
Antimicrobial Resistance and Prevalence of β-lactamase Genes Among Multidrug-Resistant Acinetobacter baumannii Isolates from Infected Diabetic Foot Ulcers

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Bacterial Isolation and Antibiogram Profile of A. baumannii
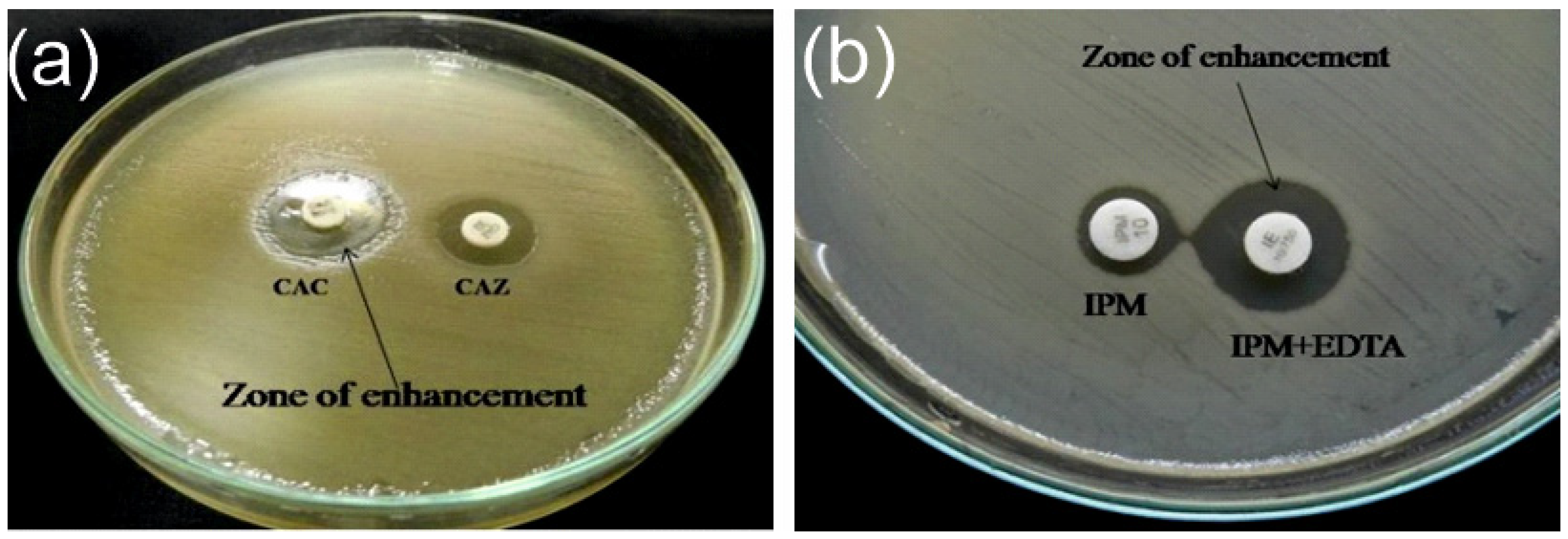
2.3. Extended Spectrum β-lactamase and Metallo-β-lactamase
2.4. DNA Extraction and Multiplex qPCR
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Antimicrobial Susceptibility and ESBL/MBL Detection
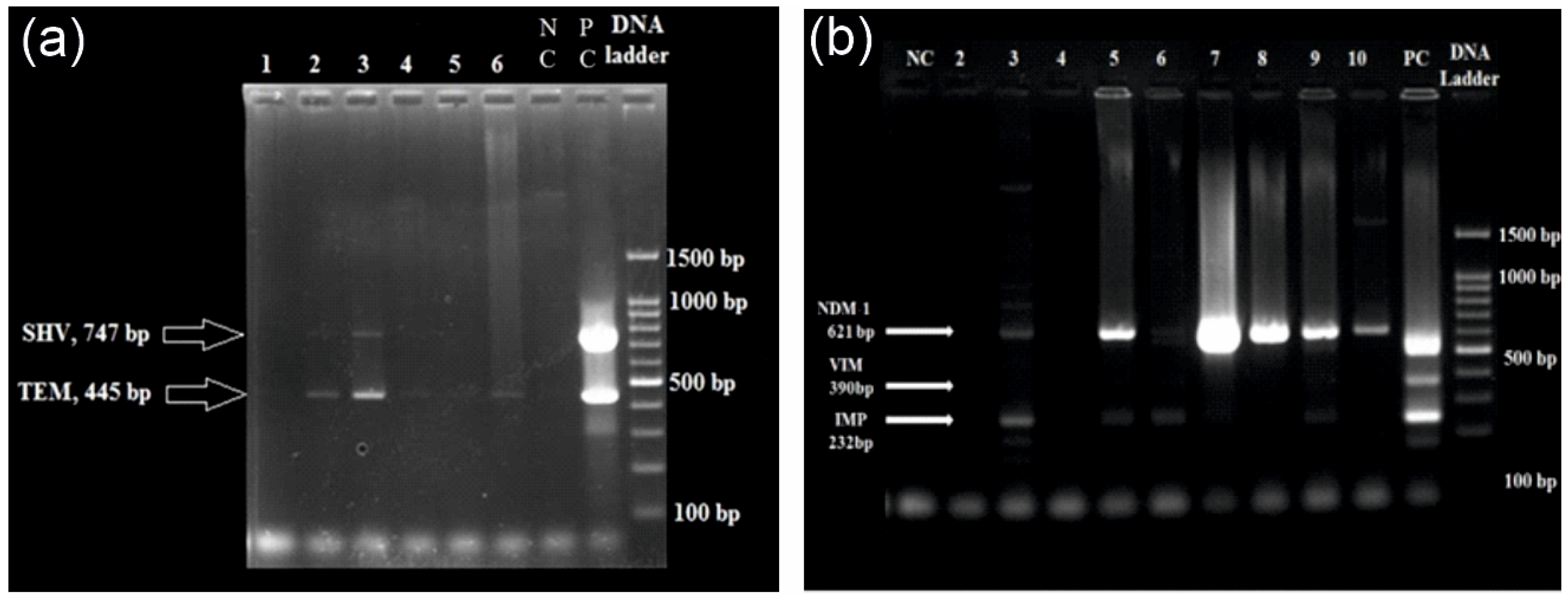
3.3. Multiplex qPCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cigna, E.; Fino, P.; Onesti, M.G.; Amorosi, V.; Scuderi, N. Diabetic foot infection treatment and care. Int. Wound J. 2016, 13, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Lauri, C.; Leone, A.; Cavallini, M.; Signore, A.; Giurato, L.; Uccioli, L. Diabetic foot infections: The diagnostic challenges. J. Clin. Med. 2020, 9, 1779. [Google Scholar] [CrossRef]
- Noor, S.; Khan, R.U.; Ahmad, J. Understanding diabetic foot infection and its management. Diabetes Metab. Syndr. 2017, 11, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.L.; Wyant, W.A.; Abdo Abujamra, B.; Kirsner, R.S.; Jozic, I. Diabetic wound-healing science. Medicina 2021, 57, 1072. [Google Scholar] [CrossRef]
- McDermott, K.; Fang, M.; Boulton, A.J.M.; Selvin, E.; Hicks, C.W. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care 2023, 46, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, M.; Manu, C.; Vas, P. The current burden of diabetic foot disease. J. Clin. Orthop. Trauma. 2021, 17, 88–93. [Google Scholar] [CrossRef]
- Hadi, P.; Rampal, S.; Neela, V.K.; Cheema, M.S.; Sarawan Singh, S.S.; Kee Tan, E.; Sinniah, A. Distribution of causative microorganisms in diabetic foot infections: A ten-year retrospective study in a tertiary care hospital in central Malaysia. Antibiotics 2023, 12, 687. [Google Scholar] [CrossRef] [PubMed]
- Turhan, V.; Mutluoglu, M.; Acar, A.; Hatipoglu, M.; Onem, Y.; Uzun, G.; Ay, H.; Oncul, O.; Gorenek, L. Increasing incidence of Gram-negative organisms in bacterial agents isolated from diabetic foot ulcers. J. Infect. Dev. Ctries. 2013, 7, 707–712. [Google Scholar] [CrossRef]
- El-Hazmi, M.M. Bacteriological profile of diabetic foot infections in a teaching hospital in Saudi Arabia. J. Pure Appl. Microbiol. 2015, 9, 1933–1943. [Google Scholar]
- Jouhar, L.; Jaafar, R.F.; Nasreddine, R.; Itani, O.; Haddad, F.; Rizk, N.; Hoballah, J.J. Microbiological profile and antimicrobial resistance among diabetic foot infections in Lebanon. Int. Wound J. 2020, 17, 1764–1773. [Google Scholar] [CrossRef]
