INTRODUCTION
The orofacial myologist with a non-dental background needs to be familiar with the terminology used to describe the dentition and its relationship to the surrounding oral structures in order to communicate with his/her referral source the results of comparing the client’s presenting occlusal relationship with the perceived norm. One of the therapist’s goals at the time of the initial evaluation is to detect any abnormalities in the dental alignment which may have been the result of behaviors which will be targeted in the treatment plan designed as a result of this evaluation, and to communicate these findings to the referral source. The Occlusal Evaluation protocol provided with this article (
Appendix A) is taken from the complete Initial Evaluation for Orofacial Myology from Orofacial myology: A Comprehensive Study Guide (
Snow, 2003). In order to achieve these goals, it is not only necessary to understand the terminology used by dentists, but also to be aware of the average (or normal) relationships of both the primary and permanent sets of teeth. This article will attempt to enable the orofacial myologist with little or no dental knowledge to make these initial assessments, and to be able to communicate them accurately. The information in this article is a synopsis of information provided in traditional dental texts (Brand, & Isselhand, 1990; Dunn, & Schulze, 1989;
Moyers, 1988; Fuller, & Denehy, 1977; Kraus, Jordan, and Abrams, 1969), and the orofacial myology texts by
Hanson and Barrett (
1988) and Hanson and Mason, (2003).
SET, ARCH, CLASS, AND TYPE TRAITS
While some of these landmarks may be familiar in layman’s terms, it will add credence to the therapist with a non-dental background to use the terminology of the dental profession; so to begin with, there are two dental arches in the oral cavity. The upper arch is called the maxillary arch and the lower arch is called the mandibular arch. The two arches are divided into quadrants at the mid-sagittal plane, which is a vertical line from the nose to the chin, resulting in upper left, lower left, upper right and lower right. The horizontal separation of the two arches is referred to as the occlusal plane. A fundamental concept of dental terminology is that you are facing a patient; therefore your right side is the patient’s left side. It is helpful to envision shaking hands with the illustration or patient being examined so as not to confuse right and left sides when describing your findings.
The two arches are designed to contain the two sets of teeth allocated to humans – the primary and the permanent sets. Primary teeth are also known as deciduous (because they are exfoliated) or milk teeth as they are associated with babies. Permanent teeth replace the primary set. Each set of teeth is divided into classes with the primary set containing three classes: two incisors, one canine, and two molars in each quadrant making a total of twenty primary teeth after eruption is completed. The four classes in the permanent set of teeth consists of two incisors, one canine, two premolars (bicuspids), and three molars in each quadrant making a total of thirty-two permanent teeth. The third molar is referred to as the “wisdom” tooth and is frequently missing or un-erupted. The extra class of teeth (premolars) in the permanent dentition is necessary because of the increase in growth of the arches.
The final classification used to identify individual teeth is called a type trait. For example, the class of incisors contains two types – the central incisor closest to the midline (mid-sagittal plane) and lateral incisor the one behind it. Canines are alone in their class because there is only one, but premolars (in the permanent dentition) are distinguished as first (closest to the mid-line) followed by the second premolar. The molars are simply numbered first, second, and third in their consecutive order. The primary dentition is made up of central and lateral incisors, one canine and a first and second molar. Dental classification also includes individual type traits which the orofacial myologist without a dental background must learn and be able to use to identify single teeth as to their arch, set, class, and type. These individual traits will not be introduced here!
INDIVIDUAL TEETH
In addition to set, arch, class, and type traits, it is necessary to identify individual teeth using a short-hand system which includes all of the traits. This is accomplished in the permanent dentition by a numerical system that starts in the maxillary right-hand quadrant with the third (last) molar and continues to the midline as 1,2,3,4,5,6,7 8 I (midline)and then continues on to the maxillary left quadrant 9, 10, 11, 12, 13, 14, 15, 16. This system makes both numbers 8 and 9 central incisors, 7 and 10 lateral incisors, 6 and 11 canines, 5 and 12 first premolars, 4 and 13, second premolars and 3,2,1 and 14,15,16 first, second and third molars. The numbering then drops down to the mandibular left quadrant to continue on as 17 through 32 in the same style as its maxillary counterpart. The primary dentition is identified by a quadrant sign __I (upper right) and a letter EI DI CI BI AIA IB IC ID IE with a reverse configuration for the mandible. There are other classification systems used to communicate specific teeth, but these two are the most commonly used.
