
Anti-IL-6 Receptor Treatment in Giant Cell Arteritis Patients Reduces Levels of IL-1β-Receptor Antagonist but Not IL-1β

 , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
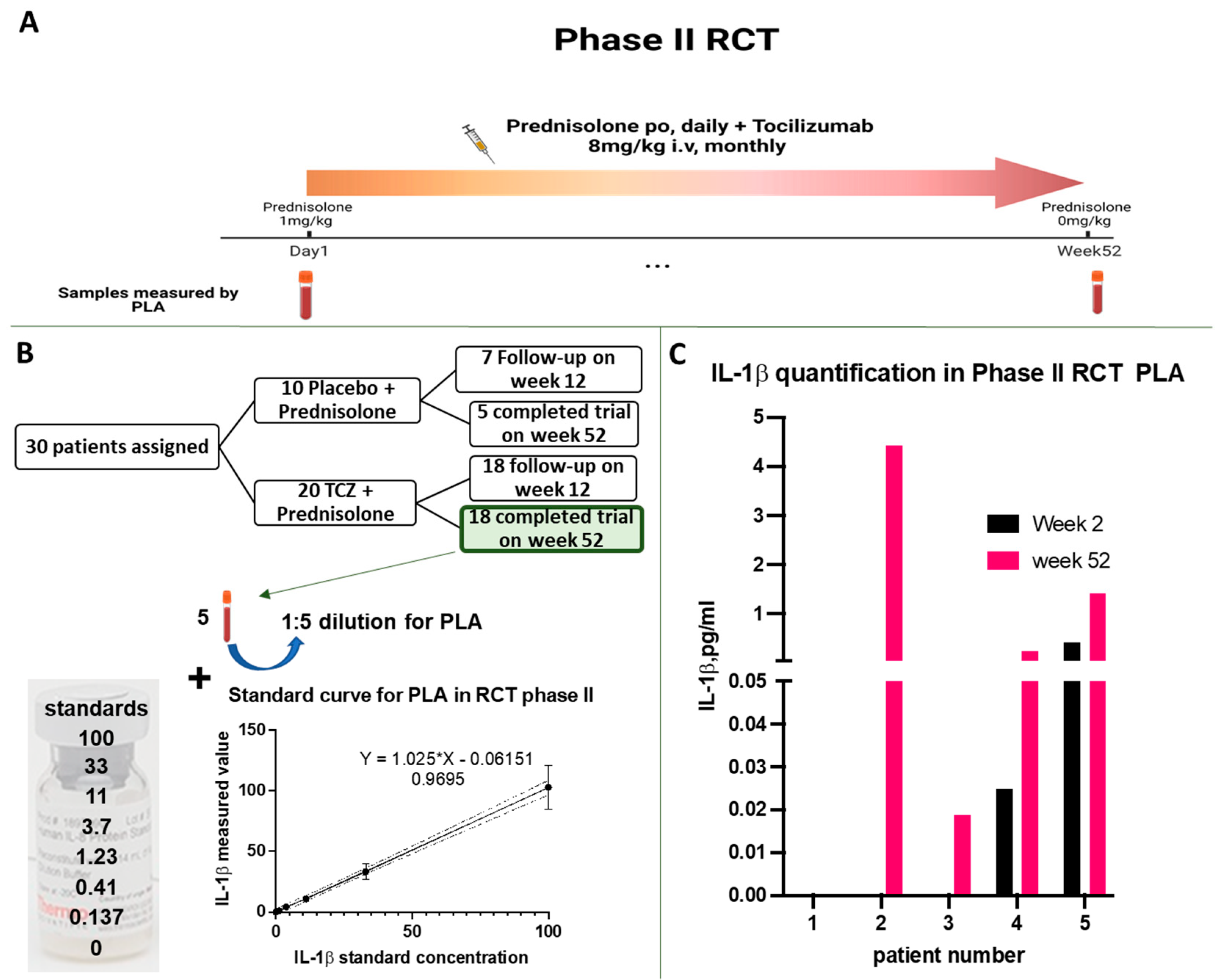
2.1. Phase II RCT for GCA
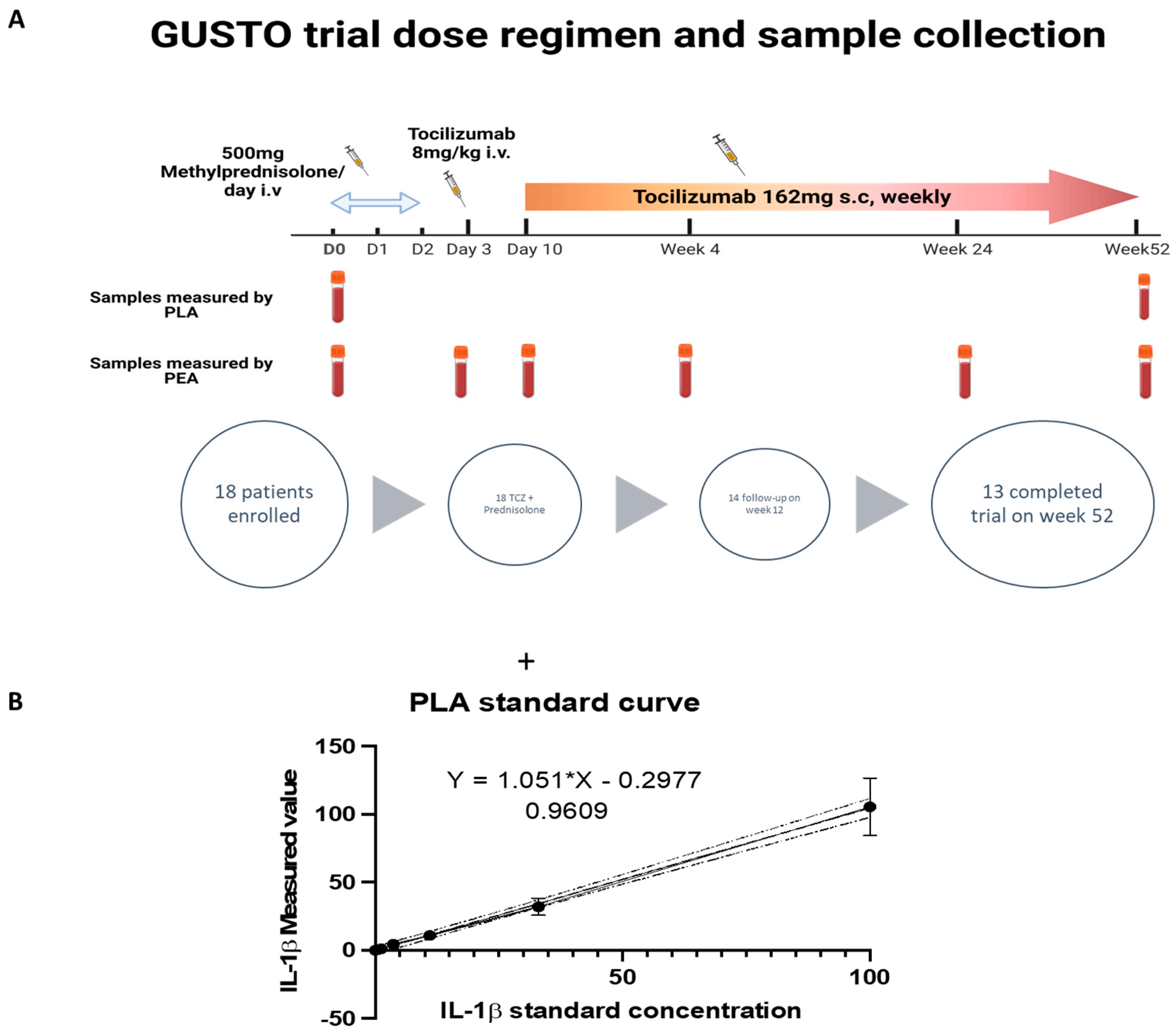
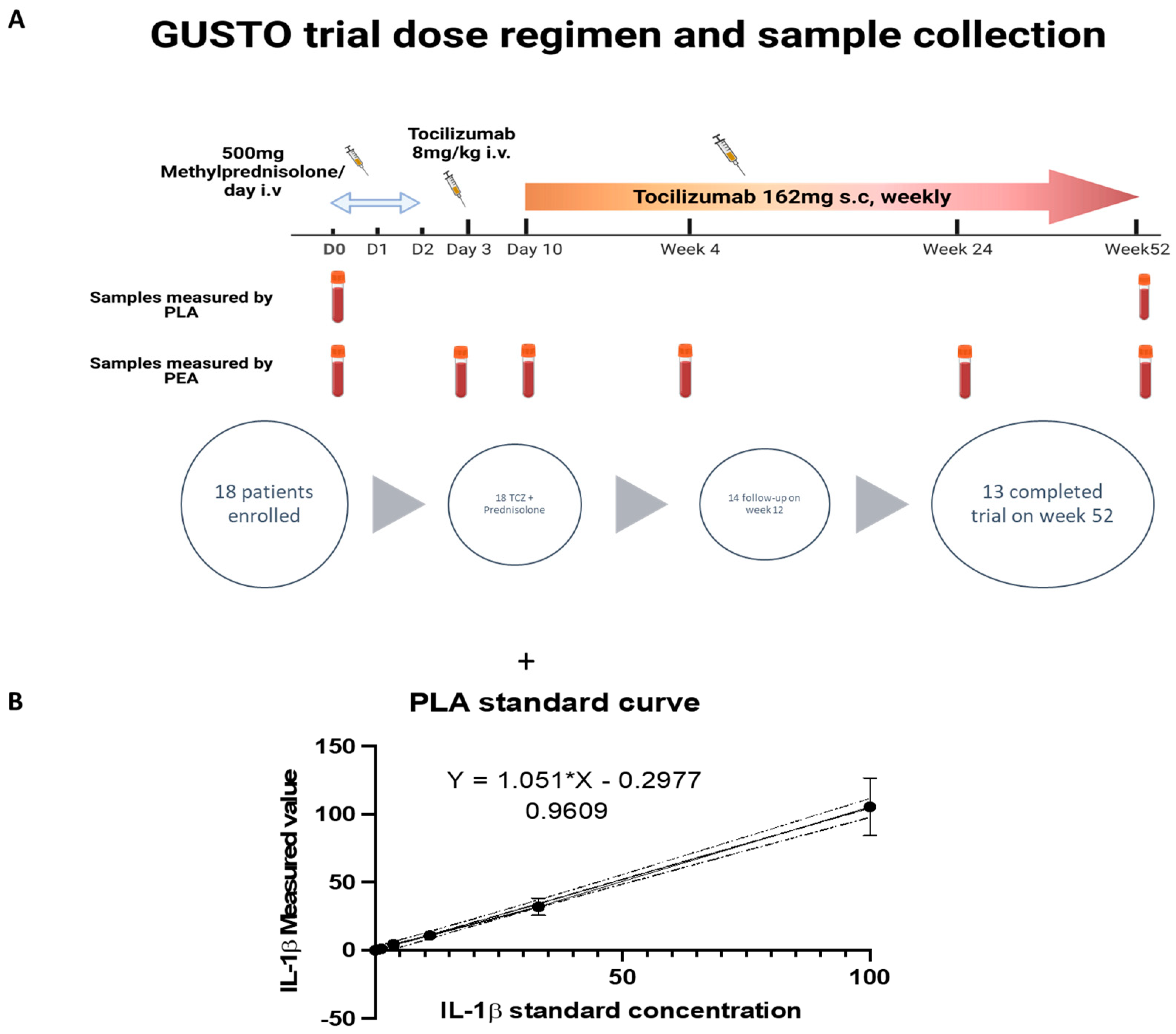
2.2. The GUSTO Trial
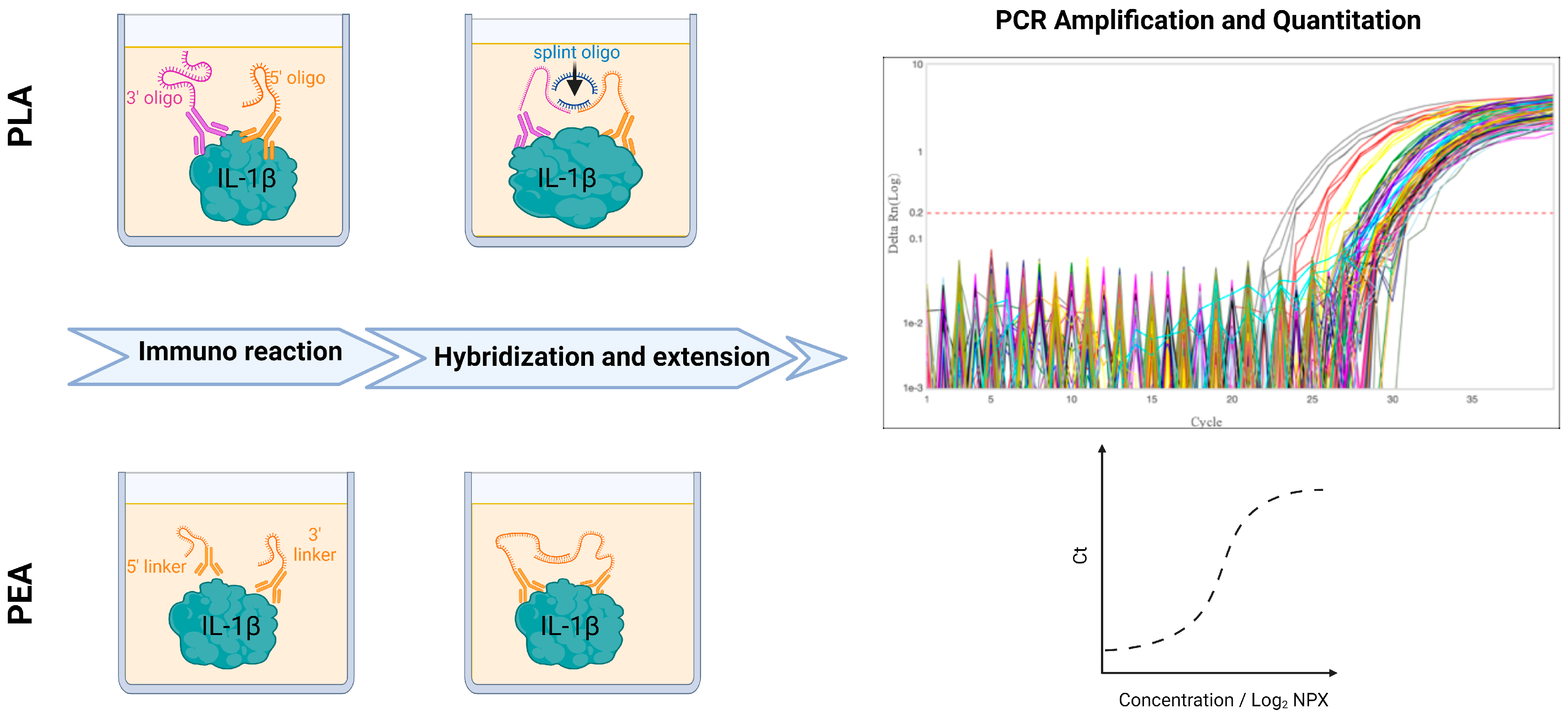
2.3. Measurement of Serum IL-1β Using Proximity Ligation Assay (PLA)
2.4. Measurement of Serum IL-1β Using Proximity Extension Assay (PEA)
2.5. Statistics
3. Results
3.1. Proof of Concept: Analysis of IL-1β in Phase II RCT for GCA Using PLA
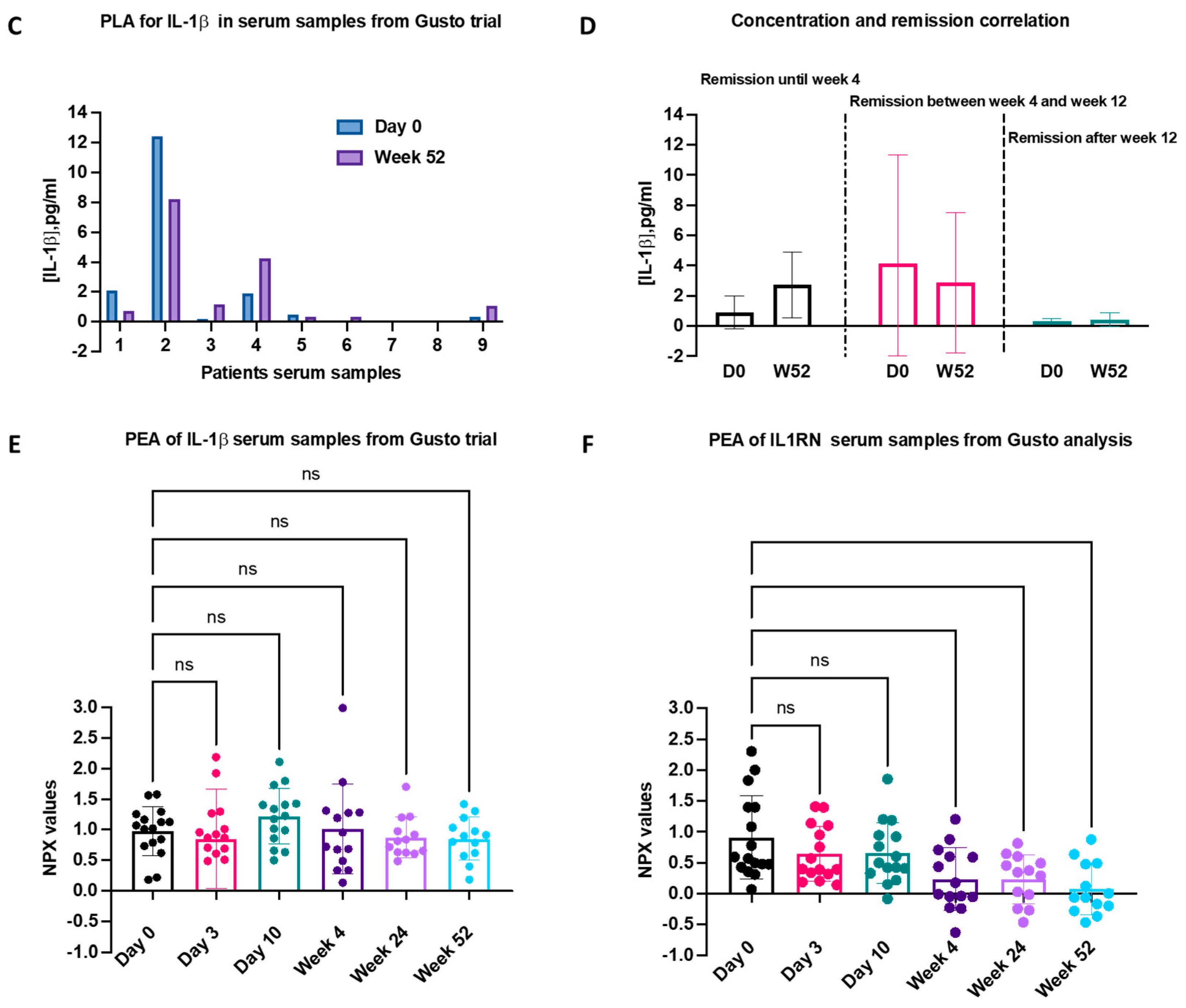
3.2. Comparison of IL-1β Serum Levels in the GUSTO Trial Using PLA and PEA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Legge, W. The Journal. Br. Med. J. 1859, s4-1, 880. [Google Scholar] [CrossRef]
- Ozcicek, F.; Kara, A.V.; Akbas, E.M.; Kurt, N.; Yazici, G.N.; Cankaya, M.; Mammadov, R.; Ozcicek, A.; Suleyman, H. Effects of anakinra on the small intestine mucositis induced by methotrexate in rats. Exp. Anim. 2020, 69, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Dhimolea, E. Canakinumab. MAbs 2010, 2, 3–13. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M. Rilonacept in the treatment of chronic inflammatory disorders. Drugs Today 2009, 45, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Ruscitti, P.; Masedu, F.; Alvaro, S.; Airò, P.; Battafarano, N.; Cantarini, L.; Cantatore, F.P.; Carlino, G.; D’Abrosca, V.; Frassi, M.; et al. Anti-interleukin-1 treatment in patients with rheumatoid arthritis and type 2 diabetes (TRACK): A multicentre, open-label, randomised controlled trial. PLoS Med. 2019, 16, e1002901. [Google Scholar] [CrossRef] [PubMed]
- A Walker, U.; Tilson, H.H.; Hawkins, P.N.; van der Poll, T.; Noviello, S.; Levy, J.; Vritzali, E.; Hoffman, H.M.; Kuemmerle-Deschner, J.B. Long-term safety and effectiveness of canakinumab therapy in patients with cryopyrin-associated periodic syndrome: Results from the β-Confident Registry. RMD Open 2021, 7, e001663. [Google Scholar] [CrossRef] [PubMed]
- Kharouf, F.; Tsemach-Toren, T.; Ben-Chetrit, E. IL-1 inhibition in familial Mediterranean fever: Clinical outcomes and expectations. Clin. Exp. Rheumatol. 2022, 40, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Galozzi, P.; Bindoli, S.; Doria, A.; Sfriso, P. Progress in Biological Therapies for Adult-Onset Still’s Disease. Biologics 2022, 16, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Haibel, H.; Poddubnyy, D.; Angermair, S.; Allers, K.; Vahldiek, J.L.; Schumann, M.; Schneider, T. Successful treatment of severe COVID-19 pneumonia, a case series