Abstract
Inflammatory bowel disease (IBD) is a group of heterogeneous chronic inflammatory diseases of the gut presenting with intestinal and extraintestinal manifestations. Most cases fit in predominantly two types, namely, ulcerative colitis and Crohn’s disease. The incidence of IBD has been increasing steadily in the past three decades. Focused research has resulted in many therapeutic options. Biologics (derived from humans or animals) and small molecules have emerged as the cornerstone in the management of IBD and have become widely available. Currently, monoclonal antibodies against tumor necrosis factor-alpha (infliximab, adalimumab, certolizumab, and golimumab), integrins (vedolizumab and natalizumab), and interleukin (IL)-12 and IL-23 antagonists (ustekinumab), along with small molecules (tofacitinib), are approved for use. This article summarizes various aspects of these drugs, like clinical pharmacology, indications for use in IBD, safety in pregnancy and lactation, and the adverse effects profile based on the studies leading to their approval. This review also focuses on the recent advances and future perspectives specific to biologics in IBD.
1. Introduction
Inflammatory bowel disease (IBD) is a cause of an important problem to the healthcare setup of any country, as both ulcerative colitis (UC) and Crohn’s disease (CD) require long-term therapy and continuous monitoring. Although it is noted in high proportions in northern and western Europe, North America, and Australia, the geographic distribution is noticeably wider, with an increasing prevalence even in countries that were initially considered low-risk areas [1,2]. Epidemiological studies from South Asia have shown UC to be more prevalent than CD, with an increasing trend of CD [2,3].
The therapeutics of IBD have witnessed a rapid evolution over the past several decades (Figure 1). From the advent of the chimeric monoclonal anti-tumor necrosis factor (TNF)-alpha antibody infliximab in the 1990s [4], to the development of newer biologics and small molecule agents, all reflect change in therapeutic targets with the common aim of achieving deep remission, the amalgamation of clinical remission and mucosal healing in IBD [5]. Agents like anti-integrin (vedolizumab), anti-interleukin (IL)-12/23 p40 (ustekinumab), anti-IL-23p19 (risankizumab), oral Janus kinase (JAK) inhibitors (tofacitinib, upadacitinib), and sphingosine-1-phosphate (S1P) receptor modulator (ozanimod) have been recently approved for management of IBD, thus expanding therapeutic armamentarium [6].
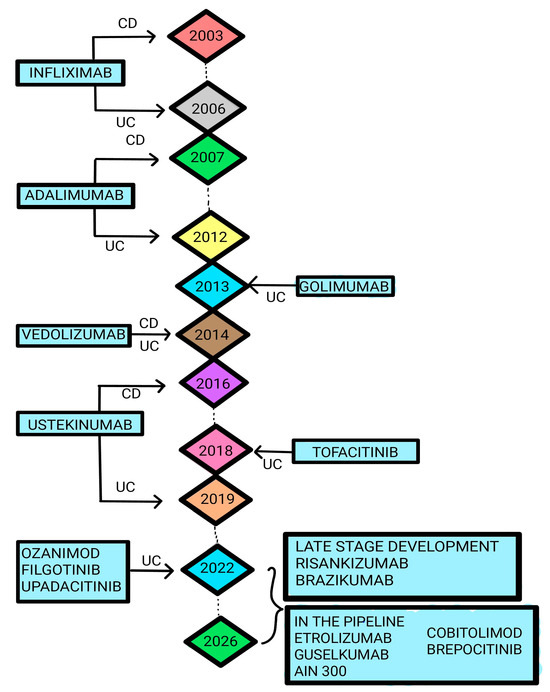
Figure 1.
Timeline for the different biologicals and small molecules approved by FDA and in the development process for the treatment of IBD. Adapted from [7], MDPI, 2023.
This review is an attempt in the direction of summarizing the available evidence on the use of biologics and small molecules in the ever-changing therapeutic goals of IBD and the emerging trends.
2. Materials and Methods
A literature search was conducted using the following ‘MeSH’ terms in the ‘PubMed’ database: ‘Inflammatory bowel disease’, ‘Ulcerative colitis’, and ‘Crohn’s disease’. The keywords “therapy”, “biologicals”, and “small molecules” were also used. Once the relevant literature was identified, a literature search was performed using individual drugs in the ‘PubMed’, ‘EMBASE’, and ‘Web of Science’ databases. Identified titles, abstracts, and some full-text articles were used by four independent reviewers while writing this review. The majority of the articles included in this review are from the last three decades.
3. Anti-TNF Therapy in IBD: The Evidence
During the last decade of the last century, tumor necrosis factor (TNF) was implicated (for the first time) in inflammatory bowel disease (IBD) when patients were shown to have elevated levels in serum [1], stool [2], and mucosal biopsy [3]. Subsequently, the first report of successful use of anti-TNF therapy was published [4] and established the clear association of TNF in the pathogenesis of IBD. Amongst the anti-TNF medications, infliximab (IFX) was the first monoclonal antibody that was approved for the management of IBD, and subsequently, adalimumab (ADA) and golimumab (GLM) have also been approved.
3.1. Infliximab
IFX, an intravenously administered chimeric IgG1 monoclonal antibody, was the first biological to be approved for the management of IBD and has been in use for more than 20 years. Data that have come from the past two decades are summarized in the table. It is, however, important to note that 30% have a primary non-response (PNR), and of those who respond, 50% have to stop or switch due to a loss of response (LOR) or develop serious adverse effects (SAE), which mandate switching or stopping. A loss of response to IFX is on most occasions due to low trough levels of the drug during the maintenance phase because of non-immune or antibody-mediated immune clearance [5], justifying the need for therapeutic drug monitoring (TDM) by the measurement of the drug concentration and antibody titers. TDM helps a clinician to effectively optimize the therapy and favorable outcomes [6].
3.1.1. Infliximab in Crohn’s Disease
The first double-blind placebo-controlled trial (TAGRAN Study) employed patients with moderate to severe CD who were randomized to receive a single intravenous infusion of either the placebo or IFX in a dose of 5, 10, or 20 mg/kg, with the primary outcome being defined as a reduction of ≥70 in the Crohn’s Disease Activity Index (CDAI) at 4 weeks. It was also important that it was not accompanied by a change in any concomitant medications. A significant response was seen at 4 weeks with 81%, 50%, and 64% in the 5, 10, and 20 mg/kg groups having a clinical response as compared to only 17% of patients in the placebo group (p < 0.001). A secondary outcome (clinical remission defined by a CDAI < 150) was achieved by 33% of patients treated with IFX as opposed to only 4% of the patients given the placebo (p = 0.005). There was a difference in the rates of adverse events [8].
The landmark ACCENT I trial was a randomized double-blind placebo-controlled trial of IFX in the long-term management of patients with moderate to severe Crohn’s disease with a CDAI score of at least 220. The patients received 5 mg/kg IFX at enrolment (week 0) and were assessed at week 2, wherein they were randomized to receive the placebo (group I), 5 mg/kg (group II), or 10 mg/kg IFX (group III) at 2 and 6 weeks and then every 8 weeks thereafter until week 46. Primary outcomes included (a) the proportion of patients who responded at two weeks and were in remission (CDAI < 150) at week 30 and (b) the time to loss of response up to 54 weeks in patients who responded at week 0. At 2 weeks, 58% of the patients had a documented response to a single infusion of IFX. At 30 weeks, 21% (group I), 39% (group II), and 45% (group III) of patients had achieved the desired endpoint (p = 0.003 and 0.0002, respectively). As a cohort, the patients in groups II and III when combined were more likely to sustain clinical remission (odds ratio 2.7, 95% confidence interval 1.6–4.6). Over the 54-week trial, the median time to a loss of response was 38 weeks and >54 weeks for groups II and III, respectively, compared with 19 weeks for group I (p = 0.002 and 0.0002, respectively). Like in the previous trials, the incidence of serious infections was similar across treatment groups [9].
In another placebo-controlled RCT within 02 years of the TAGRAN study, patients with CD with draining abdominal or perianal fistulas were assigned to the placebo, 5, or 10 mg/kg of IFX at 0, 2, and 6 weeks, with the primary outcome being a reduction of ≥50% in the number of draining fistulas observed over subsequent visits. Complete closure of the fistulas was also included as a secondary end point. At least a 50% closure of fistulas was seen in 68% and 56% in the IFX group (5 and 10 mg/kg), which was significantly higher than the placebo (26%). The secondary end point of closure was seen in 55% and 38% in the therapeutic arms (5 and 10 mg/kg, respectively) as compared to 13% in the placebo (p = 0.001 and p = 0.04, respectively). Similar to the TAGRAN study, there was no difference in the rates of adverse events, and the common adverse events included headache, upper respiratory tract infection, and fatigue [10].
ACCENT II, a randomized, double-blind, placebo-controlled trial, assessed the role of IFX in the long-term management of patients with fistulizing Crohn’s disease. It included patients with one or more draining abdominal or perianal fistulas for at least a 3-month duration. All patients received an induction dose of 5 mg/kg of IFX in weeks 0, 2, and 6. A response was defined as a reduction from a baseline CDAI ≥220 by at least 25% or 70 points. Patients who showed a response (n = 195) or had no response (n = 87) were then randomized to the placebo (group I) or 5 mg/kg (group II) of IFX every 8 weeks and were followed for 54 weeks. The primary endpoint, time to loss of follow-up, was longer for patients on IFX maintenance than for those receiving the placebo (>40 weeks versus 14 weeks, p < 0.001). The secondary endpoint, the complete absence of draining fistulas at 54 weeks, was achieved in 36% of patients on IFX compared to 19% of placebo-treated patients (p = 0.009) [11].
The SONIC trial, a randomized, double-blind trial, evaluated the combinations of azathioprine and IFX in 508 adults with moderate-to-severe CD who were naïve to immunosuppressive or biologic therapy. Patients were randomly allocated to receive 5 mg/kg IFX with or without azathioprine. Over 26 weeks of follow-up, patients on combination therapy had a higher rate of steroid-free remission than those on IFX alone (56.8 versus 44.4%, p = 0.02) or azathioprine monotherapy (56.8% versus 30%, p < 0.001). Mucosal healing was also significantly better with combination therapy as compared to monotherapy with IFX (43.9 versus 30.1%, p = 0.06) or azathioprine (43.9 versus 16.5%, p < 0.001). Two additional important points were highlighted in the study. Firstly, the incidence of adverse events was similar among the three groups, and, secondly, infusion reactions to IFX occurred in only 5% of patients in the combination therapy group compared with 16.6% in the IFX group (p < 0.001) [12].
In addition to the multiple RCTs that have been conducted for IFX, large data for the clinical efficacy and adverse effect profile also exist in the way of large observational studies, which typically reflect real-life clinical practice and have longer a follow-ups. Almost all studies validate the results of the RCTs, a large observational cohort study at a single center with 614 patients who were followed up for more than 04 years showed a primary non-response rate of only 10.9% and two-thirds of the initial responders (63.4%) had a sustained clinical benefit with a persistent improvement of the symptoms. The study also noted that approximately half the initial responders required modifications in the dosing, like frequent dosing (19.3%), increased dose or reinduction (26.3%), or a combination of both (3.8%). Five patients had serious infections necessitating IFX discontinuation [13].
Another study from the same center compared the side effect profile between IFX-treated patients (n = 734) and a control group (n = 666). Both groups had similar incidences of serious adverse effects (13 vs. 19%, p = 0.45), serious infections (1.6 vs. 1.1/100 patient-years), and mortality (0.3 versus 0.2/100 patient-years) [14].
A retrospective study analyzed the prediction of IFX failure in 261 patients who had responded to IFX and were on scheduled maintenance therapy. IFX failure was seen in 24.9% of patients over a median follow-up of 2.4 years. IFX optimization was required in 62.5% of patients, with the first modification at 41 weeks. A disease duration ≥1 year (HR 2.5, 95% CI 1.2–5.2, p = 0.02), L1 disease (HR 2, 95% CI 1.1–3.5, p = 0.02), prior anti-TNF use (HR 2.3, 95% CI 1.1–4.8, p = 0.03), Hb < 13.5 g/dL (HR 2.3, 95% CI 1.2–4.4, p = 0.02), not using TDM (HR 8, 95% CI 4.1–15.6, p < 0.001), and dose optimization within the first year (HR 3.7, 95% CI 2.1–6.6, p < 0.001) were independent predictors of IFX failure-free treatment [15].
Another retrospective, single-center study with 351 participants showed female gender (HR 2.1, 95% CI 1.4–3.3, p < 0.001) and body mass index (BMI) ≥ 23.4 (HR 1.7, 95% CI 1.1–2.7, p = 0.034) as independent factors associated with the persistence of first-line treatment with IFX [16].
Still, larger studies (registries and meta-analyses) have also evaluated IFX in the management of CD. The TREAT registry conducted a prospective study examining long-term outcomes of CD in the community in patients receiving IFX (n = 3400) or other therapies (n = 2833). Serious infection rates were significantly higher for the IFX group (2.15 versus 0.86/100 person-years) with pneumonia being the commonest. The use of steroids, age, and disease duration at enrollment, moderate/severe disease, and colonic disease independently predicted serious infections. Mortality (0.57 versus 0.67/100 person-years) and malignancy rates (0.69 versus 0.71/100 person-years) were similar between patients [17]. A pooled analysis of IFX RCTs in CD has shown similar rates of malignancy (0.49 versus 1.61/100 person-years) and mortality (0.24 versus 0.8/100 person-years) [18]. A systematic review of RCTs between January 1980 and May 2016 examined the efficacy of biological or immunomodulator therapy in CD and showed significantly reduced hospitalization (OR 0.46, 95% CI 0.36–0.6) and surgery (OR 0.23, 95% CI 0.13–0.42) compared with the placebo [19].
A recently published network meta-analysis compared the efficacy (induction and maintenance of clinical remission) and safety (SAEs and infections) of biological therapy in patients with at least moderate CD using surface under the cumulative ranking (SUCRA) probabilities. IFX ranked highest for the induction of clinical remission (SUCRA 0.93) and ranked highest for the maintenance of remission (SUCRA 0.68) [20].
3.1.2. Infliximab in the Postoperative Recurrence of CD
IFX has also been evaluated in the management of prophylaxis of postoperative recurrence after ileocolonic resection for CD. A double-blind RCT assessed the role of IFX in preventing postoperative recurrence in patients following an ileocolonic resection for CD, wherein patients were randomized to receive IFX or a placebo. The primary outcome included the proportion of patients with endoscopic recurrence at 1 year. The rates of recurrence were much higher in the placebo group at 84.6% vs. 9.1%, p = 0.0006) [21]. The study was followed up as a prospective open-label long-term follow-up and the patients were given the option to continue, stop, or start IFX therapy with the endpoint being the time to endoscopic recurrence from the initial randomization to postoperative IFX or placebo. Patients who received IFX in the first year post-surgery had a longer mean time to first recurrence (1231 ± 747 days vs. 460 ± 121 days, p = 0.003) [22]. Another RCT included 21 CD patients after curative ileocolonic resection managed with IFX (group I) and azathioprine (group II). The rate of recurrence was higher among the azathioprine group (40% vs. 9%, p = 0.14). Histological activity was persistent in about 80% of patients treated with azathioprine as compared to 18% of the IFX-treated patients (p = 0.008) [23].
The PREVENT trial was a prospective, multicenter, randomized, double-blind, placebo-controlled trial evaluating the prevention of recurrence in 297 postsurgical resection CD patients who were at an increased risk. Patients were randomized to the placebo or IFX at eight weekly intervals for 200 weeks. The primary outcome was clinical recurrence (CDAI > 200 or increase by 70) or the development of a new or redraining fistula or abscess. The IFX group had lower rates of clinical recurrence (12.9% versus 20%, p = 0.097) and endoscopic recurrence (30.6% versus 60%, p < 0.001) [22].
3.1.3. Pediatric CD
Baldassano et al. evaluated the efficacy and safety of a single dose of IFX infusion in 21 children. The intervention resulted in a 100% clinical response, and remission was achieved in 48% of the cases [23]. Cezard et al. evaluated the role of IFX (5 mg/kg) in 21 children at 0, 15, and 45 days. The patients had remission in 19 cases, and treatment was also associated with 100% fistula closure [24]. The REACH study assessed the role of IFX in the maintenance of remission. A total of 112 children underwent induction at 0, 2, and 6 weeks and then received eight weekly IFX infusions at 5 mg/kg. A clinical response was seen in 88% of the patients, with 59% achieving remission [25].
3.1.4. Infliximab in Ulcerative Colitis
The role of IFX in UC has been evaluated in great detail. Landmark RCTs like ACT 1 and ACT 2 have assessed the efficacy of IFX in the induction and maintenance of remission in patients with moderate to severe UC. In ACT I, a randomized, double-blind trial, 364 patients were randomized into three groups based on the dosing of IFX at 5 mg/kg (group I), 10 mg/kg (group II), and placebo (group III). All groups received induction dosing at 0, 2, and 6 weeks followed by every 8 weeks for 46 weeks (8 doses, including induction). The primary outcome was a clinical response defined as a decrease in the Mayo score of at least three points and at least 30%, with an accompanying decrease in the sub-score for rectal bleeding of at least one point or an absolute rectal-bleeding sub-score of 0 or 1. The secondary outcome was clinical remission. At the end of 54 weeks, more patients who received 5 mg or 10 mg of IFX had a clinical response at week 54 (45 and 44%, respectively) than those who received the placebo (20%, p < 0.001 for both comparisons). Clinical remission was seen in 22% of patients who had received IFX. ACT II also enrolled 364 patients, and the randomized, double-blind trial categorized the patients into three groups similar to ACT I. The dosing pattern was also the same, but the study duration was 22 weeks. Similar to ACT I, the primary outcome in ACT II was a clinical response defined as a decrease in the Mayo score of at least three points and at least 30%, with an accompanying decrease in the sub-score for rectal bleeding of at least one point or an absolute rectal-bleeding sub-score of 0 or 1. Clinical remission was seen in 23% of patients who had received IFX as compared to 3% of the placebo group [26]. In both studies, patients who received IFX were more likely to have a clinical response at week 30 (p ≤ 0.002 for all comparisons).
In a small double-blind RCT, 45 patients with fulminant or severe UC were randomized to receive either IFX (as a rescue therapy) or the placebo, with the primary outcome being colectomy or death within 3 months of randomization. Although there was no mortality in either group, the rates of colectomy were significantly higher in the placebo group (66.7% vs. 29.2%, OR 4.9, 95% CI 1.4–17, p = 0.017) [27].
In another open-label randomized controlled trial, patients with an acute severe flare of UC (Lichtiger score > 10 points) and steroid failure were randomized to cyclosporine (2 mg/kg per day for 1 week, followed by oral drug until day 98) or IFX (5 mg/kg on days 0, 14, and 42). The primary outcomes included the absence of clinical response at day 7, a relapse between day 7 and day 98, the absence of steroid-free remission, colectomy, or death. Treatment failure occurred more frequently in the cyclosporine group (60% vs. 54%, p = 0.52). However, the incidence of serious adverse events was more common in the IFX group (25% vs. 16%) [28]. These study subjects were also followed for 5 years, and long-term outcomes showed higher colectomy-free survival (65.5% vs. 61.5%) in the IFX group (p = 0.97) [29].
A retrospective study of the database of the British Columbia Ministry of Health assessed 7227 patients. Patients in the pre-IFX era (2003–2004) were compared with the IFX era (2008–2009). A lower colectomy rate was noted in the IFX era (8.88% vs. 9.97%, p = 0.03). However, the study also noted that amongst the patients with severe UC (having a history of steroid use), there was no significant difference (9.9 vs. 11.14%, p = 0.18) [30].