DIRECTION
In addition to identification of specific teeth, it is also necessary to be able to relate direction in the oral cavity. We have previously identified the upper arch as maxillary and the lower arch as mandibular. The next terms of importance are mesial, which means toward the midline or midsagittal plane, and distal, away from the midline, lingual meaning on the tongue side, buccal meaning on the cheek side, and labial meaning facing the lips. Another term, facial, includes both buccal and labial. The individual tooth is divided into the crown and the root with the crown divided into cervical (neck), middle, and for incisors and canines incisal thirds. Premolars and molars have occlusal thirds instead of incisal which is the reason for calling the horizontal plane mentioned previously, occlusal. The occlusal surfaces of the premolars and molars are made up of cusps and fosses, which ideally fit into their opposing mandibular or maxillary counterparts when closed together. These structural differences reflect the function of the different classes of teeth: incisal/cutting, canine/tearing, and occlusal/grinding. Another term of interest to the orofacial myologist is mammelons, which are small elevations on the newly erupted incisal edge of permanent central incisors. If there are mammelons present on a tooth, it is an indication of abnormal functioning of the cutting process as these elevations normally wear down with use.
CHANGING DENTITION
Primary teeth begin developing “in utero” and start the eruption process at an average age of eight months. The mandibular incisors are the first to appear followed by the maxillary incisors. This pattern of mandibular teeth erupting prior to maxillary is repeated throughout the changing dentition. The first primary molars erupt at approximately fourteen months followed by the canines at an average age of 16 months. Primary tooth eruption is usually complete at the age of three years with the eruption of the second molar. Girl’s tooth eruption pattern usually precedes that of boys in both sets of teeth and is an important factor in orthodontic treatment. A concept that many children have never been exposed to is that the primary teeth are temporary with new teeth developing underneath them, and that the roots holding the “baby” teeth in place will resorb leaving only the crown to fall out. Also, many children do not realize that habits such as finger/thumb sucking, pacifiers, nail biting can affect the alignment of the teeth.
The permanent first molars start calcification at birth and are usually the first permanent teeth to erupt at age six years. By this time the arch has expanded enough to make room for them behind the primary second molars. For this reason, they are frequently mistaken for another primary molar. This “six” year molar, as it is commonly called, is a vulnerable tooth because of its calcification during the time that the child is most frequently exposed to teratogens such as medication or a high fever. The permanent incisors follow closely after the first molar in the eruption pattern of the permanent dentition with an average age of seven to nine years. The age ranges have gradually been extended as tooth eruption seems to follow the general pattern of later physical maturity. The premolars replace the primary molars between the ages of ten to twelve (sometimes even later) with the canine erupting on the mandible at age nine to ten and age eleven to twelve on the maxillary arch. Canine eruption may depend on whether there is space left after the premolars have erupted. In a Class I malocclusion the canine is frequently crowded out of alignment. The second permanent molar is usually referred to as the “twelve” year molar and arrives between the ages of eleven and thirteen. The third molar (wisdom tooth), if present in the oral cavity, usually erupts between the ages of seventeen and twenty-one. It is also frequently surgically removed, because of lack of space or poor development. The period of changing dentition needs to be understood and assessed as to its normalcy taking into account the great variation in individual growth and development.
