Abstract
The aging of the global population is a significant and complex phenomenon with far-reaching implications for healthcare systems and society. By 2030, it is projected that the number of individuals over the age of 65 will increase by nearly 1 billion, largely due to advancements in healthcare and improvements in quality of life. Aging is a multifaceted process that encompasses a wide array of changes, spanning from the cellular level to the intricate physiological systems of the human body. At the central nervous system level, aging represents a major risk factor for conditions such as depression and cognitive impairment, which are likely linked to neuroinflammatory processes and can potentially lead to more severe dementias, including Alzheimer’s disease (AD). The higher prevalence of AD in women compared to men has led to speculation that the onset of menopause and associated phenomena, particularly the decline in estrogen levels, may play a role in the development of the disease. Furthermore, research has shown that physical exercise confers both physical and mental health benefits to older adults, with women potentially experiencing the greatest advantages. Understanding the multifaceted nature of aging and its implications for health will ensure that older adults receive the support and care essential for maintaining their health and quality of life.
1. Introduction
Aging is the set of alterations that occur at the cellular and physiological level as a consequence of the passage of time. According to the WHO, it is more precisely defined as the “physiological process that begins at conception and causes changes in the characteristics of the species throughout the life cycle; these changes produce a limitation of the adaptability of the organism in relation to the environment. The rates of these changes in the various organs of the same individual or in different individuals are not the same” [1,2,3]. Population aging is increasing rapidly as health care and living standards improve, especially in developed countries, and this is a major challenge facing the world’s population in general [4,5,6,7].
One of the visible consequences of aging is the onset of cognitive decline. In this last stage of life, the brain begins to atrophy, reducing blood flow and weight. This greatly affects the functioning of the central nervous system (CNS), causing memory loss, difficulty concentrating and learning problems. This reduction in the individual’s capacity is associated with an increased risk of dementia among other phenomena affecting health, such as different types of functional limitations and disability [4,6,8,9,10,11,12,13]. In fact, a first stage is the onset of depression, in turn associated with various risk factors. It is currently considered that between 30–50% of elderly people suffer from depression, a percentage that increases in individuals with cognitive impairment. A similar percentage increase can also be observed with other chronic degenerative diseases [14,15,16].
Among the pathophysiological substrates of these processes is CNS inflammation, also called neuroinflammation, which is also clearly related to cognitive impairment and aging [17]. Moreover, neuroinflammation also seems to be responsible for one of the diseases related to aging, that is, Alzheimer’s disease (AD), or dementia of Alzheimer’s type (DAD). This pathology is a neurodegenerative disorder characterized by the gradual and irreparable deterioration of memory and other cognitive functions, which impairs patients and their mental and social functioning, daily activities and way of life [18]. There are currently almost 50 million people with Alzheimer’s disease globally, with the number expected to increase by 70% by mid-century [19,20,21].
A peculiar feature of AD is that it is diagnosed more frequently in women than in men (almost two-thirds of all patients are women). Although women live an average of 4.5 years longer than men and they outnumber men from the age of 85 years in most subpopulations worldwide, which could explain this difference, it is difficult to assess differences in the actual risk of AD between men and women of the same age, since studies have found contradictory results [21].
However, this difference has been linked to the onset of menopause. Menopause is the change in a woman from a reproductive to a non-reproductive state and is diagnosed 12 months after the permanent cessation of ovarian function. It should be noted that, as life expectancy increases, women live with menopause for about one-third of their lives. It is estimated that by 2030, a total of 1.2 billion women will be menopausal or postmenopausal [22,23,24,25].
In addition, one of the factors that exacerbates a number of health problems, including menopause-related problems themselves, is physical inactivity. Physical exercise has been shown to be one of the non-pharmacological interventions with the most benefits for mental and physical health in older adults and postmenopausal women [26,27,28,29,30,31,32,33,34,35]. In addition, it also has an important role in the prevention of cognitive decline because it induces functional and structural variations in the brain that provide important biological and psychological benefits [7,36,37,38].
The importance of considering sex as a biological variable has been recently highlighted in scientific research, particularly in the field of neuroscience [39,40,41]. The exclusive use of male animal models in preclinical research has led to higher rates of misdiagnosis and adverse side effects in women. The authors also note that the lack of studies that include both sexes in preclinical research is partly due to a lack of incentives [40]. Therefore, a cultural and structural shift is needed in the way research is conducted and scientific progress is evaluated to produce a more equitable, representative, and more translational body of knowledge. Thus, it is crucial to conduct preclinical and clinical studies on both sexes to ensure that research is more representative and accurate. This is especially important when it comes to studying the effects of physical exercise in older people. Physical exercise can have a positive impact on the health of older adults, including improved cardiovascular function, increased muscle strength, and reduced risk of falls [42]. However, the study also found that the benefits of physical exercise may differ between men and women, particularly postmenopausal women. Postmenopausal women are at a higher risk of developing osteoporosis, a condition that weakens bones and increases the risk of fractures [42]. Physical exercise can help prevent osteoporosis by increasing bone density, but the benefits may be more pronounced in postmenopausal women than in men [40]. Therefore, it is essential to provide more incentives for researchers to conduct preclinical and clinical studies on both sexes to ensure that scientific research is more representative and accurate, leading to better health outcomes for all.
The main objective of this work is to know the mechanisms underlying age-related cognitive decline, with a specific emphasis on neuroinflammation, its association with depression and Alzheimer’s disease (AD), and the potential factors contributing to sexual dimorphism, particularly in relation to the hormonal status of women. Additionally, we aim to evaluate the impact of physical exercise as an intervention for preventing these conditions, particularly in the context of menopausal women.
The choice to explore cognitive decline, depression, and physical exercise in the context of menopause is underpinned by their interconnectedness and significant implications for women’s health. Cognitive decline is a complex process influenced by various factors, including neuroinflammation, which has been increasingly recognized as a contributing factor to age-related cognitive impairment. Furthermore, the link between neuroinflammation and its progression to depression and AD is a critical area of study, given the substantial burden of these conditions on individuals and healthcare systems.
Importantly, the hormonal transitions associated with menopause have been identified as a unique period in a woman’s life that may influence cognitive function and mood regulation. The fluctuations in sex hormones, particularly estrogen, during menopause have been implicated in the increased vulnerability to neuroinflammation and the higher prevalence of depression and AD in women. Understanding the underlying mechanisms linking these factors is essential for developing targeted interventions and personalized approaches to mitigate the impact of cognitive decline and mood disorders in menopausal women.
Moreover, the consideration of physical exercise as a potential intervention is motivated by its well-documented benefits in promoting cognitive health and reducing the risk of depression and AD. In the context of menopause, this role becomes even more pertinent due to its potential to mitigate the adverse effects of hormonal changes on brain health and mood regulation. Therefore, evaluating its magnitude as a preventive measure in the context of menopausal women is integral to comprehensively addressing the multifaceted nature of cognitive aging and associated conditions.
2. Methodology
A comprehensive literature review was conducted in the English language utilizing the PUBMED, WEB OF SCIENCE, and Google Scholar databases. Various combinations of search terms, including aging, cognitive impairment, depression, Alzheimer’s disease, menopause, neuroinflammation, and physical exercise, were employed. The search was restricted to articles published within the last six years. All types of scholarly articles were considered for inclusion and were assessed for relevance. Conference abstracts, book references, case reports, and content deemed irrelevant were excluded from the review process.
3. Aging
Aging is a process that takes place at different levels: physiological, morphological, cellular and molecular, but also social and psychological [35]. It is estimated that, by 2030, the number of adults over 65 years of age in the world will increase from 420 million in the year 2000 to almost 1 billion in that year. In Spain, according to data from the National Institute of Statistics (INE) in 2022, this demographic covered approximately 47 million people, of whom 19.9% were aged 65 or over. This means that around 9.3 million people are considered elderly. In addition, the aging of the population is a continuing trend, as the provision of adults over 65 is expected to continue to grow in the coming decades. According to INE projections, in 2031 it is estimated that 23.8% of the Spanish population will be over 65 years of age, and in 2066 this figure could reach 34.7% (Figure 1) [43]. As a result, old age has become the greatest risk component for the development of chronic degenerative conditions [2].
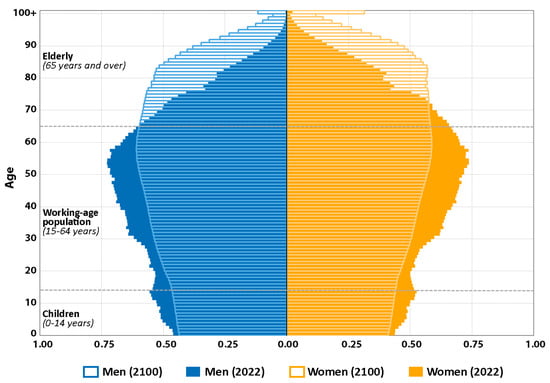
Figure 1.
Pyramid projection of world population by gender and age groups. Age is divided into three categories: children (0–14 years), working-age population (15–64 years) and elderly (65 years and over). The proportion of men (blue) and women (orange) is based on data for the year 2022 and for a projection to the year 2100. A significant increase in the proportion of elderly people is expected for the year 2100, especially among women.
Aging is a process that has been defined as universal, intrinsic, progressive and deleterious: universal, because aging occurs in all individuals; intrinsic, because the causes that produce it are endogenous, that is, it does not depend on external factors; progressive, because it occurs gradually throughout life; and harmful, because that is the way of thinking about any harmful aging process. Moreover, this definition is supported by different theories about how aging develops over time (Figure 2). However, the exact cause is unknown [44]. Among these different theories, the free radical theory states that free oxygen-derived radicals are responsible for age-related oxidative damage. As our antioxidant system cannot cope with all the reactive oxygen species (ROS) produced throughout cellular life, this creates an imbalance between oxidants and antioxidants [38,45,46,47,48].
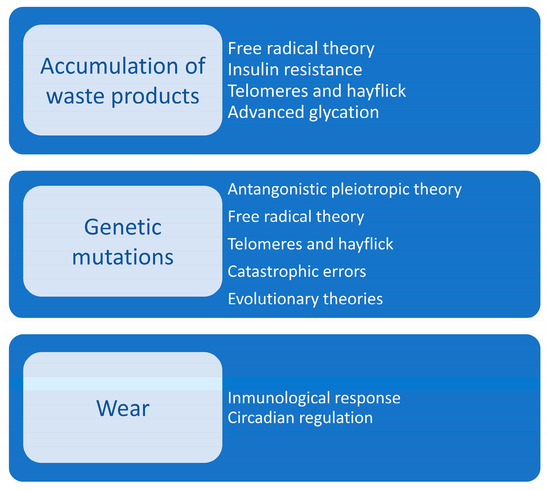
Figure 2.
Theories of aging. The diagram illustrates the three primary categories of aging theories. Each category is further subdivided into specific theories that explain the underlying mechanisms of aging processes, supporting the multifaceted nature of aging and its implications for human health and longevity.
Aging can also be divided now into two types: primary and secondary. Primary aging refers to the varieties observed in aging, those that cannot be avoided and those that are not related to diseases, that is, it focuses on the changes produced in the genetic, molecular and cellular mechanism involved in the process. Secondary aging suggests that it is due to changes produced by external phenomena that occur throughout life, such as habits and lifestyle [38,49,50,51,52]. However, it has been shown that there are multiple functional and morphological changes associated with aging that take place in the locomotor, cardiovascular, central nervous, metabolic and renal systems (Table 1). In general, the cognitive functions of individuals (attention, direction, perception, speed, memory, etc.) will change with increasing age, which will disrupt the psychological mechanisms necessary in the vital process [16,53].

Table 1.
Functional and morphological changes associated with aging that take place at different physiological systems.
At the cardiovascular level, the most relevant changes associated with aging are those that occur in the vascular wall, which promote an increase in arterial pressure with physical exercise. The increase in stiffness also produces ventricular hypertrophy and a lower capacitance of the elastic arteries, leading to difficulty in ventricular emptying and aortic dilatation. From a functional point of view, there is a decrease in vascular response due to the aging of the endothelium by reducing nitric oxide (NO) synthesis and the response to soluble guanylate cyclase (an enzyme that acts as a nitric oxide receptor and is involved in peripheral vasodilatation), thus producing an imbalance between vasodilator and vasoconstrictor substances [3,54].
Focusing additionally on this alteration, it should be pointed out that it is fundamentally characterized by a progressive decrease in the bioavailability of NO and by the increased production of vasoconstrictor factors derived from cyclooxygenase (COX). Both changes are in turn related to increased production of oxygen free radicals or reactive oxygen species (such as peroxides), both of which are vasoconstrictors. However, NO bioavailability varies according to the synthesis from its precursor, the amino acid L-arginine, by endothelial (NOSe), neuronal (NOSn) and inducible (NOSi) NO synthase isoenzymes (NOS). During aging, an increase in asymmetric NG-NG′-dimethyl-arginine (ADMA), which is a by-product of L-arginine methylation, is also observed. This functions as an endogenous inhibitor of NOSe, also producing a decrease in tetrahydrobiopterin (BH4), which is a necessary cofactor for NO synthesis. However, as a compensatory mechanism, there is an increase in NOSi expression, which is related to a pro-atheromatous phenotype and degeneration of the endothelium-dependent vasomotor response [3,54].
Thus, the important role of NO in the maintenance of neurovascular function in the CNS is evident, as it is a vasodilator and an important inhibitor of platelet aggregation. These processes also promote smooth muscle cell destruction and leukocyte adhesion, have anti-inflammatory effects, and promote angiogenesis. As a derivative of endothelial cells, NO acts as an energetic neurovascular–nerve connecting element, in addition to various regular physiological processes, such as immunological processes, vascular tone and neurotransmission processes [18,55,56,57].
Alterations in any of these processes can accelerate cognitive decline. Indeed, NO has also been shown to help regulate the expression and processing of ß-amyloid precursor protein in vascular endothelium and nervous tissue, and acts as a neurovascular protective molecule during aging; however, exercise appears to be a protective factor in cognitive decline by promoting guanylate cyclase signaling and activation of phosphodiesterase isoform inhibitors, mediators of the beneficial effects of endothelial NO [18,55,56,57].
4. Menopause
Menopause is the natural period that all women experience as they age. It is a complex interaction between genetic, biological and psychological factors. Produced by the decline in estrogen levels, it causes a variety of symptoms that can alter a woman’s quality of life, including physical, mental and sexual health [27,58,59] (Figure 3).
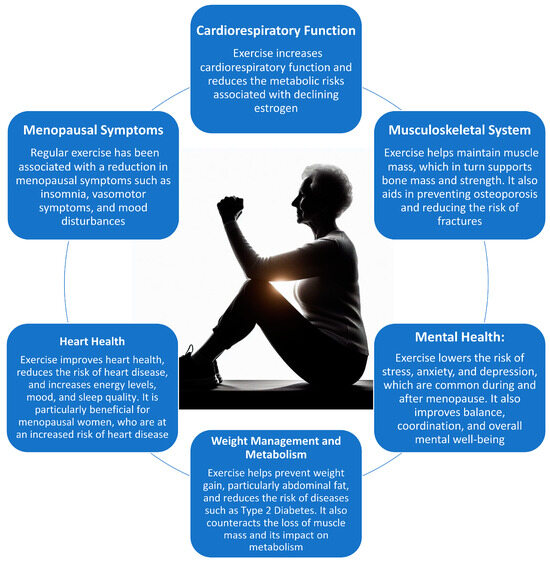
Figure 3.