Another retrospective study of 191 patients with UC on IFX had an 18.8% rate of colectomy over a follow-up of 18 months. The study assesses the independent predictors of colectomy. Predictors of colectomy included the absence of clinical response after IFX induction (HR 7, 95% CI 3.4–14.8), elevated baseline C-reactive protein > 10 mg/L (HR 5.1, 95% CI 1.8–14.8), and previous treatment with cyclosporine (HR 2.5; 95% CI 1.2–5.3) [31].
An observation study of 285 IFX-treated patients showed a relapse rate of 61% of patients and a colectomy rate of 20% during a median follow-up period of 5 years. Multiple independent predictors of colectomy-free survival included a rapid clinical response (OR 7.7, 95% CI 2.8–21.7; p < 0.001), mucosal healing (OR 4, 95% CI 1.2–14, p = 0.028), baseline CRP ≤ 5 mg/L (OR 2.9, 95% CI 1.3–6.9, p = 0.012), and baseline albumin ≥ 35 g/L (OR 3, 95% CI 1.1–8.2, p = 0.029). The study also showed that IFX concentrations (at week 14) > 2.5 μg/mL predicted relapse-free survival (p < 0.001) and colectomy-free survival (p = 0.034) [30].
3.1.5. Infliximab in Pouchitis
Almost 20–30% of the patients with UC undergo surgery in their lifetime with the majority having total procto-colectomy and IPAA [32]. The pouch can develop an inflammatory condition both in UC and CD. IFX has been evaluated in the management of pouchitis. A Belgian study of 28 patients with IPAA along with refractory pouchitis evaluated IFX in the management. A total of 56% of patients showed a sustained clinical response after a median follow-up period of 20 months [33].
In a retrospective, multi-center observational study evaluating IFX, patients (n = 35) with chronic, refractory pouchitis were treated with IFX and assessed at weeks 8, 26, and 52. Partial responses (63%, 33%, and 19%) and complete responses (21%, 33%, and 27%) were achieved at weeks 8, 26, and 52, respectively [22].
Similarly, a study from Canada of 42 patients with chronic refractory pouchitis (n = 26) or recurrence of CD after IPAA showed a complete clinical response in 29.6% of cases. It also showed that 62.6% of the participants had a partial response, underlining the role of IFX in the management of pouch-related inflammatory complications [31].
A recent meta-analysis of 313 patients on anti-TNF therapy showed short-term and long-term remission rates of 50% and 52%, respectively. The study also showed a better response for CD-like complications of the pouch than refractory pouchitis [34]. Landmark trials of use of infliximab in UC and CD are enumerated in Table 1.

Table 1.
Landmark trials of infliximab in UC and CD.
3.2. Adalimumab
For a long period after infliximab was approved as a therapeutic option in the management of IBD, IFX was the only choice available. A significant number of patients went on to lose the response, primarily due to the development of anti-IFX antibodies [24]. Additionally, a higher rate of drug-mediated reactions was also noted in the patients with these antibodies [35]. Many therapeutic interventions, like more frequent or higher dosing, were tried but this also prompted research into alternative treatment options. Adalimumab (ADA), like IFX, is a recombinant human monoclonal antibody targeting TNFα. Although the mechanism of action is the same, there are significant differences in terms of the dosing schedule and routes of administration. Moreover, it has been shown to be useful as a primary biologic and in patients who have a loss of response to IFX due to antibodies.
3.2.1. Adalimumab in CD
The earliest trial to evaluate the role of ADA in the management of CD was the CLASSIC I trial, which was a randomized, double-blind, placebo-controlled, dose-ranging trial aiming to evaluate the efficacy of adalimumab induction therapy in patients with CD. Patients with moderate to severe CD (n = 299) who were anti-TNF-naïve were randomized to receive two doses of different doses of ADA (40 mg/20 mg, 80 mg/40 mg, or 160 mg/80 mg or placebo) at 0 and 2 weeks. The primary endpoint was clinical remission at 4 weeks, which was defined as a CDAI < 150. The most significant rates of clinical remission were seen in the 160/80 mg group (36%, p = 0.001) as compared to 18% (40/20 mg), 24% (80/40 mg), and 12% (placebo). Adverse events occurred at similar rates in all 4 treatment groups, except for injection site reactions, which were more common in patients treated with adalimumab [36].
CLASSIC II followed up on patients from CLASSIC I. Out of the original 299 patients, 276 patients were enrolled in CLASSIC II and received 40 mg of ADA at weeks 0 (week 4 of CLASSIC I) and 2. Patients in remission at both weeks 0 and 4 (n = 55) were again randomized into three groups: 40 mg alternate weekly, 40 mg weekly, or placebo for 56 weeks. Patients who had not achieved remission at weeks 0 and 4 were enrolled and received open-label ADA (40 mg) every other week, which was escalated to weekly dosing in the case of a non-response or flare. Patients with a non-response or flare could upgrade to an alternate weekly or weekly schedule. The maintenance of remission (CDAI < 150) was the primary endpoint. Of the 55 patients randomized at week 4, a higher number of patients in the weekly and alternate weekly arms were in remission as compared to the placebo (83% vs. 79% vs. 44%, p < 0.05). Of the 204 patients in the open-label arm, 46% were in clinical remission at week 56 [37].
3.2.2. Adalimumab in UC
Based on the evidence that ADA was successful in the induction as well as maintenance of remission in CD, it has also been assessed as an anti-TNF agent in UC. The ULTRA 1 trial was conducted to assess the efficacy of adalimumab in inducing remission in patients with moderate-to-severe UC. ULTRA 1 was a multicenter randomized, double-blind, placebo-controlled study that assessed the role of ADA in patients with a Mayo score of ≥6 points and endoscopic sub-score of ≥2 points despite treatment with corticosteroids and/or immunosuppressants who were randomized to subcutaneous treatment with ADA (160 mg at week 0, 80 mg at week 2, or 40 mg at weeks 4 and 6) or placebo. Subsequently, a second induction group (ADA 80 mg at week 0 followed by 40 mg at weeks 2, 4, and 6) was established. The primary efficacy endpoint was clinical remission (Mayo score ≤ 2 with no individual sub-score > 1) at week 8. The study showed higher remission rates in the 160/80 group (18.5%) and ADA 80/40 group (10.0%) as compared to the placebo (9.2%). Serious adverse events occurred in 7.6%, 3.8%, and 4.0% of patients in the placebo, 80/40, and 160/80 groups, respectively [38].
ULTRA 2, a randomized, double-blind, placebo-controlled trial, assessed the role of ADA in the long-term maintenance of remission in UC in 494 patients with moderate-to-severe ulcerative colitis who also received treatment with oral corticosteroids or immunosuppressants. Patients were stratified in two groups based on previous anti-TNF exposure and then each stratum was randomized to receive ADA 160 mg at week 0, 80 mg at week 2, and then 40 mg every other week, or the placebo. The primary endpoints were remission at week 8 (like ULTRA 1) and week 52. Clinical remission rates were higher in the ADA group at week 8 (16.5% vs. 9.3%, p = 0.019) and at week 52 (17.3% vs. 8.5%, p = 0.004). It was also interesting to note that amongst anti-TNF-naïve patients, the rates were even higher for the ADA group at week 8 (21.3% vs. 11.0%, p = 0.017) and week 52 (22% vs. 12.4%, p = 0.029). Amongst the patients with exposure to anti-TNF therapy, the results still favored ADA at week 8 (9.2% vs. 6.9%, p = 0.559) and significantly more at week 52 (10.2% vs. 3%, p = 0.039) [39].
Balint et al. assessed the rates of continuous clinical response, remission, non-response, and loss of response at weeks 12, 30, and 52 with ADA in 73 patients with UC. As 67.1% of the patients had received previous IFX therapy, the secondary endpoints compared a difference in response between anti-TNF-naïve and -exposed patients. Of the patients, 75.3% showed a clinical response at week 12 and remission was maintained in 48.6% at week 52 [40].
The patients enrolled in ULTRA 1 and ULTRA 2 were followed up (ULTRA 3) as an open-label extension for four years. Of the patients who were followed up in ULTRA 3 (n = 588), 61.2% of patients remained on ADA at 3 years. Remission according to the partial Mayo score and mucosal healing was maintained by 63.6% and 59.9% of patients [41].
3.3. Golimumab
3.3.1. Golimumab in UC
Golimumab is a subcutaneously delivered human monoclonal antibody targeted against TNFα. The PURSUIT-SC trial evaluated the golimumab response in patients with moderate-to-severe UC who were naïve to anti-TNF agents, but had failed to respond to one or more of the other conventional medical therapies. It was conducted as a randomized double-blind dose-finding and dose-confirmation study involving 774 patients. The trial showed that 51% of patients receiving golimumab (200 mg followed by 100 mg 2 weeks apart) and 54.9% receiving a higher dose of golimumab (400 mg followed by 200 mg 2 weeks apart) achieved the primary endpoint of clinical response at week 6. The placebo group achieved the endpoint in 30.3% of cases (p ≤ 0.0001). Clinical remission at 6 weeks was also higher in the golimumab group: 17.8% (200 mg/100 mg) and 17.9% (400 mg/200 mg) versus 6.4% in the placebo group (p < 0.0001) [42].
The PURSUIT-maintenance trial followed PURSUIT-SC to assess long-term clinical efficacy and safety. The randomized, double-blind study enrolled 464 patients who had responded to induction therapy in PURSUIT-SC into three groups: group I (Placebo), group II (4 weekly 50 mg golimumab), and group III (4 weekly 100 mg) for 54 weeks. Golimumab maintained remission in 47% (p = 0.010) in group III and 49.7% (p < 0.001) in group II as compared to 31.2% in group I [42].
Similarly, Pursuit-J enrolled 144 patients with UC given open-label induction with golimumab. The responders entered the double-blind phase and were randomized to 100 mg of golimumab or placebo every 4 weeks for 52 weeks. The clinical response at 54 weeks was the primary response, with secondary endpoints being clinical remission and mucosal healing at weeks 30 and 54. Patients in the golimumab arm had a higher rate of maintained clinical response until week 54 (56.3% vs. 19.4%). Additionally, during the 54 weeks, a significantly higher number of patients in the golimumab arm had remission (50% vs. 6.5%), and a higher proportion of patients on golimumab (59.4%) experienced mucosal healing than in the placebo group (16.1%) [43].
GO-COLITIS was an open-label, study with a pragmatic design reflecting clinical practice. Adult UC patients (n = 205) with a disease duration > 3 months and partial Mayo score (4–9) received golimumab induction (200 mg initially and 100 mg at week 2) followed at week 6 by weight-based golimumab every 4 weeks until week 54 with a 12-week follow-up. A sustained clinical response until week 54 was achieved in 24.9% of the patients. An improvement in HRQoL was sustained through week 54. Serious AEs leading to treatment discontinuation occurred in 8.8% of patients [44].
3.3.2. Golimumab in CD
A study by Greener et al. evaluated the role of golimumab in CD in a retrospective observational study involving 45 patients with CD with a median follow-up of 22 months. A clinical response at 12 weeks was seen in 77.7% of patients. Additionally, the cumulative probabilities that patients would maintain the same response after the initial response for 12 and 36 months after the introduction of golimumab were 81% and 64%, respectively. Over a year of follow-up, endoscopic improvement and mucosal healing were achieved in 73% and 47% of patients, respectively [45].
Another trial by Pichler et al. for adolescents with CD retrospectively analyzed the role of golimumab in seven adolescents who received golimumab (median age—17 years) for a median of 7.2 months. With golimumab, 71.4% of the participants were responders and 28.6% entered remission. There were no serious side effects reported [46].
3.4. Anti-TNF in Pregnancy
As an immunoglobulin, IgG is actively transported across the placenta from the second trimester onwards using the neonatal Fc receptor of the placenta [47]. Anti-TNF levels have been measured in cord blood as a surrogate marker for exposure and cord levels of anti-TNF often exceed maternal levels at birth. Anti-TNF clearance can take 6 months or more, with slower clearance for infliximab than adalimumab [48]. Anti-TNF therapy has no negative impact on pregnancy or newborn outcomes. Narula et al., in their meta-analysis of about 1300 anti-TNF exposed pregnancies, showed no increased risk of unfavorable pregnancy outcomes, miscarriage, preterm birth, low birth weight or congenital malformations [49]. It is important to note that most of the existing data regarding anti-TNF safety in pregnant women is based on studies analyzing infliximab and adalimumab. The data for golimumab are sparse. Based on the evidence, the American Gastroenterology Association (AGA) recommends the continuation of anti-TNFs throughout pregnancy, without interruption in the third trimester. It does recommend that the last dose should be timed to achieve the lowest possible trough levels at the time of delivery. AGA recommends that the final dose of infliximab, adalimumab, and golimumab should be given 6–10 weeks, 2–3 weeks, and 4–6 weeks before the expected date of delivery, respectively [50].
Landmark trials of use of Adalimumab and Golimumab in UC and CD are enumerated in Table 2.
Table 2.
Landmark trials of adalimumab and golimumab in UC and CD.
3.5. Effect on Extraintestinal Manifestations (EIMs)
A total of 50% of the patients of IBD will experience extraintestinal manifestations (EIM) over their lifetimes, and some manifestations may be severely disabling and may need therapies beyond conventional agents. Anti-TNF agents have been extensively evaluated for the management of EIM in IBD. Broadly speaking, the two commonest types of EIM are arthropathy (axial and peripheral) and skin manifestations [54]. The largest data for the management of EIM in IBD comes from a retrospective analysis of the Swiss IBD cohort [55]. The authors noted that in more than 40% of the cases, EIMs were the reason for the initiation of the treatment with anti-TNFs. Response rates to anti-TNF were good, with an improvement reported in more than 70% of the cases, and the best responses were seen for psoriasis, aphthous stomatitis, uveitis, and peripheral arthritis. Between axial and peripheral arthropathy, anti-TNF therapy is more likely to benefit axial arthropathy due to a lack of treatment options for these patients as compared to patients with peripheral arthropathy. It is also important to note that paradoxical articular manifestations have also been described in IBD patients who have received anti-TNF agents but do not warrant the need for the discontinuation of the medication [56]. All the dermatologic and ophthalmologic manifestations respond favorably to anti-TNF therapies and are generally utilized in severe cases like pyoderma gangrenosum [57] or uveitis [58]. Hepatic EIMs include primary sclerosing cholangitis, which can precede or follow IBD. Anti-TNF therapy has a minimal role in the management of PSC.
3.6. Adverse Effects of Anti-TNF Drugs
Subcutaneous anti-TNF agents may commonly cause injection site reactions (occurring in up to 40% of patients) and are considered minor [59]. These reactions, including significant pain, typically occur within the first few months of therapy and can last 2 to 5 days but rarely warrant stopping therapy. Multiple serious adverse events (SAEs) have been reported across almost all studies and include drug-related lupus-like reactions, serious infections (like tuberculosis), and malignancies (like non-Hodgkin lymphoma). The rate of SAEs has been diverse across the studies and is shown in Table 1 and Table 2.
4. Anti-Interleukin-12/23 p 40 Biologics
4.1. Introduction
There has been a paradigm shift in the therapeutic approach to managing inflammatory bowel disease (IBD). The pendulum has shifted from achieving a clinical response, i.e., symptom control, to achieving histological remission characterized by mucosal healing. The introduction of tumor necrosis factor-alpha (TNF-α) inhibitors marked a key turning point wherein specific molecules involved in disease pathogenesis were targeted. Over the years, we have realized that around 10–20% of patients may show no response to these molecules (primary non-responders), and around 23–46% may lose the therapeutic response by 01 year (secondary non-responders). In addition, research has highlighted the incremental roles of a dysregulated immune response, mucosal barrier dysfunction, genetic predisposition, and the environment, as well as the importance of the fecal microbiota in disease pathogenesis [60].
Interleukin 12 (IL12) and interleukin 23 (IL23) have critical roles in propagating inflammation in IBD. Our current understanding of the pathogenesis of IBD highlights the fact that antigen-presenting cells activate cluster of differentiation (CD4+) T cells into effector T cells, namely, T helper 1 (Th1), T helper 2 (Th2), T helper 17 (Th17), and T helper 9 (Th9) cells. Traditionally it was believed that the dysregulatatory response of Th 1 and Th 2 cells initiates the inflammatory process wherein Th1 cells favor the development of Crohn’s disease (CD) and Th1 cells favor ulcerative colitis (UC [61]). Over the years, research has evolved to implicate Th 17 cells as well. Their associated cytokines play a crucial role in mediating the inflammatory process both in UC as well as CD [62]. Herein, it is imperative to emphasize the role of two distinct interleukins that have fueled research and led to the development of newer therapeutic molecules. IL 12 induces a Th1 response while IL 23 upregulates Th 17 cells [63,64,65]. IL 12 consists of two subunits, p 40 and p 35, whereas p 40 and p 19 are the two subunits of IL 23 [66,67]. Thus, the common subunit, i.e., p 40, plays a major role as an inflammatory mediator in IBD. The neutralizing antibodies target the p 40 subunit and have therefore been rechristened as IL12/IL 23 antibodies [68].
4.2. Ustekinumab
It is a fully humanized IgG1 monoclonal antibody. Ustekinumab effectively prevents the binding of human IL12 and IL23 to their receptors, namely IL12 Rβ1/β2 and IL-23 R β1/β2, which, in turn, are located on the surface of T cells and NK cells. The molecule, however, cannot bind to IL 12/IL 23, which are already bound to their receptors. Ustekinumab, thus, inhibits IL12-mediated STAT 4 phosphorylation and IFγ cytokine production, as well as IL23-mediated STAT 3 phosphorylation and IL 17 A, IL 17 F, and IL 22 cytokine production [60]. The drug, which was originally approved for the treatment of plaque psoriasis, was finally approved for the treatment of moderate-to-severe active CD in Sep. 2016. Data from ‘population pharmacokinetics and exposure–response analysis’ reveals that the drug has an elimination half-life of 19 days. For a 70 Kg individual, it has a clearance of 0.192 L/day, and its volume of distribution is 4.62 L. The disposition of the drug, available in intravenous (iv) and subcutaneous (sc) preparations, remains unaltered despite concomitant corticosteroid, TNFα, or immunosuppressive drug usage [69].
4.2.1. Ustekinumab in CD
Proof of efficacy induction trials, namely, UNITI-I and UNITI-2 trials, included moderate-to-severe CD patients. In total, 741 patients included in UNITI-1 were either primary or secondary non-responders to TNFα antagonists or suffered intolerable side effects from these agents. Patients were randomized to the three treatment arms as follows: induction with Inj. ustekinumab 130 mg, induction with Inj. ustekinumab 06 mg/Kg, and induction with placebo. The clinical response rate at week 06 (defined as a CDAI < 150 or a decrease in the CDAI score > 100 from baseline following induction) was 34.3%, 33.7%, and 21.5% in all the above-mentioned three arms, respectively. A total of 628 patients enrolled in the UNITI-2 trial had failed conventional therapy or had intolerable side effects from these treatments. The clinical response rate was 51.7%, 55.5%, and 28.7% for those receiving 130 mg ustekinumab, 06 mg/Kg ustekinumab, and placebo at week 06, respectively. A total of 397 patients who completed the induction trials were inducted into the maintenance trial, IM-UNITI trial, with the primary endpoint being CDAI < 150 at week 44. These patients were further randomized to receive Inj. ustekinumab 90 mg sc into either 08 weekly or 12 weekly cohorts or the placebo. In total, 53.1% of patients receiving 08 weekly doses and 48.8% receiving 12 weekly doses were in clinical remission at week 44 compared to 35.9% receiving the placebo [70].
