoa, A.R.; Ferreira, L.M.A.; Ricci-Vitor, A.L. Intra-Rater and Inter-Rater Reliability of the Kinvent Hand-Held Dynamometer in Young Adults. Med. Sci. Forum 2023, 22, 12. [Google Scholar] [CrossRef]
- Olds, M.; McLaine, S.; Magni, N. Validity and Reliability of the Kinvent Handheld Dynamometer in the Athletic Shoulder Test. J. Sport Rehabil. 2023, 32, 764–771. [Google Scholar] [CrossRef] [PubMed]
- van der Ploeg, R.J.; Oosterhuis, H.J. The “make/break test” as a diagnostic tool in functional weakness. J. Neurol. Neurosurg. Psychiatry 1991, 54, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Sisto, S.A.; Dyson-Hudson, T. Dynamometry testing in spinal cord injury. J. Rehabilit. Res. Dev. 2007, 44, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Weir, A.; Brukner, P.; Delahunt, E.; Ekstrand, J.; Griffin, D.; Khan, K.M.; Lovell, G.; Meyers, W.C.; Muschaweck, U.; Orchard, J.; et al. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br. J. Sports Med. 2015, 49, 768–774. [Google Scholar] [CrossRef]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sports 2006, 16, 83–92. [Google Scholar] [CrossRef]
- Musa, R.M.; Majeed, A.A.; Taha, Z.; Abdullah, M.; Maliki, A.H.M.; Kosni, N.A. The application of Artificial Neural Network and k-Nearest Neighbour classification models in the scouting of high-performance archers from a selected fitness and motor skill performance parameters. Sci. Sports 2019, 34, e241–e249. [Google Scholar] [CrossRef]
- Musa, R.M.; Majeed, A.P.P.A.; Taha, Z.; Chang, S.W.; Nasir, A.F.A.; Abdullah, M.R. A machine learning approach of predicting high potential archers by means of physical fitness indicators. PLoS ONE 2019, 14, e0209638. [Google Scholar] [CrossRef]
- Trost, S.G.; Zheng, Y.; Wong, W.-K. Machine learning for activity recognition: Hip versus wrist data. Physiol. Meas. 2014, 35, 2183–2189. [Google Scholar] [CrossRef]
- Taha, Z.; Musa, R.M.; Majeed, A.P.P.A.; Abdullah, M.R.; Abdullah, M.A.; Hassan, M.H.A.; Khalil, Z. The employment of Support Vector Machine to classify high and low performance archers based on bio-physiological variables. IOP Conf. Ser. Mater. Sci. Eng. 2018, 342, 012020. [Google Scholar] [CrossRef]
- Bakken, A.; Targett, S.; Bere, T.; Eirale, C.; Farooq, A.; Mosler, A.B.; Tol, J.L.; Whiteley, R.; Khan, K.M.; Bahr, R. Muscle Strength Is a Poor Screening Test for Predicting Lower Extremity Injuries in Professional Male Soccer Players: A 2-Year Prospective Cohort Study. Am. J. Sports Med. 2018, 46, 1481–1491. [Google Scholar] [CrossRef]
- Moreno-Pérez, V.; Peñaranda, M.; Soler, A.; Samanes, A.L.; Aagaard, P.; Del Coso, J. Effects of Whole-Season Training and Match-Play on Hip Adductor and Abductor Muscle Strength in Soccer Players: A Pilot Study. Sports Health A Multidiscip. Approach 2021, 14, 912–919. [Google Scholar] [CrossRef]