- Alhubail, A.; Sewify, M.; Messenger, G.; Masoetsa, R.; Hussain, I.; Nair, S.; Tiss, A. Microbiological profile of diabetic foot ulcers in Kuwait. PLoS ONE 2020, 15, e0244306. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.D.; Ou, S.J.; Zhang, W.; Li, J.X.; Xia, C.L.; Yang, Y.; Liu, J.B.; Ma, Y.F.; Jiang, N.; Wang, Y.Y.; et al. Microbiological profile of diabetic foot infections in China and worldwide: A 20-year systematic review. Front. Endocrinol. 2024, 15, 1368046. [Google Scholar] [CrossRef] [PubMed]
- Al Benwan, K.; Al Mulla, A.; Rotimi, V.O. A study of the microbiology of diabetic foot infections in a teaching hospital in Kuwait. J. Infect. Public Health 2012, 5, 1–8. [Google Scholar] [CrossRef]
- Son, S.T.; Han, S.K.; Lee, T.Y.; Namgoong, S.; Dhong, E.S. The microbiology of diabetic foot infections in Korea. J. Wound Manag. Res. 2017, 13, 8–12. [Google Scholar] [CrossRef]
- Sannathimmappa, M.B.; Nambiar, V.; Aravindakshan, R.; Al Khabori, M.S.; Al-Flaiti, A.H.; Al-Azri, K.N.; Al-Reesi, A.K.; Al Kiyumi, A.R. Diabetic foot infections: Profile and antibiotic susceptibility patterns of bacterial isolates in a tertiary care hospital of Oman. J. Educ. Health Promot. 2021, 10, 254. [Google Scholar] [CrossRef] [PubMed]
- Hitam, S.A.; Asma’Hassan, S.; Maning, N.U. The significant association between polymicrobial diabetic foot infection and its severity and outcomes. Malays. J. Med. Sci. 2019, 26, 107. [Google Scholar] [CrossRef]
- Sun, H.; Ma, Y.; Heng, H.; Liu, X.; Liang, J.; Geng, H. Microbiological Distribution, Antimicrobial Susceptibility and Risk Factors of Polymicrobial Infections in Diabetic Foot. Clin. Lab. 2024, 70. [Google Scholar] [CrossRef]
- Howard, A.; O’Donoghue, M.; Feeney, A.; Sleator, R.D. Acinetobacter baumannii: An emerging opportunistic pathogen. Virulence 2012, 3, 243–250. [Google Scholar] [CrossRef]
- Lahiri, K.K.; Mani, N.S.; Purai, S.S. Acinetobacter spp as nosocomial pathogen: Clinical significance and antimicrobial sensitivity. Med. J. Armed Forces India 2004, 60, 7–10. [Google Scholar] [CrossRef]
- Bali, N.K.; Fomda, B.A.; Bashir, H.; Zahoor, D.; Lone, S.; Koul, R.A. Emergence of carbapenem-resistant Acinetobacter in a temperate north Indian State. Br. J. Biomed. Sci. 2013, 70, 156–160. [Google Scholar] [CrossRef]
- Khan, D.M.; Manzoor, M.A.; Rao, I.V.; Moosabba, M.S. Evaluation of biofilm formation, cell surface hydrophobicity and gelatinase activity in Acinetobacter baumannii strains isolated from patients of diabetic and non-diabetic foot ulcer infections. Biocatal. Agric. Biotechnol. 2019, 18, 101007. [Google Scholar] [CrossRef]