4.2.2. Ustekinumab in UC
The efficacy of ustekinumab in patients with moderate-to-severe UC was demonstrated in 2019. These patients were assessed after 8 weeks of induction therapy and thereafter at 44 weeks on maintenance therapy. This placebo-controlled double-blind RCT enrolled 961 patients who were randomized to receive Inj. ustekinumab (300 mg iv), a weight-based regimen (06 mg/kg), or the placebo. After the initial induction phase of 08 weeks, responders were again randomized to three different arms: those receiving 90 mg sc in 08 weekly doses, 12 weekly doses, and the placebo. Clinical remission was defined by a reduction in the Mayo score < 2 and no score > 01 on any of the Mayo subscale components [70].
4.2.3. Long-Term Efficacy of Ustekinumab in UC and CD
Those patients who had demonstrated a clinical response/remission in induction and maintenance trials were eligible to participate in trials providing long-term efficacy at 03 years and 05 years. Amongst all ustekinumab-treated patients who entered the long-term extension, the clinical response rate was 56.3% for those receiving 12 weekly doses and 55.1% for those receiving 08 weekly doses. Interestingly, only 4.6% of all randomized patients developed anti-drug antibodies [71]. The results of long-term efficacy in patients with UC showed clinical remission in 56.3% of patients receiving 08 weekly ustekinumab doses vs. 54.1% in those receiving 12 weekly doses [72]. The 05-year cumulative data on CD patients receiving ustekinumab showed a clinical response rate of 34.4% amongst those who received Inj. ustekinumab 90 mg sc and 28.8% amongst those who required a dose adjustment at week 256.
4.2.4. Safety Profile of Ustekinumab
Ustekinumab has generally been shown to have a favorable and comparable safety profile to the placebo in patients with UC and CD. An analysis of data from phase II/III studies analyzing 2754 patients who received Inj. ustekinumab has reported 118.32 adverse events (AEs) per 100 patient-years vs. 165.99 for the placebo. Serious AEs, infections, serious infections, and malignancies, except for non-melanoma skin malignancies, were reported in 21.23, 64.32, 5.02, and 0.40 per 100 patient-years, respectively [73]. The majority of AEs relate to the gastrointestinal system, with abdominal pain being the most frequently reported AE [74].
4.2.5. Ustekinumab and Pregnancy
Available data suggest favorable pregnancy outcomes in pregnant females with IBD treated with Inj. ustekinumab. A comparison of pregnant females suffering from IBD treated with ustekinumab, TNFα agents, non-ustekinumab, and non-TNFα agents reveals favorable pregnancy, neonatal, and newborn profiles across all therapeutic agents [75]. A prospective study analyzing the safety profiles of ustekinumab and vedolizumab in pregnant females has demonstrated favorable pregnancy and newborn outcomes. Moreover, when compared to anti-TNF preparations, these drugs have an inverse infant-to-maternal ratio of drug levels [76]. Results from ‘Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes (PIANO)’, which included 18 pregnant patients treated with ustekinumab, have reported no increased incidence of unfavorable outcomes among newborns until 01 year of age [48]. An ongoing Spanish prospective study has included 17 patients on ustekinumab with no reported increased risk of serious AEs until now [77].
4.2.6. Ustekinumab in the Pediatric Age Group
Data on the use of Ustekinumab in pediatric IBD is sparse. The results of a phase I induction dosing, double-blind RCT in children (02 to <18 yrs., body weight > 10 kg) with moderate-to-severe Crohn’s have shown that the safety profile and AEs were similar to those in adults; however, serum concentrations of Ustekinumab were lower in children <40 kg vs. those >40 kg [77]. A retrospective chart review of Ustekinumab use in 10 pediatric CD patients who were non-responders to other approved treatments required more frequent doses (04–06 weekly) to maintain clinical remission [78].
4.2.7. Ustekinumab in Postoperative IBD
Postoperative CD recurrence is seldom studied and is a difficult-to-treat disease entity. In a retrospective multicenter study, the efficacy of Ustekinumab vs. azathioprine was studied in 63 CD patients who had had postoperative disease recurrence using a propensity score analysis. Those who were treated with Ustekinumab had a 28% recurrence rate vs. 54.5% amongst those treated with azathioprine [79]. More promising data have recently been published highlighting the efficacy in a cohort of patients who had recurrence after surgery and had already been treated with TNF-α agents or vedolizumab. A total of 80% achieved clinical remission and 73.3% achieved mucosal healing [80].
4.2.8. Ustekinumab in Stricturing CD
Three large clinical trials have studied clinical and endoscopic outcomes in structuring CD patients. Treatment arms comprised infliximab, ustekinumab, and azathioprine. A post hoc analysis of 150 such patients was performed. A total of 62.5% of patients showed resolution. In addition, there was an improvement in strictures that were passable at the end of 01 year of treatment [49]. Another recent abstract has highlighted data from 15 CD patients with strictures. While on Ustekinumab therapy, 18% required a dose escalation while 40% required an additional course of steroids [81].
4.2.9. Ustekinumab in Perianal Disease
Data from UNITI induction trials has shown a 26% overall fistula response rate vs. 16.9% in the placebo group after 08 weeks of Ustekinumab therapy. A total of 24.7% achieved fistula resolution vs. 14.1% in the placebo arm during the same period of treatment [82]. The perianal CD has been specifically analyzed in the Fresh cohort study. Among 148 patients with active perianal disease at baseline, the primary endpoint of >50% resolution of draining fistulas was achieved in 38.5% of patients after Ustekinumab treatment [83]. A systemic review and meta-analysis have shown a cumulate response rate of 41% and a 17.1% remission rate after 08 weeks of Ustekinumab treatment amongst patients with perianal CD. After 54 weeks of treatment, the remission rate remained static at 16.7%, while response rates increased to 55.9% [84].
4.2.10. Ustekinumab in Extraintestinal Manifestations (EIMs)
In the post hoc analysis of UNITI trials, the ustekinumab treatment group had no improvement in EIMs vs. the placebo-controlled group at 06 weeks and 52 weeks of treatment (36.9% vs. 39.9% at week 06 and 76.4% vs. 80% at 52 weeks, respectively) [49]. Data from a systemic review and meta-analysis show a beneficial response to ustekinumab treatment vis a vis dermatological manifestations but no definite response in axial spondyloarthritis [85]. The results of these trials providing valuable evidence on the efficacy of ustekinumab in the induction and maintenance of remission as well as long term efficacy in moderate-to-severe CD and UC have been summarized in Table 3 and Table 4.
Table 3.
Trials demonstrating the efficacy of Ustekinumab in the induction and maintenance of remission of ulcerative colitis and Crohn’s disease.
Table 4.
Trials demonstrating the long-term efficacy of ustekinumab in the maintenance of remission of ulcerative colitis and Crohn’s disease.
5. Anti-Integrins
5.1. Leukocyte Trafficking and Role of ‘Integrins’ in Propagating Inflammation in IBD
The interaction of circulating lymphocytes with endothelial cells of the gut allows the leukocytes to bind with selectins (Sialyl LewisX-modified glycoprotein) on the endothelial cells at low affinity. Thus, these leukocytes infiltrate the intestinal mucosa. Integrins are heterodimeric receptors that allow tissue-specific adhesion. These integrins, further consisting of α and β subunits, bind to cellular adhesion molecules (CAMs) present in the intestinal endothelial cells. This initiates the dysregulated inflammatory process in IBD. Research has highlighted the critical roles of three CAMs, namely, intracellular adhesion molecule (ICAM-1), vascular adhesion molecule (VCAM-1), and mucosal adhesion cellular adhesion molecule (MAdCAM-1). Inflammation propagates the release of cytokines, which in turn increases ICAM-1 expression. ICAM-1 binds to αLβ2 receptors on leukocytes. VCAM-1 binds to α4β7 receptors in the intestine, and MAd CAM-1 binds to α4β7 memory T cells. Thus, the blockade of the integrin–CAM interaction is a promising strategy in the management of IBD [88,89,90].
5.2. Vedolizumab in UC and CD
Vedolizumab is a 147 KDa recombinant humanized monoclonal antibody that binds to the α4β7 heterodimer expressed on the surface of intestine-specific lymphocytes. Domains from the mouse anti-human α4β7 antibody were fused with a conventional human IgG1 scaffold to generate this molecule. Further mutations introduced to the Fc region effectively reduced Fc-related cytotoxicity [91]. The gut specificity of vedolizumab has been established in clinical trials and, in contrast to natalizumab, another integrin inhibitor, it does not affect T cell trafficking into the central nervous system [92]. Alternative mechanisms of action include the blockage of monocyte and dendritic cell recruitment and changes in the innate immune system [93]. Vedolizumab has an average linear elimination half-life of 25.5 days. The linear clearance values have been estimated to be 0.159 L/day and 0.155 L/day for UC and CD, respectively [94,95].
The initial proof of concept phase I trial included 29 patients with moderate-to-severe UC. The anti α4β7 antibody then labelled as ‘LDP-2′ provided evidence of deep remission in those who received the antibody vs. no remission in the placebo arm [96]. In phase II double-blind, placebo-controlled study, an anti-α4β7 antibody (labelled as MLN02) was administered intravenously. This study had three different cohorts: MLN02 0.5 mg/kg, 2.0 mg/kg, and placebo. The trial demonstrated higher clinical and endoscopic remission rates in both the treatment arms vs. the placebo [97]. GEMINI trials were the pivotal trials documenting the efficacy of vedolizumab in IBD. The first GEMINI-1 trial demonstrated the efficacy of vedolizumab for induction as well as maintenance therapy vs. the placebo in patients with active UC [98]. The GEMINI-2 trial studied the efficacy of intravenous vedolizumab in adult patients with active CD while the GEMINI 3 trial addressed the usefulness in moderately severe-to-severe CD patients [99] who had either not responded to, had developed an intolerance to, or had a loss of response to anti-TNF α agents.
A systemic review and meta-analysis analyzing the efficacy of vedolizumab in active UC has shown improved rates of clinical remission with a relative risk (RR) of 0.86, 95% CI 0.80–0.91), clinical response (RR: 0.82, 95% CI 0.75–0.91), and endoscopic remission (RR 0.82, 95% CI 0.75–0.91). The therapy has proven to be superior to the placebo for the maintenance of remission of UC (clinical remission, RR: 2.73, 95% CI 1.78–4.18) and endoscopic remission (RR: 2.71, 95% CI 1.88–3.93) [100,101].
The only head-to-head RCT studying the utility of vedolizumab vs. adalimumab randomized 771 patients to the two treatment arms. In total, 80% of patients were treatment-naïve, while 20% had failed to respond to the TNF-α antagonist, except for adalimumab. The primary endpoint of clinical remission, i.e., cessation of bleeding and endoscopic improvement, and an improvement in the Mayo score, was met at 52 weeks with a statistically significant 8.8% better improvement favoring the patient cohort on vedolizumab. Although symptom-based endpoints and the rapidity of response favored vedolizumab, the point estimate of corticosteroid-free remission favored adalimumab [102].
The latest phase IV placebo-controlled RCT has evaluated the effectiveness of vedolizumab in 102 patients with chronic pouchitis after having undergone ileal pouch-anal anastomosis (IPAA) for UC. The primary endpoint of a reduction in the modified Pouchitis Disease Activity Index (mPDAI) of <4 or >2 reductions from baseline favored vedolizumab (31% vs. 10% in the placebo group). This significant percentage point difference was also seen at week 34 (17 percentage points; 95% CI, 0 to 35) [103].
5.3. Safety Profile of Vedolizumab
The GEMINI long-term safety (LTS) study enrolled 894 patients with UC and 1349 patients with CD. Over 08 years, patients with UC had received vedolizumab for an average of 42.4 months and those with CD for an average of 31.5 months. Although 93% of patients with UC and 96% of patients with CD reported adverse effects (AEs), vedolizumab discontinuation due to AEs occurred in 15% and 17% of patients with UC and CD, respectively. Two out of ten deaths over the study period were drug-related [104]. In one of the largest post-marketing surveys to date spanning 208050 patient-years of vedolizumab exposure, 80218 AEs were reported. A total of 8810 patients reported serious AEs: 10% with UC vs. 14% with CD. A total of 5876 patients developed infections, 19% had serious infections, while 5% developed opportunistic infections [105]. Overall, the most commonly reported AEs are fever, arthralgia, headache, and nasopharyngitis.
5.4. Vedolizumab and Pregnancy
The data on the use of vedolizumab in pregnant women have shown conflicting results. The initial study that extrapolated data from clinical trials and post-marketing studies found no adverse pregnancy outcomes in females either directly or indirectly exposed to vedolizumab [106]. Recent studies, including a prospective study, have reported no significant adverse pregnancy outcomes [107]. On the other hand, a recent systemic review and meta-analysis including four studies have reported overall adverse pregnancy-related outcomes (odds ratio [OR] 2.18, 95% confidence interval [CI], 1.52–3.13) in pregnant females receiving vedolizumab, with increases in both preterm births (OR 2.16, 95% CI, 1.28–3.66) and early loss of pregnancy (OR 1.79, 95% CI, 1.06–3.01) [108].
5.5. Vedolizumab in the Pediatric Age Group
Although the initial trials on vedolizumab had excluded pediatric patients with IBD, safety, and efficacy have been analyzed in a multicenter study involving pediatric patients (02–18 yrs.). Out of 64 children, all of whom were previously treated with TNF-α agents, with a median follow-up of 24 weeks, steroid-free remission was achieved in 37% of patients with UC and 14% of patients with CD [109]. Research has also characterized patients with very early onset IBD, defined as an IBD onset at <06 years of age. This study included 16 patients, 12 with UC and 04 with CD, with a median age at diagnosis of 33.5 months and 06.5 years at the initiation of vedolizumab. The primary endpoint of a reduction in Pediatric Crohn’s Disease Activity Index (PCDAI) by 12.5 points and Pediatric Ulcerative Colitis Activity Index (PUCAI) of 20 points in 4th week was achieved in 56.3% of patients [110]. A systemic review and meta-analysis including 455 patients and 10 studies reported clinical remission rates of 36% at 06 weeks, 48% at 14 weeks, 53% at 22 weeks, and 45% at 01 year for patients with UC. The same rates for patients with CD were 25% at 06 weeks, 28% at 14 weeks, 32% at 22 weeks, and 46% at 01 year. A total of 06% of patients reported serious AEs [111]. The available evidence supports the use of vedolizumab at a dose of 06 mg/Kg in patients <45 kg and 300 mg for patients >45 kg.
5.6. Vedolizumab in Fistulizing Crohn’s Disease
Management of Crohn’s fistula is one of the unmet needs of disease management. A multicenter cohort study of 102 patients (99% had received at least 01 anti-TNF agent) with active perianal disease has reported that 22.6% had no draining fistulas on vedolizumab therapy at 52 weeks [112]. The ‘Enterprise study’, a phase IV, double-blind RCT, has shown that >50% of vedolizumab-treated patients reported a reduction in the number of draining fistulas [113]. A recent systemic review and meta-analysis included 04 studies and 198 patients with peri-anal fistulas. A total of 87% of these patients had failed anti-TNF therapy. The authors have reported that the pooled complete healing rate was 27.6% (95% CI, 18.9–37.3%) and the pooled partial healing rate was 34.9% (95% CI, 23.2–47.7%) [114].
5.7. Vedolizumab in Extraintestinal Manifestations
Data on the efficacy of vedolizumab in EIMs is uncertain. Experience gained by a post-hoc analysis of RCTs has shown benefits, wherein the EIM is directly related to luminal disease activity, e.g., erythema nodosum but no effect on other associations like primary sclerosing cholangitis (PSC). A real-life study analyzing the efficacy of vedolizumab on extraintestinal manifestations of 134 patients (56 with UC and 77 with CD) has not reported any effect on the clinical evolution of EIMs. The majority of studies have multiple confounding factors, like previous treatment with anti-TNF agents [115] (Table 5).
Table 5.
Landmark trials demonstrating the efficacy of vedolizumab in induction and maintenance for IBD.
6. Small Molecules in IBD
6.1. Introduction
Recent advancements in our understanding of the pathophysiology and inflammatory mediators implicated in IBD have led to a shift towards using targeted biological agents. For patients with moderate-to-severe disease who are refractory, intolerant, or dependent on corticosteroids, anti-TNF agents such as infliximab, adalimumab, and golimumab are recommended [20,26]. However, nearly 30% of cases show primary non-response to anti-TNFs, and up to 60% may experience a secondary loss of response after a year of treatment [116,117]. As these agents are monoclonal antibodies administered parenterally against specific cytokines, the risk of developing antibodies against them is a major concern. Combining them with thiopurines reduces the formation of antidrug antibodies, but it may also raise the possibility of adverse effects [118,119]. Recently developed agents, including vedolizumab and ustekinumab, have been used to treat IBD patients who have been exposed to anti-TNFs. However, vedolizumab’s slow onset of action, high therapy cost, and non-response rates of up to 30% [120,121] and ustekinumab’s high cost, limited availability in tropical countries, and lack of long-term efficacy and safety data [122] are limitations to their use. Furthermore, in regions where tuberculosis is endemic, 8–11% of patients with inflammatory bowel disease (IBD) treated with anti-TNF agents may develop active tuberculosis, despite latent TB screening [123,124]. Types of small molecules with their target are listed in Table 6.
Table 6.
Classification of small molecules in IBD [7].
6.2. Targets of Small molecules and Mechanism of Action
6.2.1. JAK Inhibitors
Certain cytokines, including IL-9, IL-23, and interferon (INF)-γ, rely on the Janus kinases (abbreviated as “JAK”), which phosphorylate signal transducer and activator (STAT) transcription factors [125,126], since their receptors are unable to do so. The JAK enzyme family is composed of JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2). After phosphorylation, STAT proteins (comprising seven family members: STAT1–4, 5A, 5B, and 6) enter the nucleus and regulate gene transcription (refer to Figure 2). It is worth noting that Barrett and coworkers identified JAK2-related gene loci in association with an increased risk of developing CD, while Anderson et al. found similar results for UC [127,128]. It is important to be aware that JAK inhibitors can have significant side effects, such as infections and cardiovascular events. The most common infections include those of the upper airways, including influenza.
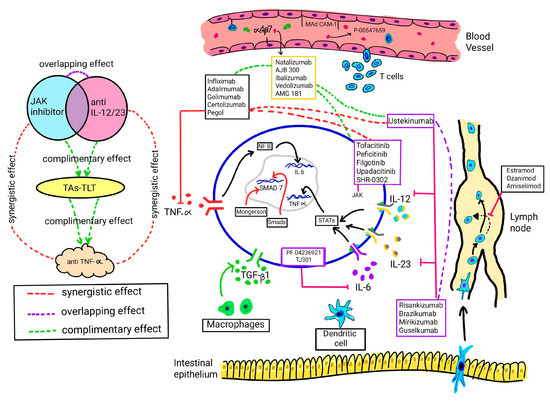
Figure 2.
Mechanisms of action of small molecules and biologicals. TAs-TLT, therapeutic agents targeting leukocyte trafficking, TNF, tumour necrosis factor, NF-B, nuclear factor, JAK, Janus kinase; IL, interleukin; MAdCAM, mucosal addressin cell associated molecule; TGF, transforming growth factor; SMAD7, mothers against decapentaplegic homolog 7, STATs, signal transducers and activators of transcription. Adapted from [129], Elsevier, 2023.