with simultaneous interleukin-1 and interleukin-6 blockade with 1-month follow-up. Ther. Adv. Musculoskelet. Dis. 2022, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; MacFadyen, J.G.; Everett, B.M.; Libby, P.; Thuren, T.; Glynn, R.J.; Kastelein, J.; Koenig, W.; Genest, J.; Lorenzatti, A.; et al. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: A secondary analysis from the CANTOS randomised controlled trial. Lancet 2018, 391, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.D.; Nedjai, B.; Hurst, T.; Pennington, D.J. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochim. Biophys. Acta 2014, 1843, 2563–2582. [Google Scholar] [CrossRef]
- Rodríguez-Pla, A.; Bosch-Gil, J.A.; Rosselló-Urgell, J.; Huguet-Redecilla, P.; Stone, J.H.; Vilardell-Tarres, M. Metalloproteinase-2 and -9 in Giant Cell Arteritis. Circulation 2005, 112, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Emilie, D.; Liozon, E.; Crevon, M.-C.; Lavignac, C.; Portier, A.; Liozon, F.; Galanaud, P. Production of interleukin 6 by granulomas of giant cell arteritis. Hum. Immunol. 1994, 39, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Villiger, P.M.; Adler, S.; Kuchen, S.; Wermelinger, F.; Dan, D.; Fiege, V.; Bütikofer, L.; Seitz, M.; Reichenbach, S. Tocilizumab for induction and maintenance of remission in giant cell arteritis: A phase 2, randomised, double-blind, placebo-controlled trial. Lancet 2016, 387, 1921–1927. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H.; Tuckwell, K.; Dimonaco, S.; Klearman, M.; Aringer, M.; Blockmans, D.; Brouwer, E.; Cid, M.C.; Dasgupta, B.; Rech, J.; et al. Trial of Tocilizumab in Giant-Cell Arteritis. N. Engl. J. Med. 2017, 377, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Christ, L.; Seitz, L.; Scholz, G.; Sarbu, A.-C.; Amsler, J.; Bütikofer, L.; Tappeiner, C.; Kollert, F.; Reichenbach, S.; Villiger, P.M. Tocilizumab monotherapy after ultra-short glucocorticoid administration in giant cell arteritis: A single-arm, open-label, proof-of-concept study. Lancet Rheumatol. 2021, 3, e619–e626. [Google Scholar] [CrossRef] [PubMed]
- Gloor, A.D.; Yerly, D.; Adler, S.; Reichenbach, S.; Kuchen, S.; Seitz, M.; Villiger, P.M. Immuno-monitoring reveals an extended subclinical disease activity in tocilizumab-treated giant cell arteritis. Rheumatology 2018, 57, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Régent, A.; Mouthon, L. Treatment of Giant Cell Arteritis (GCA). J. Clin. Med. 2022, 11, 1799. [Google Scholar] [CrossRef] [PubMed]