Effects of physical exercise in several physiological systems in menopausal women.
This universal aging process of the female reproductive system occurs at an average age of 51 years, with a range of 40 to 58 years for 88% of women. From a clinical perspective, premenopausal women have regular menstrual cycles that have less than 7 days of variability in cycle length. Perimenopausal women have irregular menstrual cycles with variations in cycle length of more than 7 days. Menopausal women achieve this designation when they exceed 12 months without a menstrual cycle [60,61,62,63].
From the point of view of endocrine physiology, the onset of menopause is caused by a reduction in the levels of a number of hormones. One of these is hypothalamic inhibin, which, in turn, reduces the synthesis of pituitary follicle stimulating hormone (FSH), leading to a decrease in estradiol (female sex hormone) by the ovary. A decrease in estrogen levels leads to a reduction in the follicular phase, the period of time between the onset of menstruation and ovulation, which results in a shorter duration of menstrual cycles [64].
Another phenomenon that takes place in menopause is the increase of FSH in the blood, due to atresia of the ovarian follicles, reducing the production of estrogens, which are responsible for producing this hormone. This is a form of negative feedback, since the hypothalamus releases more gonadotropin (GnRH), a hormone that releases FSH and luteinizing hormone (LH). Thus, the adenohypophysis receives a signal to release more FSH, produced by the decrease in blood estrogens (especially estradiol), the major problem being a deficit of follicles for such production. Therefore, during menopause, estrone is dominant, whereas during the menstrual cycle 17-ßestradiol (E2) dominates, both estrogens. This occurs because granulosa cells cannot produce aromatase to convert testosterone to estradiol, in addition to the increased peripheral conversion of androstenedione, a steroid hormone produced by the reticular layer of the adrenal cortex, estrone (Figure 4) [64,65,66,67].
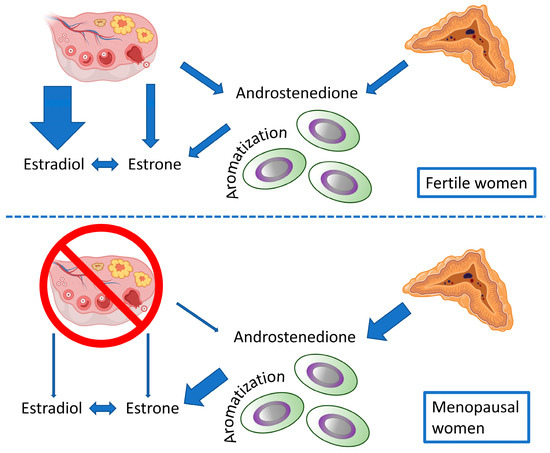
Figure 4.
Hormone synthesis in fertile and menopausal women. The diagram illustrates the conversion of androstenedione to estradiol and estrone in both fertile and menopausal women, through a process called aromatization. The diagram shows that, in fertile women, the ovary is the main site of hormone production while, in menopausal women, the adipose tissue and the adrenal glands take over this role.
Since estrogen receptors appear in all the neuronal structures of the brain that control the multiple functions of the CNS, the lack of estrogen in menopause causes many of these functions to be altered. These receptors are located in plasma membranes, mitochondria and the nucleus of cells, and are particularly abundant in the hypothalamus, which is the main thermo-regulatory center and regulator of sleep and circadian rhythms, as well as other brain regions that are crucial for learning and memory, including the prefrontal cortex, hippocampus, amygdala and posterior cingulate cortex. Other regions also contain significant amounts of estrogen receptors [63,68,69,70].
Preclinical studies indicate that, during perimenopause, when brain estrogens decline, the systems required for estrogenic activation of brain glucose metabolism rates (CMRglc) and suppression of ketogenic pathways are deactivated. Following CMRglc depletion, there is induction of an adaptive starvation reaction to increase fatty acid metabolism for the generation and utilization of ketone bodies by mitochondria as an alternative fuel. Hypometabolism, reduced mitochondrial function and subsequent oxidative damage are known to promote β-amyloid accumulation and neuronal dysfunction [60,63,71,72,73].
As we have indicated above, menopause also affects psychologically due to the various postmenopausal symptoms, such as night sweats (80% of women suffer vasomotor symptoms), hot flashes (temperature dysregulation), pain, fatigue, irritability, vaginal dryness, mood swings, depression and cognitive dysfunction. Some postmenopausal symptoms may last for a long time, being associated with poor quality of life, poorer self-esteem, lower work productivity and greater use of public health resources [24,74,75,76,77,78,79]. Postmenopausal women are also characterized by greater difficulty falling asleep than younger women. Between 40% and 60% report sleeping poorly and suffering from insomnia, which means a poorer quality of life. Poor sleep quality reduces overall health and is associated with physical and psychological problems. In addition, menopausal status is associated with a high risk of mood disorders. In women with no history of depression or anxiety, perimenopausal and postmenopausal phases were associated with an increased risk of anxiety symptoms compared to premenopausal periods [26,80,81,82,83,84,85,86].
Another possible symptom of menopause is the appearance of sarcopenia, which is characterized by the loss of muscle mass, strength and function in older adults, and it is estimated that in postmenopausal women it appears in between 10 and 40%, one of the main causes being hypoestrogenism. In addition, these women have impaired balance related to android fat distribution and low bone mass density and loss of balance, which in turn increases the frequency of falls [30,87,88,89,90].
To assess the severity of menopausal symptoms and their impact on health-related quality of life, the Menopause Rating Scale (MRS) is used. It is a self-administered questionnaire of 11 items agglomerated into three distinct subscales: somatic (four items), psychological (four items) and urogenital (three items). The higher the scores, the greater the severity of symptoms [24,91,92,93].
Importantly, women who were active around menopause had lower rates of cognitive decline compared to women who were inactive at all stages of life, confirming that physical exercise may be a vital protector factor against cognitive decline and dementia [18,94].
5. Neuroinflammation
In recent years neuroinflammation has been recognized as an important signal of neuronal death. Inflammatory processes include injury-induced molecular, cellular and physiological responses designed to prevent and eliminate infection or repair damage. In most cases, the inflammatory process is mediated by immune cells in the periphery and CNS. This process attracts different immune cells depending on the affected tissue, such as astroglia and microglia, which act in the brain tissue. Therefore, we can define it as an activation by different factors of the brain immune response. This results in different events: activation of resident cells, such as astrocytes and microglia, production of proinflammatory mediators, entry of exogenous immune cells (dendritic cells and T lymphocytes) into the cerebral circulation and activation of the complement system, together with an upregulation of cytokine expression [17,95].
The neuroinflammation–neurodegeneration relationship is clear due to the disposition of CNS immune mediators, which induces different pathological conditions related to cognitive limitations. In addition, it is known that, during the course of aging, there is an increased susceptibility to different CNS diseases and increased neuroinflammatory mechanisms, which play a fundamental role in the production of toxins leading to neuronal dysfunction or neuronal death. However, the physiology, molecular signaling pathways and cell types involved in the relationship between cellular senescence and aging processes have not yet been elucidated, but we do know that in senescence there is a secretion of inflammatory proteins that are regulated by different transcription factors, which participate in the regulation of the immune system and are related to the inflammatory response produced by NFkB, a transcription factor of complex activation. However, astrocytes are involved in the neuroimmunology and neuroinflammatory responses of aging and neurodegeneration. This is due to their ability to secrete and respond to large amounts of proinflammatory factors, such as chemokines and immunoregulatory cytokines, to different stimuli [17,96,97,98,99,100].
On the other hand, microglia present several immunophenotypic states: the M1, or proinflammatory, state is characterized by the production of proinflammatory cytokines, such as interleukin (IL), IL-1β, IL-18, TNFα, and chemokines, which promote neuronal death and cognition in chronic inflammation. In the M2 or anti-inflammatory state, the opposite effect occurs, i.e., secretion of anti-inflammatory cytokines (such as T cells and macrophages) facilitating phagocytosis of cellular debris and tissue repair, along with the promotion of extracellular matrix remodeling [2,101,102].
6. Cognitive Impairment
Cognitive impairment is the stage that precedes dementia or other brain diseases. The number of elderly people with different types of dementia is increasing, with AD and vascular dementia being among the most prevalent [16,103]. This occurs in 1% among people aged 80–85 years and in 20% in people over 90 years; in Spain the prevalence is 18.5% [104,105]. It is also suspected that, by 2050, the number of people with dementia will increase to 131.5 million [106,107].
Risk factors associated with cognitive impairment include age, gender, family history, educational level and other factors associated with pathologies [16,53].
Impairment and dementia affect both social life and health, negatively affecting the functional and physical abilities of patients, leading to a state of moderate or severe dependence. At the physiological level, it may be associated with a loss of nerve cells and connections, decreased blood circulation in the brain, reduced production and release of neurotransmitters, and changes in the structure and functions of brain areas responsible for memory and other cognitive functions. In addition, it is closely related to aging due to the decrease in cognitive reserve that aging brings, making the brain more vulnerable to the negative effects of brain diseases and injuries. In other words, cognitive decline is the result of a combination of biological, environmental and lifestyle factors [18,108,109,110,111,112]. In general, studies conclude that factors such as smoking, depressive disorders, diabetes mellitus, metabolic syndrome and APOE ε4 genotype are associated with greater cognitive decline, whereas better physical health, physical activity, Mediterranean diet and cognitive training are protective factors. However, no studies have been found that indicate that it affects women more than men or vice versa [107,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131].
However, different stages of cognitive impairment are known. Mild cognitive impairment without dementia refers to people with persistent complaints of memory loss, but without changes in other cognitive domains. Mild cognitive impairment with suspected dementia presents with more pronounced memory impairment and changes in at least one cognitive domain, such as attention, thinking, language, etc. These changes do not affect the independence and development of the individual, nor do they interfere with work and community functioning of the person, i.e., they do not affect his or her interaction with other people but do affect the ability to solve more complex tasks. These characteristics show that cognitive impairment is age-related. On the other hand, we found studies showing that people with mild cognitive impairment are more likely to suffer AD and to have an alteration in their optimal functioning. However, when depression is associated with this type of impairment, the possibility of AD and death increases [16,132,133].
7. Depression
Depression is a psychological disorder that changes a person’s thinking and behavior and hinders intra- and interpersonal relationships. It is common in the elderly, being considered the second cause of morbidity worldwide. Almost always, it is associated with other pathologies, making this disorder worse and significantly affecting the conditions of life, as those affected lose their sense of purpose in life and perceive their environment negatively. According to the World Health Organization (WHO), the prevalence of geriatric depression has been estimated to be between 10% and 20% of all older adults [16,134,135,136,137].
According to the DSM-5, for a person to be diagnosed with depression, they must have at least five symptoms, which requires the presence of discouragement, a disinterested mindset, and a diminished sense of accomplishment. In addition, they must have these symptoms daily or nearly every day for at least 2 weeks: (a) depressed mood most of the day; (b) marked loss of interest or pleasure in all or nearly all activities most of the day; (c) significant weight or appetite gain or loss, insomnia or lethargy; (d) psychomotor changes detected by an outside informant; (e) fatigue or low energy, feelings of inadequacy or excessive guilt; (f) difficulty in concentrating, and recurrent thoughts of death, suicidal attempts or plans. These symptoms can vary in intensity (mild or severe), making it difficult to perform daily tasks and solve problems. It can be treated without medication if it is mild, and if it is severe medication and psychotherapy are needed, as the affected person may attempt to end his or her own life. Several studies warn that depressive symptoms interfere with proper cognitive processing and that dementia is a risk factor for depressive symptoms, i.e., both factors maintain a fairly significant correlation [16,138].
Several pathophysiological hypotheses have attempted to explain the relationship between depression and cognitive deficit, the most prominent being related to alterations in microglia, nerve shrinkage, brain inflammation and the role of oxidative stress. In addition, it is believed that the location of the brain’s cognitive capacities and its neuroanatomical support for memory and attention change over time, in particular the structure of the prefrontal and temporal cortex, the hippocampus and the limbic system. These same regions are also essential in the processing of emotions, so these functions are expected to be altered in affective disorders [16,139].
One of the theories that has been in force is the monoaminergic theory of depression. This explains that major depressive disorder (MDD) is due to a decrease in the concentration of neurotransmitters at the synaptic level, such as serotonin, noradrenaline and dopamine. In fact, it is the basis of current antidepressant treatment, i.e., the use of selective serotonin reuptake inhibitors (SSRIs). However, it is known that this treatment is not effective in the short term, as it takes about 2–6 weeks to reduce symptoms. This is why other factors, such as genetics, environmental stressors and psychosocial factors, are currently being involved in a multifactorial disease. Together, they produce a maladaptive response, alterations in certain brain areas (prefrontal cortex, hippocampus, limbic system), inflammatory alterations, alterations in neuronal growth factors (brain-derived growth factor or BDNF), and in the hypothalamic–pituitary adrenal axis. Thus, in recent years, the role of glutamate and gamma aminobutyric acid (GABA) neurotransmitter systems in the pathophysiology of MDD has been recognized, since inhibition of N-methyl-D-aspartate receptors (NMDAR) or blockade of glutamate release have a beneficial effect on the damage produced by chronic stress in dendritic atrophy. However, other studies suggest that glutamate activation produces antidepressant effects [140,141,142,143,144,145,146,147,148,149,150,151].
Therefore, the most updated model is the synaptic model of chronic stress condition, where different traumas or repeated exposures to stressors produce a global brain effect of neuronal remodeling with a decrease in its capacity in certain brain areas, such as the left hippocampus and the prefrontal cortex. In addition, it also produces an alteration of glial cells, which are responsible for the regulation of glutamate neurotransmission. Although still unknown, current research proposes that trauma or stress produces an abnormality in glucocorticoid signaling, a modification in glutamate neurotransmission, along with a deficit in glial cell function and an alteration in glutamate uptake. However, it maintains elevated levels of extracellular glutamate [140,149,150,152]. Similarly, acute stress produces, at the frontal lobe level, a glutamate spike associated with a transient increase of glutamate at the extracellular level, causing an increase in glutamate levels.
Similarly, acute stress produces, at the frontal lobe level, a glutamate spike associated with a transient increase in glutamate at the extracellular level, causing a sustained increase in NMDAR receptor activation, α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPAR) and synaptic strengthening, whereas, in chronic stress, there is a decrease in NMDAR, AMPAR and synaptic strength [149,153].
