Lingual Frenulum Protocol

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:INTRODUCTION
METHODS
RESULTS
DISCUSSION
CONCLUSION
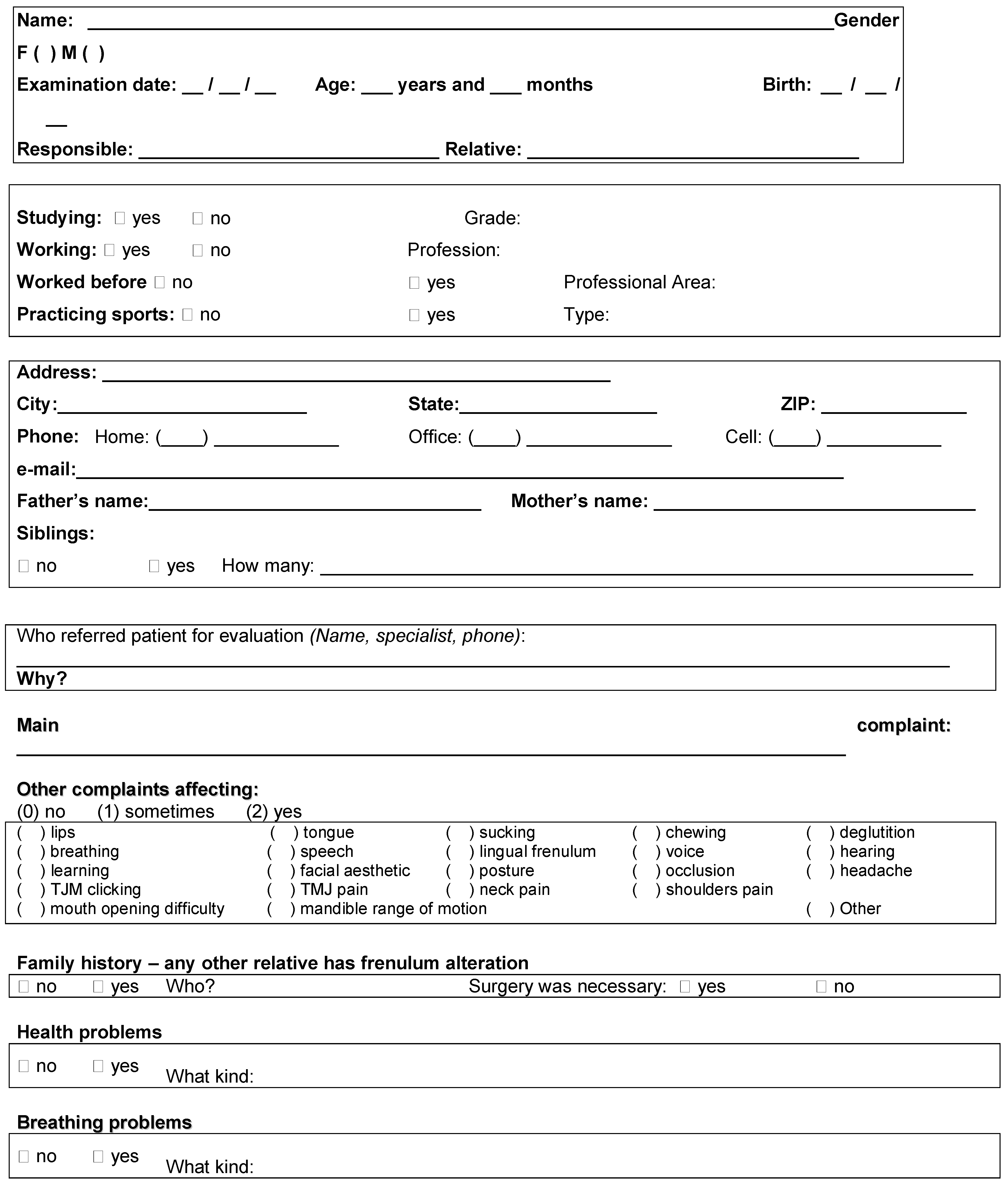
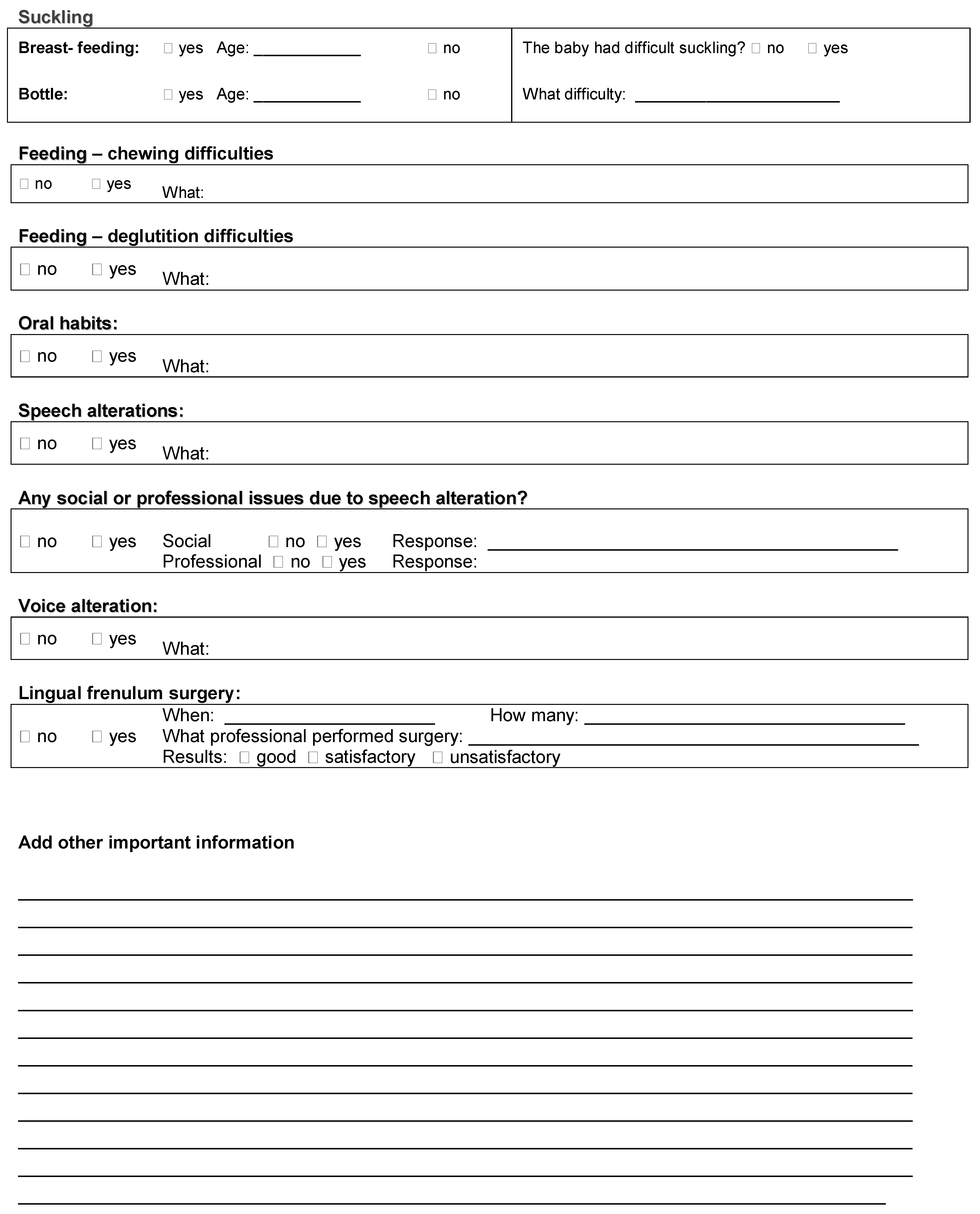
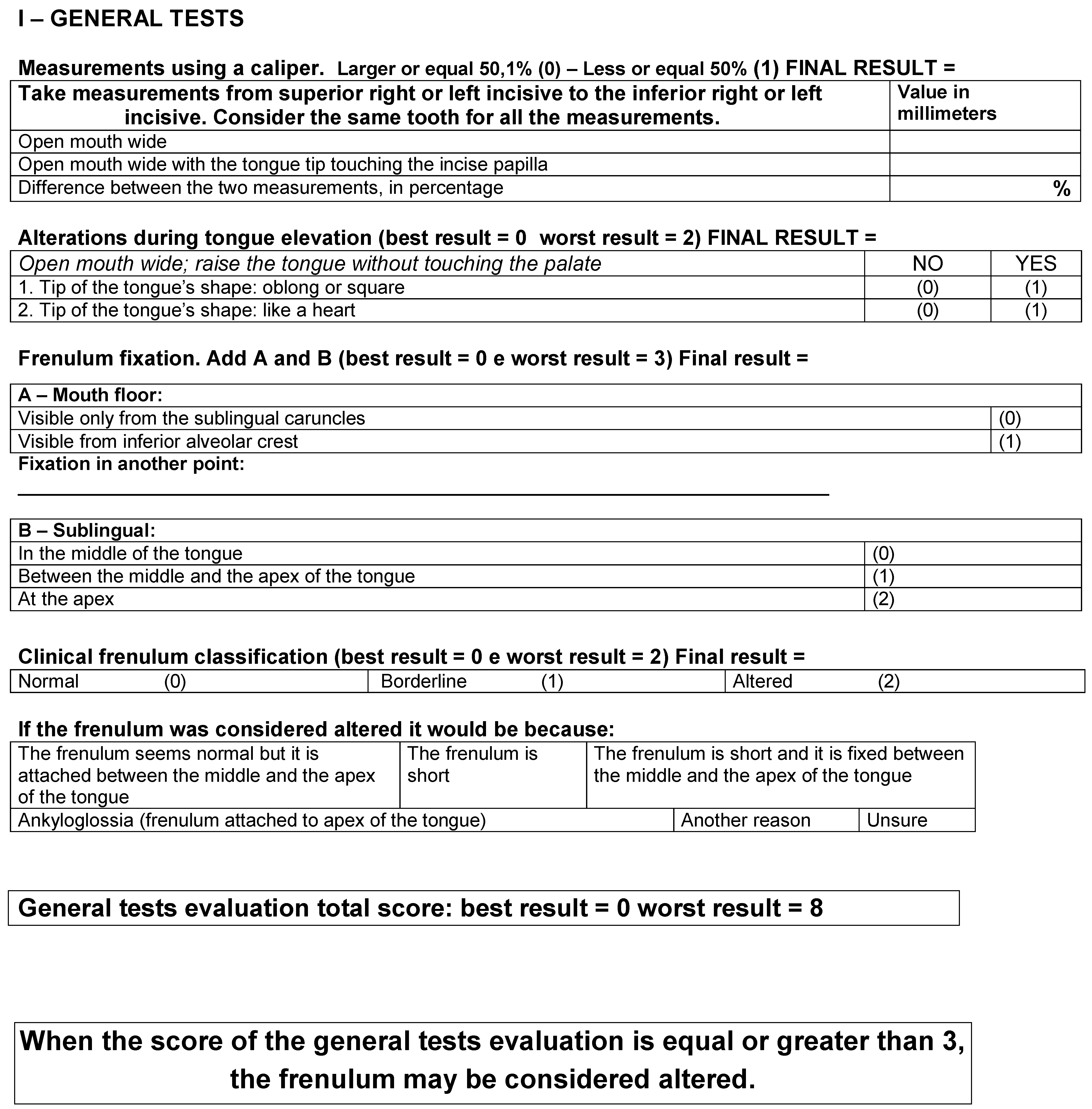
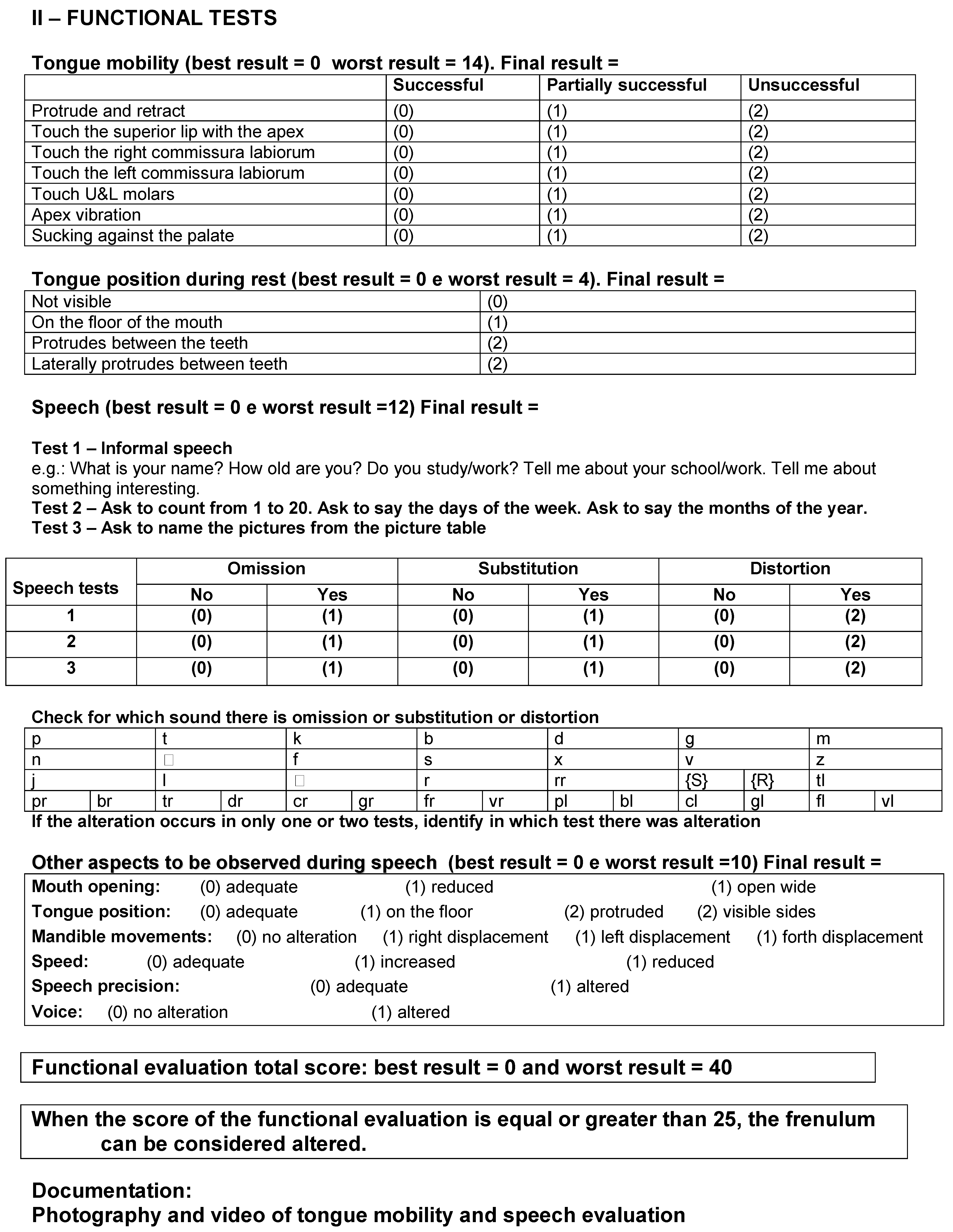
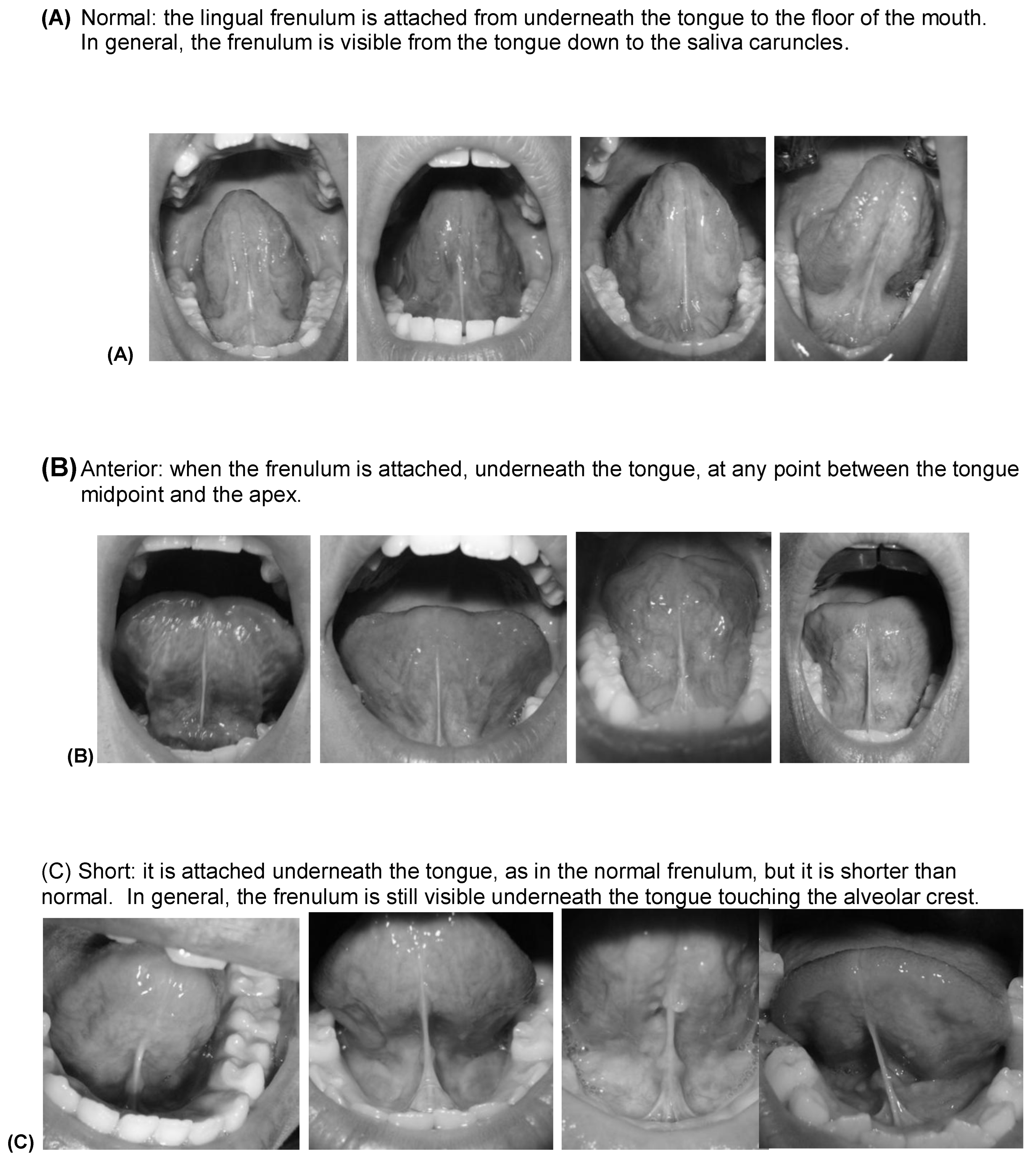
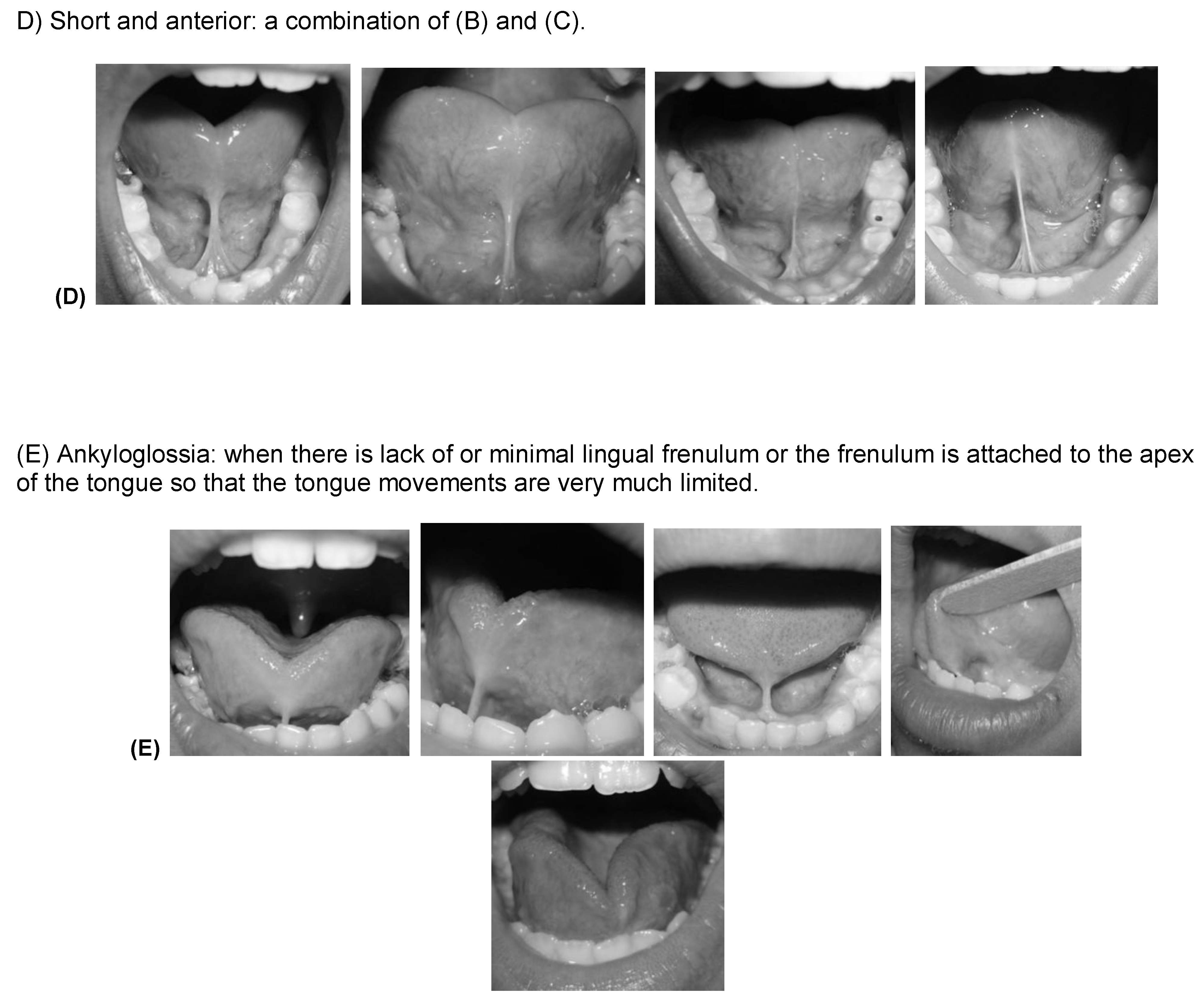
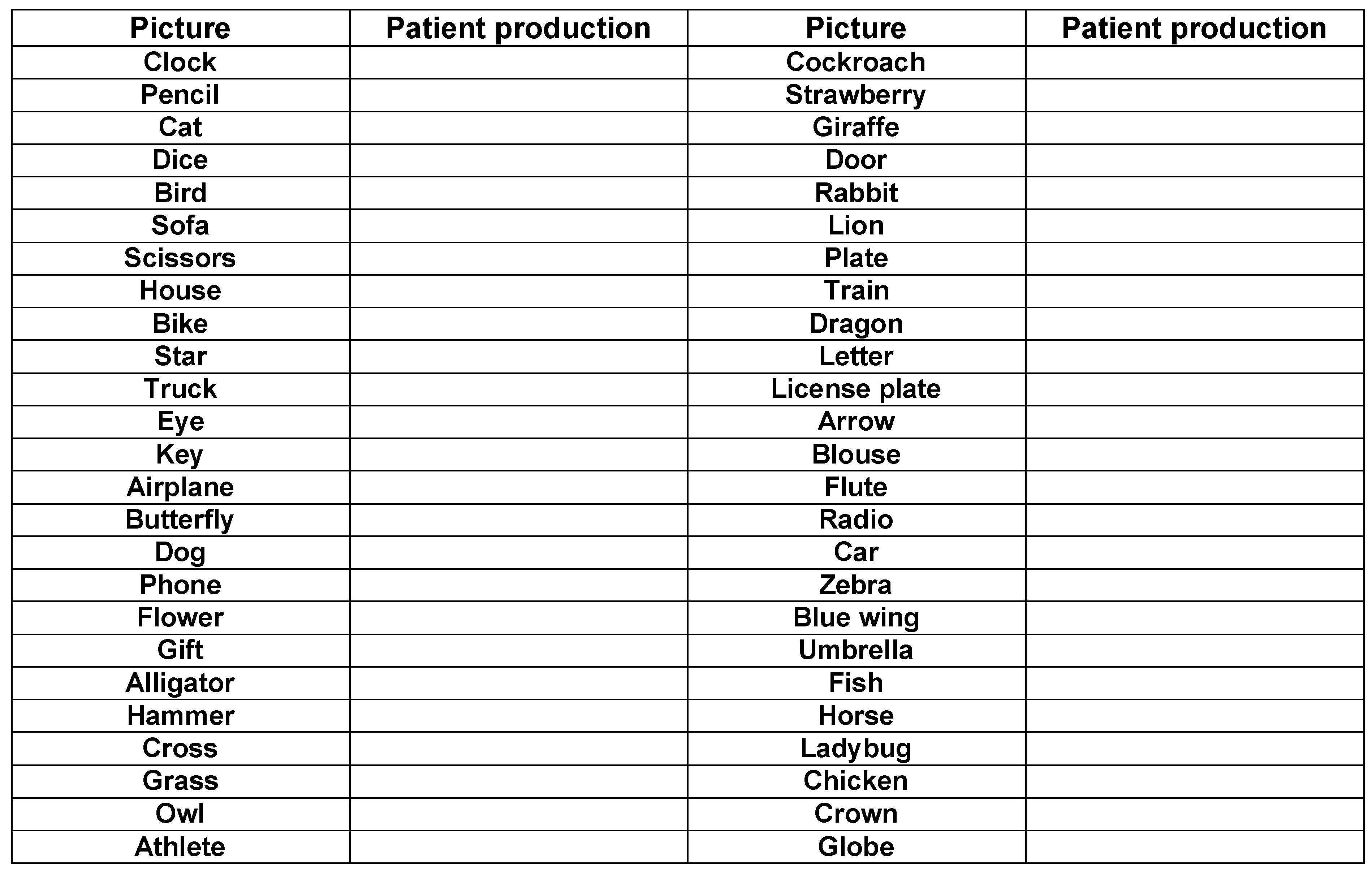
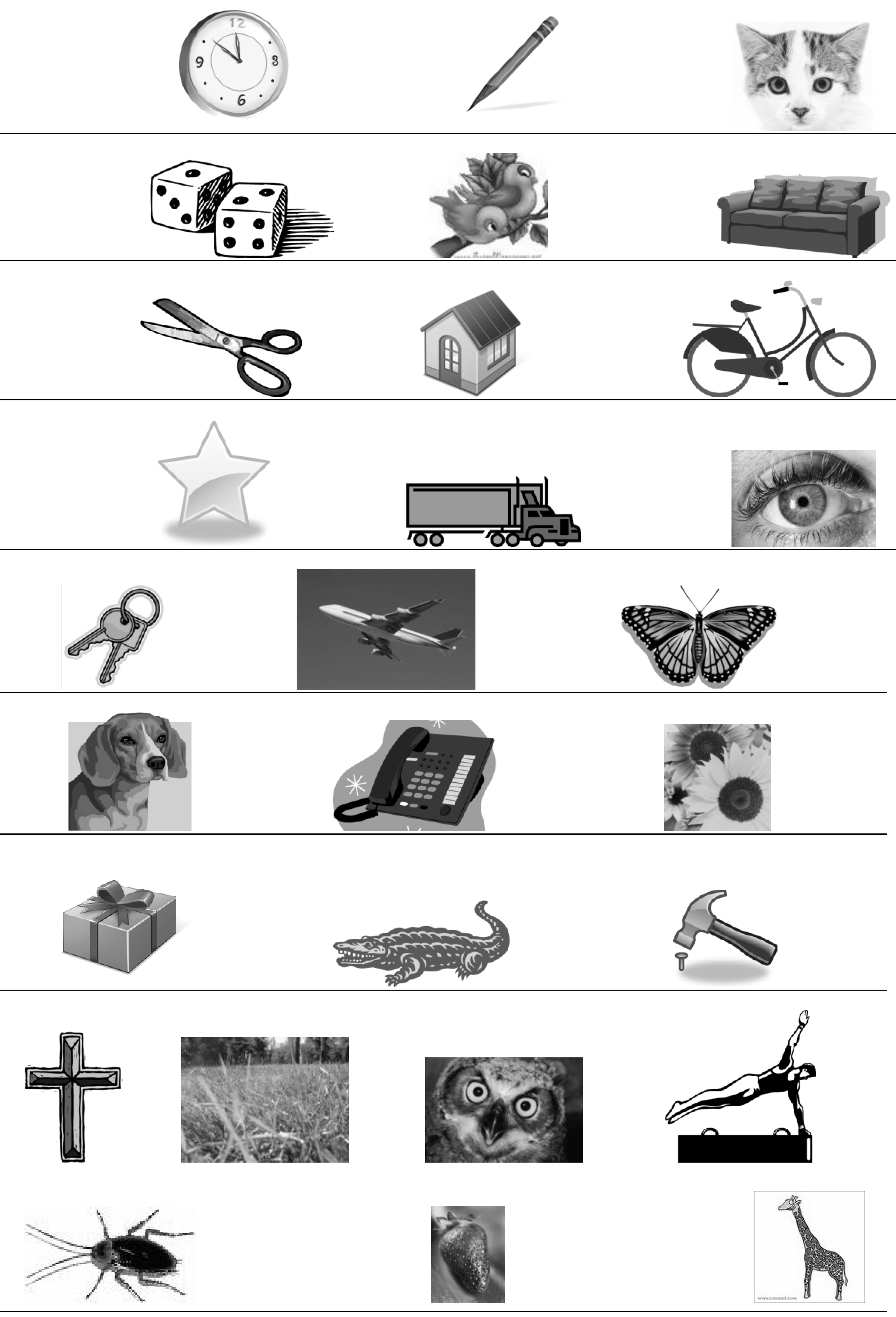
Appendix A. LINGUAL FRENULUM PROTOCOL
Appendix B. LINGUAL FRENULUM PROTOCOL (Instructional Photos)
Appendix C. LINGUAL FRENULUM PROTOCOL
References
- Ballard, J., C. Auer, and J. Khoury. 2002. Ankyloglossia: Assessment, incidence, and effect of frenuloplasty on the breastfeeding dyad. Journal of Pediatrics 110, 5: 1–6. [Google Scholar] [CrossRef] [PubMed]
- Brito, S. F., I. Q. Marchesan, C. M. Bosco, A. C. A. Carrilho, and M. I. Rehder. 2008. Frênulo lingual: Classificação e conduta segundo ótica fonoaudiológica, odontológica e otorrinolaringológica. Revista CEFAC 10, 3: 343–351. [Google Scholar] [CrossRef]
- Dorland, S. 2004. Illustrated medical dictionary, 26th ed. Saunders Company. [Google Scholar]