- Christ, L.; Gloor, A.D.; Kollert, F.; Gaber, T.; Buttgereit, F.; Reichenbach, S.; Villiger, P.M. Serum proteomics in giant cell arteritis in response to a three-day pulse of glucocorticoid followed by tocilizumab monotherapy (the GUSTO trial). Front. Immunol. 2023, 14, 1165758. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, C.M.; Lu, C.; Corbin, K.L.; Sharma, P.R.; Dula, S.B.; Carter, J.D.; Ramadan, J.W.; Xin, W.; Lee, J.K.; Nunemaker, C.S. Circulating Levels of IL-1B+IL-6 Cause ER Stress and Dysfunction in Islets From Prediabetic Male Mice. Endocrinology 2013, 154, 3077–3088. [Google Scholar] [CrossRef] [PubMed]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Björkesten, J.; Thorsen, S.B.; Ekman, D.; Eriksson, A.; Dickens, E.R.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-Plex PEA Immunoassay Exhibiting High Sensitivity, Specificity, and Excellent Scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef]
- Fredriksson, S.; Gullberg, M.; Jarvius, J.; Olsson, C.; Pietras, K.; Gústafsdóttir, S.M.; Östman, A.; Landegren, U. Protein detection using proximity-dependent DNA ligation assays. Nat. Biotechnol. 2002, 20, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, C.; Ruff, D.; Kirvell, S.; Johnson, G.; Dhillon, H.S.; Bustin, S.A. Proximity assays for sensitive quantification of proteins. Biomol. Detect. Quantif. 2015, 4, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. A clinical perspective of IL-1β as the gatekeeper of inflammation. Eur. J. Immunol. 2011, 41, 1203–1217. [Google Scholar] [CrossRef] [PubMed]