Recent studies have shown that acute stress can have sex-dependent effects on glutamate receptors in the brain [154,155]. Glutamate is the primary excitatory neurotransmitter in the brain and plays a crucial role in many cognitive processes, including learning and memory. The effects of acute stress have been described on glutamate receptors in male and female rats. Acute stress caused a significant increase in the expression of glutamate receptors in the prefrontal cortex of male rats, but not in female rats. The authors suggested that this sex-dependent effect may be due to differences in the regulation of glutamate receptors by sex hormones [156]. Other authors investigated the effects of acute stress on glutamate receptors in male and female mice. Their study found that acute stress caused a significant decrease in the expression of glutamate receptors in the hippocampus of male mice, but not in female mice. The authors suggested that this sex-dependent effect may be due to differences in the regulation of glutamate receptors by stress hormones [155]. Overall, these studies suggest that acute stress can have sex-dependent effects on glutamate receptors in the brain. These effects may be due to differences in the regulation of glutamate receptors by sex hormones and stress hormones.
It has also been observed that this pathology affects women more than men, with higher levels of neuroinflammatory, neurotrophic and serotoninergic markers found in women, and a stronger relationship between neuroinflammatory and neurotrophic factors, together with the severity of depressive symptoms, in this sex [21,157,158,159,160].
8. Cognitive Decline and Alzheimer’s Disease
AD is a multifactorial condition that generates major health, economic and social problems and affects more than 20 million individuals worldwide. At the histological level, it is determined by the appearance of extracellular senile plaques and intracellular neurofibrillary tangles, which lead to neuronal degeneration/death and cognitive loss. Both have been detected in different areas of the brain, with the highest proportion being observed in the cerebral cortex and hippocampus [1,2,161,162,163,164].
Alzheimer’s disease can be sporadic, is associated with old age and with polymorphisms in the apolipoprotein E (APOE) gene, usually 95%, and is also related to lifestyle, environment, etc., or is of the familial type, which is associated with mutations in the amyloid precursor protein (APP), Presenilin 1 (PSEN1) and Presenilin 2 (PSEN2) [1,2,161,162,163,164].
Some proteins have also been described that could be fundamental regulators in the development of aging and AD, one of them being KChlP3. It has different functions: it interrelates with presenilin, it is a transcriptional regulator with the capacity to recognize DRE elements (GTAC G sequence reaction element) that are present in its target genes, specifically in the promoter region and, finally, it interacts with type 1 voltage-dependent potassium channels. Furthermore, this protein is involved in the cognitive impairment associated, during AD, with neuroinflammation and aging. But the mechanism underlying KChIP3 in the brain and periphery is not yet known [2,165,166,167].
KChIP3 belongs to the family of neuronal calcium sensor proteins because of its four calcium binding sites. It is also known by several different names depending on its subcellular location and functions. Thus it is called calsenilin, because it interacts with presenilin, DREAM protein, because it is a transcription factor that binds to DRE (GTCA G) by silencing-off genes for neuronal activation, dendritic growth and memory consolidation, or KChlP3, by interacting with type 1-dependent potassium channels regulating somato-dendritic synapses [2,167,168,169].
Its protein levels are regulated by several factors, including the levels of intracellular calcium, glucose, cAMP and reactive oxygen species (ROS), its main modulator being calcium. However, its absence in the brain means less neuronal death in the hippocampus even at advanced ages, with KChIP3 being compromised in learning and recognition and spatial memory, promoting a proinflammatory environment in the hippocampus and compromising cognitive capacity in aging and AD [2,169].
Regarding the relationship between AD and APOE, it is known that this lipoprotein is responsible for cholesterol and phospholipid transport, and there are three genetic variants: APOE2, APOE3 and APOE4. APOE4 has been established as the strongest genetic risk factor for late-onset AD and dementia, while APOE2 is, to some extent, neuroprotective. APOE4 increases the risk of AD while the ε2 form decreases the risk compared to having the ε3 form [170,171]. Those with one copy of ε4 may have a threefold increased risk of AD compared to those with two copies of the ε3 form, and the risk increases up to 8–12 times higher if they have two copies of the ε4 form. In addition, people with the APOE-ε4 form have been shown to have amyloidosis and dementia at an earlier age than those with ε2 or ε3. Although APOE4 is the major genetic risk factor for the development of AD, women with at least one copy of APOE-ε4 often had a higher risk and more rapid cognitive decline and deterioration than male counterparts. The risk of AD and mild cognitive impairment associated with APOE4 peaks earlier in women than in men, giving a significant elevation between ages 65 and 75 for AD (4.37-fold increased risk in women compared with 3.14 in men) and between ages 55 and 70 for mild cognitive impairment (1.43 in women vs. 1.07 in men), while the risk of AD or APOE4-associated mild cognitive impairment among men peaked in the 75 to 85 age group [19,21,172,173,174,175,176,177,178,179,180,181,182].
Thus, in late-onset AD, the major risk factor is aging, whose prevalence among the 65-year-old population is about 10% and, with increasing age, the prevalence reaches about 32% in people older than 85 years. AD is an abnormal aging where neurons can be found in genomic instability, with DNA damage/oxidation, putative genetic alterations, telomeres, reduction and alteration of metabolic pathways and mitochondrial dysfunction. Aging glia and their activation also influence AD through oxidative stress, neuroinflammation and immune regulation [183]. Oxidative stress is a key factor in the development and progression of AD. Oxidative stress occurs when there is an imbalance between the production of reactive oxygen species (ROS) and the body’s ability to detoxify them. ROS can damage cellular components, such as lipids, proteins, and DNA, leading to inflammation, brain cell death, and cognitive deficits [183]. In fact, drugs with antioxidant activity may be effective in ameliorating the treatment of the disease. Several authors have found that drugs with antioxidant activity, such as vitamin E and melatonin, resveratrol and curcumin, quercetin and luteolin or astaxanthin and alpha-lipoic acid can reduce oxidative stress and improve cognitive function in patients with cognitive decline and dementia [184].
Endocrine factors, especially sex steroid hormones, have been implicated in the onset and progression of AD, and life course changes are risk factors [185]. Age-related declines in female estrogen and male androgen, leading to loss of neuroprotective hormone action, are considered a potential risk factor for the development of AD. Also known as “trigger effects”, these are more transient effects of adult sex hormones. Sex steroid hormones, including estrogens, progestins and androgens, have multiple activating effects on the brain, regulate amyloidosis, tauopathy and gliosis, improve neuronal health, and protect against mild cognitive impairment and AD. In addition, sex hormones may act more generally to enhance brain function [19,21,182,186,187,188,189,190,191]. The renin–angiotensin system has also been involved in AD [192,193].
9. Physical Exercise
The performance of physical exercise promotes a series of physiological processes to adapt to the demands it generates. Thus, on the one hand, there is an increase in blood flow to supply oxygen and nutrients to the active muscles; likewise, there is an increase in heart rate and the force of contraction of the heart to pump more blood to the body, increase blood flow to the muscles and meet their metabolic needs. Increased respiration and dilation of the bronchi becomes necessary to eliminate the carbon dioxide produced by metabolism and, in parallel, supply oxygen to the body. These processes are promoted by the activation of the sympathetic autonomic nervous system, aided by the release of hormones, such as adrenaline and cortisol, that help mobilize stored energy in the body, increase the availability of glucose and fatty acids, and promote the additional metabolism necessary to provide energy to active muscles and maintain body temperature [26,30,194,195,196,197].
Exercise is included in some clinical guidelines as an adjunct to treatment of major depressive disorder. Strength training and multicomponent training are two types of exercise that have been shown to have positive effects on cognitive function in older adults. Strength training is a type of exercise that involves the use of weights or resistance to build muscle strength and endurance. Multicomponent training, on the other hand, is a type of exercise that combines different types of exercise, such as aerobic, strength, balance, and flexibility training, into a single program [198]. Several studies have investigated the effects of strength training and multicomponent training on cognitive function in older adults. For example, a recent meta-analysis [199] found that strength training was associated with significant improvements in cognitive function, particularly in the domains of attention, processing speed, and executive function. Similarly [200], it has been found that multicomponent training was associated with significant improvements in cognitive function, particularly in the domains of memory, attention, and executive function. Another study found similar results on cognitive function in older adults with mild cognitive impairment [201], with significant improvements particularly in the domains of attention and executive function.
A recent meta-analysis supports exercise as an additional lifestyle transformation that improves overall health, including a reduction in depressive symptoms [26,30,194,195]. Furthermore, it has been inversely associated with dementia risk, showing that middle-aged women had greater cognitive improvement than men. A systematic review has described a 50% reduction in the risk of AD when exercise is persistent and intense. In addition, beneficial effects of exercise on anxiety, sleep quality and general symptom perception have also been described [30,202,203,204].
Recently, new physical exercise programs based on physical and mental training have been proposed to prevent cognitive decline in older adults, including the Pilates method and High Intensity Functional Training (HIFT). Pilates is a combination of strength, flexibility and balance exercises, which focuses on lumbar and pelvic stabilization, activates the deep abdominal muscles and seeks a complete mind–body connection. This exercise system is not limited to any age group; in fact, it is widely recommended for older adults due to the lack of impact exercises. Pilates has been shown to have beneficial effects on both physical and mental health, as it promotes coordination of body movements and rhythmic breathing, in addition to the mind–body connection [7,205,206]. On a physiological level, a relationship has been established between physical exercise and an increase in hippocampal size, as well as frontal lobe stimulation, both of which are important aspects in the maintenance of cognitive function [4].
On the other hand, we talk about HIFT, which is a form of exercise that accentuates the functional movements of multiple joints, adapting to any level of physical condition and promoting greater muscle recruitment. These exercises can last from two minutes to over an hour, depending on the intensity of the exercise, as it utilizes multiple energy pathways through multimodal movements, thus being more effective in increasing strength and exercise adherence and having a positive effect, as strength training promotes the release of brain derived neuromuscular factor (BDNF). In addition, HIFT has shown improvements in metabolic and cardiorespiratory adaptations and a positive association between cognition and movement agility in the elderly, thus having a positive effect on cognitive function in older people with mild cognitive impairment [4,207,208,209,210,211,212,213,214,215,216,217].
However, Pilates is recommended for postmenopausal women because it improves physical and mental functioning, independence, sleep quality, reduces fatigue, as well as depression and anxiety, and is associated with a decrease in the rates of cognitive and physical deterioration [26,218]. However, the American Heart Association (AHA) and American College of Sports Medicine (ACSM) recommend a series of exercises that are divided into four areas: aerobic physical education, such as walking, swimming, dancing, or others that involve the use of large muscle groups; muscle strengthening, such as that of the abdomen, arms, legs, etc.; flexibility, improving the activities of daily living; and balance training, which improves stability, in turn reducing the risk of falls [30,219,220].
We can also talk about whole body vibration exercise (WBVE), as it has been shown to reduce arterial stiffness, improve bone mineral density and help reduce symptoms related to osteoporosis and sarcopenia in postmenopausal women [221,222,223,224].
This system is based on putting the patient in contact with a vibrating platform following appropriate parameters of frequency, amplitude, distance and maximum acceleration, producing an increase in muscle strength, including knee extensors and trunk flexion, thus improving balance, as long as it is combined with strength exercises [221,222,223,224].
It also improves bone mineral density because, when a body is subjected to vibration, it requires a greater response of bone and muscle tissues to absorb and dampen the energy produced by the vibration oscillations, thus producing osteogenic effects that oppose the alterations in bone mass that occur as we age [221,222,223,224].
Another beneficial aspect of physical exercise is that it delays arterial aging in postmenopausal women by leading to functional and structural vascular adaptations that help maintain or lower normal blood pressure. It has been observed that people who exercise regularly have less arterial stiffness than sedentary people and, when sedentary people engage in physical exercise, arterial stiffness decreases. Primary functional adaptation is associated with increased NOS enzyme activity and subsequent NO release, whereas moderate or high intensity exercise, especially interval training, produces beneficial endothelial adaptations for postmenopausal women [2,30,225].
10. Conclusions
Although there are different theories of aging, the exact causes of aging are not known, with the most common being in relation to an imbalance between oxidant and antioxidant species and their associated damage. In any case, neuroinflammation of the CNS is provoked, in which both microglia and astroglia intervene, generating alterations that can lead to depression and cognitive deterioration. These phenomena are aggravated in menopausal women, who already have CNS alterations due to the lack of estrogens, which affect various brain regions, some of them crucial for learning and memory, such as the hippocampus, also affected in depression and cognitive impairment. On the other hand, physical exercise can be beneficial due to its capacity to increase the production of NO, growth factors, as well as a better regulation of the balance between oxidative and antioxidant systems. Also noteworthy is the release of hormones, such as cortisol and adrenaline, which are important for blood pressure control and stress reduction, essential in postmenopausal women.
