
Validation of the Modified Japanese 7C Readiness Scale for Parental Intentions of Child COVID-19 Vaccination

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Respondents and Data Collection
2.2. Measurement Methods (Baseline Survey)
2.3. Follow-Up Survey
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Parental Attributes and Intention Regarding Vaccinating Their Children Against COVID-19
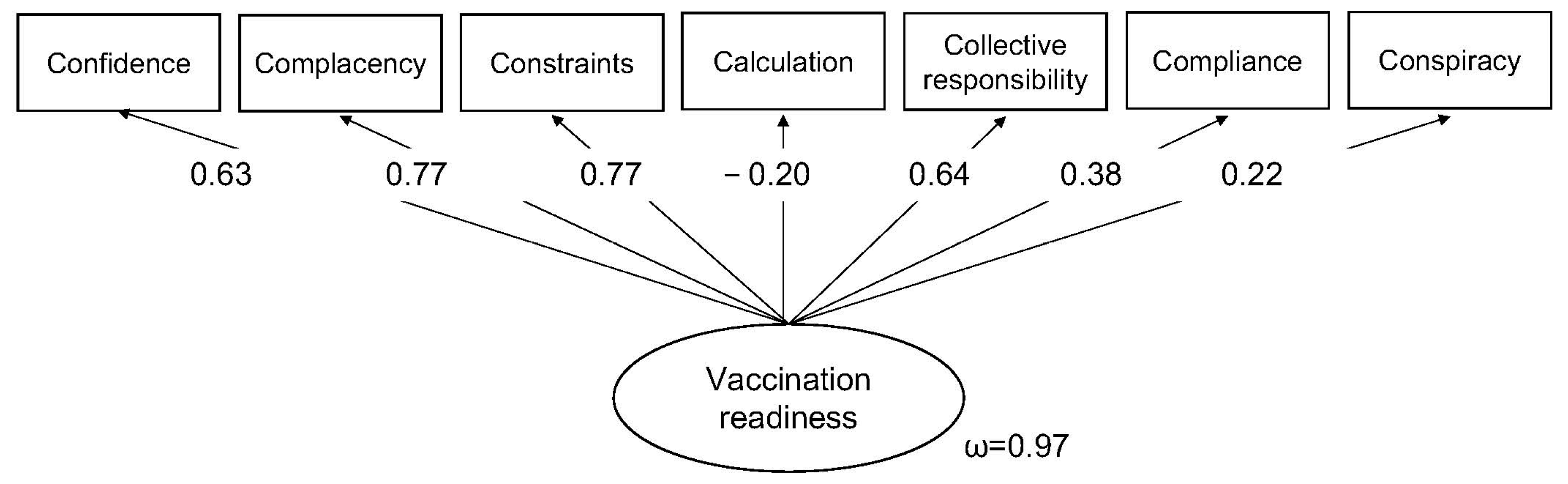
3.2. Measurement Model and Criterion Validity for Parental Readiness to Vaccinate Their Children Against COVID-19
3.3. Predictors of Parental Intention to Vaccinate Their Children Against COVID-19
3.4. Relationship Between Components of the Modified Scale and Parental Intention to Vaccinate Their Children Against COVID-19
3.5. Predicted and Observed Vaccination Behavior
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lehmann, B.A.; de Melker, H.E.; Timmermans, D.R.M.; Mollema, L. Informed decision making in the context of childhood immunization. Patient Educ. Couns. 2017, 100, 2339–2345. [Google Scholar] [CrossRef] [PubMed]
- Duclos, P.; Okwo-Bele, J.M.; Gacic-Dobo, M.; Cherian, T. Global immunization: Status, progress, challenges and future. BMC Int. Health Hum. Rights 2009, 9 (Suppl. S1), S2. [Google Scholar] [CrossRef] [PubMed]
- World Bank. World Development Report 1993; Oxford University Press: New York, NY, USA, 1993. [Google Scholar]
- Chen, F.; He, Y.; Shi, Y. Parents’ and guardians’ willingness to vaccinate their children against COVID-19: A systematic review and meta-analysis. Vaccines 2022, 10, 179. [Google Scholar] [CrossRef]
- Yang, W. Transmission dynamics of and insights from the 2018-2019 measles outbreak in New York City: A modeling study. Sci. Adv. 2020, 6, eaaz4037. [Google Scholar] [CrossRef] [PubMed]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of vaccination readiness. Eur. J. Psych. Assess. 2021, 38, 261–269. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5c psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5C validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Al-Sanafi, M.; Sallam, M. Psychological determinants of COVID-19 vaccine acceptance among healthcare workers in Kuwait: A cross-sectional study using the 5C and vaccine conspiracy beliefs scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef]
- Gallant, A.J.; Nicholls, L.A.; Rasmussen, B.S.; Cogan, N.; Young, D.; Williams, L. Changes in attitudes to vaccination as a result of the COVID-19 pandemic: A longitudinal study of older adults in the UK. PLoS ONE 2021, 16, e0261844. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Editor’s choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Trends in COVID-19 vaccination intent from pre- to post-COVID-19 vaccine distribution and their associations with the 5C psychological antecedents of vaccination by sex and age in Japan. Hum. Vaccin. Immunother. 2021, 17, 3954–3962. [Google Scholar] [CrossRef]
- Mercadante, A.R.; Law, A.V. Will they, or won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the health belief model. Res. Social. Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef]