- Fleiss, P., M. Burger, H. Ramkumar, and P. Carrington. 1990. Ankyloglossia: A cause of breastfeeding problems? Journal of Human Lactation 6, 3: 128–129. [Google Scholar] [CrossRef] [PubMed]
- Forlenza, G. P., N. M. P. Black, E. G. McNamara, and S. E. Sullivan. 2010. Ankyloglossia, exclusive breastfeeding, and failure to thrive. Journal of Pediatrics 125: 1500–1504. [Google Scholar] [CrossRef]
- Galvão Filho, S. 2001. Dicionário odonto-médico inglês-português. São Paulo: Santos. [Google Scholar]
- Geddes, D. T., D. B. Langton, I. Gollow, L. A. Jacobs, P. E. Hartmann, and K. Simmer. 2008. Frenulotomy for breastfeeding infants with ankyloglossia: Effect on milk removal and sucking mechanism as imaged by ultrasound. Journal of Pediatrics 122: e188–e194. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, C. S., and M. C. Ferreiro. 2006. Estudo da relação entre presença de frênulo lingual curto e/ou anteriorizado e a dorsalização do fone [r] na articulação da fala. Revista CEFAC 8, 1: 56–60. [Google Scholar]
- Hall, D. M. B., and M. J. Renfrew. 2005. Tongue-tie: Common problem or old wives’ tale. Archives of Disease in Childhood 90: 1211–1215. [Google Scholar] [CrossRef]