- Zarrilli, R.; Pournaras, S.; Giannouli, M.; Tsakris, A. Global evolution of multidrug-resistant Acinetobacter baumannii clonal lineages. Int. J. Antimicrob. Agents 2013, 41, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Kyriakidis, I.; Vasileiou, E.; Pana, Z.D.; Tragiannidis, A. Acinetobacter baumannii antibiotic resistance mechanisms. Pathogens 2021, 10, 373. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V. An update on newer β-lactamases. Indian J. Med. Res. 2007, 126, 417–427. [Google Scholar]
- Goel, V.; Hogade, S.A.; Karadesai, S.G. Prevalence of extended-spectrum beta-lactamases, AmpC beta-lactamase, and metallo-beta-lactamase producing Pseudomonas aeruginosa and Acinetobacter baumannii in an intensive care unit in a tertiary care hospital. J. Sci. Soc. 2013, 40, 28–31. [Google Scholar] [CrossRef]
- Humphries, R.M.; Ambler, J.; Mitchell, S.L.; Castanheira, M.; Dingle, T.; Hindler, J.A.; Koeth, L.; Sei, K. CLSI methods development and standardization working group best practices for evaluation of antimicrobial susceptibility tests. J. Clin. Microbiol. 2018, 56, 10–128. [Google Scholar] [CrossRef]
- Andrews, J.M. Determination of minimum inhibitory concentrations. J. Antimicrob. Chemother. 2001, 48 (Suppl. S1), 5–16. [Google Scholar] [CrossRef]
- Manisha, J.; Mitesh, P.H.; Nidhi, S.K.; Modi, D.J.; Vegad, M.M. Spectrum of Microbial Flora in Diabetic Foot Ulcer and Antibiotic Sensitivity Pattern in Tertiary Care Hospital in Ahmedabad, Gujarat. Nat. J. Med. Res. 2012, 3, 354–357. [Google Scholar]
- Sekhar, S.; Unnikrishnan, M.K.; Rodrigues, G.S.; Vyas, N.; Mukhopadhyay, C. Antimicrobial susceptibility pattern of aerobes in diabetic foot ulcers in a South-Indian tertiary care hospital. Foot 2018, 37, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Iacopi, E.; Pieruzzi, L.; Riitano, N.; Abbruzzese, L.; Goretti, C.; Piaggesi, A. The weakness of the strong sex: Differences between men and women affected by diabetic foot disease. Int. J. Low. Extrem. Wounds 2023, 22, 19–26. [Google Scholar] [CrossRef]
- Sahu, S.S.; Chaudhary, V.; Sharma, N.; Kumari, S.; Pal, B.; Khurana, N. Prevalence and risk factors associated with diabetic foot ulcer in India: A systematic review and meta-analysis. Int. J. Infect. Dev. Ctries. 2024. [Google Scholar] [CrossRef]