Author Contributions
Conceptualization, C.G.-G., M.J.R.-E. and J.M.M.-M.; methodology, M.J.R.-E. and J.M.M.-M.; investigation, C.G.-G., C.C.-U., M.J.R.-E. and J.M.M.-M.; writing—original draft preparation, C.G.-G., C.C.-U., M.J.R.-E. and J.M.M.-M.; writing—review and editing, C.C.-U., V.C.-H., M.J.R.-E. and J.M.M.-M.; visualization, C.C.-U. and V.C.-H.; supervision, J.M.M.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rowe, J.W. Editorial: Successful Aging: Evolution of a Concept. J. Nutr. Health Aging 2023, 27, 194–195. [Google Scholar] [CrossRef]
- Seifert, C.; Storch, S.; Bahring, R. Modulation of Kv4.2/KChIP3 interaction by the ceroid lipofuscinosis neuronal 3 protein CLN3. J. Biol. Chem. 2020, 295, 12099–12110. [Google Scholar] [CrossRef]
- Ungvari, Z.; Csiszar, A. The emerging role of IGF-1 deficiency in cardiovascular aging: Recent advances. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 599–610. [Google Scholar] [CrossRef]
- Rivas-Campo, Y.; Garcia-Garro, P.A.; Aibar-Almazan, A.; Martinez-Amat, A.; Vega-Avila, G.C.; Afanador-Restrepo, D.F.; Leon-Morillas, F.; Hita-Contreras, F. The Effects of High-Intensity Functional Training on Cognition in Older Adults with Cognitive Impairment: A Systematic Review. Healthcare 2022, 10, 670. [Google Scholar] [CrossRef]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Franco-Martin, M.; Parra-Vidales, E.; Gonzalez-Palau, F.; Bernate-Navarro, M.; Solis, A. The influence of physical exercise in the prevention of cognitive deterioration in the elderly: A systematic review. Rev. Neurol. 2013, 56, 545–554. [Google Scholar]
- Garcia-Garro, P.A.; Hita-Contreras, F.; Martinez-Amat, A.; Achalandabaso-Ochoa, A.; Jimenez-Garcia, J.D.; Cruz-Diaz, D.; Aibar-Almazan, A. Effectiveness of A Pilates Training Program on Cognitive and Functional Abilities in Postmenopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 3580. [Google Scholar] [CrossRef]
- Kawada, T. Which reduces the risk of cognitive impairment: Physical activity or daytime nap? Psychogeriatrics 2022, 22, 772. [Google Scholar] [CrossRef]
- Sun, L.; Yang, Y.; Qiu, Q.; Li, W.; Nie, J.; Zhang, J.; Li, X.; Xiao, S. The Beneficial Effect of Physical Exercise on Cognitive Function in a Non-dementia Aging Chinese Population. Front. Aging Neurosci. 2019, 11, 238. [Google Scholar] [CrossRef]
- Ramirez-Velez, R.; Saez De Asteasu, M.L.; Martinez-Velilla, N.; Zambon-Ferraresi, F.; Garcia-Hermoso, A.; Recarey, A.E.; Fernandez-Irigoyen, J.; Santamaria, E.; Palomino-Echeverria, S.; Izquierdo, M. Circulating Cytokines and Lower Body Muscle Performance in Older Adults at Hospital Admission. J. Nutr. Health Aging 2020, 24, 1131–1139. [Google Scholar] [CrossRef]
- Zeng, D.; Ling, X.Y.; Fang, Z.L.; Lu, Y.F. Optimal exercise to improve physical ability and performance in older adults with sarcopenia: A systematic review and network meta-analysis. Geriatr. Nurs. 2023, 52, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Zhang, F.; Cheng, J.; Huang, Y.; Ren, Z.; Ye, R.; Fan, J.; Li, L.; Gao, Y. The relationship between physical activity and subjective cognitive decline: Evidence from the behavioral risk factor surveillance system (BRFSS). J. Affect. Disord. 2023, 328, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Noguchi-Shinohara, M.; Yokoyama, K.; Komatsu, J.; Masuda, K.; Kouno, M.; Yoshita, M.; Ono, K. Exercise program to reduce the risk of cognitive decline and physical frailty in older adults: Study protocol for an open label double-arm clinical trial. Front. Aging Neurosci. 2023, 15, 1162765. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Cheng, C. Anxiety, Depression, Chronic Pain, and Quality of Life Among Older Adults in Rural China: An Observational, Cross-Sectional, Multi-Center Study. J. Community Health Nurs. 2022, 39, 202–212. [Google Scholar] [CrossRef]
- Segura-Cardona, A.; Cardona-Arango, D.; Segura-Cardona, A.; Garzon-Duque, M. Risk of depression and associated factors in older adults. Antioquia, Colombia. 2012. Rev. Salud Publica 2015, 17, 184–194. [Google Scholar] [CrossRef]
- Su, H.; Zhou, Y.; Sun, Y.; Cai, Y. The relationship between depression and subjective cognitive decline in older adults of China: The mediating role of general self-efficacy. Psychol. Health Med. 2023, 28, 1057–1067. [Google Scholar] [CrossRef]
- Wang, G.; Wang, X.; Zheng, X.; Sun, S.; Zhao, J.; Long, Y.; Mao, Y. Acidic oligosaccharide sugar chain combined with hyperbaric oxygen delays D-galactose-induced brain senescence in mice via attenuating oxidative stress and neuroinflammation. Neurosci. Res. 2022, 185, 40–48. [Google Scholar] [CrossRef]
- Grigoriou, S.S.; Krase, A.A.; Karatzaferi, C.; Giannaki, C.D.; Lavdas, E.; Mitrou, G.I.; Bloxham, S.; Stefanidis, I.; Sakkas, G.K. Long-term intradialytic hybrid exercise training on fatigue symptoms in patients receiving hemodialysis therapy. Int. Urol. Nephrol. 2021, 53, 771–784. [Google Scholar] [CrossRef]
- 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 2023, 19, 1598–1695. [CrossRef]
- Mielke, M.M.; Vemuri, P.; Rocca, W.A. Clinical epidemiology of Alzheimer’s disease: Assessing sex and gender differences. Clin. Epidemiol. 2014, 6, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.; Montagne, A.; Zhao, Z. Alzheimer’s pathogenic mechanisms and underlying sex difference. Cell Mol. Life Sci. 2021, 78, 4907–4920. [Google Scholar] [CrossRef]
- Greendale, G.A.; Karlamangla, A.S.; Maki, P.M. The Menopause Transition and Cognition. JAMA 2020, 323, 1495–1496. [Google Scholar] [CrossRef]
- Merghati-Khoei, E.; Sheikhan, F.; Shamsalizadeh, N.; Haghani, H.; Yousofnia Pasha, Y.R.; Killeen, T. Menopause negatively impacts sexual lives of middle-aged Iranian women: A cross-sectional study. J. Sex. Marital. Ther. 2014, 40, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Perez-Herrezuelo, I.; Aibar-Almazan, A.; Martinez-Amat, A.; Fabrega-Cuadros, R.; Diaz-Mohedo, E.; Wangensteen, R.; Hita-Contreras, F. Female Sexual Function and Its Association with the Severity of Menopause-Related Symptoms. Int. J. Environ. Res. Public Health 2020, 17, 7235. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Li, L. Urban-rural differences in epidemiology and risk factors of menopause syndrome in middle-aged Chinese women. Menopause 2023, 30, 306–316. [Google Scholar] [CrossRef]
- Aibar-Almazan, A.; Hita-Contreras, F.; Cruz-Diaz, D.; de la Torre-Cruz, M.; Jimenez-Garcia, J.D.; Martinez-Amat, A. Effects of Pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: A randomized controlled trial. Maturitas 2019, 124, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Carcelen-Fraile, M.D.C.; Aibar-Almazan, A.; Martinez-Amat, A.; Cruz-Diaz, D.; Diaz-Mohedo, E.; Redecillas-Peiro, M.T.; Hita-Contreras, F. Effects of Physical Exercise on Sexual Function and Quality of Sexual Life Related to Menopausal Symptoms in Peri- and Postmenopausal Women: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2680. [Google Scholar] [CrossRef] [PubMed]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Won, J.; Lee, S.; Hong, Y.; Kim, J.H.; Hong, Y. Benefits of Physical Exercise for Individuals with Fragile X Syndrome in Humans. J. Lifestyle Med. 2015, 5, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, N.; De Teresa, C.; Cano, A.; Godoy, D.; Hita-Contreras, F.; Lapotka, M.; Llaneza, P.; Manonelles, P.; Martinez-Amat, A.; Ocon, O.; et al. Benefits of physical exercise in postmenopausal women. Maturitas 2016, 93, 83–88. [Google Scholar] [CrossRef]
- Yu, R.; Leung, G.; Woo, J. Randomized Controlled Trial on the Effects of a Combined Intervention of Computerized Cognitive Training Preceded by Physical Exercise for Improving Frailty Status and Cognitive Function in Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 1396. [Google Scholar] [CrossRef]
- Ritchie, S.; Lawrence, V.; Jones, J.; Corbett, A. Engaging older adults in an online physical activity programme to improve cognition: A qualitative study. Int. J. Geriatr. Psychiatry 2021, 36, 1942–1949. [Google Scholar] [CrossRef]
- Borsky, P.; Holmannova, D.; Fiala, Z.; Borska, L.; Hruska, L.; Kucera, O. Physiology of ageing. Cas. Lek. Cesk 2022, 161, 11–16. [Google Scholar] [PubMed]
- Li, Q.; Gong, B.; Zhao, Y.; Wu, C. Effect of Exercise Cognitive Combined Training on Physical Function in Cognitively Healthy Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2023, 31, 155–170. [Google Scholar] [CrossRef]
- Li, X.; Karpac, J. Adaptive physiology drives ageing plasticity in locusts. Nat. Ecol. Evol. 2023, 7, 798–799. [Google Scholar] [CrossRef] [PubMed]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef]
- Llopis-Cardona, F.; Armero, C.; Sanfelix-Gimeno, G. Estimating disease incidence rates and transition probabilities in elderly patients using multi-state models: A case study in fragility fracture using a Bayesian approach. BMC Med. Res. Methodol. 2023, 23, 40. [Google Scholar] [CrossRef]
- NIH to require both sexes in preclinical studies. Cancer Discov. 2014, 4, 860. [CrossRef]
- Rich-Edwards, J.W.; Kaiser, U.B.; Chen, G.L.; Manson, J.E.; Goldstein, J.M. Sex and Gender Differences Research Design for Basic, Clinical, and Population Studies: Essentials for Investigators. Endocr. Rev. 2018, 39, 424–439. [Google Scholar] [CrossRef]
- Shansky, R.M.; Murphy, A.Z. Considering sex as a biological variable will require a global shift in science culture. Nat. Neurosci. 2021, 24, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Carmody, C.; Duesing, C.G.; Kane, A.E.; Mitchell, S.J. Is Sex as a Biological Variable Still Being Ignored in Preclinical Aging Research? J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 2177–2180. [Google Scholar] [CrossRef] [PubMed]
- INE. Indicadores de Crecimiento y Estructura de la Población. Available online: https://www.ine.es/dynt3/inebase/es/index.htm?padre=1161&dh=1 (accessed on 24 October 2023).
- Luchsinger, J.A.; Kazemi, E.J.; Sanchez, D.L.; Larkin, M.E.; Valencia, W.M.; Desouza, C.; Carlson, A.L.; Pop-Busui, R.; Seaquist, E.R.; Florez, H.J.; et al. BMI, insulin sensitivity, and cognition in early type 2 diabetes: The Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness Study. Obesity 2023, 31, 1812–1824. [Google Scholar] [CrossRef] [PubMed]
- Harman, D. Aging: Overview. Ann. N. Y. Acad. Sci. 2001, 928, 1–21. [Google Scholar] [CrossRef]
- Harman, D. Aging: A theory based on free radical and radiation chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Strehler, B.L. Aging: A challenge to science, society, and the individual. Clin. Geriatr. Med. 1985, 1, 5–13. [Google Scholar] [CrossRef]