6.2.2. S1P Receptor Modulators
S1P is a type of bioactive lipid mediator that exerts its function by activating cell-surface G protein-coupled receptors known as S1P1–S1P5. Among these receptors, S1P1 is the most widespread and is present in both lymphocytes and endothelial cells. When S1P binds to S1P1, it is taken up inside the cell, and consequently, the cell surface agonist does not produce a signal. This results in a reduction in circulating lymphocytes and a decrease in the inflammatory response. This mechanism has led to its use and further exploration for the treatment of inflammatory bowel diseases (IBDs) [130].
6.2.3. PDE 4 Inhibitors
Phosphodiesterases (PDEs) are a type of enzyme that breaks down cyclic guanosine monophosphate (cGMP) and cyclic adenosine monophosphate (cAMP). PDE4 is especially interesting because it breaks down cAMP, which activates the nuclear factor kappa B (NF-κB). NF-κB is responsible for the increased production of proinflammatory cytokines [131].
6.2.4. TLR 9 Agonist
Toll-like receptors (TLRs) are important in the innate immune system. Modulating them is a promising approach to treating autoimmune disorders. Activation of TLR-9 induces anti-inflammatory cytokines such as IL-10 and type I interferons [132].
6.2.5. TYK 2 Inhibitors
TYK2 is a part of the JAK-STAT family and plays a crucial role in intracellular cytokine signaling. Additionally, TYK2 has been found to boost interferon production in macrophages [78]. Given its involvement in the immune response and inflammation, inhibiting TYK2 could be a promising approach for managing IBD [133].
Landmark trials of established small molecules and upcoming phase 3 trials for new oral drugs are discussed in Table 7.
Table 7.
Main published and ongoing trials for small molecule drugs (SMDs) in phase III trials/FDA approved for IBD.
6.3. Use in Special Situations
6.3.1. ASUC/Acute Flare of CD
Tofacitinib: It has a short half-life, and changes on endoscopy can be observed as early as 3 days after administration [146]. Hence, the drug has the potential for use in patients with acute severe colitis. In a retrospective case–control study, outcomes in patients with acute severe ulcerative colitis (ASUC) who received tofacitinib were compared with a control arm of patients who received either infliximab or cyclosporine. In a retrospective study of 40 patients, the proportion of patients who underwent colectomy by 6 months was significantly lower in the tofacitinib arm as compared to matched controls [147]. The dose-stratified analysis revealed only 10 mg thrice daily as protective (hazard ratio: 0.11; 95% CI, 0.02–0.56, p = 0.008). Similarly, induction therapy with tofacitinib at a high dose of 10 mg thrice daily has been used in patients with ASUC [148]. A multicenter study from France of 55 patients with refractory ulcerative colitis (49 prior infliximab-exposed patients and 19 prior cyclosporine-exposed patients) revealed colectomy-free rates of 78.9% and 73.6% at 3 and 6 months, respectively, with tofacitinib. However, the majority (65%) were also on concomitant steroids. In another series of eight patients, tofacitinib as rescue therapy in severe acute colitis had shown a clinical response in five of eight patients [149]. The median time to discharge after the start of tofacitinib was 5 days (5–6 days). Multiple short case series h been published on the use of tofacitinib in ASUC; long-term prospective RCTs are required to shed more light on the subject [147,150]. The higher dosages used in the setting of ASUC may heighten the risk of adverse effects; there is one report of mortality in a patient with underlying COVID-19 due to presumed pulmonary embolism, and cases of herpes zoster in the elderly [150,151]. Other reports indicate that the risks may be similar to conventional rescue therapies [147].
Upadacitinib: Gilmore et al., in their series, was the first to highlight the potential role of upadacitinib as rescue therapy for infliximab-experienced, steroid-refractory ASUC patients. All six patients demonstrated a clinical response to upadacitinib induction during their inpatient admission. Four patients achieved corticosteroid-free clinical remission by week 8, including the complete resolution of rectal bleeding and transmural healing assessed by IUS, and sustained clinical remission at week 16. One patient proceeded to colectomy at week 15 due to refractory disease. No adverse events directly attributable to upadacitinib were identified [152].
Ozanimod: The role in ASUC has been limited to a couple of case reports where it was used for maintenance after induction with cyclosporine [153].
6.3.2. Pregnancy
Tofacitinib: There is limited data regarding the transfer of the small molecule across the placenta; however, being a small molecule, transfer across the placenta is expected. The data from the rat model have shown that at very high doses (73 times), tofacitinib was teratogenic, resulting in various soft tissue and skeletal malformations [154]. However, at doses as high as 29 times the therapeutic dose of 10 mg BD, no such effects were noted. Tofacitinib does not have any impact on fertility or sperm quality in males. Human data are scarce for the use of tofacitinib in pregnancy. In an analysis of 1157 patients with UC, there were 14 patients with paternal and 11 patients with maternal exposure. There were two medical terminations and two spontaneous abortions. There were no fetal deaths or malformations, and the pregnancy and fetal outcomes were similar to the general population [155]. This is in line with similar results from 47 pregnancies with tofacitinib in the setting of rheumatoid arthritis and psoriasis. One case of fetal malformation in the form of pulmonary valve stenosis was noted in a patient who was also on losartan [156]. However, given the limited information, pregnancy is not recommended while on tofacitinib, and contraception is recommended. Additionally, drug discontinuation should be considered in individuals who become pregnant while on tofacitinib. In the rat model, tofacitinib was present at a double concentration in rat milk than in the serum of lactating rats. Given the scarcity and limitations of available human safety data, tofacitinib should be avoided during pregnancy and lactation.
Upadacitinib is contraindicated in pregnancy and while breastfeeding [157]. Although no human studies have assessed the safety of upadacitinib for pregnancy, this drug was also found to be teratogenic in animal studies.
Ozanimod: The clinical experience with ozanimod during pregnancy is limited, there has been no increased event of fetal abnormalities or adverse pregnancy outcomes seen with ozanimod exposure in early pregnancy [158].
6.3.3. Pediatric Population
Tofacitinib: The pediatric experience of tofacitinib in UC is limited to a couple of case series. The initial study of five patients with severe refractory UC demonstrated a clinical response and steroid-free remission in all patients. The dose used was 10 mg BD. Another series of five children used tofacitinib as a part of dual therapy with vedolizumab. Four out of five patients had steroid-free remission at 6 months. Only one patient developed VTE with the combination, and the dose was reduced from 10 mg BD to 5 mg BD. A phase III trial is underway for efficacy in induction as well as maintenance [159].
Upadacitinib in children is not yet FDA-approved for both UC and CD. Data are only limited to case reports [160].
Ozanimod: The safety and efficacy of ozanimod in children and adolescents aged below 18 years has not yet been established. A phase II study investigating its role in moderate and severe ulcerative colitis is underway [161].
6.3.4. EIM
Tofacitinib: In OCTAVE (1, 2, and Sustain) post hoc analyses, there were 27% of the patients with a history of prior EIMs, and 9% with a history of active EIMs. In OCTAVE induction trials of patients with active peripheral arthritis, there was an improvement in 15.6% of the patients with tofacitinib and 14.3% of the patients with the placebo. The majority (81.3% of patients on tofacitinib and 85.7% of patients on the placebo) had no change in symptoms. The study revealed that the history of EIMs did not influence the efficacy of tofacitinib [162]. Small case series have shown improvements in pyoderma gangrenosum, erythema nodosum, and ocular EIMs [162].
Upadacitinib: It has been shown to induce clinical benefit in extraintestinal manifestations in both CD and UC. In the phase II Celest study of moderate-to-severe CD, compared with the placebo at 16 weeks, a numerically greater proportion of patients achieved the resolution of any EIM, classic EIMs, and arthropathy with upadacitinib 12 and 24 mg BID, and upadacitinib 24 mg QD doses [163]. In a phase III study of UC EIMs, symptom resolution was improved versus the placebo following induction treatment with UPA 45 mg and after maintenance treatment with UPA 15 or 30 mg, with the 30 mg dose providing statistically significant improvements versus the placebo [164].
Ozanimod: The role of ozanimod in extraintestinal manifestations is not clear.
6.3.5. Post-Surgery
Tofacitinib: Postoperative results have primarily been limited to small retrospective series. In a study of 53 patients with refractory UC, there was an increased risk of venous thromboembolism in 13.2% of the cases [165]. On the contrary, a cohort of 35 patients who underwent colectomy within 28 days of tofacitinib had no postoperative complications after exposure to tofacitinib [166].
Data on postoperative results for IBD patients on upadacitinib and ozanimod are lacking.
6.4. Adverse Effects
6.4.1. Jak Inhibitors (Tofacitinib/Upadacitinib/Filgotinib)
Infections: JAK inhibitors carry a high risk of herpes zoster virus (HZ) infection. A post hoc analysis, pooling data from induction, maintenance, and open-label studies on UC patients treated with tofacitinib, showed that 5.6% of the patients developed HZ. The incidence rate (IR) over a mean of almost 2 years was 4.07. The risk factors were an age of 65 years or older (9.55), Asian race (6.49), prior anti-TNF failure, and a tofacitinib 10 mg bid dose (4.25). The multivariate analysis identified age and prior anti-TNF failure as the only independent risk factors [167].
The immune system’s primary response to the HZ virus is initiated through the type I and II IFN pathways, which are facilitated and transmitted at the transmembrane level by various JAK pathways, such as JAK1-TYK2 and JAK1-JAK2. When activated, these pathways signal the STAT protein system. A recent network meta-analysis has shown that even low doses of JAK inhibitors, such as tofacitinib, increase the risk of herpes zoster infection. The higher risk was specifically with tofacitinib 10 mg bid (RR = 6.90; 95% CI 1.56–30.63) and upadacitinib 45 mg o.d. (RR = 7.89; 95% CI 1.04–59.59) [168].
During the phase III clinical trials for filgotinib in UC, only one case of HZ was reported in the 200 mg group and another in the 100 mg group. When analyzing the pooled data of patients with RA, it was found that the 200 mg group had a higher risk of HZ compared to the 100 mg group, with an IR of 8.7. It was also observed that a previous history of HZ, Asian race, and age ≥50 years were linked to an increased risk [124,169].
Three HZ cases were reported during the induction period of upadacitinib in CD patients and one in the upadacitinib UC trial [170].
Thus, it is recommended that the adjuvanted recombinant HZ subunit vaccine (Shingrix) be administered intramuscularly in two doses 2 months apart to prevent HZ in patients older than 50. Live vaccines (Zostavax®) are contraindicated in patients under immunosuppressive therapy, including JAK inhibitors [154,171].
Hyperlipidemia
Tofacitinib can cause a reversible rise in serum levels of lipids, mainly in the first 6 weeks. After 4–8 weeks of treatment, the levels remain stable and can return to baseline upon cessation of the drug. Previous studies of IBD have shown that inflammation can lower lipid levels; therefore, controlling the inflammatory response may result in higher levels [172].
In the pivotal studies for upadacitinib, it was observed that total cholesterol concentrations were increased in all treatment arms. In contrast, the ratio of low-density lipoprotein and high-density lipoprotein cholesterol remained normal [139]. In filgotinib studies, during induction, there were modest increases in total fasting cholesterol, LDL, and HDL in all treatment groups. However, during maintenance, there was no elevation of blood lipids in the filgotinib groups, and the levels remained stable [173].
Venous Thromboembolism
The FDA and EMA recommend avoiding JAK inhibitors in patients at risk of venous thromboembolism (VTE), including deep vein thrombosis (DVT) and PE (pulmonary embolism). The ORAL Surveillance safety study of tofacitinib in patients with RA ≥ 50 years old with one or more cardiovascular risk factors showed a higher risk of PE in patients on tofacitinib 10 mg bid compared to patients on an anti-TNF [174].
The safety and efficacy of tofacitinib were described in the OCTAVE Open study [135]. The authors concluded that tofacitinib had an acceptable safety profile during long-term therapy for UC. The IRs for thromboembolic events in tofacitinib-treated patients correspond to those reported for UC patients in general. However, the label for tofacitinib in UC was updated to include this risk.
The incidence rate of VTE for upadacitinib was 1.1 per 100 patient-years; in the case of filgotinib, one PE episode was reported in the 100 mg dose arm, and two DVTs were reported in the placebo arm. At this moment, it is unknown if this is a drug class adverse event or due to the inhibition of a specific pathway, data that must be confirmed in long-term studies; therefore, it cannot be established that selective JAK-1 inhibition is a measure to decrease the risk of VTE [175,176].
Cytopenias
Tofacitinib is known to cause a mild and temporary decrease in blood cell counts, but this is usually resolved over time in long-term studies. In a trial involving patients with RA, the incidence rates for neutropenia and lymphopenia were 0.52 and 1.11, respectively. However, none of the patients developed severe infections within a month of their lowest neutrophil count. In cases where patients experienced severe lymphopenia (defined as <0.5 × 103 cells/mm3), there were five instances of associated severe infections. This is believed to be due to the JAK2 signaling blockade, which affects hematopoiesis. Although izencitinib is also a pan-JAK inhibitor, there are no reports of it causing pancytopenia [177].
6.4.2. Ozanimod
Hypertension
Blood pressure should be monitored during ozanimod treatment due to the potential for increased blood pressure. Regardless of the hypertension history, blood pressure should be checked after 3 months of ozanimod treatment, when blood pressure changes were first observed in clinical trials [178,179].
Clinical trial data demonstrated a low incidence of serious infections [≤2.7%] with long-term ozanimod treatment in patients with UC for up to 142 weeks in the phase III True North OLE and in pooled phase II and phase III UC trials examining ozanimod over 2196 patient-years of exposure [180,181].
Infections
Ozanimod treatment should be interrupted or discontinued with certain infections [i.e., serious infection, progressive multifocal leukoencephalopathy, cryptococcal meningitis, and posterior reversible encephalopathy] [179].
Increased Transaminases
Liver enzymes and function should be assessed periodically during treatment (i.e., after 1, 3, 6, 9, and 12 months on ozanimod [per the EU summary of product characteristics] and every 3 months thereafter [per the authors’ recommendation]) or assessed with symptoms of hepatic dysfunction. Treatment should be interrupted if transaminases are confirmed to be >5 times the ULN [per the EU summary of product characteristics] and discontinued in the event of liver injury [178].
6.5. Summary
Small molecules enrich the therapeutic landmark enormously in IBD. The lack of immunogenicity, the comfort of an orally administered compound, and the rapid onset of action justify their increasing use in the treatment of UC and CD patients and could enhance medication adherence. Nevertheless, the place of SMDs in the therapeutic path deserves to be better defined. While antibodies attach to cells and cytokines, small molecules develop effects within the cells, e.g., by inhibiting or promoting transcription. Furthermore, production seems to be cheaper and easier than the manufacture of biologicals. Yet, both patients and physicians need to learn how to handle the new side effects that may limit the usage of small molecules. In conclusion, SMDs are a promising alternative to anti-TNF-α treatments and present many advantages that will possibly make them outdo anti-TNF-α treatments soon, assuming that no serious safety issues occur as their duration of follow-up increases.
7. Role of the Combination of Biologics and/or Small Molecules
7.1. Indications
There are multiple pathways of inflammatory activity activated in patients with IBD, and for this reason, treatment with monotherapies may not be sufficient for the management of all patients [181]. In patients with IBD, there are two distinct scenarios in which it can be used: (1) patients with refractory IBD without EIM; and (2) patients with IBD in remission, but with active EIMs or immune-mediated inflammatory diseases (IMID) [182].
7.2. Evidence
A recent systematic review and meta-analysis by Ahmed and colleagues investigated the safety and efficacy of dual biologic therapy in combination or with tofacitinib in 288 patients with refractory IBD [183]. Most patients were treated with two biological therapies simultaneously while a small proportion of subjects were treated with tofacitinib in combination with vedolizumab (11%), ustekinumab (6%), or anti-TNFα (3%). After a median follow-up of approximately 8 months, the pooled rates of adverse events and serious adverse events were in line with the literature data for biological drugs and small molecules alone. However, more than half of these refractory patients achieved clinical remission, and about a third of them experienced endoscopic remission, suggesting that the combination of two therapies is feasible in selected cases.
Another systematic review with meta-analysis by Alayo et al. assessed the safety and efficacy of dual biologic therapy (DBT) or a small molecule combined with a biologic therapy (SBT) in IBD patients, stratifying the results according to each drug combination [183]. Although DBT was the most frequent approach, the most used combination was tofacitinib with vedolizumab (57 patients, 21.4%) followed by vedolizumab and anti-TNFα (56 patients, 21.0%). Surprisingly, a higher rate of serious adverse events was reported in the vedolizumab–anti-TNFα group (9.6%, 95% CI, 1.5–21.4) compared with the tofacitinib–vedolizumab arm (1.0%, 95% CI, 0.0–7.6). On the other hand, no increased risk was detected with ustekinumab–anti-TNFα, tofacitinib–ustekinumab, tofacitinib–-anti-TNFα, and natalizumab–anti-TNFα. Clinical remission was reported in approximately 50% of all combinations, while endoscopic/radiological remission ranged from 18% with vedolizumab–anti-TNFα to 37.4% with tofacitinib–ustekinumab [184].
Although these data on the use of dual therapy appear promising and reassuring, it must be emphasized that the number of patients analyzed is small and that we need long-term data to draw strong conclusions on the safety profile. While the efficacy advantage associated with the use of two drugs is evident, the data concerning its safety are less clear.
7.3. Pros and Cons of Combination Therapy
The main limitation to the wide use of biologics and small molecules is the risk of infections in patients, but there are no data to support an increased risk of malignancy [185]. Another limitation to the widespread use of dual therapies is the relevant increase in direct healthcare costs. On the other hand, these therapies, allowing for greater treatment efficacy, could reduce the number of IBD-related hospitalizations and surgeries and improve patient productivity by reducing the number of working days lost due to illness. It is, therefore, legitimate to hypothesize that the association of two different therapies is a possible option. However, it is essential to define when this approach should be recommended to avoid over-treatment and expose patients to the risk of adverse events.
7.4. Expert Opinion
In the absence of data, we hypothesize that the combination of a biologic and a small molecule can be considered in patients with severe disease, a high risk of complications, relative contraindications to surgery (i.e., high risk of short bowel syndrome), or concomitant extraintestinal manifestations and active luminal disease where one drug is not enough. Further data confirming this hypothesis or opening new scenarios for the use of this combination are strongly needed.
In conclusion, dual therapy with biologics and small molecules is a promising therapeutic option that could allow the achievement of therapeutic targets and make the goal of a deep and lasting remission more concrete. However, in the absence of long-term safety data, it is right to be cautious and choose this option on a case-by-case basis, sharing the pros and cons of therapy with the patient.
8. Newer and Emerging Modalities
Since multiple inflammatory pathways are activated in the inflamed intestine, blocking one of them might not be sufficient to control inflammation, as we now do with targeted monotherapies. Meanwhile, therapeutic approaches with different mechanisms of action have been investigated from various perspectives. In this section, we discuss several possible future therapeutic targets.
8.1. Gut Microbiota Modulation
In our understanding of IBD, a disturbed gut ecosystem and the inflammatory response to the host microbiota are important concepts. Clinical remission was observed in three out of four ulcerative colitis trials when the fecal microbiota was transferred to reestablish biodiversity [186]. However, there is no agreed protocol for this intervention, and its effects are short-lived. The use of fecal microbiota transfer is restricted to patients with IBD and Clostridium difficile infection. Physicians have been alerted to the serious risk of transmission of multidrug-resistant organisms by the FDA. Early-stage interventions with specific microbial strains or products, as well as prebiotic compounds, are being developed to address this issue [187].