- Castellanos, N.; Nakanouchi, J.; Yüzen, D.I.; Fung, S.; Fernandez, J.S.; Barberis, C.; Tuchscherr, L.; Ramirez, M.S. A study on Acinetobacter baumannii and Staphylococcus aureus strains recovered from the same infection site of a diabetic patient. Curr. Microbiol. 2019, 76, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Isler, B.; Keske, Ş.; Aksoy, M.; Azap, Ö.K.; Yilmaz, M.; Yavuz, S.Ş.; Aygün, G.; Tigen, E.; Akalın, H.; Azap, A.; et al. Antibiotic overconsumption and resistance in Turkey. Clin. Microbiol. Infect. 2019, 25, 651–653. [Google Scholar] [CrossRef] [PubMed]
- Moghnieh, R.A.; Kanafani, Z.A.; Tabaja, H.Z.; Sharara, S.L.; Awad, L.S.; Kanj, S.S. Epidemiology of common resistant bacterial pathogens in the countries of the Arab League. Lancet Infect. Dis. 2018, 18, e379–e394. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report 2020. Stockholm: ECDC. 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2022 (accessed on 1 March 2025).
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Zaki, M.E.; Abou ElKheir, N.; Mofreh, M. Molecular study of quinolone resistance determining regions of gyrA gene and parC genes in clinical isolates of Acintobacter baumannii resistant to fluoroquinolone. Open Microbiol. J. 2018, 12, 116. [Google Scholar] [CrossRef]
- Vázquez-López, R.; Solano-Gálvez, S.G.; Juárez Vignon-Whaley, J.J.; Abello Vaamonde, J.A.; Padró Alonzo, L.A.; Rivera Reséndiz, A.; Muleiro Álvarez, M.; Vega López, E.N.; Franyuti-Kelly, G.; Álvarez-Hernández, D.A.; et al. Acinetobacter baumannii resistance: A real challenge for clinicians. Antibiotics 2020, 9, 205. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Hassan, K.A.; Tetu, S.G.; Naidu, V.; Pokhrel, A.; Cain, A.K.; Paulsen, I.T. The transcriptomic signature of tigecycline in Acinetobacter baumannii. Front. Microbiol. 2020, 11, 565438. [Google Scholar] [CrossRef]
- Safari, M.; Nejad, A.S.; Bahador, A.; Jafari, R.; Alikhani, M.Y. Prevalence of ESBL and MBL encoding genes in Acinetobacter baumannii strains isolated from patients of intensive care units (ICU). Saudi J. Biol. Sci. 2015, 22, 424–429. [Google Scholar] [CrossRef]
- Ranjbar, R.; Tolon, S.S.; Zayeri, S.; Sami, M. The frequency of antibiotic resistance and ESBLs among clinically Acinetobacter baumannii strains isolated from patients in a major hospital in Tehran, Iran. Open Microbiol. J. 2018, 12, 254. [Google Scholar] [CrossRef]
- Farajnia, S.; Azhari, F.; Alikhani, M.Y.; Hosseini, M.K.; Peymani, A.; Sohrabi, N. Prevalence of PER and VEB type extended spectrum betalactamases among multidrug resistant Acinetobacter baumannii isolates in North-West of Iran. Iran. J. Basic Med. Sci. 2013, 16, 751. [Google Scholar] [PubMed]