- Dupré, T.; Potthast, W. Are sprint accelerations related to groin injuries? A biomechanical analysis of adolescent soccer players. Sports Biomech. 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Dupré, T.; Tryba, J.; Potthast, W. Muscle activity of cutting manoeuvres and soccer inside passing suggests an increased groin injury risk during these movements. Sci. Rep. 2021, 11, 7223. [Google Scholar] [CrossRef] [PubMed]
- Dupré, T.; Funken, J.; Müller, R.; Mortensen, K.R.L.; Lysdal, F.G.; Braun, M.; Krahl, H.; Potthast, W. Does inside passing contribute to the high incidence of groin injuries in soccer? A biomechanical analysis. J. Sports Sci. 2018, 36, 1827–1835. [Google Scholar] [CrossRef]
- Charnock, B.L.; Lewis, C.L.; Garrett, W.E.; Queen, R.M. Adductor longus mechanics during the maximal effort soccer kick. Sports Biomech. 2009, 8, 223–234. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H. Risk factors for groin injuries in hockey. Med. Sci. Sports Exerc. 2000, 33, 1423–1433. [Google Scholar] [CrossRef] [PubMed]
- Kellis, E.; Katis, A. Biomechanical characteristics and determinants of instep soccer kick. J. Sports Sci. Med. 2007, 6, 154–165. [Google Scholar]
- Esteve, E.; Rathleff, M.S.; Vicens-Bordas, J.; Clausen, M.B.; Hölmich, P.; Sala, L.; Thorborg, K. Preseason Adductor Squeeze Strength in 303 Spanish Male Soccer Athletes: A Cross-sectional Study. Orthop. J. Sports Med. 2018, 6, 1–8. [Google Scholar] [CrossRef]
- DeLang, M.D.; Garrison, J.C.; Hannon, J.P.; McGovern, R.P.; Christoforetti, J.; Thorborg, K. Short and long lever adductor squeeze strength values in 100 elite youth soccer players: Does age and previous groin pain matter? Phys. Ther. Sport 2020, 46, 243–248. [Google Scholar] [CrossRef]
- Liew, B.X.W.; Kovacs, F.M.; Rügamer, D.; Royuela, A. Machine learning versus logistic regression for prognostic modelling in individuals with non-specific neck pain. Eur. Spine J. 2022, 31, 2082–2091. [Google Scholar] [CrossRef] [PubMed]
- Florencio, L.L.; Martins, J.; da Silva, M.R.; da Silva, J.R.; Bellizzi, G.L.; Bevilaqua-Grossi, D. Knee and hip strength measurements obtained by a hand-held dynamometer stabilized by a belt and an examiner demonstrate parallel reliability but not agreement. Phys. Ther. Sport 2019, 38, 115–122. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mechanism of Groin Injury | N |
|---|---|
| Change of direction (CoD) | 12 |
| Acceleration | 4 |
| Stretching | 3 |
| Kicking | 2 |
| Inside pass | 2 |
| Decceleration | 2 |
| Total | 25 |
| Variable | Mean-SD | |
|---|---|---|
| Injured (n = 98) | Non-Injured (n = 22) | |
| ADD D | 25.40 ± 7.56 | 26.74 ± 7.16 |
| ADD ND | 26.02 ± 7.51 | 24.30 ± 6.01 |
| ABD D | 15.16 ± 5.39 | 17.62 ± 5.22 |
| ABD ND | 13.50 ± 5.20 | 16.29 ± 5.10 |
