
Pantoea agglomerans Lipopolysaccharide Controls Nasal Discomfort—A Placebo-Controlled, Randomized, Double-Blind, Parallel-Group Comparison Trial

Abstract
1. Introduction
2. Materials and Methods
2.1. Test Foods and Intake
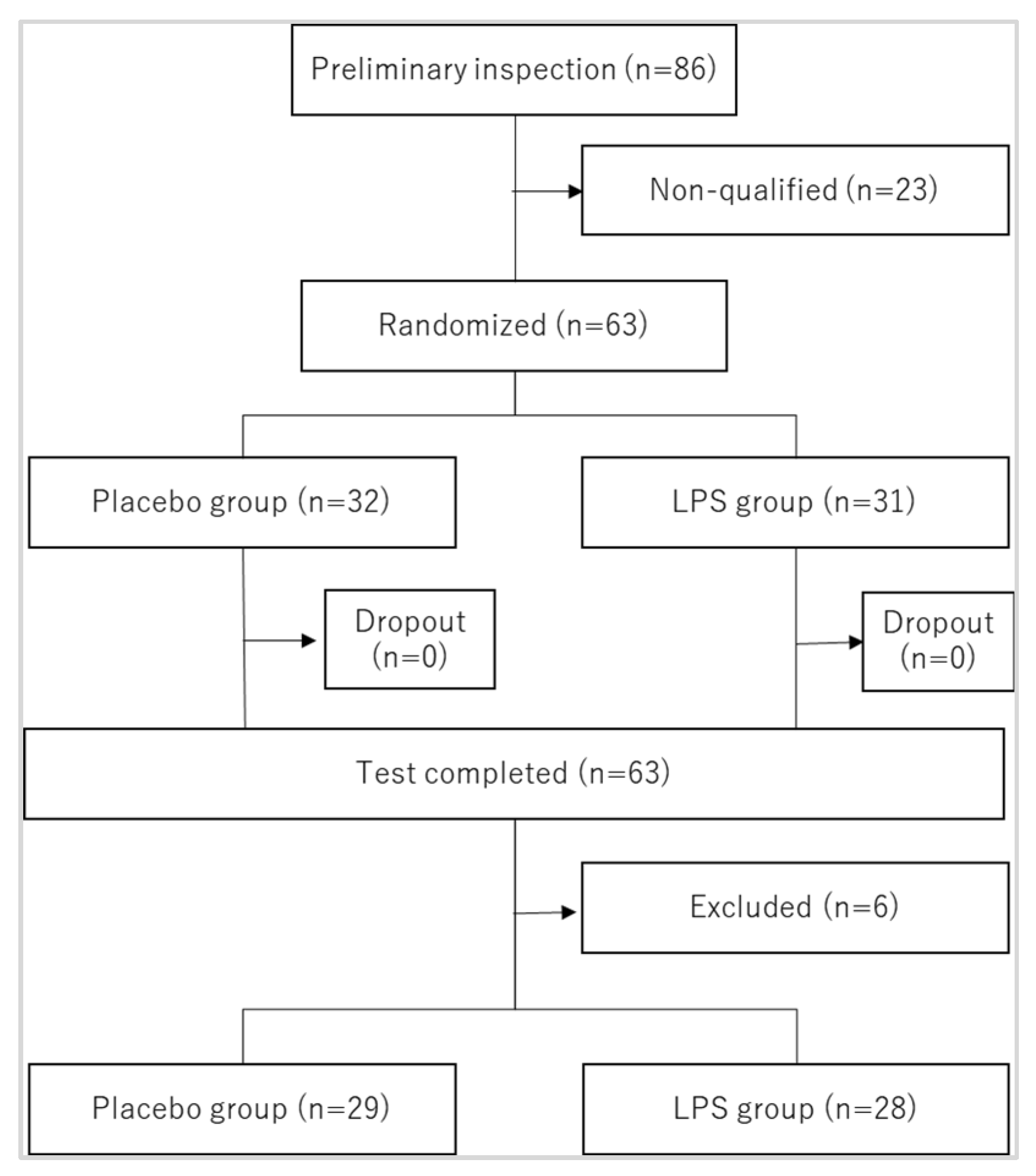
2.2. Participants
2.3. Test Design
2.4. Assessment of Subjective Symptoms of Eye–Nose Allergy