- Obohwemu, K.; Christie-de Jong, F.; Ling, J. Parental childhood vaccine hesitancy and predicting uptake of vaccinations: A systematic review. Prim. Health Care Res. Dev. 2022, 23, e68. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Liberatore, F.; Schmelzer, S.; Dratva, J. Confident and altruistic-parents’ motives to vaccinate their children against COVID-19: A cross-sectional online survey in a Swiss vaccination centre. Swiss Med. Wkly. 2022, 152, w30156. [Google Scholar] [CrossRef] [PubMed]
- Wismans, A.; Thurik, R.; Baptista, R.; Dejardin, M.; Janssen, F.; Franken, I. Psychological characteristics and the mediating role of the 5C model in explaining students’ COVID-19 vaccination intention. PLoS ONE 2021, 16, e0255382. [Google Scholar] [CrossRef]
- Cogordan, C.; Fressard, L.; Ramalli, S.; Rebaudet, P.; Malfait, A.; Dutrey-Kaiser, Y.; Attalah, D.; Roy, P.; Berthiaume, A.; Gagneur, A.; et al. Motivational interview-based health mediator interventions increase intent to vaccinate among disadvantaged individuals. Hum. Vaccin. Immunother. 2023, 19, 2261687. [Google Scholar] [CrossRef]
- Teng, Y.; Hanibuchi, T.; Machida, M.; Nakaya, T. Psychological determinants of COVID-19 vaccine acceptance: A comparison between immigrants and the host population in Japan. Vaccine 2023, 41, 1426–1430. [Google Scholar] [CrossRef]
- Williams, L.; Gallant, A.; Brown, L.; Corrigan, K.; Crowe, K.; Hendry, E. Barriers and facilitators to the future uptake of regular COVID-19 booster vaccinations among young adults in the UK. Hum. Vaccin. Immunother. 2022, 18, 2129238. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Shah, M.D.; Delgado, J.R.; Thomas, K.; Vizueta, N.; Cui, Y.; Vangala, S.; Shetgiri, R.; Kapteyn, A. Parents’ intentions and perceptions about COVID-19 vaccination for their children: Results from a national survey. Pediatrics 2021, 148, e2021052335. [Google Scholar] [CrossRef]
- Kezhong, A.; Lu, X.; Wang, J.; Hu, L.; Li, B.; Lu, Y. Association between adult vaccine hesitancy and parental acceptance of childhood COVID-19 vaccines: A web-based survey in a northwestern region in China. Vaccines 2021, 9, 1088. [Google Scholar] [CrossRef] [PubMed]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammed, O.A. Parents’ hesitancy to vaccinate their 5-11-year-old children against COVID-19 in Saudi Arabia: Predictors from the health belief model. Front. Public. Health 2022, 10, 842862. [Google Scholar] [CrossRef]
- Rane, M.S.; Robertson, M.M.; Westmoreland, D.A.; Teasdale, C.A.; Grov, C.; Nash, D. Intention to vaccinate children against COVID-19 among vaccinated and unvaccinated US parents. JAMA Pediatrics 2022, 176, 201–203. [Google Scholar] [CrossRef]
- Eberhardt, C.S.; Siegrist, C.A. Is there a role for childhood vaccination against COVID-19? Pediatr. Allergy Immunol. 2021, 32, 9–16. [Google Scholar] [CrossRef]
- Rees, F.; Geiger, M.; Lilleholt, L.; Zettler, I.; Betsch, C.; Böhm, R.; Wilhelm, O. Measuring parents’ readiness to vaccinate themselves and their children against COVID-19. Vaccine 2022, 40, 3825–3834. [Google Scholar] [CrossRef]
- Swann, O.V.; Holden, K.A.; Turtle, L.; Pollock, L.; Fairfield, C.J.; Drake, T.M.; Seth, S.; Egan, C.; Hardwick, H.E.; Halpin, S.; et al. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: Prospective multicentre observational cohort study. BMJ 2020, 370, m3249. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, S.; Sakamoto, H.; Abe, S.K.; Shinohara, R.; Kushima, M.; Otawa, S.; Yui, H.; Akiyama, Y.; Ooka, T.; Kojima, R.; et al. Factors of parental COVID-19 vaccine hesitancy: A cross-sectional study in Japan. PLoS ONE 2021, 16, e0261121. [Google Scholar] [CrossRef]