- Platchek, M.; Lu, Q.; Tran, H.; Xie, W. Comparative Analysis of Multiple Immunoassays for Cytokine Profiling in Drug Discovery. SLAS Discov. Adv. Sci. Drug Discov. 2020, 25, 1197–1213. [Google Scholar] [CrossRef] [PubMed]
- Bedin, F.; Benoit, V.; Ferrazzi, E.; Aufradet, E.; Boulet, L.; Rubens, A.; Dalbon, P.; Imbaud, P. Procalcitonin detection in human plasma specimens using a fast version of proximity extension assay. PLoS ONE 2023, 18, e0281157. [Google Scholar] [CrossRef]
- Pountain, G.; Hazleman, B.; Cawston, T.E. Circulating levels of IL-1beta, IL-6 and soluble IL-2 receptor in polymyalgia rheumatica and giant cell arteritis and rheumatoid arthritis. Br. J. Rheumatol. 1998, 37, 797–798. [Google Scholar] [CrossRef]
- Hernandez-Rodriguez, J.; Segarra, M.; Vilardell, C.; Sánchez, M.; García-Martínez, A.; Esteban, M.J.; Queralt, C.; Grau, J.M.; Urbano-Márquez, A.; Palacín, A.; et al. Tissue production of pro-inflammatory cytokines (IL-1β, TNFα and IL-6) correlates with the intesity of the systemic inflammatory response and with corticosteroid requirements in giant-cell arteritis. Rheumatology 2003, 43, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Jimbo, K.; Park, J.S.; Yokosuka, K.; Sato, K.; Nagata, K. Positive feedback loop of interleukin-1β upregulating