- Hazelbaker, A. K. 1993. The assessment tool for lingual frenulum function (ATLFF): Use in a lactation consultant private practice. Pasadena, CA: Pacific Oaks College, Thesis. [Google Scholar]
- Hogan, M., C. Westcott, and M. Griffiths. 2005. Randomized, controlled trial of division of tongue-tie in infants with feeding problems. Journal of Paediatrics and Child Health 41, 5–6: 246–250. [Google Scholar] [CrossRef]
- Jorgenson, R., S. Shapiro, C. Salinas, and L. Levin. 1982. Intraoral findings and anomalies in neonates. Journal of Pediatrics 69, 5: 577–582. [Google Scholar] [CrossRef]
- Karabulut, R., K. Sonmez, Z. Turkyilmaz, B. Demirogullari, I. O. Ozen, B. Bagbanci, N. Kale, and A. C. Basklar. 2008. Ankyloglossia and effects on breast-feeding, speech problems and mechanical/social issues in children. Belgian Ear Nose Throat Journal (B-ENT) 4, 2: 81–85. [Google Scholar]
- Kenneth, N. A., ed. 1998. Mosby’s. Medical, nursing, e allied health dictionary, 5th ed. St. Louis, MO: Mosby, Inc. [Google Scholar]
- Knox, I. 2010. Tongue-tie and frenotomy in the breastfeeding newborn. Journal of the American Academy of Pediatrics (NeoReviews) 11, 9: 513–519. [Google Scholar] [CrossRef]
