
Thirst Modulates Parasympathetic Recovery: Comparing Oral and Intravenous Rehydration



{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Thirst and Hydration Measures
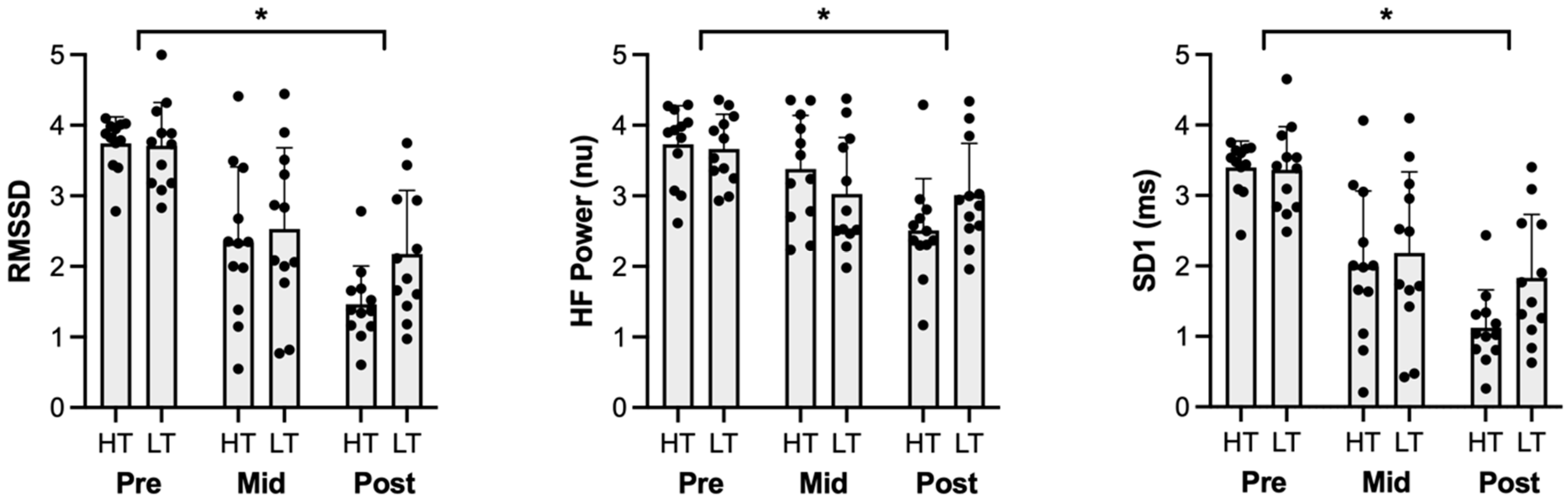
2.2. Decreases in HRV and Vagal Activity Measured by Time Domain
2.3. Decreases Parasympathetic Activity Measured by Frequency Domain
2.4. Parasympathetic and Sympathovagal Balance Is Decreased Measured by Non-Linear Measures
3. Discussion
3.1. Reducing Thirst Increases Parasympathetic Activation
3.2. Thirst Sensation and Sympathetic and Sympathovagal Responses
3.3. Limitations
4. Methods
4.1. Participants
4.2. Experimental Protocol
4.2.1. Visit 1: VO2max
4.2.2. Visits 2 and 3: Experimental Conditions
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Casa, D.J.; Ganio, M.S.; Lopez, R.M.; McDermott, B.P.; Armstrong, L.E.; Maresh, C.M. Intravenous versus Oral Rehydration: Physiological, Performance, and Legal Considerations. Curr. Sports Med. Rep. 2008, 7, S41. [Google Scholar] [CrossRef]
- Pyne, S. Intravenous Fluids Post Marathon. Sports Med. 2007, 37, 434–436. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; Maresh, C.M.; Armstrong, L.E.; Kavouras, S.A.; Herrera, J.A.; Hacker, F.T., Jr.; Keith, N.R.; Elliott, T.A. Intravenous versus oral rehydration during a brief period: Responses to subsequent exercise in the heat. Med. Sci. Sports Exerc. 2000, 32, 124–133. [Google Scholar] [CrossRef]
- Casa, D.J.; Maresh, C.M.; Armstrong, L.E.; Kavouras, S.A.; Herrera-Soto, J.A.; Hacker, F.T., Jr.; Scheett, T.P.; Stoppani, J. Intravenous versus Oral Rehydration during a Brief Period: Stress Hormone Responses to Subsequent Exhaustive Exercise in the Heat. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Kenefick, R.W.; Maresh, C.M.; Armstrong, L.E.; Castellani, J.W.; Riebe, D.; Echegaray, M.E.; Kavorous, S.A. Plasma vasopressin and aldosterone responses to oral and intravenous saline rehydration. J. Appl. Physiol. 2000, 89, 2117–2122. [Google Scholar] [CrossRef] [PubMed]
- Kenefick, R.W.; O’moore, K.M.; Mahood, N.V.; Castellani, J.W. Rapid IV versus Oral Rehydration: Responses to Subsequent Exercise Heat Stress. Med. Sci. Sports Exerc. 2006, 38, 2125. [Google Scholar] [CrossRef]
- Adams, J.D.; Sekiguchi, Y.; Suh, H.G.; Seal, A.D.; Sprong, C.A.; Kirkland, T.W.; Kavouras, S.A. Dehydration Impairs Cycling Performance, Independently of Thirst: A Blinded Study. Med. Sci. Sports Exerc. 2018, 50, 1697–1703. [Google Scholar] [CrossRef]
