
Clinical Features and Predictors for Mortality in Neurolisteriosis: An Administrative Data-Based Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Feature Engineering and Preprocessing
2.3. Analyses of Features
3. Results
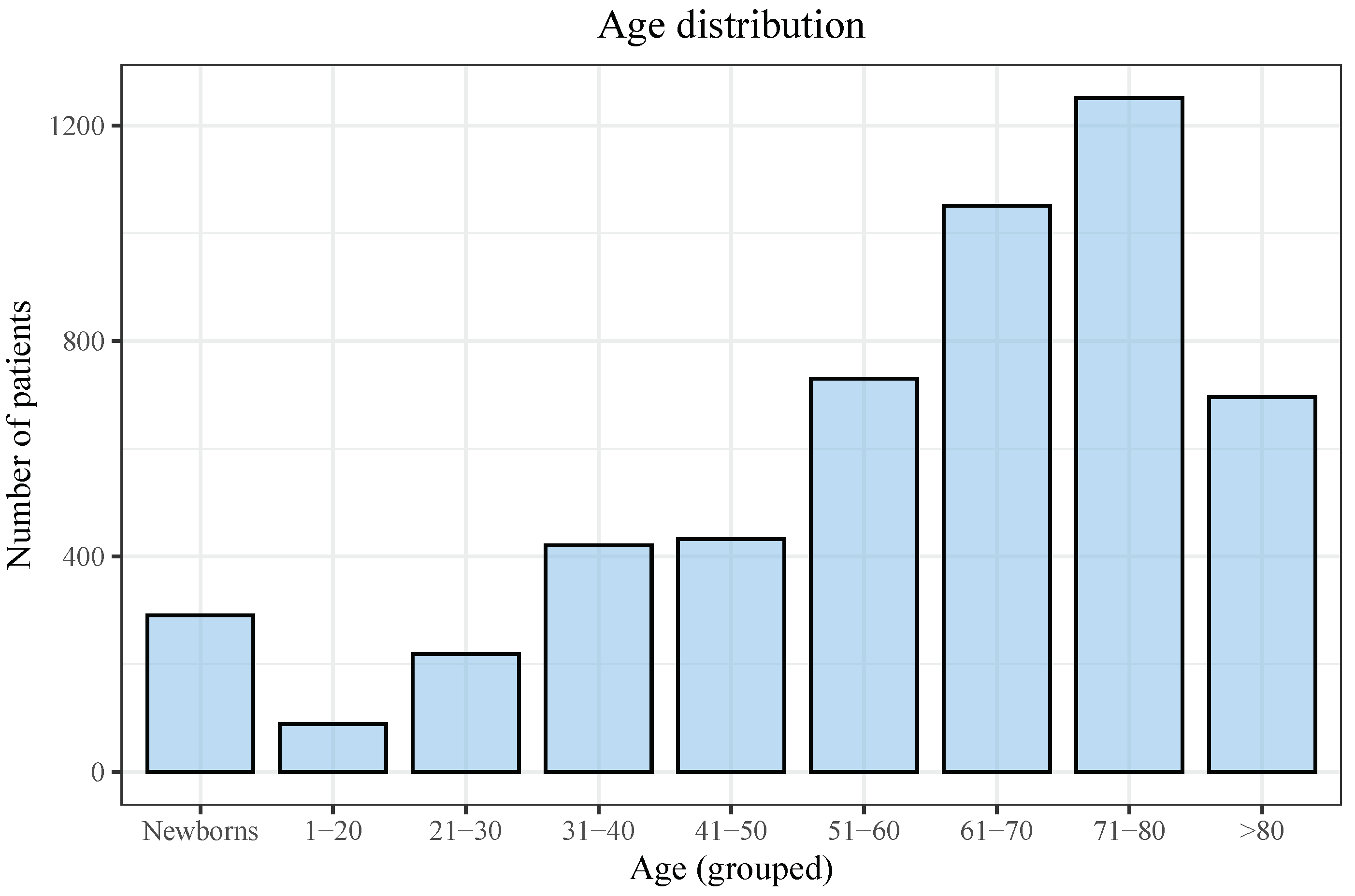
3.1. Descriptive Analyses
3.2. Bivariate and Multivariate Analyses
4. Discussion
Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICD-9 | International Classification of Diseases, 9th Revision |
| ICD-10 | International Classification of Diseases, 10th Revision |
| MBDS | Minimum Basic Data Set |
| COPD | Chronic obstructive pulmonary disease |
| CKD | Chronic kidney disease |
| OR | Odds ratio |
| CNS | Central nervous system |
| EU | European Union |
References
- Swaminathan, B.; Gerner-Smidt, P. The epidemiology of human listeriosis. Microbes Infect. 2007, 9, 1236–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farber, J.M.; Peterkin, P.I. Listeria monocytogenes, a food-borne pathogen. Microbiol. Rev. 1991, 55, 476–511. [Google Scholar] [CrossRef]
- Lorber, B. Listeria Monocytogenes. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Bennett, J., Dolin, R., Blaser, M., Eds.; Elsevier/Saunders’: Philadelphia, PA, USA, 2015; pp. 2383–2390.e2. [Google Scholar] [CrossRef]
- Charlier, C.; Perrodeau, É.; Leclercq, A.; Cazenave, B.; Pilmis, B.; Henry, B.; Lopes, A.; Maury, M.M.; Moura, A.; Goffinet, F.; et al. Clinical features and prognostic factors of listeriosis: The MONALISA national prospective cohort study. Lancet Infect. Dis. 2017, 17, 510–519. [Google Scholar] [CrossRef]
- Herrador, Z.; Gherasim, A.; López-Vélez, R.; Benito, A. Listeriosis in Spain based on hospitalisation records, 1997 to 2015: Need for greater awareness. Eurosurveillance 2019, 24, 1800271. [Google Scholar] [CrossRef]
- Scobie, A.; Kanagarajah, S.; Harris, R.J.; Byrne, L.; Amar, C.; Grant, K.; Godbole, G. Mortality risk factors for listeriosis–A 10 year review of non-pregnancy associated cases in England 2006–2015. J. Infect. 2019, 78, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Pagliano, P.; Ascione, T.; Boccia, G.; De Caro, F.; Esposito, S. Listeria monocytogenes meningitis in the elderly: Epidemiological, clinical and therapeutic findings. Infez. Med. 2016, 24, 105–111. [Google Scholar]