- Vina, J.; Borras, C.; Miquel, J. Theories of ageing. IUBMB Life 2007, 59, 249–254. [Google Scholar] [CrossRef]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef]
- Ong, A.D.; Ram, N. Fragile and Enduring Positive Affect: Implications for Adaptive Aging. Gerontology 2017, 63, 263–269. [Google Scholar] [CrossRef]
- The Lancet Healthy, L. Ageing populations: Unaffordable demography. Lancet Healthy Longev. 2022, 3, e804. [Google Scholar] [CrossRef]
- Dai, Y.; Hsu, Y.C.; Fernandes, B.S.; Zhang, K.; Li, X.; Enduru, N.; Liu, A.; Manuel, A.M.; Jiang, X.; Zhao, Z. Alzheimer’s Disease Neuroimaging Initiative. Disentangling Accelerated Cognitive Decline from the Normal Aging Process and Unraveling Its Genetic Components: A Neuroimaging-Based Deep Learning Approach. J. Alzheimer’s Dis. 2024, 97, 1807–1827. [Google Scholar] [CrossRef]
- Tampi, R.R. Diabetes, Cognition, and Mortality. Am. J. Geriatr. Psychiatry 2023, 31, 583–585. [Google Scholar] [CrossRef] [PubMed]
- Nigam, Y.; Knight, J.; Bhattacharya, S.; Bayer, A. Physiological changes associated with aging and immobility. J. Aging Res. 2012, 2012, 468469. [Google Scholar] [CrossRef] [PubMed]
- Katusic, Z.S.; Austin, S.A. Neurovascular Protective Function of Endothelial Nitric Oxide—Recent Advances. Circ. J. 2016, 80, 1499–1503. [Google Scholar] [CrossRef] [PubMed]
- Lourenco, C.F.; Ledo, A.; Barbosa, R.M.; Laranjinha, J. Neurovascular-neuroenergetic coupling axis in the brain: Master regulation by nitric oxide and consequences in aging and neurodegeneration. Free Radic. Biol. Med. 2017, 108, 668–682. [Google Scholar] [CrossRef]
- Pitsikas, N. The role of nitric oxide in the object recognition memory. Behav. Brain Res. 2015, 285, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Forman, M.R.; Mangini, L.D.; Thelus-Jean, R.; Hayward, M.D. Life-course origins of the ages at menarche and menopause. Adolesc. Health Med. Ther. 2013, 4, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Shirvani, M.; Heidari, M. Quality of Life in Postmenopausal Female Members and Non-members of the Elderly Support Association. J. Menopausal Med. 2016, 22, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Brinton, R.D.; Yao, J.; Yin, F.; Mack, W.J.; Cadenas, E. Perimenopause as a neurological transition state. Nat. Rev. Endocrinol. 2015, 11, 393–405. [Google Scholar] [CrossRef]
- Harlow, S.D.; Gass, M.; Hall, J.E.; Lobo, R.; Maki, P.; Rebar, R.W.; Sherman, S.; Sluss, P.M.; de Villiers, T.J.; Group, S.C. Executive summary of the Stages of Reproductive Aging Workshop + 10: Addressing the unfinished agenda of staging reproductive aging. Menopause 2012, 19, 387–395. [Google Scholar] [CrossRef]
- Nelson, H.D. Menopause. Lancet 2008, 371, 760–770. [Google Scholar] [CrossRef]
- Scheyer, O.; Rahman, A.; Hristov, H.; Berkowitz, C.; Isaacson, R.S.; Diaz Brinton, R.; Mosconi, L. Female Sex and Alzheimer’s Risk: The Menopause Connection. J. Prev. Alzheimers Dis. 2018, 5, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Armeni, A.; Armeni, E.; Augoulea, A.; Stergiotis, S.; Kaparos, G.; Alexandrou, A.; Eleftheriadis, M.; Georgopoulos, N.; Vlahos, N.; Lambrinoudaki, I. Climacteric symptoms, age, and sense of coherence are associated with sexual function scores in women after menopause. J. Sex. Med. 2023, 20, 313–323. [Google Scholar] [CrossRef]
- Fritz, M.A.; Speroff, L. Clinical Gynecologic Endocrinology and Infertility, 8th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; p. 684. 1439p. [Google Scholar]
- Rhoades, R.; Bell, D.R. Medical Physiology: Principles for Clinical Medicine, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018; p. xvii. 860p. [Google Scholar]
- Wecker, L.; Taylor, D.A.; Theobald, R.J. Brody’s Human Pharmacology: Molecular to Clinical, 6th ed.; Elsevier, Inc.: Philadelphia, PA, USA, 2019. [Google Scholar]
- Brinton, R.D. Estrogen-induced plasticity from cells to circuits: Predictions for cognitive function. Trends Pharmacol. Sci. 2009, 30, 212–222. [Google Scholar] [CrossRef]
- McEwen, B.S.; Akama, K.T.; Spencer-Segal, J.L.; Milner, T.A.; Waters, E.M. Estrogen effects on the brain: Actions beyond the hypothalamus via novel mechanisms. Behav. Neurosci. 2012, 126, 4–16. [Google Scholar] [CrossRef]
- Nilsson, S.; Koehler, K.F.; Gustafsson, J.A. Development of subtype-selective oestrogen receptor-based therapeutics. Nat. Rev. Drug Discov. 2011, 10, 778–792. [Google Scholar] [CrossRef]
- Mattson, M.P.; Magnus, T. Ageing and neuronal vulnerability. Nat. Rev. Neurosci. 2006, 7, 278–294. [Google Scholar] [CrossRef] [PubMed]
- Rettberg, J.R.; Dang, H.; Hodis, H.N.; Henderson, V.W.; St John, J.A.; Mack, W.J.; Brinton, R.D. Identifying postmenopausal women at risk for cognitive decline within a healthy cohort using a panel of clinical metabolic indicators: Potential for detecting an at-Alzheimer’s risk metabolic phenotype. Neurobiol. Aging 2016, 40, 155–163. [Google Scholar] [CrossRef]
- Yin, F.; Yao, J.; Sancheti, H.; Feng, T.; Melcangi, R.C.; Morgan, T.E.; Finch, C.E.; Pike, C.J.; Mack, W.J.; Cadenas, E.; et al. The perimenopausal aging transition in the female rat brain: Decline in bioenergetic systems and synaptic plasticity. Neurobiol. Aging 2015, 36, 2282–2295. [Google Scholar] [CrossRef]
- Anderson, D.; Yoshizawa, T.; Gollschewski, S.; Atogami, F.; Courtney, M. Menopause in Australia and Japan: Effects of country of residence on menopausal status and menopausal symptoms. Climacteric 2004, 7, 165–174. [Google Scholar] [CrossRef]
- Blumel, J.E.; Chedraui, P.; Baron, G.; Belzares, E.; Bencosme, A.; Calle, A.; Danckers, L.; Espinoza, M.T.; Flores, D.; Gomez, G.; et al. A large multinational study of vasomotor symptom prevalence, duration, and impact on quality of life in middle-aged women. Menopause 2011, 18, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Dias-da-Costa, J.S.; Olinto, M.T.; Gigante, D.P.; Menezes, A.M.; Macedo, S.; Daltoe, T.; Santos Ida, S.; Fuchs, S.C. Use of outpatient services in Pelotas, Rio Grande do Sul State, Brazil: Factors related to above-average number of physician visits. Cad. Saude Publica 2008, 24, 353–363. [Google Scholar] [CrossRef]
- Politi, M.C.; Schleinitz, M.D.; Col, N.F. Revisiting the duration of vasomotor symptoms of menopause: A meta-analysis. J. Gen. Intern. Med. 2008, 23, 1507–1513. [Google Scholar] [CrossRef]
- Whiteley, J.; Wagner, J.S.; Bushmakin, A.; Kopenhafer, L.; Dibonaventura, M.; Racketa, J. Impact of the severity of vasomotor symptoms on health status, resource use, and productivity. Menopause 2013, 20, 518–524. [Google Scholar] [CrossRef]
- Woods, N.F.; Mitchell, E.S. Symptoms during the perimenopause: Prevalence, severity, trajectory, and significance in women’s lives. Am. J. Med. 2005, 118 (Suppl. 12B), 14–24. [Google Scholar] [CrossRef]
- da Silva, A.A.; de Mello, R.G.; Schaan, C.W.; Fuchs, F.D.; Redline, S.; Fuchs, S.C. Sleep duration and mortality in the elderly: A systematic review with meta-analysis. BMJ Open 2016, 6, e008119. [Google Scholar] [CrossRef]
- Goldman, S.E.; Stone, K.L.; Ancoli-Israel, S.; Blackwell, T.; Ewing, S.K.; Boudreau, R.; Cauley, J.A.; Hall, M.; Matthews, K.A.; Newman, A.B. Poor sleep is associated with poorer physical performance and greater functional limitations in older women. Sleep 2007, 30, 1317–1324. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Zagalaz-Anula, N.; Martinez-Amat, A.; Cruz-Diaz, D.; Sanchez-Montesinos, I.; Aibar-Almazan, A.; Lomas-Vega, R. Sleep quality and its association with postural stability and fear of falling among Spanish postmenopausal women. Menopause 2018, 25, 62–69. [Google Scholar] [CrossRef]
- Mulhall, S.; Andel, R.; Anstey, K.J. Variation in symptoms of depression and anxiety in midlife women by menopausal status. Maturitas 2018, 108, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Naufel, M.F.; Frange, C.; Andersen, M.L.; Girao, M.; Tufik, S.; Beraldi Ribeiro, E.; Hachul, H. Association between obesity and sleep disorders in postmenopausal women. Menopause 2018, 25, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Shaver, J.L.; Woods, N.F. Sleep and menopause: A narrative review. Menopause 2015, 22, 899–915. [Google Scholar] [CrossRef] [PubMed]
- Ding, R.; Ding, P.; Tian, L.; Kuang, X.; Huang, L.; Shi, H. Sleep duration trajectories and all-cause mortality among Chinese elderly: A community-based cohort study. BMC Public Health 2023, 23, 1095. [Google Scholar] [CrossRef] [PubMed]
- Hita-Contreras, F.; Martinez-Amat, A.; Lomas-Vega, R.; Alvarez, P.; Mendoza, N.; Romero-Franco, N.; Aranega, A. Relationship of body mass index and body fat distribution with postural balance and risk of falls in Spanish postmenopausal women. Menopause 2013, 20, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Maltais, M.L.; Desroches, J.; Dionne, I.J. Changes in muscle mass and strength after menopause. J. Musculoskelet. Neuronal Interact. 2009, 9, 186–197. [Google Scholar] [PubMed]
- Yuan, S.; Larsson, S.C. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef]
- Heinemann, K.; Ruebig, A.; Potthoff, P.; Schneider, H.P.; Strelow, F.; Heinemann, L.A.; Do, M.T. The Menopause Rating Scale (MRS) scale: A methodological review. Health Qual. Life Outcomes 2004, 2, 45. [Google Scholar] [CrossRef]
- Heinemann, L.A.; Potthoff, P.; Schneider, H.P. International versions of the Menopause Rating Scale (MRS). Health Qual. Life Outcomes 2003, 1, 28. [Google Scholar] [CrossRef]
- Potthoff, P.; Heinemann, L.A.; Schneider, H.P.; Rosemeier, H.P.; Hauser, G.A. The Menopause Rating Scale (MRS II): Methodological standardization in the German population. Zentralblatt Gynakol. 2000, 122, 280–286. [Google Scholar]
- Csipo, T.; Lipecz, A.; Ashpole, N.M.; Balasubramanian, P.; Tarantini, S. Astrocyte senescence contributes to cognitive decline. Geroscience 2020, 42, 51–55. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Beydoun, H.A.; Gamaldo, A.A.; Teel, A.; Zonderman, A.B.; Wang, Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: Systematic review and meta-analysis. BMC Public Health 2014, 14, 643. [Google Scholar] [CrossRef]
- Salminen, A.; Ojala, J.; Kaarniranta, K.; Haapasalo, A.; Hiltunen, M.; Soininen, H. Astrocytes in the aging brain express characteristics of senescence-associated secretory phenotype. Eur. J. Neurosci. 2011, 34, 3–11. [Google Scholar] [CrossRef]
- Bhat, R.; Crowe, E.P.; Bitto, A.; Moh, M.; Katsetos, C.D.; Garcia, F.U.; Johnson, F.B.; Trojanowski, J.Q.; Sell, C.; Torres, C. Astrocyte senescence as a component of Alzheimer’s disease. PLoS ONE 2012, 7, e45069. [Google Scholar] [CrossRef]
- Godbout, J.P.; Johnson, R.W. Age and neuroinflammation: A lifetime of psychoneuroimmune consequences. Immunol. Allergy Clin. N. Am. 2009, 29, 321–337. [Google Scholar] [CrossRef]