- Kotlow, L. A. 1999. Ankyloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence International 30: 259–262. [Google Scholar] [PubMed]
- Lalakea, M. L., and A. H. Messner. 2003. Ankiloglossia: The adolescent and adult perspective. Otolaryngology Head Neck Surgery 128: 746–752. [Google Scholar] [CrossRef] [PubMed]
- Lee, S. K., Y. S. Kim, and C. Y. Lim. 1989. A pathological consideration of ankyloglossia and lingual myoplasty. Taehan Chikkwa Uisa Hyophoe Chi 27, 3: 287–308. [Google Scholar]
- Marchesan, I. Q. 2004. Lingual frenulum: Classification and speech interference. International Journal of Orofacial Myology 30: 31–38. [Google Scholar] [CrossRef]
- Marchesan, I. Q. 2005. Lingual frenulum: Quantitative evaluation proposal. International Journal of Orofacial Myology 31: 39–48. [Google Scholar] [CrossRef]
- Marchesan, I. Q., M. I. B. C. Rehder, R. L. C. Martinelli, M. L. V. C. M. Costa, R. L. T. Araújo, M. R. T. Caltabellotta, and L. R. Oliveira. 2009. Fala e frênulo da língua. Existe alguma relação? In XVII congresso brasileiro de fonoaudiologia, 2009, Salvador. Revista da Sociedade Brasileira de Fonoaudiologia. Suplemento Especial. São Paulo: Sociedade Brasileira de Fonoaudiologia. [Google Scholar]