- Mook, P.; Patel, B.; Gillespie, I. Risk factors for mortality in non-pregnancy-related listeriosis. Epidemiol. Infect. 2012, 140, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Elinav, H.; Hershko-Klement, A.; Valinsky, L.; Jaffe, J.; Wiseman, A.; Shimon, H.; Braun, E.; Paitan, Y.; Block, C.; Sorek, R.; et al. Pregnancy-associated listeriosis: Clinical characteristics and geospatial analysis of a 10-year period in Israel. Clin. Infect. Dis. 2014, 59, 953–961. [Google Scholar] [CrossRef] [Green Version]
- Wadhwa Desai, R.; Smith, M.A. Pregnancy-related listeriosis. Birth Defects Res. 2017, 109, 324–335. [Google Scholar] [CrossRef] [Green Version]
- Arslan, F.; Meynet, E.; Sunbul, M.; Sipahi, O.R.; Kurtaran, B.; Kaya, S.; Inkaya, A.C.; Pagliano, P.; Sengoz, G.; Batirel, A.; et al. The clinical features, diagnosis, treatment, and prognosis of neuroinvasive listeriosis: A multinational study. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- de Noordhout, C.M.; Devleesschauwer, B.; Angulo, F.J.; Verbeke, G.; Haagsma, J.; Kirk, M.; Havelaar, A.; Speybroeck, N. The global burden of listeriosis: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 1073–1082. [Google Scholar] [CrossRef] [Green Version]
- Zunt, J.R.; Kassebaum, N.J.; Blake, N.; Glennie, L.; Wright, C.; Nichols, E.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Adamu, A.A.; et al. Global, regional, and national burden of meningitis, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 1061–1082. [Google Scholar] [CrossRef] [Green Version]
- van de Beek, D.; de Gans, J.; Spanjaard, L.; Weisfelt, M.; Reitsma, J.B.; Vermeulen, M. Clinical features and prognostic factors in adults with bacterial meningitis. N. Engl. J. Med. 2004, 351, 1849–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, M.C.; van de Beek, D.; Heckenberg, S.G.B.; Spanjaard, L.; de Gans, J. Community-acquired Listeria monocytogenes meningitis in adults. Clin. Infect. Dis. 2006, 43, 1233–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goulet, V.; Hebert, M.; Hedberg, C.; Laurent, E.; Vaillant, V.; De Valk, H.; Desenclos, J.C. Incidence of Listeriosis and Related Mortality Among Groups at Risk of Acquiring Listeriosis. Clin. Infect. Dis. 2011, 54, 652–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Sanidad Consumo y Bienestar Social. Portal Estadistico. Area de Inteligencia de Gestion. Available online: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/S (accessed on 22 December 2017).