- Pertusa, M.; Garcia-Matas, S.; Rodriguez-Farre, E.; Sanfeliu, C.; Cristofol, R. Astrocytes aged in vitro show a decreased neuroprotective capacity. J. Neurochem. 2007, 101, 794–805. [Google Scholar] [CrossRef]
- Vogel, C.F.A.; Van Winkle, L.S.; Esser, C.; Haarmann-Stemmann, T. The aryl hydrocarbon receptor as a target of environmental stressors—Implications for pollution mediated stress and inflammatory responses. Redox Biol. 2020, 34, 101530. [Google Scholar] [CrossRef]
- Souza, D.G.; Bellaver, B.; Raupp, G.S.; Souza, D.O.; Quincozes-Santos, A. Astrocytes from adult Wistar rats aged in vitro show changes in glial functions. Neurochem. Int. 2015, 90, 93–97. [Google Scholar] [CrossRef]
- Cortese, G.P.; Burger, C. Neuroinflammatory challenges compromise neuronal function in the aging brain: Postoperative cognitive delirium and Alzheimer’s disease. Behav. Brain Res. 2017, 322, 269–279. [Google Scholar] [CrossRef]
- Sala, G.; Nishita, Y.; Tange, C.; Tomida, M.; Gondo, Y.; Shimokata, H.; Otsuka, R. No Appreciable Effect of Education on Aging-Associated Declines in Cognition: A 20-Year Follow-Up Study. Psychol. Sci. 2023, 34, 527–536. [Google Scholar] [CrossRef]
- Chen, Y.; Lv, C.; Li, X.; Zhang, J.; Chen, K.; Liu, Z.; Li, H.; Fan, J.; Qin, T.; Luo, L.; et al. The positive impacts of early-life education on cognition, leisure activity, and brain structure in healthy aging. Aging 2019, 11, 4923–4942. [Google Scholar] [CrossRef] [PubMed]
- Maltais, M.; de Souto Barreto, P.; Bowman, G.L.; Smith, A.D.; Cantet, C.; Andrieu, S.; Rolland, Y. Omega-3 Supplementation for the Prevention of Cognitive Decline in Older Adults: Does It Depend on Homocysteine Levels? J. Nutr. Health Aging 2022, 26, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Scher, C.; Nepomnyaschy, L.; Amano, T. Comparison of Cognitive and Physical Decline as Predictors of Depression Among Older Adults. J. Appl. Gerontol. 2023, 42, 387–398. [Google Scholar] [CrossRef]
- Stephan, B.C.M.; Siervo, M.; Brayne, C. How can population-based studies best be utilized to reduce the global impact of dementia? Recommendations for researchers, funders, and policymakers. Alzheimers Dement. 2020, 16, 1448–1456. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Cagney, K.; Choi, Y. Predictors of cognitive functioning trajectories among older Americans: A new investigation covering 20 years of age- and non-age-related cognitive change. PLoS ONE 2023, 18, e0281139. [Google Scholar] [CrossRef]
- Cassani, R.; Estarellas, M.; San-Martin, R.; Fraga, F.J.; Falk, T.H. Systematic Review on Resting-State EEG for Alzheimer’s Disease Diagnosis and Progression Assessment. Dis. Markers 2018, 2018, 5174815. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Hampel, H.; Feldman, H.H.; Scheltens, P.; Aisen, P.; Andrieu, S.; Bakardjian, H.; Benali, H.; Bertram, L.; Blennow, K.; et al. Preclinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimers Dement. 2016, 12, 292–323. [Google Scholar] [CrossRef]
- Gagliardi, C.; Papa, R.; Postacchini, D.; Giuli, C. Association between Cognitive Status and Physical Activity: Study Profile on Baseline Survey of the My Mind Project. Int. J. Environ. Res. Public Health 2016, 13, 585. [Google Scholar] [CrossRef]
- Henley, D.B.; Dowsett, S.A.; Chen, Y.F.; Liu-Seifert, H.; Grill, J.D.; Doody, R.S.; Aisen, P.; Raman, R.; Miller, D.S.; Hake, A.M.; et al. Alzheimer’s disease progression by geographical region in a clinical trial setting. Alzheimers Res. Ther. 2015, 7, 43. [Google Scholar] [CrossRef]
- Blair, C.K.; Folsom, A.R.; Knopman, D.S.; Bray, M.S.; Mosley, T.H.; Boerwinkle, E.; Investigators, A.S. genotype and cognitive decline in a middle-aged cohort. Neurology 2005, 64, 268–276. [Google Scholar] [CrossRef]
- Anstey, K.J.; von Sanden, C.; Salim, A.; O’Kearney, R. Smoking as a risk factor for dementia and cognitive decline: A meta-analysis of prospective studies. Am. J. Epidemiol. 2007, 166, 367–378. [Google Scholar] [CrossRef]
- Bangen, K.J.; Beiser, A.; Delano-Wood, L.; Nation, D.A.; Lamar, M.; Libon, D.J.; Bondi, M.W.; Seshadri, S.; Wolf, P.A.; Au, R. APOE Genotype Modifies the Relationship between Midlife Vascular Risk Factors and Later Cognitive Decline. J. Stroke Cerebrovasc. 2013, 22, 1361–1369. [Google Scholar] [CrossRef]
- Carmelli, D.; Swan, G.E.; Reed, T.; Miller, B.; Wolf, P.A.; Jarvik, G.P.; Schellenberg, G.D. Midlife cardiovascular risk factors, ApoE, and cognitive decline in elderly male twins. Neurology 1998, 50, 1580–1585. [Google Scholar] [CrossRef]
- Dintica, C.S.; Hoang, T.; Allen, N.; Sidney, S.; Yaffe, K. The Metabolic Syndrome Is Associated With Lower Cognitive Performance and Reduced White Matter Integrity in Midlife: The CARDIA Study. Front. Neurosci. 2022, 16, 942743. [Google Scholar] [CrossRef]
- Emery, C.F.; Finkel, D.; Pedersen, N.L. Pulmonary Function as a Cause of Cognitive Aging. Psychol. Sci. 2012, 23, 1024–1032. [Google Scholar] [CrossRef]
- Finkel, D.; Ernsth-Bravell, M.; Pedersen, N.L. Temporal Dynamics of Motor Functioning and Cognitive Aging. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Allerhand, M.; Deary, I.J.; Team, H.S. Is there a bidirectional relationship between depressive symptoms and cognitive ability in older people? A prospective study using the English Longitudinal Study of Ageing. Psychol. Med. 2012, 42, 2057–2069. [Google Scholar] [CrossRef]
- Knopman, D.S.; Mosley, T.H.; Catellier, D.J.; Coker, L.H.; Atherosclerosis Risk in Communities Study Brain MRI Study. Fourteen-year longitudinal study of vascular risk factors, genotype, and cognition: The ARIC MRI Study. Alzheimers Dement. 2009, 5, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Radler, K.H.; Chapman, S.; Zdrodowska, M.A.; Dowd, H.N.; Liu, X.H.; Huey, E.D.; Cosentino, S.; Louis, E.D. Physical Activity as a Predictor of Cognitive Decline in an Elderly Essential Tremor Cohort: A Prospective, Longitudinal Study. Front. Neurol. 2021, 12, 658527. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Schneider, J.A.; Boyle, P.A.; Arnold, S.E.; Tang, Y.; Bennett, D.A. Chronic distress and incidence of mild cognitive impairment. Neurology 2007, 68, 2085–2092. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Blackwell, T.; Gore, R.; Sands, L.; Reus, V.; Browner, W.S. Depressive symptoms and cognitive decline in nondemented elderly women—A prospective study. Arch. Gen. Psychiatry 1999, 56, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Chuang, I.C.; Liao, W.W.; Wu, C.Y.; Yeh, T.T.; Chen, C.L.; Lin, C.H.; Huang, T.H.; Pei, Y.C. Baseline Global Cognitive Function Affects Cognitive and Functional Outcomes of Combined Physical and Cognitive Training Among Older Adults With Cognitive Decline. Am. J. Occup. Ther. 2022, 76, 7602205140. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Casares, N.; Fuentes, P.G.; Barbancho, M.A.; Lopez-Gigosos, R.; Garcia-Rodriguez, A.; Gutierrez-Bedmar, M. Alzheimer’s Disease, Mild Cognitive Impairment and Mediterranean Diet. A Systematic Review and Dose-Response Meta-Analysis. J. Clin. Med. 2021, 10, 4642. [Google Scholar] [CrossRef]
- Teixeira, C.V.L.; Weiler, M.; Vicentini, J.E.; Junqueira, T.; Cendes, F.; Balthazar, M.L.F. Physical Activity and Hippocampus Volume in Alzheimer Disease, Mild Cognitive Impairment and Normal Cognitive Elderly. Med. Sci. Sports Exerc. 2015, 47, 457–458. [Google Scholar] [CrossRef]
- Koutsonida, M.; Koskeridis, F.; Markozannes, G.; Kanellopoulou, A.; Mousas, A.; Ntotsikas, E.; Ioannidis, P.; Aretouli, E.; Tsilidis, K.K. Metabolic syndrome and cognitive deficits in the Greek cohort of Epirus Health Study. Neurol. Sci. 2023, 44, 3523–3533. [Google Scholar] [CrossRef]
- Koutsonida, M.; Markozannes, G.; Bouras, E.; Aretouli, E.; Tsilidis, K.K. Metabolic syndrome and cognition: A systematic review across cognitive domains and a bibliometric analysis. Front. Psychol. 2022, 13, 981379. [Google Scholar] [CrossRef]
- Pillai, J.A.; Bena, J.; Bekris, L.; Kodur, N.; Kasumov, T.; Leverenz, J.B.; Kashyap, S.R.; Init, A.D.N. Metabolic syndrome biomarkers relate to rate of cognitive decline in MCI and dementia stages of Alzheimer’s disease. Alzheimers Res. Ther. 2023, 15, 54. [Google Scholar] [CrossRef]
- Stirland, L.E.; O’Shea, C.I.; Russ, T.C. Passive smoking as a risk factor for dementia and cognitive impairment: Systematic review of observational studies. Int. Psychogeriatr. 2018, 30, 1177–1187. [Google Scholar] [CrossRef]
- Tzimourta, K.D.; Christou, V.; Tzallas, A.T.; Giannakeas, N.; Astrakas, L.G.; Angelidis, P.; Tsalikakis, D.; Tsipouras, M.G. Machine Learning Algorithms and Statistical Approaches for Alzheimer’s Disease Analysis Based on Resting-State EEG Recordings: A Systematic Review. Int. J. Neural Syst. 2021, 31, 2130002. [Google Scholar] [CrossRef]
- Lewis, E.D.; Apostol, M.; Langston, J.; Parker, A.; Evans, M. A Multi-Center, Open-Label Exploratory Study to Assess Cognitive Function Response to Lifestyle Changes Plus Supplementation in Healthy Adults with Risk Factors Associated with Cognitive Decline. Appl. Sci. 2023, 13, 2818. [Google Scholar] [CrossRef]
- Wimo, A.; Seeher, K.; Cataldi, R.; Cyhlarova, E.; Dielemann, J.L.; Frisell, O.; Guerchet, M.; Jönsson, L.; Malaha, A.K.; Nichols, E.; et al. The worldwide costs of dementia in 2019. Alzheimers Dement. 2023, 19, 2865–2873. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.; Chin, S.; Sedai, A.K. The welfare cost of late-life depression. J. Econ. Behav. Organ. 2022, 204, 15–36. [Google Scholar] [CrossRef]
- Yuan, J.; Wang, Y.; Liu, Z.J. Temporal relationship between depression and cognitive decline in the elderly: A two-wave cross-lagged study in a Chinese sample. Aging Ment. Health 2023, 27, 2179–2186. [Google Scholar] [CrossRef]
- Hwang, I.C.; Ahn, H.Y. The effect of depression on cognitive decline among Korean retirees. J. Res. Med. Sci. 2023, 28, 33. [Google Scholar] [CrossRef]
- Soares, B.; Kanevsky, G.; Teng, C.T.; Pérez-Esparza, R.; Bonetto, G.G.; Lacerda, A.L.T.; Uribe, E.S.; Cordoba, R.; Lupo, C.; Samora, A.M.; et al. Prevalence and Impact of Treatment-Resistant Depression in Latin America: A Prospective, Observational Study. Psychiatr. Q. 2021, 92, 1797–1815. [Google Scholar] [CrossRef] [PubMed]
- Evans-Lacko, S.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Benjet, C.; Bruffaerts, R.; Chiu, W.T.; Florescu, S.; de Girolamo, G.; Gureje, O.; et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO World Mental Health (WMH) surveys. Psychol. Med. 2018, 48, 1560–1571. [Google Scholar] [CrossRef] [PubMed]