8.2. Stem Cell Therapy
Allogeneic mesenchymal stem (stromal) cells are harvested from adipose tissue through liposuction. After debridement with a curette, flushing with saline, and closure of internal fistula tract openings, cultured and expanded cells (darvadstrocel) are injected next to the tract. Their local exposure to TNF-α and interferon-γ or Toll-like receptor 3 engagement by double-stranded RNA (dsRNA) is believed to induce an immunosuppressive phenotype with the secretion of indoleamine (IDO), prostaglandin E2 (PGE2), nitric oxide (NO), transforming growth factor β (TGF-β), hepatocyte growth factor (HGF), heme oxygenase (HO), and soluble HLA-G (sHLA-G), all of which are known to suppress T cell proliferation and drive differentiation into regulatory T cells (Tregs). Moreover, the production of interleukin-6, IDO, and PGE2 by the mesenchymal stem cells, together with cell–cell contacts, transforms M0 macrophages into anti-inflammatory M2 macrophages. M2 macrophages secrete interleukin-10 and chemokine (C-C motif) ligand 18 (CCL18) and thereby also promote Treg differentiation [188].
8.3. Regulation of Fibrosis
Gastrointestinal stricture is a condition where there is a narrowing of the gastrointestinal tract due to the formation of fibrotic tissue. This is a common complication of Crohn’s disease (CD), a condition that causes chronic inflammation. Fibroblasts get activated due to this inflammation, leading to an excessive accumulation of extracellular matrix (ECM) and the expansion of mesenchymal cells. The production and degradation of ECM are controlled by enzymes called matrix metalloproteinases (MMPs) and MMP inhibitors. When the production of ECM exceeds the degradation rate, it leads to fibrosis. Recent studies have identified some potential therapies for this condition, including anti-fibrotic drugs, anti-MMP9 antibodies, and the inhibition of pH-sensing ovarian cancer G-protein-coupled receptor 1 and BCL2 [189].
8.4. Regulation of Innate Lymphoid Cells
Intestinal lymphoid cells (ILCs) play a significant role in the development of inflammatory bowel disease (IBD) by interacting with the microbiota, regulating the integrity of the epithelial barrier, and producing cytokines. During an active state of IBD, there is an increase in IFN-γ-producing ILC1s and IL-17-producing ILC3s, whereas IL-22-producing ILC3s decrease. While ILC3s are the primary component of intestinal ILCs in their normal state, ILC2s contribute to IBD by sensing the microbiota and maintaining the intestinal barrier. Further research is required to understand the mechanisms that change the subpopulation and function of ILCs and how these cells exert their protective and inflammatory effects [190].
8.5. Regulation of B Cells
B cells at the intestinal mucosal surface are important for immune balance. A dysregulated B cell response is a potential therapeutic target for IBD patients. Inhibiting CD40L may reduce inflammatory IgG1 responses while preserving T cell-independent IgA responses. BAFF is overexpressed in IBD, and belimumab, a human monoclonal anti-BAFF IgG1 antibody, may help alleviate intestinal inflammation. Vedolizumab may inhibit the infiltration of circulating α4β7+ plasmablasts into inflamed mucosa. Blocking the Fcγ receptor function may be an attractive approach for steroid-refractory IBD patients [191].
8.6. Regulation of the Gut-Brain Axis
The gut–brain axis involves bidirectional communication between the gut and nervous system, and it is driven by various signals. The VN is a crucial component of the autonomic nervous system and plays a significant role in the brain–gut axis. Dysregulation of the gut–brain axis is linked to gastrointestinal and neurological diseases and a high risk of developing Parkinson’s disease and MS in IBD patients. The major factors for altered structure and function in the CNS are enteric dysbiosis, translocation of microbial metabolites, and inflammatory factors derived from the inflamed intestinal mucosa that cross the gut epithelial barrier (leaky gut) and blood–brain barrier [192,193].
9. Conclusions
Although the armamentarium for optimizing the therapy of IBD is expanding at a brisk pace, the point of genuine concern is far from satisfactory remission rates, which need a lot to be optimal and desirable. There is a felt need for better-designed clinical trials incorporating a wider population to promote generalizability, the detection of novel biomarkers, and the discovery of new treatment targets to achieve substantial development in the therapy of IBD. There is a requirement for a multimodality approach with probably precision medicine to attain the goal of lasting remission and the probable cure of this enigmatic illness.
Author Contributions
Conceptualization, M.M.; methodology, M.M.; software, M.M, A.A.J., S.D., A.V.P.; validation, M.M.; formal analysis, M.M., A.A.J., S.D., A.V.P.; investigation, M.M., A.A.J., S.D., A.V.P.; resources, M.M., A.A.J., S.D., A.V.P.; data curation, M.M., A.A.J., S.D., A.V.P.; writing—original draft preparation, M.M., A.A.J., S.D., A.V.P.; writing—review and editing, M.M., A.V.P.; visualization, M.M.; supervision, M.M.; project administration, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
The research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Murch, S.H.; Lamkin, V.A.; Savage, M.O.; Walker-Smith, J.A.; MacDonald, T.T. Serum concentrations of tumour necrosis factor alpha in childhood chronic inflammatory bowel disease. Gut 1991, 32, 913–917. [Google Scholar] [CrossRef]
- Braegger, C.P.; Nicholls, S.; Murch, S.H.; MacDonald, T.T.; Stephens, S. Tumour necrosis factor alpha in stool as a marker of intestinal inflammation. Lancet 1992, 339, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Breese, E.J.; Michie, C.A.; Nicholls, S.W.; Murch, S.H.; Williams, C.B.; Domizio, P.; Walker-Smith, J.A.; MacDonald, T.T. Tumor necrosis factor alpha-producing cells in the intestinal mucosa of children with inflammatory bowel disease. Gastroenterology 1994, 106, 1455–1466. [Google Scholar] [CrossRef] [PubMed]
- Derkx, B.; Taminiau, J.; Radema, S.; Stronkhorst, A.; Wortel, C.; Tytgat, G.; van Deventer, S. Tumour-necrosis-factor antibody treatment in Crohn’s disease. Lancet 1993, 342, 173–174. [Google Scholar] [CrossRef]
- Papamichael, K.; Gils, A.; Rutgeerts, P.; Levesque, B.G.; Vermeire, S.; Sandborn, W.J.; Vande Casteele, N. Role for therapeutic drug monitoring during induction therapy with TNF antagonists in IBD: Evolution in the definition and management of primary nonresponse. Inflamm. Bowel Dis. 2015, 21, 182–197. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Chachu, K.A.; Vajravelu, R.K.; Vaughn, B.P.; Ni, J.; Osterman, M.T.; Cheifetz, A.S. Improved Long-term Outcomes of Patients With Inflammatory Bowel Disease Receiving Proactive Compared With Reactive Monitoring of Serum Concentrations of Infliximab. Clin. Gastroenterol. Hepatol. 2017, 15, 1580–1588.e3. [Google Scholar] [CrossRef] [PubMed]
- Zurba, Y.; Gros, B.; Shehab, M. Exploring the Pipeline of Novel Therapies for Inflammatory Bowel Disease; State of the Art Review. Biomedicines 2023, 11, 747. [Google Scholar] [CrossRef] [PubMed]
- Targan, S.R.; Hanauer, S.B.; van Deventer, S.J.; Mayer, L.; Present, D.H.; Braakman, T.; DeWoody, K.L.; Schaible, T.F.; Rutgeerts, P.J. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn’s disease. Crohn’s Disease cA2 Study Group. N. Engl. J. Med. 1997, 337, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Hanauer, S.B.; Feagan, B.G.; Lichtenstein, G.R.; Mayer, L.F.; Schreiber, S.; Colombel, J.F.; Rachmilewitz, D.; Wolf, D.C.; Olson, A.; Bao, W.; et al. Maintenance infliximab for Crohn’s disease: The ACCENT I randomised trial. Lancet 2002, 359, 1541–1549. [Google Scholar] [CrossRef]
- Present, D.H.; Rutgeerts, P.; Targan, S.; Hanauer, S.B.; Mayer, L.; van Hogezand, R.A.; Podolsky, D.K.; Sands, B.E.; Braakman, T.; DeWoody, K.L.; et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N. Engl. J. Med. 1999, 340, 1398–1405. [Google Scholar] [CrossRef]
- Sands, B.E.; Anderson, F.H.; Bernstein, C.N.; Chey, W.Y.; Feagan, B.G.; Fedorak, R.N.; Kamm, M.A.; Korzenik, J.R.; Lashner, B.A.; Onken, J.E.; et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N. Engl. J. Med. 2004, 350, 876–885. [Google Scholar] [CrossRef]
- Colombel, J.F.; Sandborn, W.J.; Reinisch, W.; Mantzaris, G.J.; Kornbluth, A.; Rachmilewitz, D.; Lichtiger, S.; D’Haens, G.; Diamond, R.H.; Broussard, D.L.; et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N. Engl. J. Med. 2010, 362, 1383–1395. [Google Scholar] [CrossRef]
- Schnitzler, F.; Fidder, H.; Ferrante, M.; Noman, M.; Arijs, I.; Van Assche, G.; Hoffman, I.; Van Steen, K.; Vermeire, S.; Rutgeerts, P. Long-term outcome of treatment with infliximab in 614 patients with Crohn’s disease: Results from a single-centre cohort. Gut 2009, 58, 492–500. [Google Scholar] [CrossRef]
- Fidder, H.; Schnitzler, F.; Ferrante, M.; Noman, M.; Katsanos, K.; Segaert, S.; Henckaerts, L.; Van Assche, G.; Vermeire, S.; Rutgeerts, P. Long-term safety of infliximab for the treatment of inflammatory bowel disease: A single-centre cohort study. Gut 2009, 58, 501–508. [Google Scholar] [CrossRef]
- Billiet, T.; Cleynen, I.; Ballet, V.; Ferrante, M.; Van Assche, G.; Gils, A.; Vermeire, S. Prognostic factors for long-term infliximab treatment in Crohn’s disease patients: A 20-year single centre experience. Aliment. Pharmacol. Ther. 2016, 44, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Olivera, P.; Thiriet, L.; Luc, A.; Baumann, C.; Danese, S.; Peyrin-Biroulet, L. Treatment Persistence for Infliximab Versus Adalimumab in Crohn’s Disease: A 14-Year Single-Center Experience. Inflamm. Bowel Dis. 2017, 23, 976–985. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, G.R.; Feagan, B.G.; Cohen, R.D.; Salzberg, B.A.; Safdi, M.; Popp, J.W.; Langholff, W.; Sandborn, W.J. Infliximab for Crohn’s Disease: More Than 13 Years of Real-world Experience. Inflamm. Bowel Dis. 2018, 24, 490–501. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Rutgeerts, P.; Sandborn, W.J.; Sands, B.E.; Diamond, R.H.; Blank, M.; Montello, J.; Tang, L.; Cornillie, F.; Colombel, J.-F. A pooled analysis of infections, malignancy, and mortality in infliximab- and immunomodulator-treated adult patients with inflammatory bowel disease. Am. J. Gastroenterol. 2012, 107, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Mao, E.J.; Hazlewood, G.S.; Kaplan, G.G.; Peyrin-Biroulet, L.; Ananthakrishnan, A.N. Systematic review with meta-analysis: Comparative efficacy of immunosuppressants and biologics for reducing hospitalisation and surgery in Crohn’s disease and ulcerative colitis. Aliment. Pharmacol. Ther. 2017, 45, 3–13. [Google Scholar] [CrossRef]
- Singh, S.; Fumery, M.; Sandborn, W.J.; Murad, M.H. Systematic review and network meta-analysis: First- and second-line biologic therapies for moderate-severe Crohn’s disease. Aliment. Pharmacol. Ther. 2018, 48, 394–409. [Google Scholar] [CrossRef]
- Barreiro-de Acosta, M.; García-Bosch, O.; Souto, R.; Mañosa, M.; Miranda, J.; García-Sanchez, V.; Gordillo, J.; Chacon, S.; Loras, C.; Carpio, D.; et al. Efficacy of infliximab rescue therapy in patients with chronic refractory pouchitis: A multicenter study. Inflamm. Bowel Dis. 2012, 18, 812–817. [Google Scholar] [CrossRef]
- Regueiro, M.; Feagan, B.G.; Zou, B.; Johanns, J.; Blank, M.A.; Chevrier, M.; Plevy, S.; Popp, J.; Cornillie, F.J.; Lukas, M.; et al. Infliximab Reduces Endoscopic, but Not Clinical, Recurrence of Crohn’s Disease After Ileocolonic Resection. Gastroenterology. 2016, 150, 1568–1578. [Google Scholar] [CrossRef]
- Huguet, M.; Pereira, B.; Goutte, M.; Goutorbe, F.; Dubois, A.; Bommelaer, G.; Buisson, A. Systematic Review With Meta-Analysis: Anti-TNF Therapy in Refractory Pouchitis and Crohn’s Disease-Like Complications of the Pouch After Ileal Pouch-Anal Anastomosis Following Colectomy for Ulcerative Colitis. Inflamm. Bowel Dis. 2018, 24, 261–268. [Google Scholar] [CrossRef]
- Cezard, J.P.; Nouaili, N.; Talbotec, C.; Hugot, J.P.; Gobert, J.G.; Schmitz, J.; Mougenot, J.F.; Alberti, C.; Goulet, O. A prospective study of the efficacy and tolerance of a chimeric antibody to tumor necrosis factors in severe pediatric Crohn’s disease. J. Pediatr. Gastroenterol. Nutr. 2003, 36, 632–636. [Google Scholar]
- Armuzzi, A.; Felice, C.; Papa, A.; Marzo, M.; Pugliese, D.; Andrisani, G.; Federico, F.; De Vitis, I.; Rapaccini, G.L.; Guidi, L. Prevention of postoperative recurrence with azathioprine or infliximab in patients with Crohn’s disease: An open-label pilot study. J. Crohn’s Colitis 2013, 7, e623–e629. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef]
- Järnerot, G.; Hertervig, E.; Friis-Liby, I.; Blomquist, L.; Karlén, P.; Grännö, C.; Vilien, M.; Ström, M.; Danielsson, A.; Verbaan, H.; et al. Infliximab as rescue therapy in severe to moderately severe ulcerative colitis: A randomized, placebo-controlled study. Gastroenterology 2005, 128, 1805–1811. [Google Scholar] [CrossRef]
- Laharie, D.; Bourreille, A.; Branche, J.; Allez, M.; Bouhnik, Y.; Filippi, J.; Zerbib, F.; Savoye, G.; Nachury, M.; Moreau, J.; et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: A parallel, open-label randomised controlled trial. Lancet 2012, 380, 1909–1915. [Google Scholar] [CrossRef] [PubMed]
- Laharie, D.; Bourreille, A.; Branche, J.; Allez, M.; Bouhnik, Y.; Filippi, J.; Zerbib, F.; Savoye, G.; Vuitton, L.; Moreau, J.; et al. Long-term outcome of patients with steroid-refractory acute severe UC treated with ciclosporin or infliximab. Gut 2018, 67, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.E.; McGrail, K.M.; Peterson, S.; Raval, M.J.; Karimuddin, A.A.; Phang, P.T.; Bressler, B.; Brown, C.J. Infliximab in ulcerative colitis: The impact of preoperative treatment on rates of colectomy and prescribing practices in the province of British Columbia, Canada. Dis. Colon. Rectum 2014, 57, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Arias, M.T.; Vande Casteele, N.; Vermeire, S.; de Buck van Overstraeten, A.; Billiet, T.; Baert, F.; Wolthuis, A.; Van Assche, G.; Noman, M.; Hoffman, I.; et al. A panel to predict long-term outcome of infliximab therapy for patients with ulcerative colitis. Clin. Gastroenterol. Hepatol. 2015, 13, 531–538. [Google Scholar] [CrossRef]
- Kelly, O.B.; Rosenberg, M.; Tyler, A.D.; Stempak, J.M.; Steinhart, A.H.; Cohen, Z.; Greenberg, G.R.; Silverberg, M.S. Infliximab to Treat Refractory Inflammation After Pelvic Pouch Surgery for Ulcerative Colitis. J. Crohn’s Colitis 2016, 10, 410–417. [Google Scholar] [CrossRef]
- Oussalah, A.; Evesque, L.; Laharie, D.; Roblin, X.; Boschetti, G.; Nancey, S.; Filippi, J.; Flourié, B.; Hebuterne, X.; Bigard, M.-A.; et al. A multicenter experience with infliximab for ulcerative colitis: Outcomes and predictors of response, optimization, colectomy, and hospitalization. Am. J. Gastroenterol. 2010, 105, 2617–2625. [Google Scholar] [CrossRef]
- Ferrante, M.; D’Haens, G.; Dewit, O.; Baert, F.; Holvoet, J.; Geboes, K.; De Hertogh, G.; Van Assche, G.; Vermeire, S.; Rutgeerts, P.; et al. Efficacy of infliximab in refractory pouchitis and Crohn’s disease-related complications of the pouch: A Belgian case series. Inflamm. Bowel Dis. 2010, 16, 243–249. [Google Scholar] [CrossRef]
- Baldassano, R.; Braegger, C.P.; Escher, J.C.; DeWoody, K.; Hendricks, D.F.; Keenan, G.F.; Winter, H.S. Infliximab (REMICADE) therapy in the treatment of pediatric Crohn’s disease. Am. J. Gastroenterol. 2003, 98, 833–838. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Sandborn, W.J.; Rutgeerts, P.; Fedorak, R.N.; Lukas, M.; MacIntosh, D.; Panaccione, R.; Wolf, D.; Pollack, P. Human anti-tumor necrosis factor monoclonal antibody (adalimumab) in Crohn’s disease: The CLASSIC-I trial. Gastroenterology 2006, 130, 323–333, quiz 591. [Google Scholar] [CrossRef] [PubMed]
- Hyams, J.; Crandall, W.; Kugathasan, S.; Griffiths, A.; Olson, A.; Johanns, J.; Liu, G.; Travers, S.; Heuschkel, R.; Markowitz, J.; et al. Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn’s disease in children. Gastroenterology 2007, 132, 863–873, q. [Google Scholar] [CrossRef] [PubMed]
- Baert, F.; Noman, M.; Vermeire, S.; Van Assche, G.; D’ Haens, G.; Carbonez, A.; Rutgeerts, P. Influence of immunogenicity on the long-term efficacy of infliximab in Crohn’s disease. N. Engl. J. Med. 2003, 348, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Nanda, K.S.; Cheifetz, A.S.; Moss, A.C. Impact of antibodies to infliximab on clinical outcomes and serum infliximab levels in patients with inflammatory bowel disease (IBD): A meta-analysis. Am. J. Gastroenterol. 2013, 108, 40–47, quiz 48. [Google Scholar] [CrossRef] [PubMed]
- Bálint, A.; Farkas, K.; Palatka, K.; Lakner, L.; Miheller, P.; Rácz, I.; Hegede, G.; Vincze, Á.; Horváth, G.; Szabó, A.; et al. Efficacy and Safety of Adalimumab in Ulcerative Colitis Refractory to Conventional Therapy in Routine Clinical Practice. J. Crohn’s Colitis 2016, 10, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Hanauer, S.B.; Rutgeerts, P.; Fedorak, R.N.; Lukas, M.; MacIntosh, D.G.; Panaccione, R.; Wolf, D.; Kent, J.D.; Bittle, B.; et al. Adalimumab for maintenance treatment of Crohn’s disease: Results of the CLASSIC II trial. Gut 2007, 56, 1232–1239. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Marano, C.; Zhang, H.; Strauss, R.; Johanns, J.; Adedokun, O.J.; Guzzo, C.; Colombel, J.-F.; Reinisch, W.; et al. Subcutaneous golimumab induces clinical response and remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2014, 146, 85–95, quiz e14–15. [Google Scholar] [CrossRef]
- Hibi, T.; Imai, Y.; Senoo, A.; Ohta, K.; Ukyo, Y. Efficacy and safety of golimumab 52-week maintenance therapy in Japanese patients with moderate to severely active ulcerative colitis: A phase 3, double-blind, randomized, placebo-controlled study-(PURSUIT-J study). J. Gastroenterol. 2017, 52, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Probert, C.S.; Sebastian, S.; Gaya, D.R.; Hamlin, P.J.; Gillespie, G.; Rose, A.; Tate, H.; Wheeler, C.; Irving, P.M. Golimumab induction and maintenance for moderate to severe ulcerative colitis: Results from GO-COLITIS (Golimumab: A Phase 4, UK, open label, single arm study on its utilization and impact in ulcerative Colitis). BMJ Open Gastroenterol. 2018, 5, e000212. [Google Scholar] [CrossRef] [PubMed]
- Greener, T.; Boland, K.; Steinhart, A.H.; Silverberg, M.S. The Unfinished Symphony: Golimumab Therapy for Anti-Tumour Necrosis Factor Refractory Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Pichler, J.; Memaran, N.; Huber, W.D.; Aufricht, C.; Bidmon-Fliegenschnee, B. Golimumab in adolescents with Crohn’s disease refractory to previous tumour necrosis factor antibody. Acta Paediatr. 2021, 110, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Simister, N.E. Placental transport of immunoglobulin G. Vaccine 2003, 21, 3365–3369. [Google Scholar] [CrossRef] [PubMed]
- Mahadevan, U.; Long, M.D.; Kane, S.V.; Roy, A.; Dubinsky, M.C.; Sands, B.E.; Cohen, R.D.; Chambers, C.D.; Sandborn, W.J. Crohn’s Colitis Foundation Clinical Research Alliance Pregnancy and Neonatal Outcomes After Fetal Exposure to Biologics and Thiopurines Among Women With Inflammatory Bowel Disease. Gastroenterology 2021, 160, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Narula, N.; Wong, E.C.L.; Dulai, P.S.; Marshall, J.K.; Colombel, J.-F.; Reinisch, W. Outcomes of Passable and Non-passable Strictures in Clinical Trials of Crohn’s Disease: A Post-hoc Analysis. J. Crohn’s Colitis 2021, 15, 1649–1657. [Google Scholar] [CrossRef]
- Mahadevan, U.; Robinson, C.; Bernasko, N.; Boland, B.; Chambers, C.; Dubinsky, M.; Friedman, S.; Kane, S.; Manthey, J.; Sauberan, J.; et al. Inflammatory Bowel Disease in Pregnancy Clinical Care Pathway: A Report From the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology 2019, 156, 1508–1524. [Google Scholar] [CrossRef]
- Reinisch, W.; Sandborn, W.J.; Hommes, D.W.; D’Haens, G.; Hanauer, S.; Schreiber, S.; Panaccione, R.; Fedorak, R.N.; Tighe, M.B.; Huang, B.; et al. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: Results of a randomised controlled trial. Gut 2011, 60, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results. Gastroenterol. Hepatol. 2013, 9, 317–320.