- Figaro, M.K.; Mack, G.W. Regulation of fluid intake in dehydrated humans: Role of oropharyngeal stimulation. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 1997, 272, R1740–R1746. [Google Scholar] [CrossRef]
- Robertson, G.L. Abnormalities of thirst regulation. Kidney Int. 1984, 25, 460–469. [Google Scholar] [CrossRef]
- Routledge, H.C.; Chowdhary, S.; Coote, J.H.; Townend, J.N. Cardiac vagal response to water ingestion in normal human subjects. Clin. Sci. 2002, 103, 157–162. [Google Scholar] [CrossRef]
- Young, H.A.; Cousins, A.; Johnston, S.; Fletcher, J.M.; Benton, D. Autonomic adaptations mediate the effect of hydration on brain functioning and mood: Evidence from two randomized controlled trials. Sci. Rep. 2019, 9, 16412. [Google Scholar] [CrossRef]
- Aubert, A.E.; Seps, B.; Beckers, F. Heart rate variability in athletes. Sports Med. 2003, 33, 889–919. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, Y.; Huggins, R.A.; Curtis, R.M.; Benjamin, C.L.; Adams, W.M.; Looney, D.P.; West, C.A.; Casa, D.J. Relationship Between Heart Rate Variability and Acute:Chronic Load Ratio Throughout a Season in NCAA D1 Men’s Soccer Players. J. Strength. Cond. Res. 2021, 35, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Vacca, G.; Vono, P. The primary reflex effects of distension of the stomach on heart rate, arterial pressure and left ventricular contractility in the anaesthetized pig. Pflügers Arch. 1993, 425, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Longhurst, J.C.; Ibarra, J. Sympathoadrenal mechanisms in hemodynamic responses to gastric distension in cats. Am. J. Physiol.-Heart Circ. Physiol. 1982, 243, H748–H753. [Google Scholar] [CrossRef]
- Vacca, G.; Mary, D.; Battaglia, A.; Grossini, E.; Molinari, C. The effect of distension of the stomach on peripheral blood flow in anaesthetized pigs. Exp. Physiol. 1996, 81, 385–396. [Google Scholar] [CrossRef]
- Longhurst, J.C.; Spilker, H.L.; Ordway, G.A. Cardiovascular reflexes elicited by passive gastric distension in anesthetized cats. Am. J. Physiol.-Heart Circ. Physiol. 1981, 240, H539–H545. [Google Scholar] [CrossRef]
- Rossi, P.; Andriesse, G.I.; Oey, P.L.; Wieneke, G.H.; Roelofs, J.M.M.; Akkermans, L.M.A. Stomach distension increases efferent muscle sympathetic nerve activity and blood pressure in healthy humans. J. Neurol. Sci. 1998, 161, 148–155. [Google Scholar] [CrossRef]
- Haberich, F.J. Osmoreception in the portal circulation. Fed. Proc. 1968, 27, 1137–1141. [Google Scholar]