- Marmet, C., E. Shell, and R. Marmet. 1990. Neonatal frenotomy may be necessary to correct breastfeeding problems. Journal of Human Lactation 6, 3: 117–121. [Google Scholar] [CrossRef]
- Martinelli, R. L. C., I. Q. Marchesan, A. C. Rodrigues, and G. Berretin-Felix. 2012. Protocolo de avaliação do frênulo da língua em bebês. Revista CEFAC 14, 1: 138–145. [Google Scholar] [CrossRef]
- Merdad, H., and A. K. Mascarenhas. 2010. Ankyloglossia may cause breastfeeding, tongue mobility, and speech difficulties, with inconclusive results on treatment choices. Journal of Evidence-Based Dental Practice 10, 3: 152–153. [Google Scholar] [CrossRef]
- Messner, A., M. Lalakea, J. Macmahon, and E. Bair. 2000. Ankyloglossia: Incidence and associated feeding difficulties. Archives Otolaryngology Head & Neck Surgery 126, 1: 36–39. [Google Scholar]
- Messner, A., and M. Lalakea. 2000. Ankyloglossia: Controversies in management. International Journal of Pediatric Otoryinolaryngology 54, 2: 123–131. [Google Scholar] [CrossRef] [PubMed]
- Miranda, B. H., and C. J. Milroy. 2010. A quick snip-A study of the impact of outpatient tongue-tie release on neonatal growth and breastfeeding. Journal of Plastic, Reconstructive & Aesthetic Surgery 63, 9: e683–e685. [Google Scholar]
- Moore, K. L., and A. F. Dalley. 2001. Anatomia orientada para a clínica, 4th ed. Rio de Janeiro: Guanabara Koogan. [Google Scholar]
- Navarro, N. P., and M. López. 2002. Anquiloglossia en niños de 5 a 11 años de edad. Diagnóstico y tratamiento. Revista Cubana Estomatologia 39, 3: 3–7. [Google Scholar]
- Notestine, G. 1990. The importance of the identification of ankyloglossia (short lingual frenulum) as a cause of breastfeeding problems. Journal of Human Lactation 6, 3: 113–115. [Google Scholar] [CrossRef]
- Ostapiuk, B. 2006. Tongue mobility in ankyloglossia with regard to articulation. Annales Academiae Medicae Stetinensis 52 Suppl. 3: 37–47. [Google Scholar] [PubMed]
- Post, E. D., A. W. Rupert, and T. W. Schulpen. 2010. Problematic breastfeeding due to a short frenulum. Nederlands Tijdschrift voor Geneeskunde 154: A918. [Google Scholar] [PubMed]