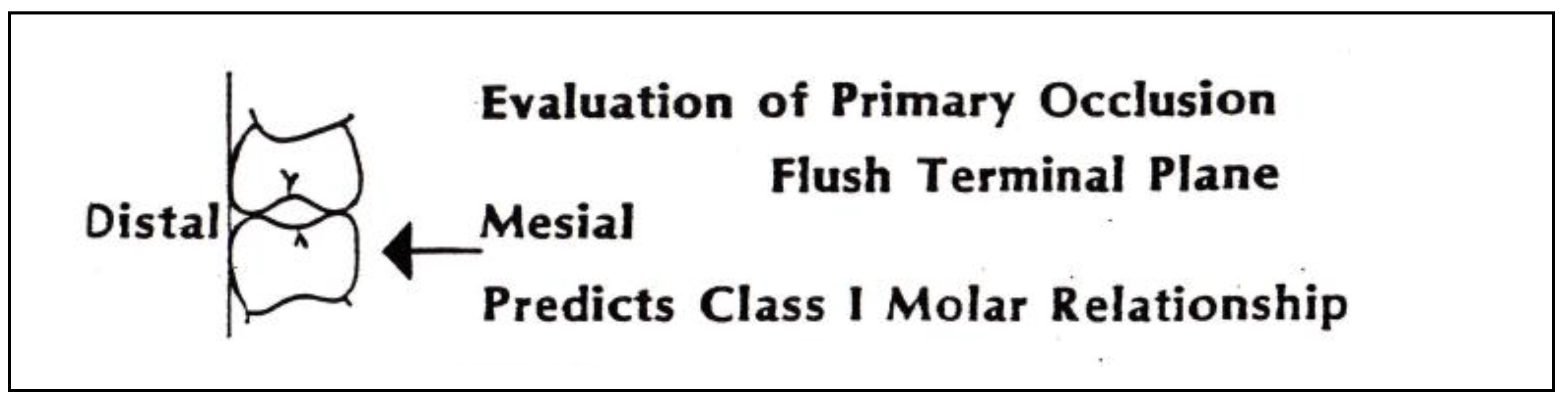
EVALUATION OF PRIMARY DENTITION OCCLUSION
The occlusal evaluation of the primary dentition is important for the orofacial myologist as a predictor of the permanent dentition occlusion. The accompanying
Figure 1,
Figure 2 and
Figure 3 illustrate the relationship between the maxillary and mandibular primary first molars based on Angle’s classification of the permanent dentition occlusion. A so-called normal or
Class I relationship would have either a
flush distal plane, meaning that a line drawn behind the distal buccal surface of the maxillary and mandibular molars would contact both equally, or there would be a
mesial step relationship, indicating a slight forward positioning of the mandibular primary molar (
Figure 1).
If instead of either of these two relationships, there is a distal positioning of the mandibular molar, meaning that a vertical line drawn distal to the primary mandibular molar surface creates a
distal step relationship to the maxillary molar, this would predict a
Class II permanent molar relationship (
Figure 2).
The reverse of the distal relationship would be a mesial or forward positioning of the mandible which is called a
mesial step and predicts a
Class III permanent dentition occlusion (
Figure 3).
The normal alignment of the permanent dentition when in occlusion has the maxillary posterior teeth overlapping the mandibular posterior teeth and the anterior maxillary teeth overlapping the mandibular anterior teeth. The purpose of this overlap (including the posterior distal) is called a “self-protective” feature in that it precludes harm to the soft tissues of the oral cavity during mastication. The horizontal overlapping relationship of the anterior teeth is referred to as the overjet and should be approximately two or three millimeters in width. In a normal dental alignment there is also a vertical overlapping of the incisal teeth which covers the cervical one-third of the mandibular incisers, this is called the overbite. When in a relaxed, non-functional state there is normally a freeway space of approximately two to three millimeters between the opposing posterior teeth and three to five millimeters in the anterior.
There are many dental instruments for the therapist’s use which measure in millimeters as well as instruments designed specifically for orofacial myologists, including millimeter rulers and throw away paper devices in the Therabite line of products (ATOS Medical) that do not require sterilization. Deviations in any of these norms are of concern to the orofacial myologist and need to be documented. During therapy the numbers are also of importance in documenting therapy progress as they gradually return toward normal. In the normal alignment of the teeth there are contact points where all but the most distal surface of the last tooth in each quadrant contacts the tooth next to it. A fairly frequent example of a lack of contact between two teeth occurs with the maxillary central incisors. This space is called a diastema and should be measured in millimeters and recorded in the occlusal evaluation. If there is no soft tissue separating these teeth, this space may possibly be the result of a behavior pattern that needs to be addressed in the treatment plan. These spaces will be discussed again when describing the primary dentition. Dental symmetry refers to the alignment of the teeth in reference to the midsagittal plane. This vertical line divides the arches into right and left quadrants, and ideally the upper and lower central incisors should line up adjacent to it.