- Nakai, M. Cardiovascular Responses to Gastric Hypo-Osmolar Stimulation in Anesthetized Dogs. Jpn. J. Physiol. 1993, 43, 335–346. [Google Scholar] [CrossRef]
- Sekiguchi, Y.; Ky, A.T.; Benjamin, C.L.; Griswold, J.A.; Kavouras, S.A.; Adams, J.D. Thirst sensation decreases exercise performance and increases core temperature and heart rate independent of hydration status. Under Review.
- Goldberger, J.J.; Le, F.K.; Lahiri, M.; Kannankeril, P.J.; Ng, J.; Kadish, A.H. Assessment of parasympathetic reactivation after exercise. Am. J. Physiol.-Heart Circ. Physiol. 2006, 290, H2446–H2452. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Millet, G.P.; Parisy, A.; Pourchez, S.; Laursen, P.B.; Ahmaidi, S. Supramaximal Training and Postexercise Parasympathetic Reactivation in Adolescents. Med. Sci. Sports Exerc. 2008, 40, 362. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Laursen, P.B.; Ahmaidi, S. Parasympathetic reactivation after repeated sprint exercise. Am. J. Physiol.-Heart Circ. Physiol. 2007, 293, H133–H141. [Google Scholar] [CrossRef] [PubMed]
- Maresh, C.M.; Herrera-Soto, J.A.; Armstrong, L.E.; Casa, D.J.; Kavouras, S.A.; Hacker, F.T., Jr.; Elliott, T.A.; Stoppani, J.; Scheett, T.P. Perceptual responses in the heat after brief intravenous versus oral rehydration. Med. Sci. Sports Exerc. 2001, 33, 1039. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public. Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Tiwari, R.; Kumar, R.; Malik, S.; Raj, T.; Kumar, P. Analysis of Heart Rate Variability and Implication of Different Factors on Heart Rate Variability. Curr. Cardiol. Rev. 2021, 17, 11–20. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ky, A.T.; Dunn, R.A.; Keefe, M.S.; Sekiguchi, Y. Thirst Modulates Parasympathetic Recovery: Comparing Oral and Intravenous Rehydration. Physiologia 2025, 5, 16. https://doi.org/10.3390/physiologia5020016
Ky AT, Dunn RA, Keefe MS, Sekiguchi Y. Thirst Modulates Parasympathetic Recovery: Comparing Oral and Intravenous Rehydration. Physiologia. 2025; 5(2):16. https://doi.org/10.3390/physiologia5020016
Chicago/Turabian StyleKy, Alan T., Ryan A. Dunn, Marcos S. Keefe, and Yasuki Sekiguchi. 2025. "Thirst Modulates Parasympathetic Recovery: Comparing Oral and Intravenous Rehydration" Physiologia 5, no. 2: 16. https://doi.org/10.3390/physiologia5020016
APA StyleKy, A. T., Dunn, R. A., Keefe, M. S., & Sekiguchi, Y. (2025). Thirst Modulates Parasympathetic Recovery: Comparing Oral and Intravenous Rehydration. Physiologia, 5(2), 16. https://doi.org/10.3390/physiologia5020016