- Ruffoli, R., M. A. Giambelluca, M. C. Scavuzzo, D. Bonfigli, R. Cristofani, M. Gabriele, M. R. Giuca, and F. Giannessi. 2005. Ankyloglossia: A morphofunctional investigation in children. International Journal of Oral Diseases 11, 3: 170–174. [Google Scholar] [CrossRef]
- Segal, L. M., R. Stephenson, M. Dawes, and P. Feldman. 2007. Prevalence, diagnosis, and treatment of ankyloglossia: Methodological review. Canadian Family Physician 53, 6: 1027–1033. [Google Scholar]
- Singh, S., and R. D. Kent. 2000. Dictionary of speech-language pathology. San Diego, CA: Singular’s. [Google Scholar]
- Stedman, T. L. 2003. Medical dictionary, 27th ed. Rio de Janeiro: Guanabara Koogan. [Google Scholar]
- Suter, V. G., and M. M. Bornstein. 2009. Ankyloglossia: Facts and myths in diagnosis and treatment. Journal of Periodontology 80, 8: 1204–1219. [Google Scholar] [CrossRef]
- Tuli, A., and A. Singh. 2010. Monopolar diathermy used for correction of ankyloglossia. Journal of Indian Society of Pedodonyics and Preventive Dentistry 28: 130–133. [Google Scholar] [CrossRef]
- Wallace, H., and S. Clarke. 2006. Tongue-tie division in infants with breast-feeding difficulties. International Journal of Pediatric Otoryinolaryngology 70, 7: 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Williams, W. N., and C. M. Waldron. 