- Colombel, J.-F.; Sandborn, W.J.; Ghosh, S.; Wolf, D.C.; Panaccione, R.; Feagan, B.; Reinisch, W.; Robinson, A.M.; Lazar, A.; Kron, M.; et al. Four-year maintenance treatment with adalimumab in patients with moderately to severely active ulcerative colitis: Data from ULTRA 1, 2, and 3. Am. J. Gastroenterol. 2014, 109, 1771–1780. [Google Scholar] [CrossRef]
- Levine, J.S.; Burakoff, R. Extraintestinal manifestations of inflammatory bowel disease. Gastroenterol. Hepatol. 2011, 7, 235–241. [Google Scholar]
- Vavricka, S.R.; Gubler, M.; Gantenbein, C.; Spoerri, M.; Froehlich, F.; Seibold, F.; Protic, M.; Michetti, P.; Straumann, A.; Fournier, N.; et al. Anti-TNF Treatment for Extraintestinal Manifestations of Inflammatory Bowel Disease in the Swiss IBD Cohort Study. Inflamm. Bowel Dis. 2017, 23, 1174–1181. [Google Scholar] [CrossRef]
- Thiebault, H.; Boyard-Lasselin, P.; Guignant, C.; Guillaume, N.; Wacrenier, A.; Sabbagh, C.; Rebibo, L.; Brazier, F.; Meynier, J.; Nguyen-Khac, E.; et al. Paradoxical articular manifestations in patients with inflammatory bowel diseases treated with infliximab. Eur. J. Gastroenterol. Hepatol. 2016, 28, 876–881. [Google Scholar] [CrossRef]
- Kugathasan, S.; Miranda, A.; Nocton, J.; Drolet, B.A.; Raasch, C.; Binion, D.G. Dermatologic manifestations of Crohn disease in children: Response to infliximab. J. Pediatr. Gastroenterol. Nutr. 2003, 37, 150–154. [Google Scholar]
- Fries, W.; Giofré, M.R.; Catanoso, M.; Lo Gullo, R. Treatment of acute uveitis associated with Crohn’s disease and sacroileitis with infliximab. Am. J. Gastroenterol. 2002, 97, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Moreland, L.W.; Baumgartner, S.W.; Schiff, M.H.; Tindall, E.A.; Fleischmann, R.M.; Weaver, A.L.; Ettlinger, R.E.; Cohen, S.; Koopman, W.J.; Mohler, K.; et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor (p75)-Fc fusion protein. N. Engl. J. Med. 1997, 337, 141–147. [Google Scholar] [CrossRef]
- Benson, J.M.; Peritt, D.; Scallon, B.J.; Heavner, G.A.; Shealy, D.J.; Giles-Komar, J.M.; Mascelli, M.A. Discovery and mechanism of ustekinumab. MAbs 2011, 3, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, B.; Magnusson, M.K.; Öhman, L. Mucosal immune system of the gastrointestinal tract: Maintaining balance between the good and the bad. Scand. J. Gastroenterol. 2017, 52, 1185–1193. [Google Scholar] [CrossRef]
- Ahluwalia, B.; Moraes, L.; Magnusson, M.K.; Öhman, L. Immunopathogenesis of inflammatory bowel disease and mechanisms of biological therapies. Scand. J. Gastroenterol. 2018, 53, 379–389. [Google Scholar] [CrossRef]
- Monteleone, G.; Biancone, L.; Marasco, R.; Morrone, G.; Marasco, O.; Luzza, F.; Pallone, F. Interleukin 12 is expressed and actively released by Crohn’s disease intestinal lamina propria mononuclear cells. Gastroenterology 1997, 112, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- McGovern, D.; Powrie, F. The IL23 axis plays a key role in the pathogenesis of IBD. Gut 2007, 56, 1333–1336. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, W.; Kolls, J.K.; Zheng, Y. The biological functions of T helper 17 cell effector cytokines in inflammation. Immunity 2008, 28, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Gubler, U.; Chua, A.O.; Schoenhaut, D.S.; Dwyer, C.M.; McComas, W.; Motyka, R.; Nabavi, N.; Wolitzky, A.G.; Quinn, P.M.; Familletti, P.C. Coexpression of two distinct genes is required to generate secreted bioactive cytotoxic lymphocyte maturation factor. Proc. Natl. Acad. Sci. USA 1991, 88, 4143–4147. [Google Scholar] [CrossRef] [PubMed]
- Oppmann, B.; Lesley, R.; Blom, B.; Timans, J.C.; Xu, Y.; Hunte, B.; Vega, F.; Yu, N.; Wang, J.; Singh, K.; et al. Novel p19 protein engages IL-12p40 to form a cytokine, IL-23, with biological activities similar as well as distinct from IL-12. Immunity 2000, 13, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Moschen, A.R.; Tilg, H.; Raine, T. IL-12, IL-23 and IL-17 in IBD: Immunobiology and therapeutic targeting. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Adedokun, O.J.; Xu, Z.; Gasink, C.; Kowalski, K.; Sandborn, W.J.; Feagan, B. Population Pharmacokinetics and Exposure-Response Analyses of Ustekinumab in Patients With Moderately to Severely Active Crohn’s Disease. Clin. Ther. 2022, 44, 1336–1355. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.-L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Sandborn, W.J.; Feagan, B.G.; Gasink, C.; Jacobstein, D.; Zou, B.; Johanns, J.; Adedokun, O.J.; Sands, B.E.; Rutgeerts, P.; et al. IM-UNITI: Three-year Efficacy, Safety, and Immunogenicity of Ustekinumab Treatment of Crohn’s Disease. J. Crohn’s Colitis 2020, 14, 23–32. [Google Scholar] [CrossRef]
- Abreu, M.T.; Rowbotham, D.S.; Danese, S.; Sandborn, W.J.; Miao, Y.; Zhang, H.; Tikhonov, I.; Panaccione, R.; Hisamatsu, T.; Scherl, E.J.; et al. Efficacy and Safety of Maintenance Ustekinumab for Ulcerative Colitis Through 3 Years: UNIFI Long-term Extension. J. Crohn’s Colitis 2022, 16, 1222–1234. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Danese, S.; O’Brien, C.D.; Ott, E.; Marano, C.; Baker, T.; Zhou, Y.; Volger, S.; Tikhonov, I.; et al. Safety of Ustekinumab in Inflammatory Bowel Disease: Pooled Safety Analysis of Results from Phase 2/3 Studies. Inflamm. Bowel Dis. 2021, 27, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Chebli, J.M.F.; Parra, R.S.; Flores, C.; Moraes, A.C.; Nones, R.B.; Gomes, T.N.F.; Perdomo, A.M.B.; Scapini, G.; Zaltman, C. Effectiveness and Safety of Ustekinumab for Moderate to Severely Active Crohn’s Disease: Results from an Early Access Program in Brazil. J. Clin. Med. 2022, 11, 6481. [Google Scholar] [CrossRef]
- Avni-Biron, I.; Mishael, T.; Zittan, E.; Livne-Margolin, M.; Zinger, A.; Tzadok, R.; Goldenberg, R.; Kopylov, U.; Ron, Y.; Hadar, E.; et al. Ustekinumab during pregnancy in patients with inflammatory bowel disease: A prospective multicentre cohort study. Aliment. Pharmacol. Ther. 2022, 56, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Mitrova, K.; Pipek, B.; Bortlik, M.; Bouchner, L.; Brezina, J.; Douda, T.; Drasar, T.; Klvana, P.; Kohout, P.; Leksa, V.; et al. Safety of Ustekinumab and Vedolizumab During Pregnancy-Pregnancy, Neonatal, and Infant Outcome: A Prospective Multicentre Study. J. Crohn’s Colitis 2022, 16, 1808–1815. [Google Scholar] [CrossRef] [PubMed]
- Admin, S. European Crohn’s and Colitis Organisation—ECCO—DOP52 Safety of Inflammatory Bowel Disease Drugs during Pregnancy and Breastfeeding: Mothers and babies’ Outcomes (DUMBO Registry). Available online: https://www.ecco-ibd.eu/publications/congress-abstracts/item/dop52-safety-of-inflammatory-bowel-disease-drugs-during-pregnancy-and-breastfeeding-mothers-and-babies-outcomes-dumbo-registry-2.html (accessed on 16 November 2023).
- Rosh, J.R.; Turner, D.; Griffiths, A.; Cohen, S.A.; Jacobstein, D.; Adedokun, O.J.; Padgett, L.; Terry, N.A.; O’Brien, C.; Hyams, J.S. Ustekinumab in Paediatric Patients with Moderately to Severely Active Crohn’s Disease: Pharmacokinetics, Safety, and Efficacy Results from UniStar, a Phase 1 Study. J. Crohn’s Colitis 2021, 15, 1931–1942. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Seigne, A.-L.; D’huart, M.-C.; Bigard, M.-A.; Peyrin-Biroulet, L. The extra burden of infliximab infusions in inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 2464–2467. [Google Scholar] [CrossRef]
- Tursi, A.; Mocci, G.; Picchio, M.; Elisei, W.; Maconi, G. Letter: Ustekinumab for the treatment of post-surgical and refractory Crohn’s disease. Aliment. Pharmacol. Ther. 2021, 53, 859–860. [Google Scholar] [CrossRef] [PubMed]
- Inc, M.G. Vedolizumab and Ustekinumab for the Treatment of Symptomatic Small… by Dr. Sara El Ouali. Available online: https://eposters.ddw.org/ddw/2021/ddw-2021-virtual/320964/sara.el.ouali.vedolizumab.and.ustekinumab.for.the.treatment.of.symptomatic.html?f=listing%3D5%2Abrowseby%3D8%2Asortby%3D2%2Ace_id%3D2020%2Alabel%3D21916%2Amarker%3D1277 (accessed on 16 November 2023).
- Singh, S.; Proctor, D.; Scott, F.I.; Falck-Ytter, Y.; Feuerstein, J.D. AGA Technical Review on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn’s Disease. Gastroenterology 2021, 160, 2512–2556.e9. [Google Scholar] [CrossRef]
- Chapuis-Biron, C.; Kirchgesner, J.; Pariente, B.; Bouhnik, Y.; Amiot, A.; Viennot, S.; Serrero, M.; Fumery, M.; Allez, M.; Siproudhis, L.; et al. Ustekinumab for Perianal Crohn’s Disease: The BioLAP Multicenter Study From the GETAID. Am. J. Gastroenterol. 2020, 115, 1812–1820. [Google Scholar] [CrossRef]
- Attauabi, M.; Burisch, J.; Seidelin, J.B. Efficacy of ustekinumab for active perianal fistulizing Crohn’s disease: A systematic review and meta-analysis of the current literature. Scand. J. Gastroenterol. 2021, 56, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Guillo, L.; D’Amico, F.; Danese, S.; Peyrin-Biroulet, L. Ustekinumab for Extra-intestinal Manifestations of Inflammatory Bowel Disease: A Systematic Literature Review. J. Crohn’s Colitis 2021, 15, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Sandborn, W.J.; Panaccione, R.; O’Brien, C.D.; Zhang, H.; Johanns, J.; Adedokun, O.J.; Li, K.; Peyrin-Biroulet, L.; Van Assche, G.; et al. Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2019, 381, 1201–1214. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Rebuck, R.; Wang, Y.; Zou, B.; Adedokun, O.J.; Gasink, C.; Sands, B.E.; Hanauer, S.B.; Targan, S.; Ghosh, S.; et al. Five-Year Efficacy and Safety of Ustekinumab Treatment in Crohn’s Disease: The IM-UNITI Trial. Clin. Gastroenterol. Hepatol. 2022, 20, 578–590.e4. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.D.; Cooper, D. Glycobiology of leukocyte trafficking in inflammation. Glycobiology 2014, 24, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Arseneau, K.O.; Cominelli, F. Targeting leukocyte trafficking for the treatment of inflammatory bowel disease. Clin. Pharmacol. Ther. 2015, 97, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Schippers, A.; Muschaweck, M.; Clahsen, T.; Tautorat, S.; Grieb, L.; Tenbrock, K.; Gaßler, N.; Wagner, N. β7-Integrin exacerbates experimental DSS-induced colitis in mice by directing inflammatory monocytes into the colon. Mucosal. Immunol. 2016, 9, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Rosario, M.; Dirks, N.L.; Milch, C.; Parikh, A.; Bargfrede, M.; Wyant, T.; Fedyk, E.; Fox, I. A Review of the Clinical Pharmacokinetics, Pharmacodynamics, and Immunogenicity of Vedolizumab. Clin. Pharmacokinet. 2017, 56, 1287–1301. [Google Scholar] [CrossRef]
- Milch, C.; Wyant, T.; Xu, J.; Parikh, A.; Kent, W.; Fox, I.; Berger, J. Vedolizumab, a monoclonal antibody to the gut homing α4β7 integrin, does not affect cerebrospinal fluid T-lymphocyte immunophenotype. J. Neuroimmunol. 2013, 264, 123–126. [Google Scholar] [CrossRef]
- Zeissig, S.; Rosati, E.; Dowds, C.M.; Aden, K.; Bethge, J.; Schulte, B.; Pan, W.H.; Mishra, N.; Zuhayra, M.; Marx, M.; et al. Vedolizumab is associated with changes in innate rather than adaptive immunity in patients with inflammatory bowel disease. Gut 2019, 68, 25–39. [Google Scholar] [CrossRef]
- Battat, R.; Dulai, P.S.; Jairath, V.; Vande Casteele, N. A product review of vedolizumab in inflammatory bowel disease. Hum. Vaccin. Immunother. 2019, 15, 2482–2490. [Google Scholar] [CrossRef]
- Feagan, B.G.; McDonald, J.; Greenberg, G.; Wild, G.; Pare, P.; Fedorak, R.N.; Landau, S.B.; Brettrnan, L.R. An ascending dose trial of a humanized A4B7 antibody in ulcerative colitis (UC). Gastroenterology 2000, 118, a874. [Google Scholar] [CrossRef]
- Feagan, B.G.; Greenberg, G.R.; Wild, G.; Fedorak, R.N.; Paré, P.; McDonald, J.W.D.; Dubé, R.; Cohen, A.; Steinhart, A.H.; Landau, S.; et al. Treatment of ulcerative colitis with a humanized antibody to the alpha4beta7 integrin. N. Engl. J. Med. 2005, 352, 2499–2507. [Google Scholar] [CrossRef]
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.-F.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.-J.; Danese, S.; et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.-F.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Feagan, B.G.; Rutgeerts, P.; Colombel, J.-F.; Sandborn, W.J.; Sy, R.; D’Haens, G.; Ben-Horin, S.; Xu, J.; Rosario, M.; et al. Effects of vedolizumab induction therapy for patients with Crohn’s disease in whom tumor necrosis factor antagonist treatment failed. Gastroenterology 2014, 147, 618–627.e3. [Google Scholar] [CrossRef] [PubMed]
- Bickston, S.J.; Behm, B.W.; Tsoulis, D.J.; Cheng, J.; MacDonald, J.K.; Khanna, R.; Feagan, B.G. Vedolizumab for induction and maintenance of remission in ulcerative colitis. Cochrane Database Syst. Rev. 2014, 8, CD007571. [Google Scholar] [CrossRef] [PubMed]
- Mosli, M.H.; MacDonald, J.K.; Bickston, S.J.; Behm, B.W.; Tsoulis, D.J.; Cheng, J.; Khanna, R.; Feagan, B.G. Vedolizumab for induction and maintenance of remission in ulcerative colitis: A Cochrane systematic review and meta-analysis. Inflamm. Bowel Dis. 2015, 21, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Peyrin-Biroulet, L.; Loftus, E.V.; Danese, S.; Colombel, J.-F.; Törüner, M.; Jonaitis, L.; Abhyankar, B.; Chen, J.; Rogers, R.; et al. Vedolizumab versus Adalimumab for Moderate-to-Severe Ulcerative Colitis. N. Engl. J. Med. 2019, 381, 1215. [Google Scholar] [CrossRef] [PubMed]
- Travis, S.; Silverberg, M.S.; Danese, S.; Gionchetti, P.; Löwenberg, M.; Jairath, V.; Feagan, B.G.; Bressler, B.; Ferrante, M.; Hart, A.; et al. Vedolizumab for the Treatment of Chronic Pouchitis. N. Engl. J. Med. 2023, 388, 1191–1200. [Google Scholar] [CrossRef] [PubMed]
- Loftus, E.V., Jr.; Feagan, B.G.; Panaccione, R.; Colombel, J.F.; Sandborn, W.J.; Sands, B.E.; Danese, S.; D’Haens, G.; Rubin, D.T.; Shafran, I.; et al. Long-term safety of vedolizumab for inflammatory bowel disease. Aliment Pharmacol Ther. 2020, 52, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.D.; Bhayat, F.; Blake, A.; Travis, S. The Safety Profile of Vedolizumab in Ulcerative Colitis and Crohn’s Disease: 4 Years of Global Post-marketing Data. J. Crohn’s Colitis 2020, 14, 192–204. [Google Scholar] [CrossRef] [PubMed]
- Mahadevan, U.; Vermeire, S.; Lasch, K.; Abhyankar, B.; Bhayat, F.; Blake, A.; Dubinsky, M. Vedolizumab exposure in pregnancy: Outcomes from clinical studies in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 45, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Wils, P.; Seksik, P.; Stefanescu, C.; Nancey, S.; Allez, M.; Pineton de Chambrun, G.; Altwegg, R.; Gilletta, C.; Vuitton, L.; Viennot, S.; et al. Safety of ustekinumab or vedolizumab in pregnant inflammatory bowel disease patients: A multicentre cohort study. Aliment. Pharmacol. Ther. 2021, 53, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.; Tandon, P.; Lentz, E.; Marshall, J.K.; Narula, N. Systematic review and meta-analysis: Safety of vedolizumab during pregnancy in patients with inflammatory bowel disease. J. Gastroenterol. Hepatol. 2021, 36, 2640–2648. [Google Scholar] [CrossRef] [PubMed]
- Ledder, O.; Assa, A.; Levine, A.; Escher, J.C.; de Ridder, L.; Ruemmele, F.; Shah, N.; Shaoul, R.; Wolters, V.M.; Rodrigues, A.; et al. Vedolizumab in Paediatric Inflammatory Bowel Disease: A Retrospective Multi-Centre Experience From the Paediatric IBD Porto Group of ESPGHAN. J. Crohn’s Colitis 2017, 11, 1230–1237. [Google Scholar] [CrossRef]
- Fabiszewska, S.; Derda, E.; Szymanska, E.; Osiecki, M.; Kierkus, J. Safety and Effectiveness of Vedolizumab for the Treatment of Pediatric Patients with Very Early Onset Inflammatory Bowel Diseases. J. Clin. Med. 2021, 10, 2997. [Google Scholar] [CrossRef]
- Fang, S.; Song, Y.; Zhang, C.; Wang, L. Efficacy and safety of vedolizumab for pediatrics with inflammatory bowel disease: A systematic review. BMC Pediatr. 2022, 22, 175. [Google Scholar] [CrossRef]
- Chapuis-Biron, C.; Bourrier, A.; Nachury, M.; Nancey, S.; Bouhnik, Y.; Serrero, M.; Armengol-Debeir, L.; Buisson, A.; Tran-Minh, M.-L.; Zallot, C.; et al. Vedolizumab for perianal Crohn’s disease: A multicentre cohort study in 151 patients. Aliment. Pharmacol. Ther. 2020, 51, 719–727. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Peyrin-Biroulet, L.; Lasch, K.; Adsul, S.; Danese, S. Efficacy and Safety of 2 Vedolizumab Intravenous Regimens for Perianal Fistulizing Crohn’s Disease: ENTERPRISE Study. Clin. Gastroenterol. Hepatol. 2022, 20, 1059–1067.e9. [Google Scholar] [CrossRef]
- Ayoub, F.; Odenwald, M.; Micic, D.; Dalal, S.R.; Pekow, J.; Cohen, R.D.; Rubin, D.T.; Sakuraba, A. Vedolizumab for perianal fistulizing Crohn’s disease: Systematic review and meta-analysis. Intest. Res. 2022, 20, 240–250. [Google Scholar] [CrossRef]
- Hanzel, J.; Ma, C.; Casteele, N.V.; Khanna, R.; Jairath, V.; Feagan, B.G. Vedolizumab and Extraintestinal Manifestations in Inflammatory Bowel Disease. Drugs 2021, 81, 333–347. [Google Scholar] [CrossRef]
- Vedolizumab as Induction and Maintenance Therapy for Ulcerative Colitis | NEJM. Available online: https://www.nejm.org/doi/10.1056/NEJMoa1215734?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200www.ncbi.nlm.nih.gov (accessed on 8 October 2023).