- Maertens De Noordhout, C.; Devleesschauwer, B.; Maertens De Noordhout, A.; Blocher, J.; Haagsma, J.A.; Havelaar, A.H.; Speybroeck, N. Comorbidities and factors associated with central nervous system infections and death in non-perinatal listeriosis: A clinical case series. BMC Infect. Dis. 2016, 16, 256. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Instituto Nacional de Estadística. Población Residente por Fecha, Sexo y Edad; 2019. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=9687 (accessed on 21 December 2019).
- European Food Safety Authority and European Centre for Disease Prevention and Control (EFSA and ECDC). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food-borne outbreaks in 2017. EFSa J. 2018, 16, e05500. [Google Scholar] [CrossRef]
- Vugia, D.; Cronquist, A.; Cartter, M.; Tobin-D’Angelo, M.; Blythe, D.; Smith, K.; Lathrop, S.; Morse, D.; Cieslak, P.; Dunn, J.; et al. Preliminary FoodNet Data on the incidence of infection with pathogens transmitted commonly through food–10 States, 2008. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 333–337. [Google Scholar]
- Scallan, E. Activities, achievements, and lessons learned during the first 10 years of the Foodborne Diseases Active Surveillance Network: 1996–2005. Clin. Infect. Dis. 2007, 44, 718–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- España. Ministerio de Sanidad, Servicios Sociales e Igualdad. Orden SSI/445/2015, de 9 de Marzo, por la que se Modifican los Anexos I, II y III del Real Decreto 2210/1995, de 28 de Diciembre, por el que se crea Ministerio de Sanidad la Red Nacional de Vigilancia Epidemiológica, Relativos a la Lista de Enfermedades de Declaración Obligatoria. 2015, pp. 24012–24015. Available online: https://www.boe.es/eli/es/o/2015/03/09/ssi445 (accessed on 21 December 2019).
- Mailles, A.; Lecuit, M.; Goulet, V.; Leclercq, A.; Stahl, J.P. Listeria monocytogenes encephalitis in France. Med. Mal. Infect. 2011, 41, 594–601. [Google Scholar] [CrossRef]
- Costerus, J.M.; Brouwer, M.C.; van der Ende, A.; van de Beek, D. Community-acquired bacterial meningitis in adults with cancer or a history of cancer. Neurology 2016, 86, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Beamonte Vela, B.N.; Garcia-Carretero, R.; Carrasco-Fernandez, B.; Gil-Romero, Y.; Perez-Pomata, M.T. Listeria monocytogenes infections: Analysis of 41 patients. Med. Clin. 2019, 155, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.A.; Hohmann, S.F.; Hall, J.B.; Kress, J.P.; David, M.Z. Validation of a Method to Identify Immunocompromised Patients with Severe Sepsis in Administrative Databases. Ann. Am. Thorac. Soc. 2016, 13, 253–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Feature Name | Type |
|---|---|
| Patient’s hospital medical record number (hash) | numeric |
| Patient identifier (hash) | numeric |
| Department | categorical |
| Date of birth | date |
| Date of admission | date |
| Date of discharge | date |
| Type of discharge | categorical |
| Main diagnosis + 14 secondary diagnoses (if applicable) | categorical |
| Main procedure + 20 secondary procedures (if applicable) | categorical |
| Type of admission (urgent/scheduled) | categorical |
| Hospital (hash) | numeric |
| Postal code | categorical |
| Billing/insurance type | categorical |