1985. Assessment of lingual function when ankyloglossia (tongue-tie) is suspected. The Journal of the American Dental Association 110, 3: 353–356. [Google Scholar] [CrossRef] [PubMed]
- Zemlin, W. R. 2000. Princípios de anatomia e fisiologia em fonoaudiologia, 4th ed. Porto Alegre: Artmed. [Google Scholar]
© 2012 by the author. 2012 Irene Queiroz Marchesan.
Share and Cite
Marchesan, I.Q. Lingual Frenulum Protocol. Int. J. Orofac. Myol. Myofunct. Ther. 2012, 38, 89-103. https://doi.org/10.52010/ijom.2012.38.1.7
Marchesan IQ. Lingual Frenulum Protocol. International Journal of Orofacial Myology and Myofunctional Therapy. 2012; 38(1):89-103. https://doi.org/10.52010/ijom.2012.38.1.7
Chicago/Turabian StyleMarchesan, Irene Queiroz. 2012. "Lingual Frenulum Protocol" International Journal of Orofacial Myology and Myofunctional Therapy 38, no. 1: 89-103. https://doi.org/10.52010/ijom.2012.38.1.7
APA StyleMarchesan, I. Q. (2012). Lingual Frenulum Protocol. International Journal of Orofacial Myology and Myofunctional Therapy, 38(1), 89-103. https://doi.org/10.52010/ijom.2012.38.1.7