production of inflammatory mediators in human intervertebral disc cells in vitro. J. Neurosurg. Spine 2005, 2, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Nicklin, M.J.; Hughes, D.E.; Barton, J.L.; Ure, J.M.; Duff, G.W. Arterial Inflammation in Mice Lacking the Interleukin 1 Receptor Antagonist Gene. J. Exp. Med. 2000, 191, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Burger, D.; Chicheportiche, R.; Giri, J.G.; Dayer, J.M. The Inhibitory Activity of Human Interleukin-1 Receptor Antagonist Is Enhanced by Type 11 Interleukin-1 Soluble Receptor and Hindered by Type I Interleukin-1 Soluble Receptor. J. Clin. Investig. 1995, 96, 38–41. [Google Scholar] [CrossRef] [PubMed]
- O’neill, L.; McCormick, J.; Gao, W.; Veale, D.J.; McCarthy, G.M.; Murphy, C.C.; Fearon, U.; Molloy, E.S. Interleukin-6 does not upregulate pro-inflammatory cytokine expression in an ex vivo model of giant cell arteritis. Rheumatol. Adv. Pract. 2019, 3, rkz011. [Google Scholar] [CrossRef] [PubMed]
- Ly, K.-H.; Stirnemann, J.; Liozon, E.; Michel, M.; Fain, O.; Fauchais, A.-L. Interleukin-1 blockade in refractory giant cell arteritis. Jt. Bone Spine 2014, 81, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Deshayes, S.; Ly, K.H.; Rieu, V.; Maigné, G.; Martin Silva, N.; Manrique, A.; Monteil, J.; de Boysson, H.; Aouba, A.; French Study Group