| Date of surgical intervention | date |
| Total (n = 5180) | Neurolisteriosis (n = 2313) | |
|---|---|---|
| Sex (women) | 2130 (41.1%) | 815 (35.2%) |
| Newborns | 291 (5.6%) | 112 (4.8%) |
| Pregnancy | 281 (5.4%) | 1 (0.001%) |
| Adults | 4889 (94.4%) | 2.201 (95%) |
| Age, all patients (median) | 65 (22.6) | 64 (21.2) |
| Age, only adults (median) | 66 (18.2) | 65 (22.6) |
| Clinical presentation | ||
| Neurological (all) | 2313 (44.7%) | 2313 (100%) |
| Meningitis | 2090 (40.3%) | 2090 (90.4%) |
| Encephalomyelitis | 156 (3.0%) | 156 (6.7%) |
| Intracranial abscess | 113 (2.2%) | 113 (4.9%) |
| Endocarditis | 45 (0.9%) | 8 (0.3%) |
| Febrile gastroenteritis | 212 (4.1%) | 51 (2.2%) |
| Sepsis/septic shock | 465 (9.0%) | 167 (7.2%) |
| Death | 879 (17.0%) | 443 (19.2%) |
| Comorbidities | ||
| Diabetes mellitus | 822 (15.9%) | 340 (14.7%) |
| COPD | 492 (9.5%) | 219 (9.5%) |
| Chronic liver disease | 710 (13.7%) | 247 (10.7%) |
| Chronic kidney disease | 468 (9.0%) | 124 (5.4%) |
| Immunosuppression | 2.222 (42.9%) | 810 (35%) |
| Malignancy | 1341 (25.9%) | 412 (17.8%) |
| Mortality (n = 443) | Survival (n = 1870) | p-Value | |
|---|---|---|---|
| Sex (women) | 168 (37.9%) | 647 (34.6%) | 0.207 |
| Newborns | 5 (1.1%) | 107 (5.7%) | <0.001 |
| Pregnancy | 0 (0.0%) | 1 (0.1%) | 0.999 |
| Age, in years (median, IQR) | 73 (15.9) | 62 (21.6) | <0.001 |
| CNS involvement | |||
| Meningitis | 403 (91%) | 1687 (90.2%) | 0.692 |
| Encephalomyelitis | 33 (7.4%) | 123 (6.6%) | 0.580 |
| Intracranial abscess | 23 (5.2%) | 90 (4.8%) | 0.833 |
| Other manifestations | |||
| Endocarditis | 2 (0.5%) | 6 (0.3%) | 0.999 |
| Febrile gastroenteritis | 5 (1.1%) | 46 (2.5%) | 0.124 |
| Sepsis/septic shock | 78 (17.6%) | 89 (4.8%) | <0.001 |
| Comorbidities | |||
| Diabetes mellitus | 74 (16.7%) | 266 (14.2%) | 0.211 |
| COPD | 46 (10.4%) | 173 (9.3%) | 0.521 |
| Chronic liver disease | 62 (14%) | 185 (9.9%) | 0.150 |
| CKD | 45 (10.2%) | 79 (4.2%) | <0.001 |
| Immunosuppression | 195 (44%) | 615 (32.9%) | <0.001 |
| Malignancy | 130 (29.3%) | 282 (15.1%) | <0.001 |
| Odds Ratio | 2.5% | 97.5% | p-Value | |
|---|---|---|---|---|
| Age | 1.039 | 1.031 | 1.047 | <0.001 |
| Sepsis/septic shock | 4.527 | 3.190 | 6.430 | <0.001 |
| Chronic liver disease | 1.625 | 1.161 | 2.250 | 0.004 |
| CKD | 2.048 | 1.355 | 3.061 | <0.001 |
| Immunosuppression | 1.133 | 0.838 | 1.521 | 0.410 |
| Malignancy | 2.154 | 1.540 | 3.025 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Carretero, R. Clinical Features and Predictors for Mortality in Neurolisteriosis: An Administrative Data-Based Study. Bacteria 2022, 1, 3-11. https://doi.org/10.3390/bacteria1010002
Garcia-Carretero R. Clinical Features and Predictors for Mortality in Neurolisteriosis: An Administrative Data-Based Study. Bacteria. 2022; 1(1):3-11. https://doi.org/10.3390/bacteria1010002
Chicago/Turabian StyleGarcia-Carretero, Rafael. 2022. "Clinical Features and Predictors for Mortality in Neurolisteriosis: An Administrative Data-Based Study" Bacteria 1, no. 1: 3-11. https://doi.org/10.3390/bacteria1010002
APA StyleGarcia-Carretero, R. (2022). Clinical Features and Predictors for Mortality in Neurolisteriosis: An Administrative Data-Based Study. Bacteria, 1(1), 3-11. https://doi.org/10.3390/bacteria1010002