- Azizi, M.; Mortazavi, S.H.; Etemadimajed, M.; Gheini, S.; Vaziri, S.; Alvandi, A.; Kashef, M.; Ahmadi, K. Prevalence of extended-spectrum β-Lactamases and antibiotic resistance patterns in Acinetobacter baumannii isolated from clinical samples in Kermanshah, Iran. Jundishapur J. Microbiol. 2017, 10, e61522. [Google Scholar] [CrossRef]
- Zarabadi-Pour, M.; Peymani, A.; Habibollah-Pourzereshki, N.; Sarookhani, M.R.; Karami, A.A.; Javadi, A. Detection of extended-spectrum ß-lactamases among Acinetobacter baumannii isolated from hospitals of Qazvin, Iran. Ethiop. J. Health Sci. 2021, 31, 229–236. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| All | Males | Females | Difference Between Males and Females | ||
|---|---|---|---|---|---|
| 480 (100.00%) | 365 (76%) | 115 (24%) | p a | ||
| Age, y | 56.5 (11.4) | 56.9 (11.1) | 55.1 (12.3) | 0.116 | |
| Wagner Grade, n (%) | Grade 2 | 98 (20.5) | 70 (19.2) | 28 (24.4) | 0.237 |
| Grade 3 | 199 (40.3) | 154 (42.2) | 45 (39.1) | ||
| Grade 4 | 147 (30.7) | 117 (35.5) | 30 (26.1) | ||
| Grade 5 | 36 (7.5) | 24 (6.6) | 12 (10.4) | ||
| Diabetes mellitus, n (%) | 480 (100.00) | 365 (76) | 115 (24) | - | |
| Hypertension, n (%) | 249 (51.9) | 182 (49.9) | 67 (58.3) | 0.071 | |
| Ischemic heart disease, n (%) | 80 (16.7) | 63 (17.3) | 17 (14.8) | 0.321 | |
| Peripheral vascular disease, n (%) | 300 (62.5) | 226 (61.9) | 74 (64.3) | 0.361 | |
| Retinopathy, n (%) | 275 (57.7) | 211 (55.8) | 64 (55.7) | 0.443 | |
| Nephropathy, n (%) | 85 (17.7) | 68 (18.6) | 17 (14.8) | 0.213 | |
| Smoking, n (%) | 263 (54.8) | 260 (71.2) | 3 (2.6) | <0.001 | |
| Alcohol use, n (%) | 218 (45.4) | 215 (58.9) | 3 (2.6) | <0.001 | |
| Haemoglobin, (g/dL) | 10.9 (4.8) | 11.2 (5.4) | 10.1 (1.8) | 0.032 | |
| Random blood sugar, (mg/dL) | 251.8 (104.5) | 243.6 (99.6) | 277.6 (115.3) | <0.001 | |
| Fasting blood sugar, (mg/dL) | 141.2 (65.2) | 135.9 (63.1) | 115 (68.9) | 0.002 | |
| Postprandial blood sugar, (mg/dL) | 199.8 (94.2) | 189.6 (86.8) | 232.1 (108.7) | <0.001 | |
| Urine ketone bodies, (mg/dL) | 70 (14.6) | 46 (12.6) | 24 (20.9) | 0.034 | |
| Antibiotics | Sensitive | Moderate or Intermediate Sensitive | Resistant |
|---|---|---|---|
| β-lactams | |||
| Aminoglycosides | |||
| Amikacin (30 µg) | 2 (2.9%) | 0 | 68 (97%) |
| Gentamicin (10 µg) | 3 (4.3%) | 0 | 67 (95.7%) |
| Tobramycin (10 µg) | 5 (7.1%) | 0 | 65 (92.9%) |
| Carbapenems | |||
| Imipenem (10 µg) | 6 (8.6%) | 0 | 64 (91.4%) |
| Meropenem (10 µg) | 8 (11.4%) | 0 | 62 (88.6%) |
| Cephalosporins | |||
| Cefepime (30 µg) | 0 | 0 | 70 (100%) |
| Ceftazidime (30 µg) | 0 | 0 | 70 (100%) |
| Cefotaxime (30 µg) | 2 (2.9%) | 0 | 68 (97%) |
