Negative Pressure and Muscle Activity During Discrete Sips from High Resistance Straws

Abstract
:INTRODUCTION
Negative Pressure and Muscle Activity during Discrete Sips from High Resistance Straws
METHOD
Participants
Materials and Procedures
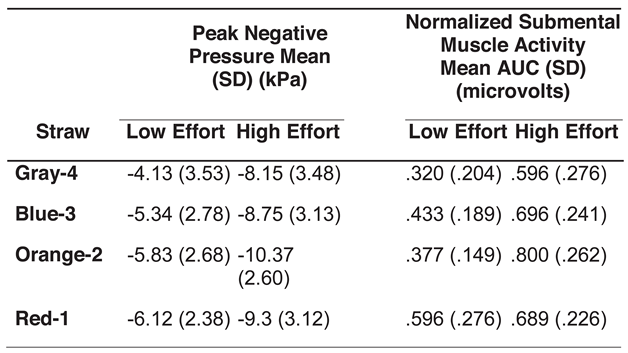
RESULTS
Negative Intra-oral Pressure
Submental Muscle Activity
DISCUSSION
Effects of Straw Diameter
Effects of Effort
Comparison to Previous Findings
Study Limitations
SUMMARY
Conflicts of Interest
References
- Ahlgren, J. 1995. EMG studies of lip and cheek activity in sucking habits. Swedish Dental Journal 19, 3: 95–101. [Google Scholar] [PubMed]
- Geddes, D. T., J. C. Kent, L. R. Mitoulas, and P. E. Hartmann. 2008. Tongue movement and intra-oral vacuum in breastfeeding infants. [Research Support, Non-U.S. Gov't]. Early Human Development 84, 7: 471–477. [Google Scholar] [CrossRef] [PubMed]
- Geddes, D. T., V. S. Sakalidis, A. R. Hepworth, H. L. McClellan, J. C. Kent, C. T. Lai, and P. E. Hartmann. 2012. Tongue movement and intra-oral vacuum of term infants during breastfeeding and feeding from an experimental teat that released milk under vacuum only. [Research Support, Non-U.S. Gov't]. Early Human Development 88, 6: 443–449. [Google Scholar] [CrossRef] [PubMed]
- Mueller, V., R. F. Mucha, and P. Pauli. 2003. Electromyographic activity of the lip muscle as a measure of puffing on a cigarette. Physiol Behav 78, 4–5: 741–749. [Google Scholar] [CrossRef] [PubMed]
- Murray, K. A., C. R. Larson, and J. A. Logemann. 1998. Electromyographic response of the labial muscles during normal liquid swallows using a spoon, a straw, and a cup. Dysphagia 13, 3: 160–166. [Google Scholar] [PubMed]
- Netto, K. J., and A. F. Burnett. 2006. Reliability of normalisation methods for EMG analysis of neck muscles. [Research Support, Non-U.S. Gov't Validation Studies]. Work 26, 2: 123–130. [Google Scholar] [PubMed]
- Nilsson, H., O. Ekberg, and B. Hindfelt. 1995. Oral function test for monitoring suction and swallowing in the neurologic patient. [Case Reports Comparative Study Research Support, Non-U.S. Gov't]. Dysphagia 10, 2: 93–100. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, H., O. Ekberg, R. Olsson, and B. Hindfelt. 1996a. Quantitative aspects of swallowing in an elderly nondysphagic population. [Comparative Study Research Support, Non-U.S. Gov't]. Dysphagia 11, 3: 180–184. [Google Scholar] [PubMed]
- Nilsson, H., O. Ekberg, R. Olsson, and B. Hindfelt. 1996b. Quantitative assessment of oral and pharyngeal function in Parkinson's disease. Dysphagia 11, 2: 144–150. [Google Scholar] [PubMed]
- Nilsson, H., O. Ekberg, R. Olsson, and B. Hindfelt. 1998. Dysphagia in stroke: A prospective study of quantitative aspects of swallowing in dysphagic patients. Dysphagia 13, 1: 32–38. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, H., O. Ekberg, R. Olsson, O. Kjellin, and B. Hindfelt. 1996. Quantitative assessment of swallowing in healthy adults. Dysphagia 11, 2: 110–116. [Google Scholar] [CrossRef] [PubMed]
- Palmer, P. M., E. S. Luschei, D. Jaffe, and T. M. McCulloch. 1999. Contributions of individual muscles to the submental surface electromyogram during swallowing. [Comparative Study Research Support, Non-U.S. Gov't Research Support, U.S. Gov't, P.H.S.]. Journal of Speech, Language, and Hearing Research 42, 6: 1378–1391. [Google Scholar] [PubMed]
- Rosenfeldt-Johnson, S. 2001. Oral motor exercises for speech clarity. Tuscon, AZ: Ravenhawk. [Google Scholar]
- Rushmer, R. F., and J. A. Hendron. 1951. The act of deglutition; a cinefluorographic study. Journal of Applied Physiology 3, 10: 622–630. [Google Scholar] [CrossRef]
- Smead, K. 2010. Strengthening the swallow. http://speech-language-pathology-audiology.advanceweb.com/Editorial/Content/Editorial.aspx?CC=190090.
- Stepp, C. E. 2012. Surface electromyography for speech and swallowing systems: Measurement, analysis, and interpretation. Journal of Speech, Language, and Hearing Research 55, 4: 1232–1246. [Google Scholar] [CrossRef] [PubMed]
- Thexton, A. J., A. W. Crompton, and R. Z. German. 1998. Transition from suckling to drinking at weaning: A kinematic and electromyographic study in miniature pigs. [Research Support, U.S. Gov't, P.H.S.]. Journal of Experimental Zoology 280, 5: 327–343. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
 |
 |
© 2013 by the authors. 2013 Heather M. Clark, Natalia Shelton.
Share and Cite
Clark, H.M.; Shelton, N. Negative Pressure and Muscle Activity During Discrete Sips from High Resistance Straws. Int. J. Orofac. Myol. Myofunct. Ther. 2013, 39, 4-11. https://doi.org/10.52010/ijom.2013.39.1.1
Clark HM, Shelton N. Negative Pressure and Muscle Activity During Discrete Sips from High Resistance Straws. International Journal of Orofacial Myology and Myofunctional Therapy. 2013; 39(1):4-11. https://doi.org/10.52010/ijom.2013.39.1.1
Chicago/Turabian StyleClark, Heather M., and Natalia Shelton. 2013. "Negative Pressure and Muscle Activity During Discrete Sips from High Resistance Straws" International Journal of Orofacial Myology and Myofunctional Therapy 39, no. 1: 4-11. https://doi.org/10.52010/ijom.2013.39.1.1
APA StyleClark, H. M., & Shelton, N. (2013). Negative Pressure and Muscle Activity During Discrete Sips from High Resistance Straws. International Journal of Orofacial Myology and Myofunctional Therapy, 39(1), 4-11. https://doi.org/10.52010/ijom.2013.39.1.1