- Ma, C.; Huang, V.; Fedorak, D.K.; Kroeker, K.I.; Dieleman, L.A.; Halloran, B.P.; Fedorak, R.N. Outpatient Ulcerative Colitis Primary Anti-TNF Responders Receiving Adalimumab or Infliximab Maintenance Therapy Have Similar Rates of Secondary Loss of Response. J. Clin. Gastroenterol. 2015, 49, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Roblin, X.; Williet, N.; Boschetti, G.; Phelip, J.-M.; Del Tedesco, E.; Berger, A.-E.; Vedrines, P.; Duru, G.; Peyrin-Biroulet, L.; Nancey, S.; et al. Addition of azathioprine to the switch of anti-TNF in patients with IBD in clinical relapse with undetectable anti-TNF trough levels and antidrug antibodies: A prospective randomised trial. Gut 2020, 69, 1206–1212. [Google Scholar] [CrossRef]
- Ungar, B.; Chowers, Y.; Yavzori, M.; Picard, O.; Fudim, E.; Har-Noy, O.; Kopylov, U.; Eliakim, R.; Ben-Horin, S. ABIRISK consortium The temporal evolution of antidrug antibodies in patients with inflammatory bowel disease treated with infliximab. Gut 2014, 63, 1258–1264. [Google Scholar] [CrossRef]
- Eriksson, C.; Rundquist, S.; Lykiardopoulos, V.; Udumyan, R.; Karlén, P.; Grip, O.; Söderman, C.; Almer, S.; Hertervig, E.; Marsal, J.; et al. Real-world effectiveness of vedolizumab in inflammatory bowel disease: Week 52 results from the Swedish prospective multicentre SVEAH study. Therap. Adv. Gastroenterol. 2021, 14, 17562848211023386. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.H.; Chan, P.W.; Chuah, S.W.; Schwender, B.J.; Kong, S.C.; Ling, K.L. A review of vedolizumab and ustekinumab for the treatment of inflammatory bowel diseases. JGH Open 2018, 2, 223–234. [Google Scholar] [CrossRef]
- Fiorino, G.; Allocca, M.; Correale, C.; Roda, G.; Furfaro, F.; Loy, L.; Zilli, A.; Peyrin-Biroulet, L.; Danese, S. Positioning ustekinumab in moderate-to-severe ulcerative colitis: New kid on the block. Expert Opin. Biol. Ther. 2020, 20, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Kedia, S.; Jain, S.; Gupta, V.; Bopanna, S.; Yadav, D.P.; Goyal, S.; Mouli, V.P.; Dhingra, R.; Makharia, G.; et al. High risk of tuberculosis during infliximab therapy despite tuberculosis screening in inflammatory bowel disease patients in India. Intest. Res. 2018, 16, 588–598. [Google Scholar] [CrossRef]
- Fehily, S.R.; Al-Ani, A.H.; Abdelmalak, J.; Rentch, C.; Zhang, E.; Denholm, J.T.; Johnson, D.; Ng, S.C.; Sharma, V.; Rubin, D.T.; et al. Review article: Latent tuberculosis in patients with inflammatory bowel diseases receiving immunosuppression-risks, screening, diagnosis and management. Aliment. Pharmacol. Ther. 2022, 56, 6–27. [Google Scholar] [CrossRef]
- Higashiyama, M.; Hokari, R. New and Emerging Treatments for Inflammatory Bowel Disease. Digestion 2022, 104, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Al-Bawardy, B.; Shivashankar, R.; Proctor, D.D. Novel and Emerging Therapies for Inflammatory Bowel Disease. Front. Pharmacol. 2021, 12. [Google Scholar] [CrossRef]
- Anderson, C.A.; Boucher, G.; Lees, C.W.; Franke, A.; D’Amato, M.; Taylor, K.D.; Lee, J.C.; Goyette, P.; Imielinski, M.; Latiano, A.; et al. Meta-analysis identifies 29 additional ulcerative colitis risk loci, increasing the number of confirmed associations to 47. Nat. Genet. 2011, 43, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.C.; Hansoul, S.; Nicolae, D.L.; Cho, J.H.; Duerr, R.H.; Rioux, J.D.; Brant, S.R.; Silverberg, M.S.; Taylor, K.D.; Barmada, M.M.; et al. Genome-wide association defines more than 30 distinct susceptibility loci for Crohn’s disease. Nat. Genet. 2008, 40, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Kang, G.; Wang, J.; Gao, X.; Wang, X.; Ye, Y.; Liu, L.; Zhao, J.; Liu, X.; Huang, H.; et al. Breaking through the therapeutic ceiling of inflammatory bowel disease: Dual-targeted therapies. Biomed. Pharmacother. 2023, 158, 114174. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; D’Haens, G.; Wolf, D.C.; Jovanovic, I.; Hanauer, S.B.; Ghosh, S.; Petersen, A.; Hua, S.Y.; Lee, J.H.; et al. Ozanimod as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2021, 385, 1280–1291. [Google Scholar] [CrossRef]
- Danese, S.; Neurath, M.F.; Kopoń, A.; Zakko, S.F.; Simmons, T.C.; Fogel, R.; Siegel, C.A.; Panaccione, R.; Zhan, X.; Usiskin, K.; et al. Effects of Apremilast, an Oral Inhibitor of Phosphodiesterase 4, in a Randomized Trial of Patients With Active Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2020, 18, 2526–2534.e9. [Google Scholar] [CrossRef]
- Atreya, R.; Bloom, S.; Scaldaferri, F.; Gerardi, V.; Admyre, C.; Karlsson, Å.; Knittel, T.; Kowalski, J.; Lukas, M.; Löfberg, R.; et al. Clinical Effects of a Topically Applied Toll-like Receptor 9 Agonist in Active Moderate-to-Severe Ulcerative Colitis. J. Crohn’s Colitis 2016, 10, 1294–1302. [Google Scholar] [CrossRef]
- Nogueira, M.; Puig, L.; Torres, T. JAK Inhibitors for Treatment of Psoriasis: Focus on Selective TYK2 Inhibitors. Drugs 2020, 80, 341–352. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Su, C.; Sands, B.E.; D’Haens, G.R.; Vermeire, S.; Schreiber, S.; Danese, S.; Feagan, B.G.; Reinisch, W.; Niezychowski, W.; et al. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2017, 376, 1723–1736. [Google Scholar] [CrossRef]
- Sands, B.E.; Armuzzi, A.; Marshall, J.K.; Lindsay, J.O.; Sandborn, W.J.; Danese, S.; Panés, J.; Bressler, B.; Colombel, J.-F.; Lawendy, N.; et al. Efficacy and safety of tofacitinib dose de-escalation and dose escalation for patients with ulcerative colitis: Results from OCTAVE Open. Aliment. Pharmacol. Ther. 2020, 51, 271–280. [Google Scholar] [CrossRef]
- Vermeire, S.; Su, C.; Lawendy, N.; Kobayashi, T.; Sandborn, W.J.; Rubin, D.T.; Modesto, I.; Gardiner, S.; Kulisek, N.; Zhang, H.; et al. Outcomes of Tofacitinib Dose Reduction in Patients with Ulcerative Colitis in Stable Remission from the Randomised RIVETING Trial. J. Crohn’s Colitis 2020, 15, 1130–1141. [Google Scholar] [CrossRef] [PubMed]
- Panés, J.; Sandborn, W.J.; Schreiber, S.; Sands, B.E.; Vermeire, S.; D’Haens, G.; Panaccione, R.; Higgins, P.D.R.; Colombel, J.-F.; Feagan, B.G.; et al. Tofacitinib for induction and maintenance therapy of Crohn’s disease: Results of two phase IIb randomised placebo-controlled trials. Gut 2017, 66, 1049–1059. [Google Scholar] [CrossRef]
- Loftus, E.V.; Panés, J.; Lacerda, A.P.; Peyrin-Biroulet, L.; D’Haens, G.; Panaccione, R.; Reinisch, W.; Louis, E.; Chen, M.; Nakase, H.; et al. Upadacitinib Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2023, 388, 1966–1980. [Google Scholar] [CrossRef]
- Danese, S.; Vermeire, S.; Zhou, W.; Pangan, A.L.; Siffledeen, J.; Greenbloom, S.; Hébuterne, X.; D’Haens, G.; Nakase, H.; Panés, J.; et al. Upadacitinib as induction and maintenance therapy for moderately to severely active ulcerative colitis: Results from three phase 3, multicentre, double-blind, randomised trials. Lancet 2022, 399, 2113–2128. [Google Scholar] [CrossRef]
- Schreiber, S.; Feagan, B.G.; Peyrin-Biroulet, L.; Vermeire, S.; Faes, M.; Harris, K.; Oortwijn, A.; Daniele, P.; Patel, H.; Danese, S. Filgotinib Improved Health-Related Quality of Life and Led to Comprehensive Disease Control in Individuals with Ulcerative Colitis: Data from the SELECTION Trial. J. Crohn’s Colitis 2023, 17, 863–875. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, S.; Schreiber, S.; Petryka, R.; Kuehbacher, T.; Hebuterne, X.; Roblin, X.; Klopocka, M.; Goldis, A.; Wisniewska-Jarosinska, M.; Baranovsky, A.; et al. Clinical remission in patients with moderate-to-severe Crohn’s disease treated with filgotinib (the FITZROY study): Results from a phase 2, double-blind, randomised, placebo-controlled trial. Lancet 2017, 389, 266–275. [Google Scholar] [CrossRef]
- D’Haens, G.R.; Lee, S.; Taylor, S.A.; Serone, A.; Rimola, J.; Colombel, J.-F.; Besuyen, R.; Gecse, K.; McKevitt, M.; Reinisch, W.; et al. Filgotinib for the Treatment of Small Bowel Crohn’s Disease: The DIVERGENCE 1 Trial. Gastroenterology 2023, 165, 289–292.e3. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Hanauer, S.; Vermeire, S.; Ghosh, S.; Liu, W.J.; Petersen, A.; Charles, L.; Huang, V.; Usiskin, K.; et al. Long-Term Efficacy and Safety of Ozanimod in Moderately to Severely Active Ulcerative Colitis: Results From the Open-Label Extension of the Randomized, Phase 2 TOUCHSTONE Study. J. Crohn’s Colitis 2021, 15, 1120–1129. [Google Scholar] [CrossRef]
- Feagan, B.G.; Sandborn, W.J.; Danese, S.; Wolf, D.C.; Liu, W.J.; Hua, S.Y.; Minton, N.; Olson, A.; D’Haens, G. Ozanimod induction therapy for patients with moderate to severe Crohn’s disease: A single-arm, phase 2, prospective observer-blinded endpoint study. Lancet Gastroenterol. Hepatol. 2020, 5, 819–828. [Google Scholar] [CrossRef]
- Feagan, B.G.; Schreiber, S.; Afzali, A.; Rieder, F.; Hyams, J.; Kollengode, K.; Pearlman, J.; Son, V.; Marta, C.; Wolf, D.C.; et al. Ozanimod as a novel oral small molecule therapy for the treatment of Crohn’s disease: The YELLOWSTONE clinical trial program. Contemp. Clin. Trials 2022, 122, 106958. [Google Scholar] [CrossRef] [PubMed]
- Hanauer, S.; Panaccione, R.; Danese, S.; Cheifetz, A.; Reinisch, W.; Higgins, P.D.R.; Woodworth, D.A.; Zhang, H.; Friedman, G.S.; Lawendy, N.; et al. Tofacitinib Induction Therapy Reduces Symptoms Within 3 Days for Patients With Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2019, 17, 139–147. [Google Scholar] [CrossRef]
- Berinstein, J.A.; Sheehan, J.L.; Dias, M.; Berinstein, E.M.; Steiner, C.A.; Johnson, L.A.; Regal, R.E.; Allen, J.I.; Cushing, K.C.; Stidham, R.W.; et al. Tofacitinib for Biologic-Experienced Hospitalized Patients With Acute Severe Ulcerative Colitis: A Retrospective Case-Control Study. Clin. Gastroenterol. Hepatol. 2021, 19, 2112–2120.e1. [Google Scholar] [CrossRef]
- Gilmore, R.; Hilley, P.; Srinivasan, A.; Choy, M.; De Cruz, P. Sequential Use of High-Dose Tofacitinib After Infliximab Salvage Theapy in Acute Severe Ulcerative Colitis. J. Crohn’s Colitis 2022, 16, 166–168. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Benoit, N.; Sedano, R.; Jairath, V.; Narula, N.; McCurdy, J.D.; Rosenfeld, G.; Afif, W.; Lakatos, P.L.; Bessissow, T. Effectiveness of Tofacitinib for Hospitalized Patients with Acute Severe Ulcerative Colitis: Case Series. Dig. Dis. Sci. 2022, 67, 5213–5219. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.; Mishra, S.; Sachan, A.; Singh, H.; Singh, A.K.; Sharma, V. Tofacitinib in Acute Severe Ulcerative Colitis: Case Series and a Systematic Review. Inflamm. Bowel Dis. 2021, 27, e101–e103. [Google Scholar] [CrossRef]
- Uzzan, M.; Bresteau, C.; Laharie, D.; Stefanescu, C.; Bellanger, C.; Carbonnel, F.; Serrero, M.; Viennot, S.; Nachury, M.; Amiot, A.; et al. Tofacitinib as salvage therapy for 55 patients hospitalised with refractory severe ulcerative colitis: A GETAID cohort. Aliment. Pharmacol. Ther. 2021, 54, 312–319. [Google Scholar] [CrossRef]
- Gilmore, R.; Tan, W.L.; Fernandes, R.; An, Y.K.; Begun, J. Upadacitinib Salvage Therapy for Infliximab-Experienced Patients with Acute Severe Ulcerative Colitis. J. Crohn’s Colitis 2023, 17, 2033–2036. [Google Scholar] [CrossRef]
- Cohen, N.A.; Dalal, S.R.; Choi, D.; Rubin, D.T. Ozanimod Maintenance Therapy After Cyclosporine Induction in Acute Severe Ulcerative Colitis. ACG Case Rep. J. 2022, 9, e00832. [Google Scholar] [CrossRef]
- Agrawal, M.; Kim, E.S.; Colombel, J.F. JAK Inhibitors Safety in Ulcerative Colitis: Practical Implications. J. Crohn’s Colitis 2020, 14 (Suppl. S2), S755–S760. [Google Scholar] [CrossRef]
- Mahadevan, U.; Dubinsky, M.C.; Su, C.; Lawendy, N.; Jones, T.V.; Marren, A.; Zhang, H.; Graham, D.; Clowse, M.E.B.; Feldman, S.R.; et al. Outcomes of Pregnancies With Maternal/Paternal Exposure in the Tofacitinib Safety Databases for Ulcerative Colitis. Inflamm. Bowel Dis. 2018, 24, 2494–2500. [Google Scholar] [CrossRef]
- Clowse, M.E.B.; Feldman, S.R.; Isaacs, J.D.; Kimball, A.B.; Strand, V.; Warren, R.B.; Xibillé, D.; Chen, Y.; Frazier, D.; Geier, J.; et al. Pregnancy Outcomes in the Tofacitinib Safety Databases for Rheumatoid Arthritis and Psoriasis. Drug Saf. 2016, 39, 755–762. [Google Scholar] [CrossRef]
- Padda, I.S.; Bhatt, R.; Parmar, M. Upadacitinib. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK572088/ (accessed on 8 November 2023).