- Machida, M.; Kojima, T.; Popiel, H.A.; Geiger, M.; Odagiri, Y.; Inoue, S. Development, validity, and reliability of the Japanese version of the 7C of vaccination readiness scale. Am. J. Infect. Control 2023, 51, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Dyda, A.; King, C.; Dey, A.; Leask, J.; Dunn, A.G. A systematic review of studies that measure parental vaccine attitudes and beliefs in childhood vaccination. BMC Public Health 2020, 20, 1253. [Google Scholar] [CrossRef]
- Opel, D.J.; Mangione-Smith, R.; Taylor, J.A.; Korfiatis, C.; Wiese, C.; Catz, S.; Martin, D.P. Development of a survey to identify vaccine-hesitant parents: The parent attitudes about childhood vaccines survey. Hum. Vaccin. 2011, 7, 419–425. [Google Scholar] [CrossRef]
- Opel, D.J.; Taylor, J.A.; Mangione-Smith, R.; Solomon, C.; Zhao, C.; Catz, S.; Martin, D. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine 2011, 29, 6598–6605. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Taylor, J.A.; Zhou, C.; Catz, S.; Myaing, M.; Mangione-Smith, R. The relationship between parent attitudes about childhood vaccines survey scores and future child immunization status: A validation study. JAMA Pediatr. 2013, 167, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Truong, B.Q.Q.; Ong, K.I.C.; Shibanuma, A.; Kiriya, J.; Jimba, M. Adaptation and application of the parent attitudes about childhood vaccines survey tool in the vietnamese language: A cross-sectional study. BMC Public Health 2024, 24, 946. [Google Scholar] [CrossRef]
- Abd Halim, H.; Abdul-Razak, S.; Yasin, M.M.; Isa, M.R. Validation study of the parent attitudes about childhood vaccines (pacv) questionnaire: The malay version. Hum. Vaccin. Immunother. 2020, 16, 1040–1049. [Google Scholar] [CrossRef]
- Cunningham, R.M.; Kerr, G.B.; Orobio, J.; Munoz, F.M.; Correa, A.; Villafranco, N.; Monterrey, A.C.; Opel, D.J.; Boom, J.A. Development of a spanish version of the parent attitudes about childhood vaccines survey. Hum. Vaccin. Immunother. 2019, 15, 1106–1110. [Google Scholar] [CrossRef] [PubMed]
- Olarewaju, V.O.; Jafflin, K.; Deml, M.J.; Zimmermann, C.; Sonderegger, J.; Preda, T.; Staub, H.; Kwiatkowski, M.; Kloetzer, A.; Huber, B.M.; et al. Application of the parent attitudes about childhood vaccines (pacv) survey in three national languages in switzerland: Exploratory factor analysis and mokken scale analysis. Hum. Vaccin. Immunother. 2021, 17, 2652–2660. [Google Scholar] [CrossRef]
- Tokiya, M.; Hara, M.; Matsumoto, A.; Ashenagar, M.S.; Nakano, T.; Hirota, Y. Acceptance of booster COVID-19 vaccine and its association with components of vaccination readiness in the general population: A cross-sectional survey for starting booster dose in Japan. Vaccines 2022, 10, 1102. [Google Scholar] [CrossRef]
- Ministry of Health, Labour, and Welfare. About COVID-19 Vaccine (shingata korona wakutin ni tuite). Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/vaccine_00184.html (accessed on 1 October 2024).