| Ceftriaxone (30 µg) | 0 | 0 | 70 (100%) |
| Fluroquinolones | |||
| Ciprofloxacin (5 µg) | 4 (5.7%) | 0 | 66 (94.3) |
| Levofloxacin (5 µg) | 4 (5.7%) | 3 (4.3%) | 63 (90%) |
| Penicillins | |||
| Piperacillin (100 µg) | 1 (1.4%) | 0 | 69 (98.6%) |
| Tetracycline (30 µg) | 3 (4.3%) | 1(1.4%) | 66 (94.3%) |
| Folate-pathway inhibitors | |||
| Trimethoprim/sulfamethoxazole (25 µg) | 4 (5.7%) | 0 | 66 (94.3%) |
| Β-lactam inhibitor combinations | |||
| Piperacillin/tazobactam (30 µg) | 4 (5.7%) | 3 (4.3%) | 63 (90%) |
| Gene | ESBL Producer (n = 17) | Non-ESBL Producer (n = 17) | MBL Producer (n = 17) Producer (n = 17) | Non-MBL Producer (n = 17) |
|---|---|---|---|---|
| blaCTX-M | 1 (5.88%) | 1 (5.88%) | - | - |
| blaSHV | 0 | 0 | - | - |
| blaTEM | 9 (52.94%) | 5 (29.41%) | - | - |
| blaCTX-M + SHV + TEM | 1 (5.88%) | 1 (5.88%) | - | - |
| blaSHV + blaTEM | 1 (5.88%) | 3 (17.64%) | - | - |
| blaCTX-M + blaSHV | 0 | 1 (5.88%) | - | - |
| blaIMP | - | - | 0 | 0 |
| blaVIM | - | - | 0 | 0 |
| blaNDM-1 | - | - | 9 (52.94%) | 10 (58.82%) |
| blaIMP+ VIM + NDM-1 | - | - | 1 (5.88%) | 0 |
| blaVIM + blaNDM-1 | - | - | 0 | 1 (5.88%) |
| blaIMP + blaVIM | - | - | 1 (5.88%) | 2 (11.76%) |
| blaIMP + blaNDM-1 | - | - | 3 (17.64%) | 2 (11.76%) |
| Total | 12 (70.59%) | 11 (64.70%) | 14 (82.35%) | 15 (88.24%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, D.M.; Rao, V.I.; Moosabba, M.S.; MubarakAli, D.; Manzoor, M. Antimicrobial Resistance and Prevalence of β-lactamase Genes Among Multidrug-Resistant Acinetobacter baumannii Isolates from Infected Diabetic Foot Ulcers. Bacteria 2025, 4, 24. https://doi.org/10.3390/bacteria4020024
Khan DM, Rao VI, Moosabba MS, MubarakAli D, Manzoor M. Antimicrobial Resistance and Prevalence of β-lactamase Genes Among Multidrug-Resistant Acinetobacter baumannii Isolates from Infected Diabetic Foot Ulcers. Bacteria. 2025; 4(2):24. https://doi.org/10.3390/bacteria4020024
Chicago/Turabian StyleKhan, Diwan Mahmood, Venkatakrishna I. Rao, M. S. Moosabba, Davoodbasha MubarakAli, and Muhammed Manzoor. 2025. "Antimicrobial Resistance and Prevalence of β-lactamase Genes Among Multidrug-Resistant Acinetobacter baumannii Isolates from Infected Diabetic Foot Ulcers" Bacteria 4, no. 2: 24. https://doi.org/10.3390/bacteria4020024
APA StyleKhan, D. M., Rao, V. I., Moosabba, M. S., MubarakAli, D., & Manzoor, M. (2025). Antimicrobial Resistance and Prevalence of β-lactamase Genes Among Multidrug-Resistant Acinetobacter baumannii Isolates from Infected Diabetic Foot Ulcers. Bacteria, 4(2), 24. https://doi.org/10.3390/bacteria4020024