for Large Vessel Vasculitis (GEFA). Steroid-sparing effect of anakinra in giant-cell arteritis: A case series with clinical, biological and iconographic long-term assessments. Rheumatology 2022, 61, 400–406. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Costa, J.J.; Christ, L.; Villiger, P.M.; Vogel, M.; Bachmann, M.F. Anti-IL-6 Receptor Treatment in Giant Cell Arteritis Patients Reduces Levels of IL-1β-Receptor Antagonist but Not IL-1β. Rheumato 2024, 4, 63-74. https://doi.org/10.3390/rheumato4020006
da Costa JJ, Christ L, Villiger PM, Vogel M, Bachmann MF. Anti-IL-6 Receptor Treatment in Giant Cell Arteritis Patients Reduces Levels of IL-1β-Receptor Antagonist but Not IL-1β. Rheumato. 2024; 4(2):63-74. https://doi.org/10.3390/rheumato4020006
Chicago/Turabian Styleda Costa, Joana J., Lisa Christ, Peter M. Villiger, Monique Vogel, and Martin F. Bachmann. 2024. "Anti-IL-6 Receptor Treatment in Giant Cell Arteritis Patients Reduces Levels of IL-1β-Receptor Antagonist but Not IL-1β" Rheumato 4, no. 2: 63-74. https://doi.org/10.3390/rheumato4020006
APA Styleda Costa, J. J., Christ, L., Villiger, P. M., Vogel, M., & Bachmann, M. F. (2024). Anti-IL-6 Receptor Treatment in Giant Cell Arteritis Patients Reduces Levels of IL-1β-Receptor Antagonist but Not IL-1β. Rheumato, 4(2), 63-74. https://doi.org/10.3390/rheumato4020006