- Machida, M.; Kojima, T.H.; Popiel, A.; Geiger, M.; Odagiri, Y.; Inoue. Japanese Version of the 7Cs of Vaccination Readiness. 2021. Available online: http://www.tmu-ph.ac/news/data/vaccination-readiness-01.pdf (accessed on 1 October 2024).
- Goretzko, D.; Siemund, K.; Sterner, P. Evaluating model fit of measurement models in confirmatory factor analysis. Edu. Psych. Manag 2024, 84, 123–144. [Google Scholar] [CrossRef]
- Ministry of Health, Labour, and Welfare. Number of Doses of the COVID-19 Vaccine. 2024. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/kekkaku-kansenshou/yobou-sesshu/syukeihou_00002.html (accessed on 1 October 2024).
- Nguyen, T.; Henningsen, K.H.; Brehaut, J.C.; Hoe, E.; Wilson, K. Acceptance of a pandemic influenza vaccine: A systematic review of surveys of the general public. Infect. Drug Resist. 2011, 4, 197–207. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child. Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Rajapakse, N.; Dixit, D. Human and novel coronavirus infections in children: A review. Paediatr. Int. Child. Health 2021, 41, 36–55. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Pittet, L.F.; Finn, A.; Pollard, A.J.; Curtis, N. Should children be vaccinated against COVID-19? Arch. Dis. Child. 2022, 107, e1. [Google Scholar] [CrossRef] [PubMed]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- McMurray, J.; McNeil, H.; Gordon, A.; Elliott, J.; Stolee, P. Psychometric testing of a rehabilitative care patient experience instrument. Arch. Phys. Med. Rehabil. 2018, 99, 1840–1847. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| 7C Scale Original Version Short Version | Modified 7C Scale Version | Modified 7C Scale Japanese Version | |
|---|---|---|---|
| Confidence | I am convinced the appropriate authorities do only allow effective and safe vaccines. | I am convinced the appropriate authorities do only allow effective and safe vaccines for children. | 政府関係機関が小児に対して効果的で安全なワクチンのみを許可すると確信している. |
| Complacency | I get vaccinated because it is too risky to get infected. | I get my child vaccinated because it is too risky for children to get infected. | 小児が感染すると非常に危険なので,子どもに予防接種を受けさせる. |
| Constraints | Vaccinations are so important to me that I prioritize getting vaccinated over other things. | Vaccinations are so important for my child that I prioritize getting them vaccinated over other things. | 予防接種は子どもにとってとても大切なので,他のことよりも優先する. |
| Calculation | I only get vaccinated when the benefits clearly outweigh the risks. (R) | I only get my child vaccinated when the benefits clearly outweigh the risks. (R) | 利益が危険性より明らかに上回る場合にのみ,予防接種を受けさせる.(R) |
| Collective responsibility | I see vaccination as a collective task against the spread of diseases. | I see vaccinations as a collective task against the spread of disease in schools. | 予防接種は学校での病気の蔓延を防ぐための集団行動だと思う. |