Primary teeth are smaller, whiter, and more “squat” in appearance than permanent teeth. The eruption and exfoliation norms may be found in
Lunt & Law (
1974) and
Wheeler (
1974). Normally, there is little or no overlap of the maxillary arch over the mandibular in the primary dentition resulting in a lack of overbite or overjet. This lack of overlap also results in what is called a “flush terminal plane” for the upper and lower second molars. The primary teeth begin formation prenatally by trimester with approximately 20% of their calcification complete at birth. Consequently they present good clues to teratogens that may have been present prenatally or during early childhood which may result in dental anomalies of interest to the therapist. Frequently there will be spacing between primary teeth as the arches grow which is called
leeway space. This is not to be confused with diastemas and is a normal result of arch expansion. The therapist should be able to distinguish primary from permanent teeth in order to identify retained primary teeth in a space where there is a congenitally missing permanent tooth as well as to evaluate the stages of mixed dentition.
The orofacial myologist doing an initial evaluation of a primary dentition will be primarily concerned with the overbite, overjet, and whether or not there is a cross bite or open bite. Deviations in overbite and overjet may indicate a behavior pattern that should be targeted in therapy. A crossbite would indicate that the occlusal and incisal planes of the two arches are abnormal in their relationship to each other resulting in asymmetry of the arches and again may indicate inclusion in therapy treatment plan. One of the most common abnormalities found in orofacial myology clients is an open bite which indicates a negative overbite and again is measured in millimeters and documented in the evaluation. Another clue may be a prognathic (forward) positioning of the mandible which could be functional (result of a habit) as opposed to structural (inherited). The primary dentition provides a prediction of the permanent occlusal pattern and is helpful in determining whether heredity or habits are influencing the development of the occlusion.
ANGLE’S CLASSIFICATION OF PERMANENT DENTITION OCCLUSION
This system of classification is based on an anterioposterior relationship of the jaws and as described above is divided into
Classes (
Moyers, 1988). The normal relationship of the posterior teeth has the first permanent molar’s mesiobuccal cusp articulating with the buccal grove of the first mandibular molar. This relationship is illustrated in
Figure 3 as a “mesial Step” and consequently positions the upper first molar’s distobuccal cusp slightly distal to the lower first molar. This results in the distal overlap of the normal
Class I occlusion which serves as the self-protective feature discussed previously. The Class I occlusion definition would imply that all of the teeth are correctly aligned; consequently most Class I occlusions are malocclusion indicating that one or more teeth are out of alignment even though the molar relationship is correct. The typical
Class I malocclusion is evidenced by crowding where frequently the canines or incisors are forced out of alignment. A
Class II malocclusion has a “distal step” relationship as illustrated in
Figure 2. This results in an excessive over-jet (over 3 millimeters) and is frequently referred to as “buck teeth” with a retruded mandibular profile. Class II malocclusions are divided into two categories,
Division I was just described and
Division II has the same distal step molar relationship but with a lingual version (and excessive overbite) of the maxillary central incisors and a labial version and overlapping of the lateral incisors.
Class III malocclusions are the result of a mesial step relationship of the mandibular first molar to its maxillary counterpart which is evidenced by a protruding jaw or what may be called a “prognathic index”. A
pseudo Class III malocclusion may result from behavioral patterns and would require radiographs to distinguish it from a
skeletal Class III malocclusion. Class II malocclusions usually result in a
convex facial profile where as Class III malocclusions usually result in a
concave facial profile. All of these malocclusions can be influenced by muscle patterns and rest postures that are of concern to the orofacial myologist.
CONCLUSIONS
It is incumbent upon the orofacial myologist to evaluate the presenting client’s occlusion and detect any behaviors which may be influencing the alignment of the dentition or interfering with the treatment plan of the referral source. In order to accomplish these tasks, it is necessary to share some common terminology and to effectively communicate between all the participants involved in the treatment plan. The purpose of this article is to assist in accomplishing these goals.

{kind=link}
{kind=link}
{kind=link}
{kind=link}