- Dubinsky, M.C.; Mahadevan, U.; Charles, L.; Afsari, S.; Henry, A.; Comi, G.; Selmaj, K.; van der Woude, C.J. DOP53 Pregnancy outcomes in the ozanimod clinical development program in relapsing multiple sclerosis, Ulcerative Colitis, and Crohn’s Disease. J. Crohn’s Colitis 2021, 15 (Suppl. S1), S088–S089. [Google Scholar] [CrossRef]
- Dolinger, M.T.; Rolfes, P.; Phan, B.L.; Dubinsky, M.C. Letter: Tofacitinib use for bio- logic-refractory paediatric inflammatory bowel disease. Aliment Pharmacol. Ther. 2019, 50, 966–967. [Google Scholar] [CrossRef]
- Collen, L.V. Rapid Clinical Remission With Upadacitinib in a Pediatric Patient With Refractory Crohn’s Disease. Inflamm. Bowel. Dis. 2023, 29, 1175–1176. [Google Scholar] [CrossRef]
- A Study Investigating Oral Ozanimod (RPC1063) in Pediatric Participants with Moderate to Severe Active Ulcerative Colitis [Internet]. Crohn’s & Colitis Foundation. Available online: https://www.crohnscolitisfoundation.org/a-study-investigating-oral-ozanimod-rpc1063-pediatric-participants-with-moderate-to-severe-active-0 (accessed on 18 October 2023).
- Rubin, D.T.; Reinisch, W.; Greuter, T.; Kotze, P.G.; Pinheiro, M.; Mundayat, R.; Maller, E.; Fellmann, M.; Lawendy, N.; Modesto, I.; et al. Extraintestinal manifestations at baseline, and the effect of tofacitinib, in patients with moderate to severe ulcerative colitis. Ther. Adv. Gastroenterol. 2021, 14, 17562848211005708. [Google Scholar] [CrossRef]
- Colombel, J.; Cao, Q.; Ghosh, S.; Reinisch, W.; Zhou, W.; Ilo, D.; Shu, L.; Yao, X.; Rubin, D. OP33 Effect of upadacitinib (UPA) treatment on extraintestinal manifestations (EIMs) in patients with moderate-to-severe Ulcerative Colitis (UC): Results from the UPA Phase 3 programme. J. Crohn’s Colitis 2022, 16, i036–i037. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Danese, S.; Louis, E.; Higgins, P.D.R.; Dubinsky, M.; Cataldi, F.; Zhou, Q.; Lee, W.-J.; Kligys, K.; Lacerda, A.P. DOP50 Effect of upadacitinib on extra-intestinal manifestations in patients with moderate to severe Crohn’s disease: Data from the CELEST study. J. Crohn’s Colitis 2019, 13, S057. [Google Scholar] [CrossRef]
- Lightner, A.L.; Vaidya, P.; Holubar, S.; Warusavitarne, J.; Sahnan, K.; Carrano, F.M.; Spinelli, A.; Zaghiyan, K.; Fleshner, P.R. Perioperative safety of tofacitinib in surgical ulcerative colitis patients. Colorectal. Dis. 2021, 23, 2085–2090. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Alayo, Q.A.; Khatiwada, A.; Lin, B.; Fenster, M.; Dimopoulos, C.; Bader, G.; Weisshof, R.; Jacobs, M.; Gutierrez, A.; et al. Safety of Tofacitinib in a Real-World Cohort of Patients With Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2021, 19, 1592–1601.e3. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Melmed, G.Y.; Vermeire, S.; Long, M.D.; Chan, G.; Pedersen, R.D.; Lawendy, N.; Thorpe, A.J.; Nduaka, C.I.; Su, C. Herpes Zoster Infection in Patients With Ulcerative Colitis Receiving Tofacitinib. Inflamm. Bowel. Dis. 2018, 24, 2258–2265. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.-F. Herpes Zoster in Patients Receiving JAK Inhibitors for Ulcerative Colitis: Mechanism, Epidemiology, Management, and Prevention. Inflamm. Bowel Dis. 2018, 24, 2173–2182. [Google Scholar] [CrossRef]
- Kim, E.S.; Keam, S.J. Filgotinib in Rheumatoid Arthritis: A Profile of Its Use. Clin. Drug Investig. 2021, 41, 741–749. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Loftus, E.V.; Peyrin-Biroulet, L.; Van Assche, G.; D’Haens, G.; Schreiber, S.; Colombel, J.F.; Lewis, J.D.; Ghosh, S.; et al. Efficacy and Safety of Upadacitinib in a Randomized Trial of Patients With Crohn’s Disease. Gastroenterology 2020, 158, 2123–2138.e8. [Google Scholar] [CrossRef] [PubMed]
- Spiewak, T.A.; Patel, A. User’s guide to JAK inhibitors in inflammatory bowel disease. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100096. [Google Scholar] [CrossRef] [PubMed]
- López-Sanromán, A.; Esplugues, J.V.; Domènech, E. Pharmacology and safety of tofacitinib in ulcerative colitis. Gastroenterol. Hepatol. 2021, 44, 39–48. [Google Scholar] [CrossRef]
- Feagan, B.G.; Danese, S.; Loftus, E.V.; Vermeire, S.; Schreiber, S.; Ritter, T.; Fogel, R.; Mehta, R.; Nijhawan, S.; Kempiński, R.; et al. Filgotinib as induction and maintenance therapy for ulcerative colitis (SELECTION): A phase 2b/3 double-blind, randomised, placebo-controlled trial. Lancet 2021, 397, 2372–2384. [Google Scholar] [CrossRef]
- Charles-Schoeman, C.; Fleischmann, R.M.; Mysler, E.; Greenwald, M.; Wang, C.; Chen, A.S.; Connell, C.A.; Woolcott, J.; Menon, S.; Chen, Y.; et al. Pos0239 risk of venous thromboembolic events in patients with rheumatoid arthritis aged ≥50 years with ≥1 cardiovascular risk factor: Results from a phase 3b/4 randomised study of tofacitinib vs tumour necrosis factor inhibitors. Ann. Rheum. Dis. 2022, 81, 358–359. [Google Scholar] [CrossRef]
- Mannucci, A.; D’Amico, F.; El Saadi, A.; Peyrin-Biroulet, L.; Danese, S. Filgotinib for moderately to severely active ulcerative colitis. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 927–940. [Google Scholar] [CrossRef]
- Colombel, J.F.; Panaccione, R.; Nakase, H.; Burmester, G.; Cohen, S.B.; Mease, P.; Guttman-Yassky, E.; Liu, J.; Zhou, W.; Ilo, D.; et al. P573 The safety profile of upadacitinib maintenance therapy in ulcerative colitis in the Phase 3 U-ACHIEVE study is consistent with that in approved indications. J. Crohn’s Colitis 2022, 16, i514. [Google Scholar] [CrossRef]
- Wollenhaupt, J.; Lee, E.-B.; Curtis, J.R.; Silverfield, J.; Terry, K.; Soma, K.; Mojcik, C.; DeMasi, R.; Strengholt, S.; Kwok, K.; et al. Safety and efficacy of tofacitinib for up to 9.5 years in the treatment of rheumatoid arthritis: Final results of a global, open-label, long-term extension study. Arthritis Res. Ther. 2019, 21, 89. [Google Scholar] [CrossRef]
- Bristol Myers Squibb Presents New Zeposia (ozanimod) Data on Long-Term Disease Progression and Cognition in Patients with Relapsing Forms of Multiple Sclerosis. Available online: https://news.bms.com/news/corporate-financial/2023/Bristol-Myers-Squibb-Presents-New-Zeposia-ozanimod-Data-on-Long-Term-Disease-Progression-and-Cognition-in-Patients-with-Relapsing-Forms-of-Multiple-Sclerosis/default.aspx (accessed on 21 November 2023).
- Long-Term Use of Ozanimod in Patients With Moderately to Severely Active Ulcerative Colitis. Gastroenterol. Hepatol. 2022, 18 (Suppl. S1), 6.
- Cree, B.; Danese, S.; Wolf, D.; Alekseeva, O.; Charles, L.; Petersen, A.; Sheffield, J.; Cheng, C.Y.; Riolo, J.; Silva, D.; et al. Long-term Safety of Ozanimod in Relapsing Multiple Sclerosis and Moderately to Severely Active Ulcerative Colitis (P7-3.007). Neurol. J. 2023, 100. [Google Scholar] [CrossRef]
- Graham, D.B.; Xavier, R.J. Pathway paradigms revealed from the genetics of inflammatory bowel disease. Nature 2020, 578, 527–539. [Google Scholar] [CrossRef]
- Gold, S.L.; Steinlauf, A.F. Efficacy and Safety of Dual Biologic Therapy in Patients with Inflammatory Bowel Disease: A Review of the Literature. Gastroenterol. Hepatol. 2021, 17, 406–414. [Google Scholar]
- Ahmed, W.; Galati, J.; Kumar, A.; Christos, P.J.; Longman, R.; Lukin, D.J.; Scherl, E.; Battat, R. Dual Biologic or Small Molecule Therapy for Treatment of Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, e361–e379. [Google Scholar] [CrossRef] [PubMed]
- Alayo, Q.A.; Fenster, M.; Altayar, O.; Glassner, K.L.; Llano, E.; Clark-Snustad, K.; Patel, A.; Kwapisz, L.; Yarur, A.J.; Cohen, B.L.; et al. Systematic Review With Meta-analysis: Safety and Effectiveness of Combining Biologics and Small Molecules in Inflammatory Bowel Disease. Crohns Colitis 360 2022, 4, otac002. [Google Scholar] [CrossRef] [PubMed]
- Bonovas, S.; Fiorino, G.; Allocca, M.; Lytras, T.; Nikolopoulos, G.K.; Peyrin-Biroulet, L.; Danese, S. Biologic Therapies and Risk of Infection and Malignancy in Patients with Inflammatory Bowel Disease: A Systematic Review and Network Meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 1385–1397.e10. [Google Scholar] [CrossRef] [PubMed]
- Amoroso, C.; Perillo, F.; Strati, F.; Fantini, M.C.; Caprioli, F.; Facciotti, F. The Role of Gut Microbiota Biomodulators on Mucosal Immunity and Intestinal Inflammation. Cells 2020, 9, 1234. [Google Scholar] [CrossRef]
- Tan, X.-Y.; Xie, Y.-J.; Liu, X.-L.; Li, X.-Y.; Jia, B. A Systematic Review and Meta-Analysis of Randomized Controlled Trials of Fecal Microbiota Transplantation for the Treatment of Inflammatory Bowel Disease. Evid. Based Complement. Alternat. Med. 2022, 2022, 8266793. [Google Scholar] [CrossRef]
- Bernardo, M.E.; Fibbe, W.E. Mesenchymal stromal cells: Sensors and switchers of inflammation. Cell Stem Cell 2013, 13, 392–402. [Google Scholar] [PubMed]
- Iwata, K.; Mikami, Y.; Kato, M.; Yahagi, N.; Kanai, T. Pathogenesis and management of gastrointestinal inflammation and fibrosis: From inflammatory bowel diseases to endoscopic surgery. Inflamm. Regen. 2021, 41, 21. [Google Scholar] [CrossRef] [PubMed]
- Saez, A.; Gomez-Bris, R.; Herrero-Fernandez, B.; Mingorance, C.; Rius, C.; Gonzalez-Granado, J.M. Innate Lymphoid Cells in Intestinal Homeostasis and Inflammatory Bowel Disease. Int. J. Mol. Sci. 2021, 22, 7618. [Google Scholar] [CrossRef] [PubMed]
- Castro-Dopico, T.; Colombel, J.F.; Mehandru, S. Targeting B cells for inflammatory bowel disease treatment: Back to the future. Curr. Opin. Pharmacol. 2020, 55, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Günther, C.; Rothhammer, V.; Karow, M.; Neurath, M.; Winner, B. The Gut-Brain Axis in Inflammatory Bowel Disease-Current and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 8870. [Google Scholar] [CrossRef]
- Bonaz, B. Is-there a place for vagus nerve stimulation in inflammatory bowel diseases? Bioelectron. Med. 2018, 4, 4. [Google Scholar] [CrossRef]
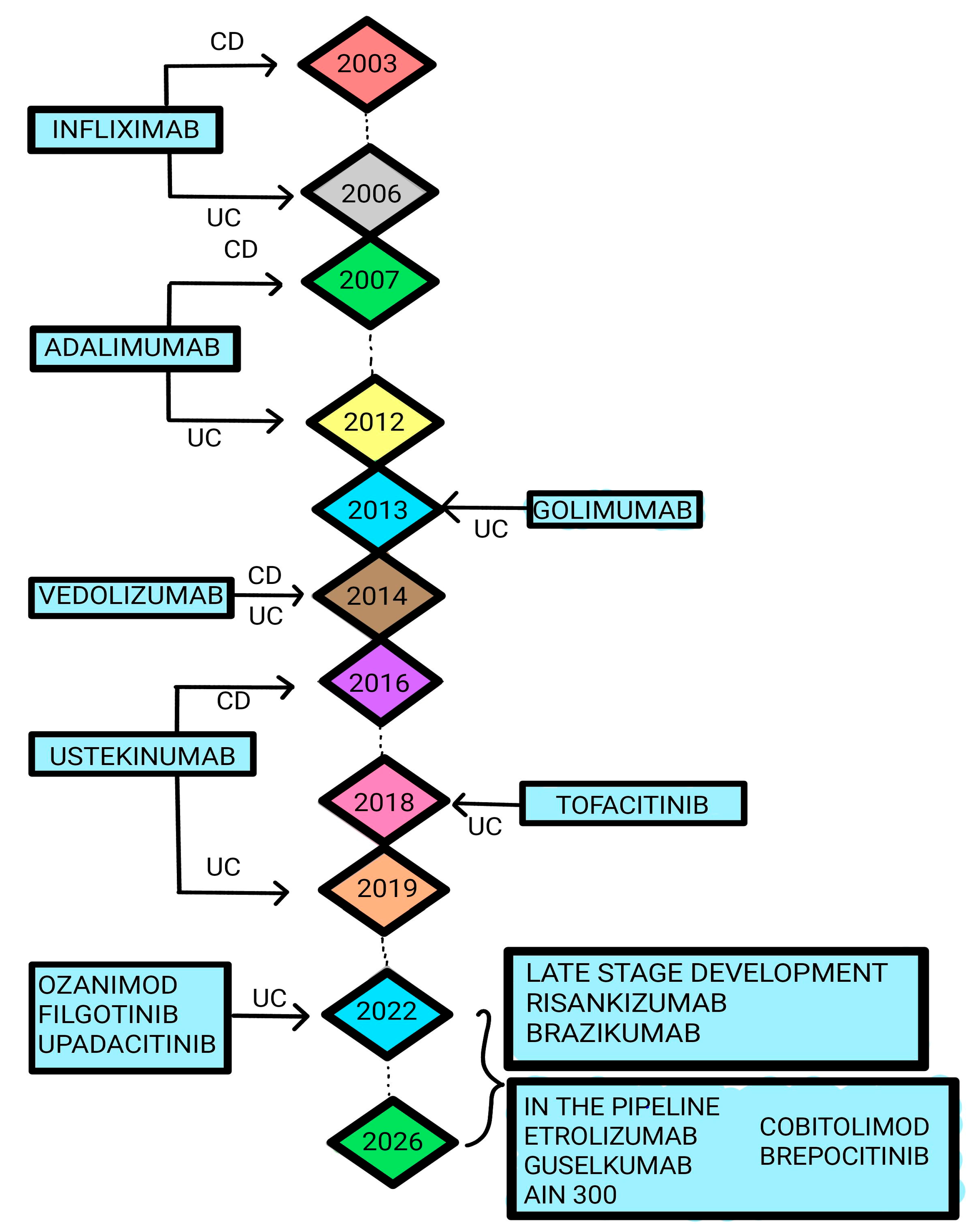
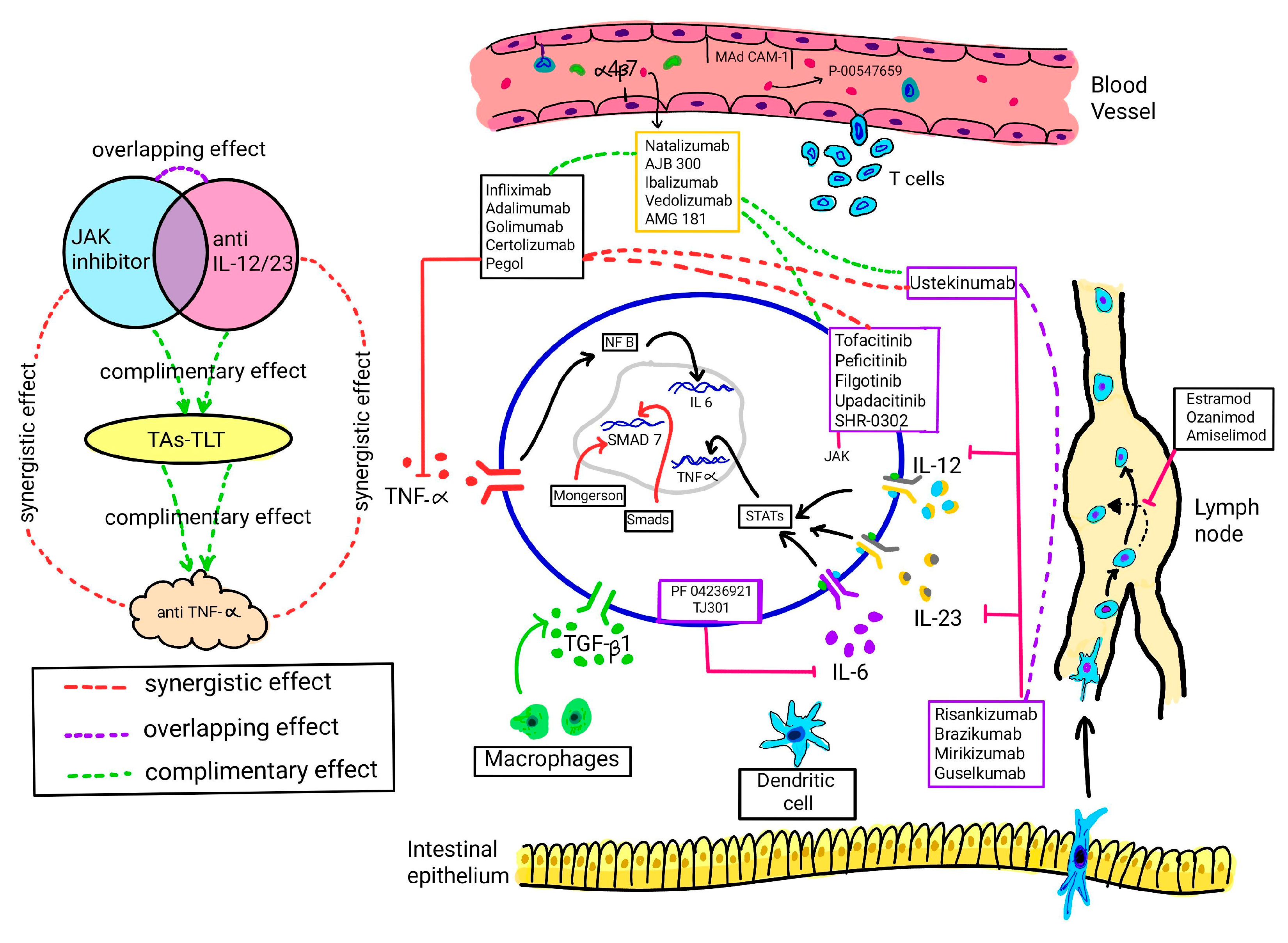
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).