| Compliance | It should be possible to sanction people who do not follow the vaccination recommendations by health authorities. | It should be possible to sanction parents who do not follow the vaccination recommendations by health authorities. | 保健機関による予防接種の推奨に従わない人には,制裁を加えることができるようにすべきだ. |
| Conspiracy | Vaccinations cause diseases and allergies that are more serious than the diseases they ought to protect from. (R) | Vaccinations cause diseases and allergies that are more serious than the diseases they ought to protect from. (R) | ワクチンの接種は,それが本来防ぐ病気よりも,もっと深刻な病気やアレルギーを引き起こす.(R) |
| Characteristic | When a Pediatric Vaccine for COVID-19 Becomes Available, I Will Vaccinate My Children | p-Value a | ||||
|---|---|---|---|---|---|---|
| Strongly Disagree (N = 88) n (%) | Disagree (N = 154) n (%) | Undecided (N = 430) n (%) | Agree (N = 405) n (%) | Strongly Agree (N = 113) n (%) | ||
| Percent of responses | (7.4%) | (12.9%) | (36.1%) | (34.0%) | (9.5%) | |
| Sex | 0.009 | |||||
| Male | 36 (40.9) | 58 (37.7) | 171 (39.8) | 178 (44.0) | 65 (57.5) | |
| Female | 52 (59.1) | 96 (62.3) | 259 (60.2) | 227 (56.1) | 48 (42.5) | |
| Age (years), mean ± SD | 37.5 ± 6.5 | 36.5 ± 6.6 | 37.6 ± 7.8 | 40.3 ± 9.0 | 39.8 ± 9.0 | <0.001 b |
| Residential region | 0.544 | |||||
| Hokkaido | 4 (4.6) | 7 (4.6) | 22 (5.1) | 19 (4.7) | 6 (5.3) | |
| Tohoku | 6 (6.8) | 5 (3.3) | 19 (4.4) | 22(5.4) | 7 (6.2) | |
| Kanto | 22 (25.0) | 37 (24.0) | 136 (31.6) | 131 (32.4) | 43 (38.1) | |
| Chubu | 14 (15.9) | 36 (23.4) | 83 (19.3) | 80 (19.8) | 17 (15.0) | |
| Kinki | 22 (25.0) | 30 (19.5) | 82 (19.1) | 74 (18.3) | 24 (21.2) | |
| Chugoku | 6 (6.8) | 7 (4.6) | 26 (6.1) | 27 (6.7) | 5 (4.4) | |
| Shikoku | 3 (3.4) | 2 (1.3) | 12 (2.8) | 12 (2.9) | 2 (1.8) | |
| Kyusyu | 11 (12.5) | 30 (19.5) | 50 (11.6) | 40 (9.9) | 9 (8.0) | |
| Marital status | 0.017 | |||||
| Unmarried | 7 (8.0) | 9 (5.8) | 36 (8.4) | 13 (3.2) | 4 (3.5) | |
| Married | 81 (92.1) | 145 (94.2) | 394 (91.6) | 392 (96.8) | 109 (96.5) | |
| Household income | 0.365 | |||||
| <JPY 4 million | 16 (18.2) | 15 (9.7) | 65 (15.1) | 61 (15.1) | 12 (10.6) | |
| ≥JPY 4 million | 54 (61.4) | 107 (69.5) | 278 (64.7) | 268 (66.2) | 85 (75.2) | |
| Unknown | 18 (20.5) | 32 (20.8) | 87 (20.2) | 76 (18.8) | 16 (14.2) | |
| Level of education | 0.140 | |||||
| ≤High school | 15 (17.1) | 35 (22.7) | 109 (25.4) | 84 (20.7) | 18 (15.9) | |
| >High school | 73 (83.0) | 119 (77.3) | 321 (74.7) | 321 (79.3) | 95(84.1) | |
| Concerns about adverse events | ||||||
| Strongly disagree | 6 (6.8) | 5 (3.3) | 5 (1.2) | 1 (0.3) | 2 (1.8) | <0.001 |
| Disagree | 4 (4.6) | 15 (9.7) | 25 (5.8) | 14 (3.5) | 12 (10.6) | |