- Sampath, D.; Sathyanesan, M.; Newton, S.S. Cognitive dysfunction in major depression and Alzheimer’s disease is associated with hippocampal-prefrontal cortex dysconnectivity. Neuropsychiatr. Dis. Treat. 2017, 13, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, C.G.; Jackowski, A.; Salas, R.; Gupta, S.; Sato, J.R.; Mao, X.; Coplan, J.D.; Shungu, D.C.; Mathew, S.J. The Nucleus Accumbens and Ketamine Treatment in Major Depressive Disorder. Neuropsychopharmacology 2017, 42, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, G.M.; Zhang, J.; Thomas, M.; Banasr, M.; Ma, X.; Pittman, B.; Bristow, L.; Schaeffer, E.; Duman, R.S.; Rothman, D.L.; et al. Transiently increased glutamate cycling in rat PFC is associated with rapid onset of antidepressant-like effects. Mol. Psychiatry 2017, 22, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, R.M.A. History and evolution of the monoamine hypothesis of depression. J. Clin. Psychiatry 2000, 61, 4–6. [Google Scholar] [PubMed]
- Kupfer, D.J.; Frank, E.; Phillips, M.L. Major Depressive Disorder: New Clinical, Neurobiological, and Treatment Perspectives. Focus 2016, 14, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Lener, M.S.; Niciu, M.J.; Ballard, E.D.; Park, M.; Park, L.T.; Nugent, A.C.; Zarate, C.A., Jr. Glutamate and Gamma-Aminobutyric Acid Systems in the Pathophysiology of Major Depression and Antidepressant Response to Ketamine. Biol. Psychiatry 2017, 81, 886–897. [Google Scholar] [CrossRef]
- Lin, Y.F.; Chen, C.A.; Hsu, F.Y.; Hsiao, Y.H. Elevated Hippocampal CRMP5 Mediates Chronic Stress-Induced Cognitive Deficits by Disrupting Synaptic Plasticity, Hindering AMPAR Trafficking, and Triggering Cytokine Release. Int. J. Mol. Sci. 2023, 24, 4898. [Google Scholar] [CrossRef]
- Lopez-Munoz, F.; D’Ocon, P.; Romero, A.; Guerra, J.A.; Alamo, C. Role of serendipity in the discovery of classical antidepressant drugs: Applying operational criteria and patterns of discovery. World J. Psychiatry 2022, 12, 588–602. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, B.; Adams, B.; Verma, A.; Daly, D. Activation of glutamatergic neurotransmission by ketamine: A novel step in the pathway from NMDA receptor blockade to dopaminergic and cognitive disruptions associated with the prefrontal cortex. J. Neurosci. 1997, 17, 2921–2927. [Google Scholar] [CrossRef] [PubMed]
- Perez-Esparza, R. Ketamine for Treatment-Resistant Depression: A New Advocate. Rev. Investig. Clin. 2018, 70, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Esparza, R.; Kobayashi-Romero, L.F.; García-Mendoza, A.M.; Lamas-Aguilar, R.M.; Fonseca-Perezamador, A. Promises and concerns regarding the use of ketamine and esketamine in the treatment of depression. Acta Psychiatr. Scand. 2019, 140, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Ritter, C.; Buchmann, A.; Muller, S.T.; Volleberg, M.; Haynes, M.; Ghisleni, C.; Noeske, R.; Tuura, R.; Hasler, G. Evaluation of Prefrontal gamma-Aminobutyric Acid and Glutamate Levels in Individuals with Major Depressive Disorder Using Proton Magnetic Resonance Spectroscopy. JAMA Psychiatry 2022, 79, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Sanacora, G.; Banasr, M. From pathophysiology to novel antidepressant drugs: Glial contributions to the pathology and treatment of mood disorders. Biol. Psychiatry 2013, 73, 1172–1179. [Google Scholar] [CrossRef]
- Yuen, E.Y.; Liu, W.; Karatsoreos, I.N.; Ren, Y.; Feng, J.; McEwen, B.S.; Yan, Z. Mechanisms for acute stress-induced enhancement of glutamatergic transmission and working memory. Mol. Psychiatry 2011, 16, 156–170. [Google Scholar] [CrossRef]
- Giacometti, L.L.; Barker, J.M. Sex differences in the glutamate system: Implications for addiction. Neurosci. Biobehav. Rev. 2020, 113, 157–168. [Google Scholar] [CrossRef]
- Torrisi, S.A.; Rizzo, S.; Laudani, S.; Ieraci, A.; Drago, F.; Leggio, G.M. Acute stress alters recognition memory and AMPA/NMDA receptor subunits in a sex-dependent manner. Neurobiol. Stress 2023, 25, 100545. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Akil, H. Revisiting the Stress Concept: Implications for Affective Disorders. J. Neurosci. 2020, 40, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Eid, R.S.; Gobinath, A.R.; Galea, L.A.M. Sex differences in depression: Insights from clinical and preclinical studies. Prog. Neurobiol. 2019, 176, 86–102. [Google Scholar] [CrossRef]
- Labaka, A.; Goni-Balentziaga, O.; Lebena, A.; Perez-Tejada, J. Biological Sex Differences in Depression: A Systematic Review. Biol. Res. Nurs. 2018, 20, 383–392. [Google Scholar] [CrossRef]
- Jett, S.; Dyke, J.P.; Boneu Yepez, C.; Zarate, C.; Carlton, C.; Schelbaum, E.; Jang, G.; Pahlajani, S.; Williams, S.; Diaz Brinton, R.; et al. Effects of sex and APOE epsilon4 genotype on brain mitochondrial high-energy phosphates in midlife individuals at risk for Alzheimer’s disease: A 31Phosphorus MR spectroscopy study. PLoS ONE 2023, 18, e0281302. [Google Scholar] [CrossRef] [PubMed]
- Sauty, B.; Durrleman, S. Impact of sex and APOE-epsilon4 genotype on patterns of regional brain atrophy in Alzheimer’s disease and healthy aging. Front. Neurol. 2023, 14, 1161527. [Google Scholar] [CrossRef]
- Dawkins, E.; Small, D.H. Insights into the physiological function of the beta-amyloid precursor protein: Beyond Alzheimer’s disease. J. Neurochem. 2014, 129, 756–769. [Google Scholar] [CrossRef]
- Heneka, M.T.; Kummer, M.P.; Stutz, A.; Delekate, A.; Schwartz, S.; Vieira-Saecker, A.; Griep, A.; Axt, D.; Remus, A.; Tzeng, T.C.; et al. NLRP3 is activated in Alzheimer’s disease and contributes to pathology in APP/PS1 mice. Nature 2013, 493, 674–678. [Google Scholar] [CrossRef]
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chetelat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat. Rev. Dis. Primers 2021, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Ma, Q.; Zhang, Y.W.; Xu, H. Proteolytic processing of Alzheimer’s beta-amyloid precursor protein. J. Neurochem. 2012, 120 (Suppl. 1), 9–21. [Google Scholar] [CrossRef] [PubMed]
- Jang, C.; Choi, J.K.; Na, Y.J.; Jang, B.; Wasco, W.; Buxbaum, J.D.; Kim, Y.S.; Choi, E.K. Calsenilin regulates presenilin 1/gamma-secretase-mediated N-cadherin epsilon-cleavage and beta-catenin signaling. FASEB J. 2011, 25, 4174–4183. [Google Scholar] [CrossRef]
- Jin, J.K.; Choi, J.K.; Wasco, W.; Buxbaum, J.D.; Kozlowski, P.B.; Carp, R.I.; Kim, Y.S.; Choi, E.K. Expression of calsenilin in neurons and astrocytes in the Alzheimer’s disease brain. Neuroreport 2005, 16, 451–455. [Google Scholar] [CrossRef]
- Rivas, M.; Villar, D.; González, P.; Dopazo, X.M.; Mellstrom, B.; Naranjo, J.R. Building the DREAM interactome. Sci. China Life Sci. 2011, 54, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Lusin, J.D.; Vanarotti, M.; Dace, A.; Li, C.M.; Valiveti, A.; Ames, J.B. NMR structure of DREAM: Implications for Ca -dependent DNA binding and protein dimerization. Biochemistry 2008, 47, 2252–2264. [Google Scholar] [CrossRef] [PubMed]
- Spreafico, F.; Barski, J.J.; Farina, C.; Meyer, M. Mouse DREAM/Calsenilin/KChIP3: Gene structure, coding potential, and expression. Mol. Cell Neurosci. 2001, 17, 1–16. [Google Scholar] [CrossRef]
- Misiura, M.B.; Butts, B.; Hammerschlag, B.; Munkombwe, C.; Bird, A.; Fyffe, M.; Hemphill, A.; Dotson, V.M.; Wharton, W. Intersectionality in Alzheimer’s Disease: The Role of Female Sex and Black American Race in the Development and Prevalence of Alzheimer’s Disease. Neurotherapeutics 2023, 20, 1019–1036. [Google Scholar] [CrossRef]
- Sundermann, E.E.; Tran, M.; Maki, P.M.; Bondi, M.W. Sex differences in the association between apolipoprotein E epsilon4 allele and Alzheimer’s disease markers. Alzheimers Dement. 2018, 10, 438–447. [Google Scholar] [CrossRef]
- Arnold, M.; Nho, K.; Kueider-Paisley, A.; Massaro, T.; Huynh, K.; Brauner, B.; MahmoudianDehkordi, S.; Louie, G.; Moseley, M.A.; Thompson, J.W.; et al. Sex and APOE epsilon4 genotype modify the Alzheimer’s disease serum metabolome. Nat. Commun. 2020, 11, 1148. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Boueiz, A.; Abougergi, M.S.; Kitner-Triolo, M.H.; Beydoun, H.A.; Resnick, S.M.; O’Brien, R.; Zonderman, A.B. Sex differences in the association of the apolipoprotein E epsilon 4 allele with incidence of dementia, cognitive impairment, and decline. Neurobiol. Aging 2012, 33, 720–731.e4. [Google Scholar] [CrossRef]
- Gamache, J.; Yun, Y.; Chiba-Falek, O. Sex-dependent effect of APOE on Alzheimer’s disease and other age-related neurodegenerative disorders. Dis. Model. Mech. 2020, 13, dmm045211. [Google Scholar] [CrossRef]
- Hou, X.; Adeosun, S.O.; Zhang, Q.; Barlow, B.; Brents, M.; Zheng, B.; Wang, J. Differential contributions of ApoE4 and female sex to BACE1 activity and expression mediate Abeta deposition and learning and memory in mouse models of Alzheimer’s disease. Front. Aging Neurosci. 2015, 7, 207. [Google Scholar] [CrossRef]
- Neu, S.C.; Pa, J.; Kukull, W.; Beekly, D.; Kuzma, A.; Gangadharan, P.; Wang, L.S.; Romero, K.; Arneric, S.P.; Redolfi, A.; et al. Apolipoprotein E Genotype and Sex Risk Factors for Alzheimer Disease: A Meta-analysis. JAMA Neurol. 2017, 74, 1178–1189. [Google Scholar] [CrossRef] [PubMed]
- Riedel, B.C.; Thompson, P.M.; Brinton, R.D. Age, APOE and sex: Triad of risk of Alzheimer’s disease. J. Steroid Biochem. Mol. Biol. 2016, 160, 134–147. [Google Scholar] [CrossRef]
- Shinohara, M.; Murray, M.E.; Frank, R.D.; Shinohara, M.; DeTure, M.; Yamazaki, Y.; Tachibana, M.; Atagi, Y.; Davis, M.D.; Liu, C.C.; et al. Impact of sex and APOE4 on cerebral amyloid angiopathy in Alzheimer’s disease. Acta Neuropathol. 2016, 132, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Tensil, M.; Hessler, J.B.; Gutsmiedl, M.; Riedl, L.; Grimmer, T.; Diehl-Schmid, J. Sex Differences in Neuropsychological Test Performance in Alzheimer’s Disease and the Influence of the ApoE Genotype. Alzheimer Dis. Assoc. Disord. 2018, 32, 145–149. [Google Scholar] [CrossRef]
- Toro, C.A.; Zhang, L.; Cao, J.; Cai, D. Sex differences in Alzheimer’s disease: Understanding the molecular impact. Brain Res. 2019, 1719, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Vermunt, L.; Sikkes, S.A.M.; van den Hout, A.; Handels, R.; Bos, I.; van der Flier, W.M.; Kern, S.; Ousset, P.J.; Maruff, P.; Skoog, I.; et al. Duration of preclinical, prodromal, and dementia stages of Alzheimer’s disease in relation to age, sex, and APOE genotype. Alzheimers Dement. 2019, 15, 888–898. [Google Scholar] [CrossRef]
- Zhao, N.; Ren, Y.; Yamazaki, Y.; Qiao, W.; Li, F.; Felton, L.M.; Mahmoudiandehkordi, S.; Kueider-Paisley, A.; Sonoustoun, B.; Arnold, M.; et al. Alzheimer’s Risk Factors Age, APOE Genotype, and Sex Drive Distinct Molecular Pathways. Neuron 2020, 106, 727–742.e726. [Google Scholar] [CrossRef]