| HMS D | 24.51 ± 5.60 | 23.99 ± 6.38 |
| HMS ND | 23.55 ± 5.63 | 22.28 ± 6.16 |
| HFL D | 27.26 ± 7.79 | 28.02 ± 6.51 |
| HFL ND | 26.33 ± 6.67 | 26.05 ± 5.96 |
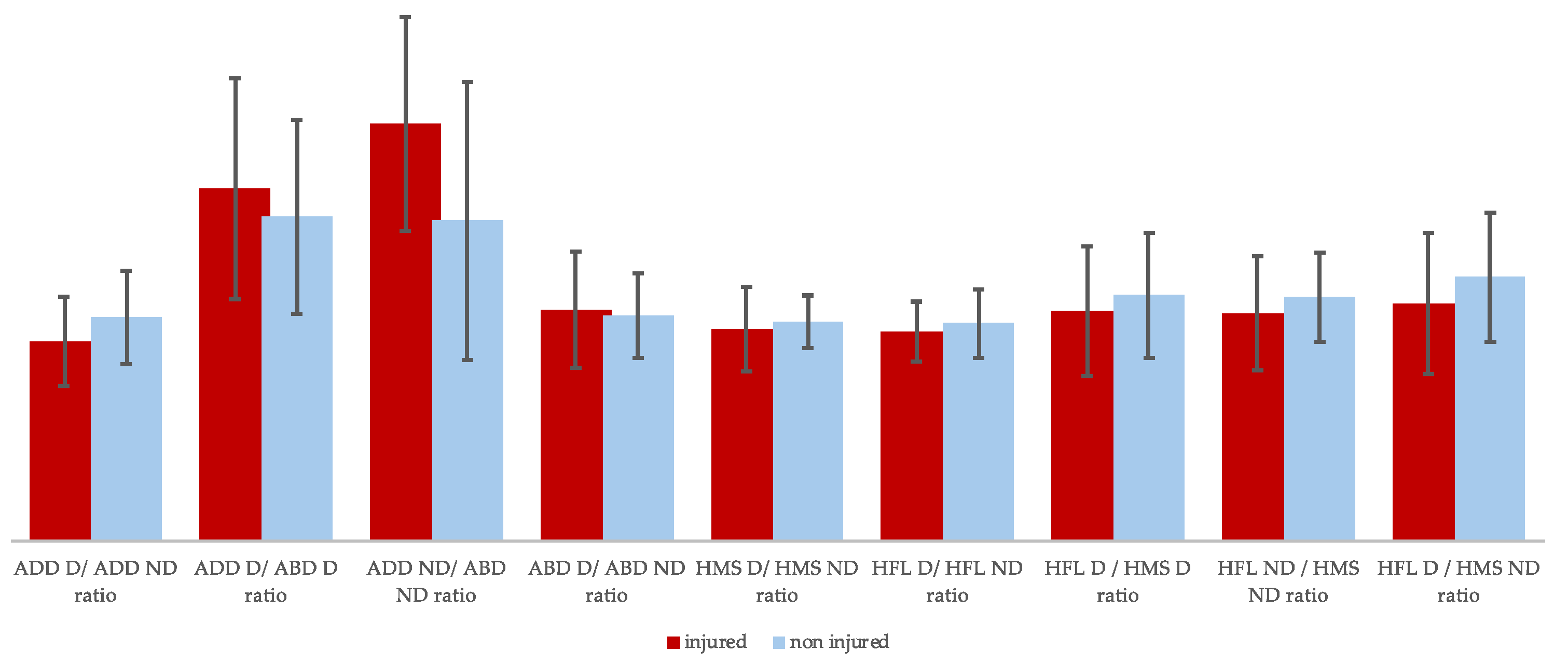
| ADD D/ADD ND ratio | 0.99 ± 0.23 | 1.11 ± 0.22 |
| ADD D/ABD D ratio | 1.75 ± 0.48 | 1.61 ± 0.55 |
| ADD ND/ABD ND ratio | 2.07 ± 0.69 | 1.59 ± 0.53 |
| ABD D/ABD ND ratio | 1.15 ± 0.21 | 1.12 ± 0.29 |
| HMS D/HMS ND ratio | 1.05 ± 0.13 | 1.09 ± 0.21 |
| HFL D/HFL ND ratio | 1.04 ±0.17 | 1.08 ± 0.15 |
| HFL D/HMS D ratio | 1.14 ± 0.31 | 1.22 ± 0.32 |
| HFL D/HMS ND ratio | 1.13 ± 0.22 | 1.21 ± 0.28 |
| HFL ND/HMS ND ratio | 1.18 ±0.32 | 1.31 ± 0.35 |
| Accuracy | AUC | Recall | Prec. | F1 | |
|---|---|---|---|---|---|
| Mean | 0.556 | 0.425 | 0.609 | 0.806 | 0.688 |
| Std | 0.131 | 0.278 | 0.941 | 0.108 | 0.197 |
| 95% Confidence Interval | |||||||
|---|---|---|---|---|---|---|---|
| Variables | B | SE | Z | p | Odds Ratio | Lower | Upper |
| Intercept | 2.5628 | 1.744 | 1.4697 | 0.142 | 12.972 | 0.4253 | 395.618 |
| History | −1.0997 | 0.58 | −1.8952 | 0.050 * | 0.333 | 0.1068 | 1.038 |
| HFL ND/HMS ND ratio | 0.1479 | 1.703 | 0.0869 | 0.931 | 1.159 | 0.0412 | 32.626 |
| HFL D/HMS D ratio | 0.0499 | 1.354 | 0.0368 | 0.971 | 1.051 | 0.0739 | 14.943 |
| HFL D/HMS ND ratio | 1.1717 | 1.55 | 0.7558 | 0.45 | 3.228 | 0.1546 | 67.366 |
| ABD D/ABD ND ratio | 0.4482 | 1.113 | 0.4028 | 0.687 | 1.566 | 0.1768 | 13.862 |
| ADD ND/ABD ND ratio | −1.4362 | 0.448 | −3.2047 | 0.001 * | 0.238 | 0.0988 | 0.572 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kekelekis, A.; Musa, R.M.; Nikolaidis, P.T.; Clemente, F.M.; Kellis, E. Hip Muscle Strength Ratios Predicting Groin Injury in Male Soccer Players Using Machine Learning and Multivariate Analysis—A Prospective Cohort Study. Muscles 2024, 3, 297-309. https://doi.org/10.3390/muscles3030026
Kekelekis A, Musa RM, Nikolaidis PT, Clemente FM, Kellis E. Hip Muscle Strength Ratios Predicting Groin Injury in Male Soccer Players Using Machine Learning and Multivariate Analysis—A Prospective Cohort Study. Muscles. 2024; 3(3):297-309. https://doi.org/10.3390/muscles3030026
Chicago/Turabian StyleKekelekis, Afxentios, Rabiu Muazu Musa, Pantelis T. Nikolaidis, Filipe Manuel Clemente, and Eleftherios Kellis. 2024. "Hip Muscle Strength Ratios Predicting Groin Injury in Male Soccer Players Using Machine Learning and Multivariate Analysis—A Prospective Cohort Study" Muscles 3, no. 3: 297-309. https://doi.org/10.3390/muscles3030026
APA StyleKekelekis, A., Musa, R. M., Nikolaidis, P. T., Clemente, F. M., & Kellis, E. (2024). Hip Muscle Strength Ratios Predicting Groin Injury in Male Soccer Players Using Machine Learning and Multivariate Analysis—A Prospective Cohort Study. Muscles, 3(3), 297-309. https://doi.org/10.3390/muscles3030026