| Not sure | 2 (2.3) | 18 (11.7) | 91 (21.2) | 58 (14.3) | 24 (21.2) | |
| Agree | 10 (11.4) | 47 (30.5) | 148 (34.4) | 209 (51.6) | 35 (31.0) | |
| Strongly agree | 66 (75.0) | 69 (44.8) | 161 (37.4) | 123 (30.4) | 40 (35.4) | |
| Parental vaccination for COVID-19 | ||||||
| None | 40 (45.5) | 32 (20.8) | 49 (11.4) | 13 (3.2) | 4 (3.5) | <0.001 |
| Once | 1 (1.1) | 2 (1.3) | 9 (2.1) | 7 (1.7) | 1 (0.9) | |
| Twice | 47 (53.4) | 116 (75.3) | 364 (84.7) | 375 (92.6) | 106 (93.8) | |
| Three times | 0 (0.0) | 4 (2.6) | 8 (1.9) | 10 (2.5) | 2 (1.8) | |
| Number of valid responses | N = 48 | N = 122 | N = 381 | N = 392 | N = 109 | |
| Experienced any adverse events c | ||||||
| Fever | 26 (54.2) | 66 (54.1) | 234 (61.4) | 210 (53.6) | 62 (56.9) | 0.238 d |
| Fatigue | 27 (56.3) | 70(57.4) | 240 (63.0) | 226 (57.7) | 60(55.1) | 0.429 d |
| Headache | 17 (35.4) | 41 (33.6) | 140 (36.8) | 119 (30.4) | 35 (32.1) | 0.443 d |
| Chill | 13 (27.1) | 20 (16.4) | 78 (20.5) | 69 (17.6) | 23 (21.1) | 0.421 d |
| Vomiting | 0 (0.0) | 0 (0.0) | 11 (2.9) | 5 (1.3) | 3 (2.8) | 0.159 d |
| Diarrhea | 1 (2.1) | 2 (1.6) | 7 (1.8) | 14 (3.6) | 4 (3.7) | 0.508 d |
| Muscular pain | 15 (31.3) | 36 (29.5) | 102 (26.8) | 104 (26.5) | 32 (29.4) | 0.882 d |
| Arthralgia | 5 (10.4) | 25 (20.5) | 58 (15.2) | 64 (16.3) | 21 (19.3) | 0.444 d |
| Anaphylactic shock | 0 (0.0) | 1 (0.8) | 1 (0.3) | 1 (0.3) | 0 (0.0) | 0.702 d |
| Component | When a Pediatric Vaccine for COVID-19 Becomes Available, I Will Vaccinate My Children | ρ | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Strongly Disagree (Mean ± SD) | Disagree (Mean ± SD) | Neither Agree Nor Disagree (Mean ± SD) | Agree (Mean ± SD) | Strongly Agree (Mean ± SD) | |||
| Confidence | 1.91 ± 1.06 | 2.58 ± 0.88 | 3.03 ± 0.74 | 3.49 ± 0.78 | 3.91 ± 0.87 | 0.513 | <0.001 |
| Complacency | 1.82 ± 1.07 | 2.56 ± 0.75 | 3.06 ± 0.56 | 3.74 ± 0.67 | 4.27 ± 0.90 | 0.667 | <0.001 |
| Constraints | 1.98 ± 1.10 | 2.40 ± 0.79 | 2.97 ± 0.69 | 3.58 ± 0.69 | 4.14 ± 0.85 | 0.610 | <0.001 |
| Calculation | 3.16 ± 1.42 | 2.69 ± 0.96 | 2.58 ± 0.78 | 2.50 ± 0.85 | 2.50 ± 1.13 | −0.127 | <0.001 |
| Collective responsibility | 2.44 ± 1.26 | 3.09 ± 0.86 | 3.43 ± 0.76 | 3.99 ± 0.61 | 4.43 ± 0.79 | 0.549 | <0.001 |
| Compliance | 1.56 ± 0.96 | 1.93 ± 0.92 | 2.39 ± 0.94 | 2.55 ± 1.05 | 2.88 ± 1.27 | 0.278 | <0.001 |
| Conspiracy | 2.33 ± 1.15 | 2.90 ± 0.88 | 2.98 ± 0.69 | 3.03 ± 0.76 | 3.20 ± 1.15 | 0.170 | <0.001 |
| Total vaccination readiness | 15.19 ± 4.50 | 18.16 ± 2.62 | 20.45 ± 2.35 | 22.87 ± 2.36 | 25.35 ± 3.14 | 0.678 | <0.001 |
| Vaccinated Against COVID-19 | ||
|---|---|---|
| No N = 406 | Yes N = 130 | |
| Confidence, n (%) | ||
| Strongly disagree | 30 (85.7) | 5 (14.3) |
| Disagree | 62 (89.9) | 7 (10.1) |