- Puertas, M.C.; Martinez-Martos, J.M.; Cobo, M.P.; Carrera, M.P.; Mayas, M.D.; Ramirez-Exposito, M.J. Plasma oxidative stress parameters in men and women with early stage Alzheimer type dementia. Exp. Gerontol. 2012, 47, 625–630. [Google Scholar] [CrossRef]
- Ayaz, M.; Mosa, O.F.; Nawaz, A.; Hamdoon, A.A.E.; Elkhalifa, M.E.M.; Sadiq, A.; Ullah, F.; Ahmed, A.; Kabra, A.; Khan, H.; et al. Neuroprotective potentials of Lead phytochemicals against Alzheimer’s disease with focus on oxidative stress-mediated signaling pathways: Pharmacokinetic challenges, target specificity, clinical trials and future perspectives. Phytomedicine 2024, 124, 155272. [Google Scholar] [CrossRef]
- Barth, C.; Crestol, A.; de Lange, A.G.; Galea, L.A.M. Sex steroids and the female brain across the lifespan: Insights into risk of depression and Alzheimer’s disease. Lancet Diabetes Endocrinol. 2023, 11, 926–941. [Google Scholar] [CrossRef]
- Guo, T.; Zhang, D.; Zeng, Y.; Huang, T.Y.; Xu, H.; Zhao, Y. Molecular and cellular mechanisms underlying the pathogenesis of Alzheimer’s disease. Mol. Neurodegener. 2020, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, A.; Carroll, J.C.; Morgan, T.E.; Lin, S.; Zhao, L.; Arimoto, J.M.; Murphy, M.P.; Beckett, T.L.; Finch, C.E.; Brinton, R.D.; et al. 17beta-estradiol and progesterone regulate expression of beta-amyloid clearance factors in primary neuron cultures and female rat brain. Endocrinology 2012, 153, 5467–5479. [Google Scholar] [CrossRef]
- Pike, C.J. Sex and the development of Alzheimer’s disease. J. Neurosci. Res. 2017, 95, 671–680. [Google Scholar] [CrossRef]
- Poling, M.C.; Kauffman, A.S. Organizational and activational effects of sex steroids on kisspeptin neuron development. Front. Neuroendocrinol. 2013, 34, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Rosario, E.R.; Pike, C.J. Androgen regulation of beta-amyloid protein and the risk of Alzheimer’s disease. Brain Res. Rev. 2008, 57, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Tublin, J.M.; Adelstein, J.M.; Del Monte, F.; Combs, C.K.; Wold, L.E. Getting to the Heart of Alzheimer Disease. Circ. Res. 2019, 124, 142–149. [Google Scholar] [CrossRef]
- Carrera-González, M.P.; Ramírez-Expósito, M.J.; Guerrero-González, C.; Martínez-Martos, J.M. Alzheimer’s disease: Is there a relationship between brain renin-angiotensin system, estradiol and glucose transporter-4 (GLUT-4)? AIMS Mol. Sci. 2023, 10, 37–51. [Google Scholar] [CrossRef]
- Puertas Mdel, C.; Martinez-Martos, J.M.; Cobo, M.; Lorite, P.; Sandalio, R.M.; Palomeque, T.; Torres, M.I.; Carrera-Gonzalez, M.P.; Mayas, M.D.; Ramirez-Exposito, M.J. Plasma renin-angiotensin system-regulating aminopeptidase activities are modified in early stage Alzheimer’s disease and show gender differences but are not related to apolipoprotein E genotype. Exp. Gerontol. 2013, 48, 557–564. [Google Scholar] [CrossRef]
- Perez-Lopez, F.R.; Martinez-Dominguez, S.J.; Lajusticia, H.; Chedraui, P.; Health Outcomes Systematic Analyses, P. Effects of programmed exercise on depressive symptoms in midlife and older women: A meta-analysis of randomized controlled trials. Maturitas 2017, 106, 38–47. [Google Scholar] [CrossRef]
- Ravindran, A.V.; Balneaves, L.G.; Faulkner, G.; Ortiz, A.; McIntosh, D.; Morehouse, R.L.; Ravindran, L.; Yatham, L.N.; Kennedy, S.H.; Lam, R.W.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 5. Complementary and Alternative Medicine Treatments. Focus 2018, 16, 85–94. [Google Scholar] [CrossRef]
- Byrnes, K.; Wu, P.J.; Whillier, S. Is Pilates an effective rehabilitation tool? A systematic review. J. Bodyw. Mov. Ther. 2018, 22, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Chen, C. Research on exercise fatigue estimation method of Pilates rehabilitation based on ECG and sEMG feature fusion. BMC Med. Inform. Decis. Mak. 2022, 22, 67. [Google Scholar] [CrossRef]
- Pinheiro, É.P.; do Espirito Santo, R.C.; Dos Santos, L.P.; Goncalves, W.V.; Júnior, L.A.F.; Xavier, R.M.; Filippin, L.I. Multicomponent or Resistance Training for Nursing Home Residents: A Systematic Review with Meta-Analysis. J. Am. Med. Dir. Assoc. 2022, 23, 1926.e1–1926.e10. [Google Scholar] [CrossRef]
- Li, L.; Liu, M.; Zeng, H.; Pan, L. Multi-component exercise training improves the physical and cognitive function of the elderly with mild cognitive impairment: A six-month randomized controlled trial. Ann. Palliat. Med. 2021, 10, 8919–8929. [Google Scholar] [CrossRef]
- Herold, F.; Torpel, A.; Schega, L.; Muller, N.G. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements—A systematic review. Eur. Rev. Aging Phys. Act. 2019, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Zhao, X.; Li, B.; Cai, Y.; Zhang, S.; Wan, Q.; Yu, F. Comparative efficacy of various exercise interventions on cognitive function in patients with mild cognitive impairment or dementia: A systematic review and network meta-analysis. J. Sports Health Sci. 2022, 11, 212–223. [Google Scholar] [CrossRef]
- Etgen, T.; Sander, D.; Bickel, H.; Forstl, H. Mild cognitive impairment and dementia: The importance of modifiable risk factors. Dtsch. Arztebl. Int. 2011, 108, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol. Med. 2009, 39, 3–11. [Google Scholar] [CrossRef]
- Kirshner, D.; Spiegelhalder, K.; Shahar, R.T.; Shochat, T.; Agmon, M. The association between objective measurements of sleep quality and postural control in adults: A systematic review. Sleep Med. Rev. 2022, 63, 101633. [Google Scholar] [CrossRef]
- Bergamin, M.; Gobbo, S.; Bullo, V.; Zanotto, T.; Vendramin, B.; Duregon, F.; Cugusi, L.; Camozzi, V.; Zaccaria, M.; Neunhaeuserer, D.; et al. Effects of a Pilates exercise program on muscle strength, postural control and body composition: Results from a pilot study in a group of post-menopausal women. Age 2015, 37, 118. [Google Scholar] [CrossRef]
- Di Lorenzo, C.E. Pilates: What is it? Should it be used in rehabilitation? Sports Health 2011, 3, 352–361. [Google Scholar] [CrossRef]
- Ben-Zeev, T.; Hirsh, T.; Weiss, I.; Gornstein, M.; Okun, E. The Effects of High-intensity Functional Training (HIFT) on Spatial Learning, Visual Pattern Separation and Attention Span in Adolescents. Front. Behav. Neurosci. 2020, 14, 577390. [Google Scholar] [CrossRef]
- Ben-Zeev, T.; Okun, E. High-Intensity Functional Training: Molecular Mechanisms and Benefits. Neuromol. Med. 2021, 23, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Buckley, S.; Knapp, K.; Lackie, A.; Lewry, C.; Horvey, K.; Benko, C.; Trinh, J.; Butcher, S. Multimodal high-intensity interval training increases muscle function and metabolic performance in females. Appl. Physiol. Nutr. Metab. 2015, 40, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Heinrich, K.M.; Butcher, S.J.; Poston, W.S.C. High-Intensity Functional Training (HIFT): Definition and Research Implications for Improved Fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef]
- Fisher, J.; Sales, A.; Carlson, L.; Steele, J. A comparison of the motivational factors between CrossFit participants and other resistance exercise modalities: A pilot study. J. Sports Med. Phys. Fitness 2017, 57, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; Macdonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14, 789. [Google Scholar] [CrossRef]
- Jimenez-Garcia, J.D.; Martinez-Amat, A.; De la Torre-Cruz, M.J.; Fabrega-Cuadros, R.; Cruz-Diaz, D.; Aibar-Almazan, A.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Suspension Training HIIT Improves Gait Speed, Strength and Quality of Life in Older Adults. Int. J. Sports Med. 2019, 40, 116–124. [Google Scholar] [CrossRef]
- Kliszczewicz, B.; Williamson, C.; Bechke, E.; McKenzie, M.; Hoffstetter, W. Autonomic response to a short and long bout of high-intensity functional training. J. Sports Sci. 2018, 36, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Quiles, J.M.; Klemp, A.; Dolan, C.; Maharaj, A.; Huang, C.J.; Khamoui, A.V.; Trexler, E.T.; Whitehurst, M.; Zourdos, M.C. Impact of resistance training program configuration on the circulating brain-derived neurotrophic factor response. Appl. Physiol. Nutr. Metab. 2020, 45, 667–674. [Google Scholar] [CrossRef]
- Wilke, J. Functional high-intensity exercise is more effective in acutely increasing working memory than aerobic walking: An exploratory randomized, controlled trial. Sci. Rep. 2020, 10, 12335. [Google Scholar] [CrossRef] [PubMed]
- Hita-Contreras, F.; Martinez-Amat, A.; Cruz-Diaz, D.; Perez-Lopez, F.R. Fall prevention in postmenopausal women: The role of Pilates exercise training. Climacteric 2016, 19, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Fisher, K.J.; McAuley, E.; Chaumeton, N.; Eckstrom, E.; Wilson, N.L. Tai Chi and fall reductions in older adults: A randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C.; American College of Sports, M.; American Heart, A. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef]
- de Oliveira, R.D.J.; de Oliveira, R.G.; de Oliveira, L.C.; Santos-Filho, S.D.; Sa-Caputo, D.C.; Bernardo-Filho, M. Effectiveness of whole-body vibration on bone mineral density in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Osteoporos. Int. 2023, 34, 29–52. [Google Scholar] [CrossRef]
- Figueroa, A.; Kalfon, R.; Madzima, T.A.; Wong, A. Whole-body vibration exercise training reduces arterial stiffness in postmenopausal women with prehypertension and hypertension. Menopause 2014, 21, 131–136. [Google Scholar] [CrossRef]
- Guedes De Aguiar, E.O.; Moreira Marconi, E.; Monteiro-Oliveira, B.B.; Gomes-Santos, A.C.; Coelho Oliveira, A.C.; Paineiras-Domingos, L.L.; Sa-Caputo, D.C.; Bernardo Filho, M. Whole-Body Vibration Exercise Improves the Functionality in Postmenopausal Women: A Systematic Review. Iran. J. Public Health 2023, 52, 476–487. [Google Scholar] [CrossRef]
- Marin-Cascales, E.; Alcaraz, P.E.; Ramos-Campo, D.J.; Martinez-Rodriguez, A.; Chung, L.H.; Rubio-Arias, J.A. Whole-body vibration training and bone health in postmenopausal women: A systematic review and meta-analysis. Medicine 2018, 97, e11918. [Google Scholar] [CrossRef]
- Matsubara, T.; Miyaki, A.; Akazawa, N.; Choi, Y.; Ra, S.G.; Tanahashi, K.; Kumagai, H.; Oikawa, S.; Maeda, S. Aerobic exercise training increases plasma Klotho levels and reduces arterial stiffness in postmenopausal women. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H348–H355. [Google Scholar] [CrossRef] [PubMed]
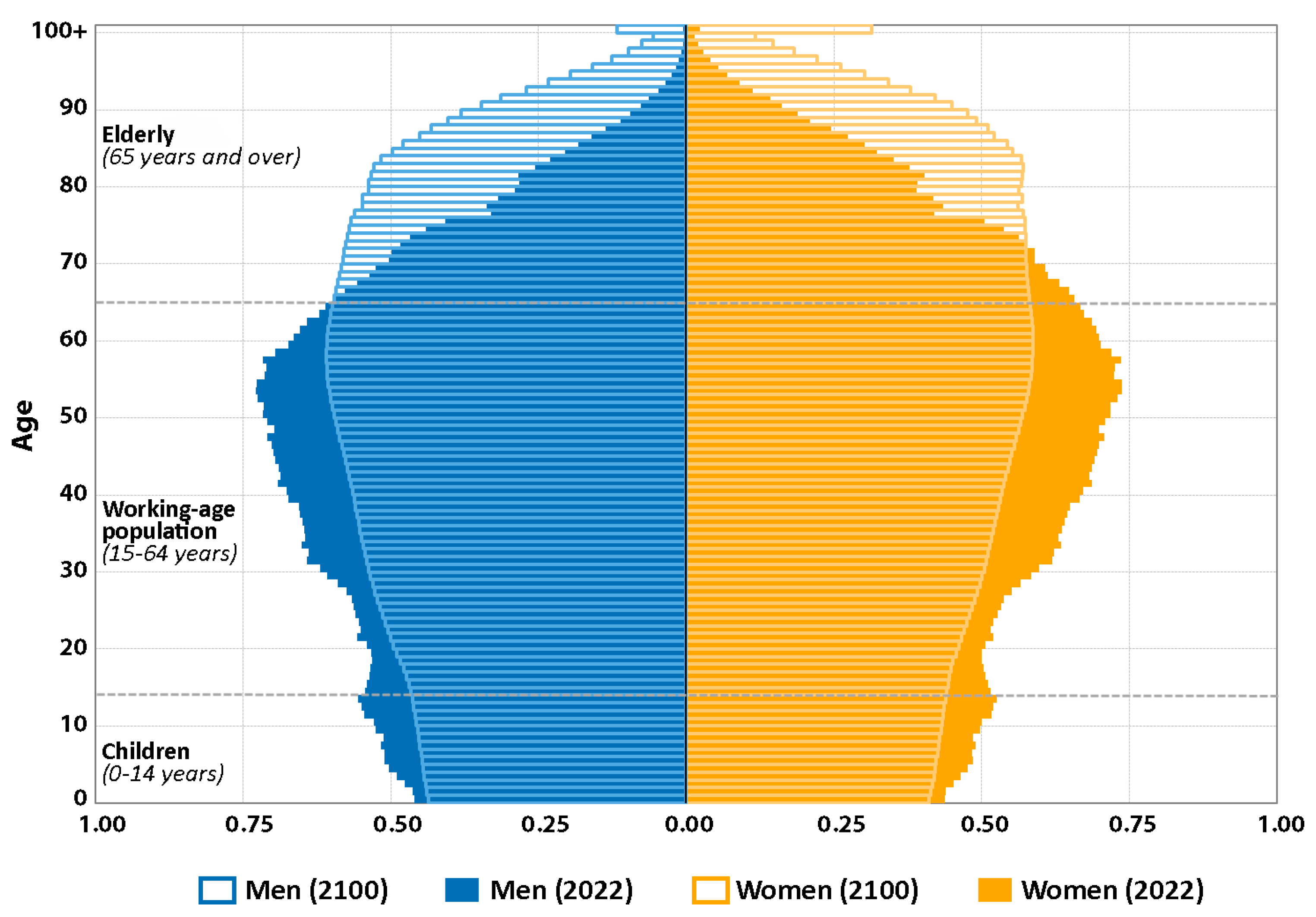
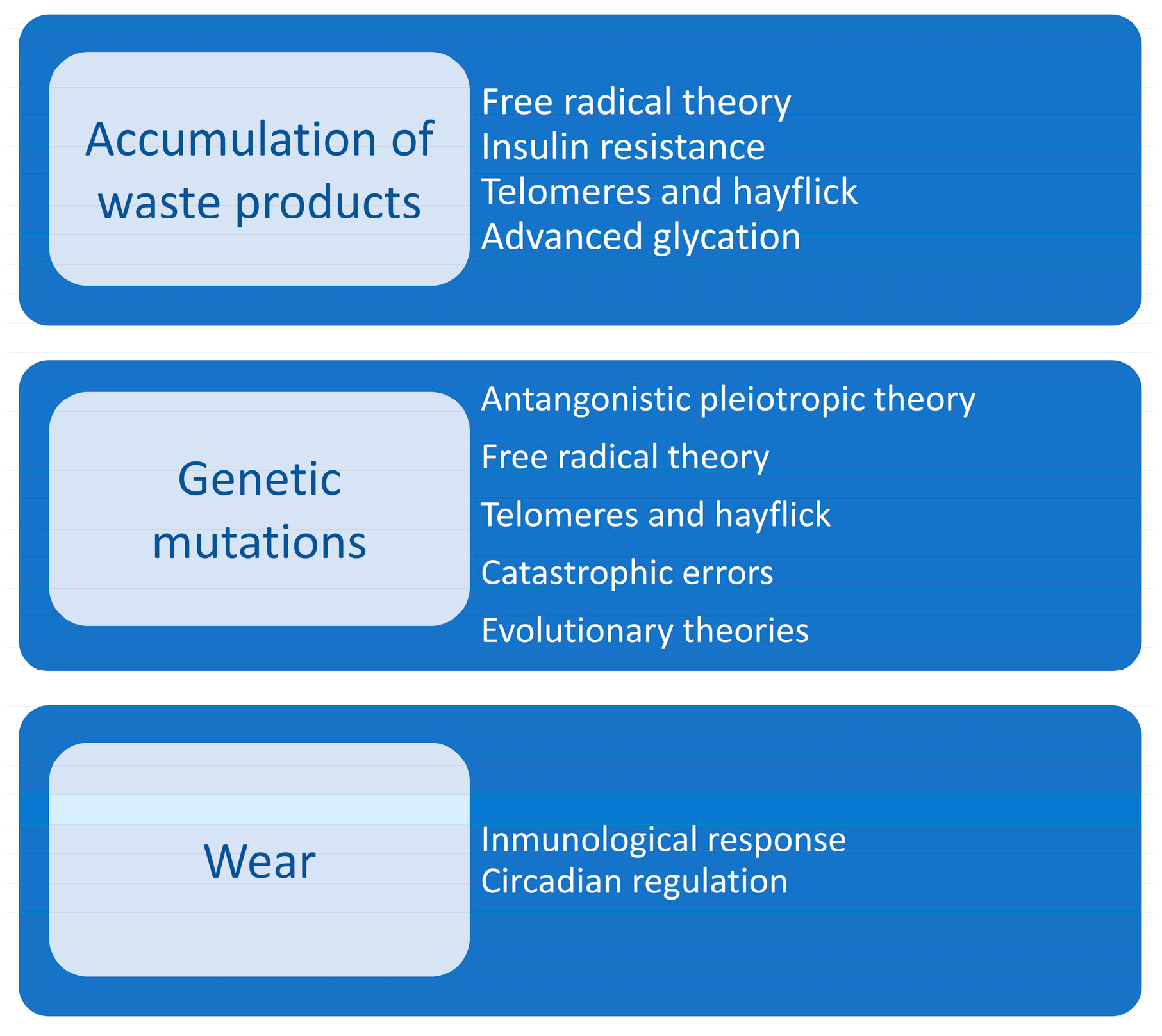
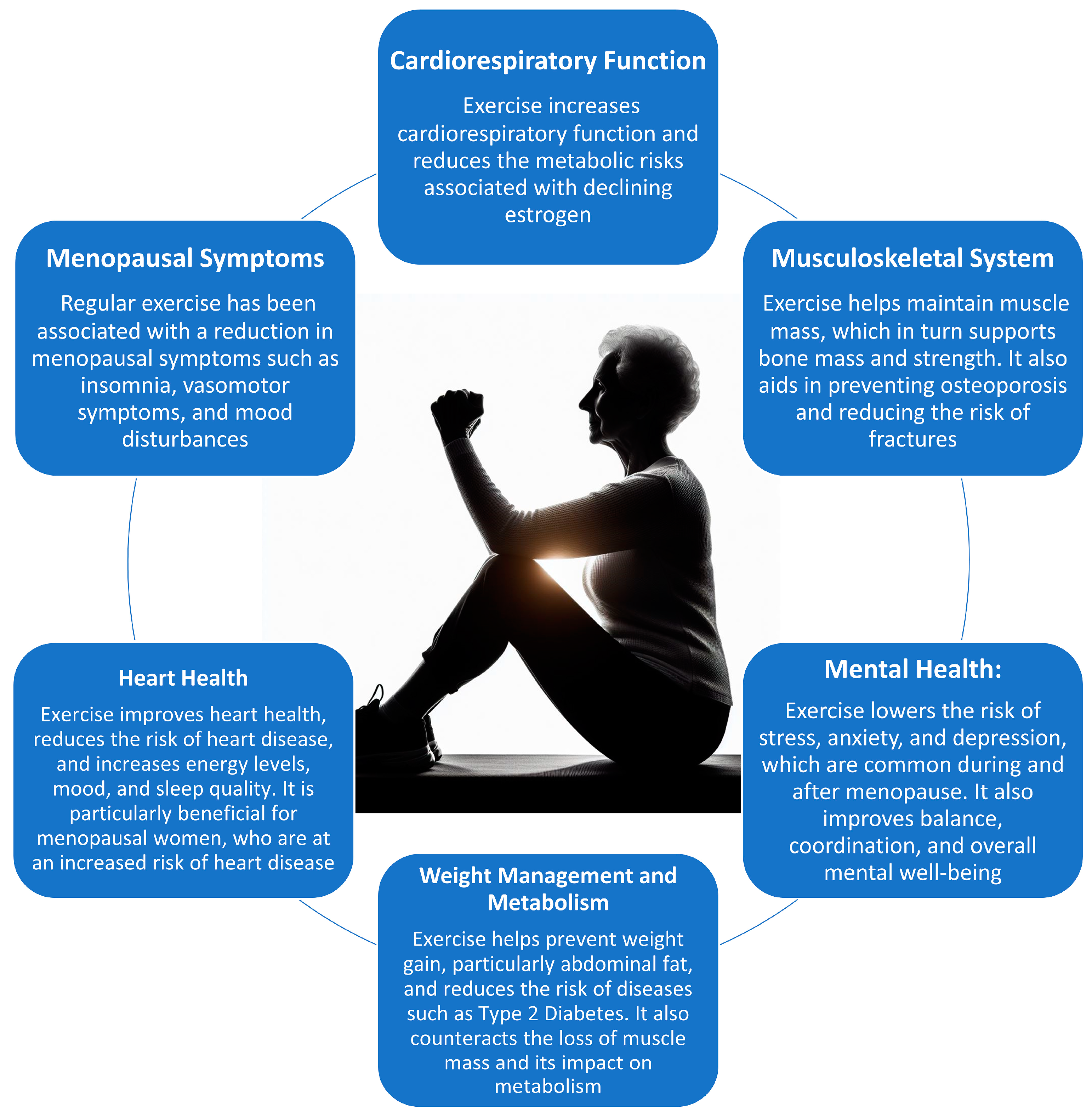
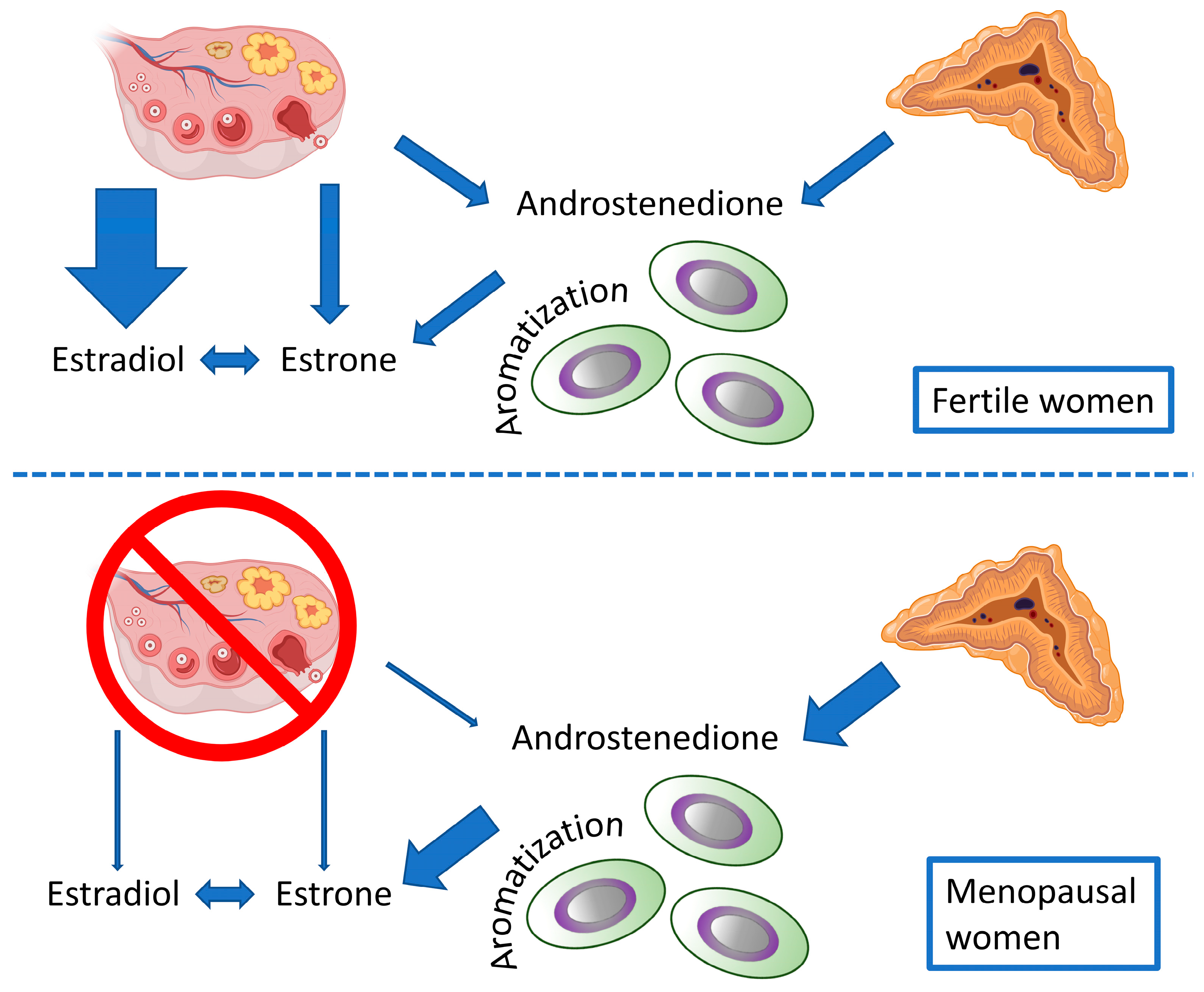
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).