| Neither agree nor disagree | 184 (78.6) | 50 (21.4) |
| Agree | 114 (66.3) | 58 (33.7) |
| Strongly agree | 16 (61.5) | 10 (38.5) |
| Complacency, n (%) | ||
| Strongly disagree | 20 (80.0) | 5 (20.0) |
| Disagree | 47 (88.7) | 6 (11.3) |
| Neither agree nor disagree | 196 (83.4) | 39 (16.6) |
| Agree | 123 (66.8) | 61 (33.2) |
| Strongly agree | 20 (51.3) | 19 (48.7) |
| Constraints, n (%) | ||
| Strongly disagree | 27 (90.0) | 3 (10.0) |
| Disagree | 71 (91.0) | 7 (9.0) |
| Neither agree nor disagree | 182 (77.4) | 53 (22.6) |
| Agree | 114 (69.5) | 50 (30.5) |
| Strongly agree | 12 (41.4) | 17 (58.6) |
| Calculation, n (%) | ||
| Strongly disagree | 11 (73.3) | 4 (26.7) |
| Disagree | 38 (70.4) | 16 (29.6) |
| Neither agree nor disagree | 159 (79.5) | 41 (20.5) |
| Agree | 151 (72.2) | 58 (27.8) |
| Strongly agree | 47 (81.0) | 11 (19.0) |
| Collective responsibility, n (%) | ||
| Strongly disagree | 18 (85.7) | 3 (14.3) |
| Disagree | 17 (77.3) | 5 (22.7) |
| Neither agree nor disagree | 131 (85.1) | 23 (14.9) |
| Agree | 192 (71.6) | 76 (28.4) |
| Strongly agree | 48 (67.6) | 23 (32.4) |
| Compliance, n (%) | ||
| Strongly disagree | 123 (89.8) | 14 (10.2) |
| Disagree | 113 (76.4) | 35 (23.6) |
| Neither agree nor disagree | 120 (70.2) | 51 (29.8) |
| Agree | 41 (66.1) | 21 (33.9) |
| Strongly agree | 9 (50.0) | 9 (50.0) |
| Conspiracy, n (%) | ||
| Strongly disagree | 14 (70.0) | 6 (30.0) |
| Disagree | 65 (66.3) | 33 (33.7) |
| Neither agree nor disagree | 222 (79.6) | 57 (20.4) |
| Agree | 89 (74.8) | 30 (25.2) |
| Strongly agree | 16 (80.0) | 4 (20.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tokiya, M.; Matsumoto, A.; Furukawa, Y.; Kobayashi, T.; Nakano, T.; Hirota, Y.; Hara, M. Validation of the Modified Japanese 7C Readiness Scale for Parental Intentions of Child COVID-19 Vaccination. Hygiene 2024, 4, 515-526. https://doi.org/10.3390/hygiene4040039
Tokiya M, Matsumoto A, Furukawa Y, Kobayashi T, Nakano T, Hirota Y, Hara M. Validation of the Modified Japanese 7C Readiness Scale for Parental Intentions of Child COVID-19 Vaccination. Hygiene. 2024; 4(4):515-526. https://doi.org/10.3390/hygiene4040039
Chicago/Turabian StyleTokiya, Mikiko, Akiko Matsumoto, Yutaro Furukawa, Takaomi Kobayashi, Takashi Nakano, Yoshio Hirota, and Megumi Hara. 2024. "Validation of the Modified Japanese 7C Readiness Scale for Parental Intentions of Child COVID-19 Vaccination" Hygiene 4, no. 4: 515-526. https://doi.org/10.3390/hygiene4040039
APA StyleTokiya, M., Matsumoto, A., Furukawa, Y., Kobayashi, T., Nakano, T., Hirota, Y., & Hara, M. (2024). Validation of the Modified Japanese 7C Readiness Scale for Parental Intentions of Child COVID-19 Vaccination. Hygiene, 4(4), 515-526. https://doi.org/10.3390/hygiene4040039