2.5. IgE and Eosinophil Counts
2.6. Questionnaire Survey on Daily Life and Medication (Daily Diary)
2.7. Safety Assessment (Hematology and Blood Chemistry Tests)
2.8. Statistical Analysis
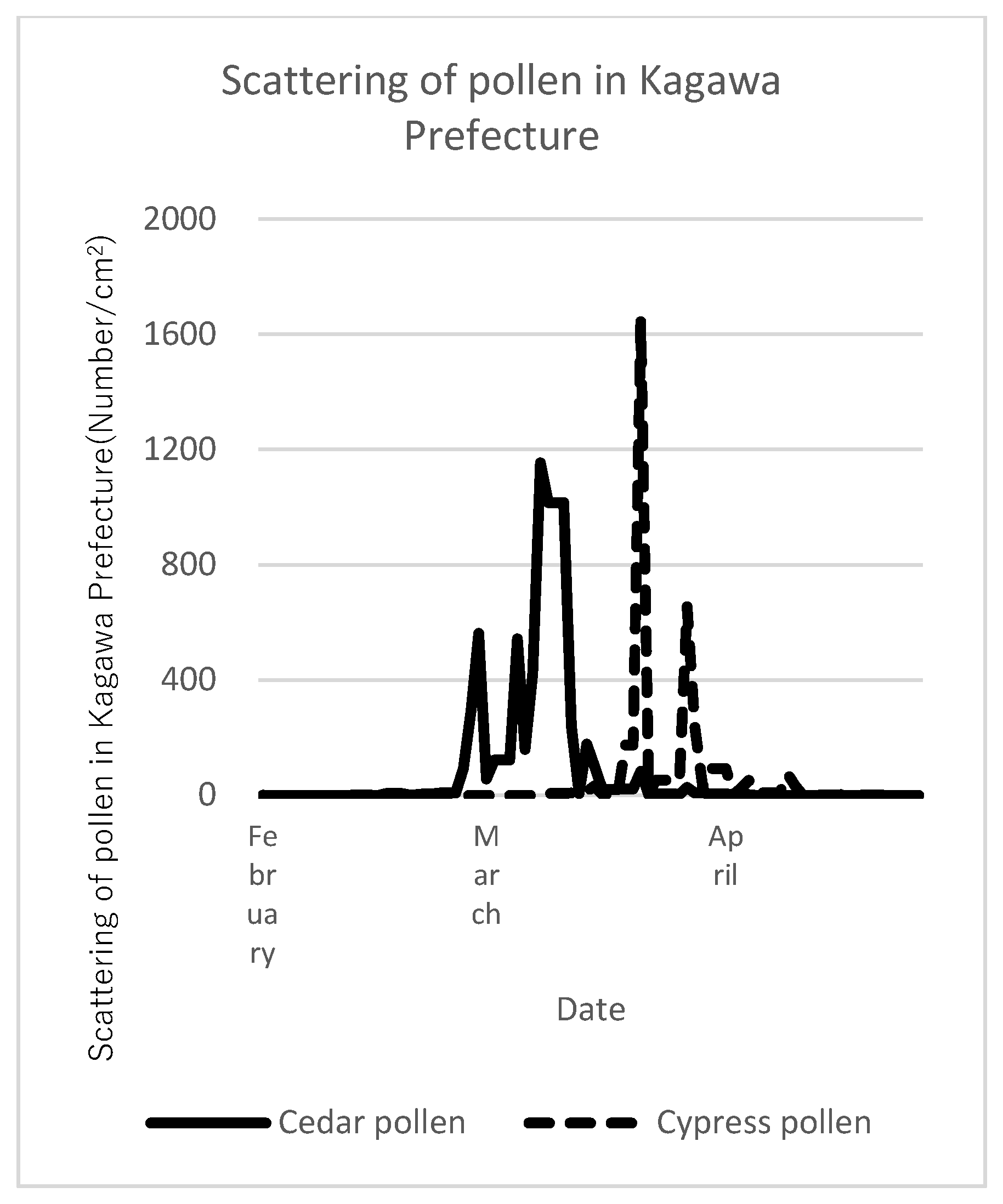
2.9. Pollen Dispersal Status
3. Results
3.1. Participants’ Basic Characteristics
3.2. Eye–Nose Allergic Symptoms
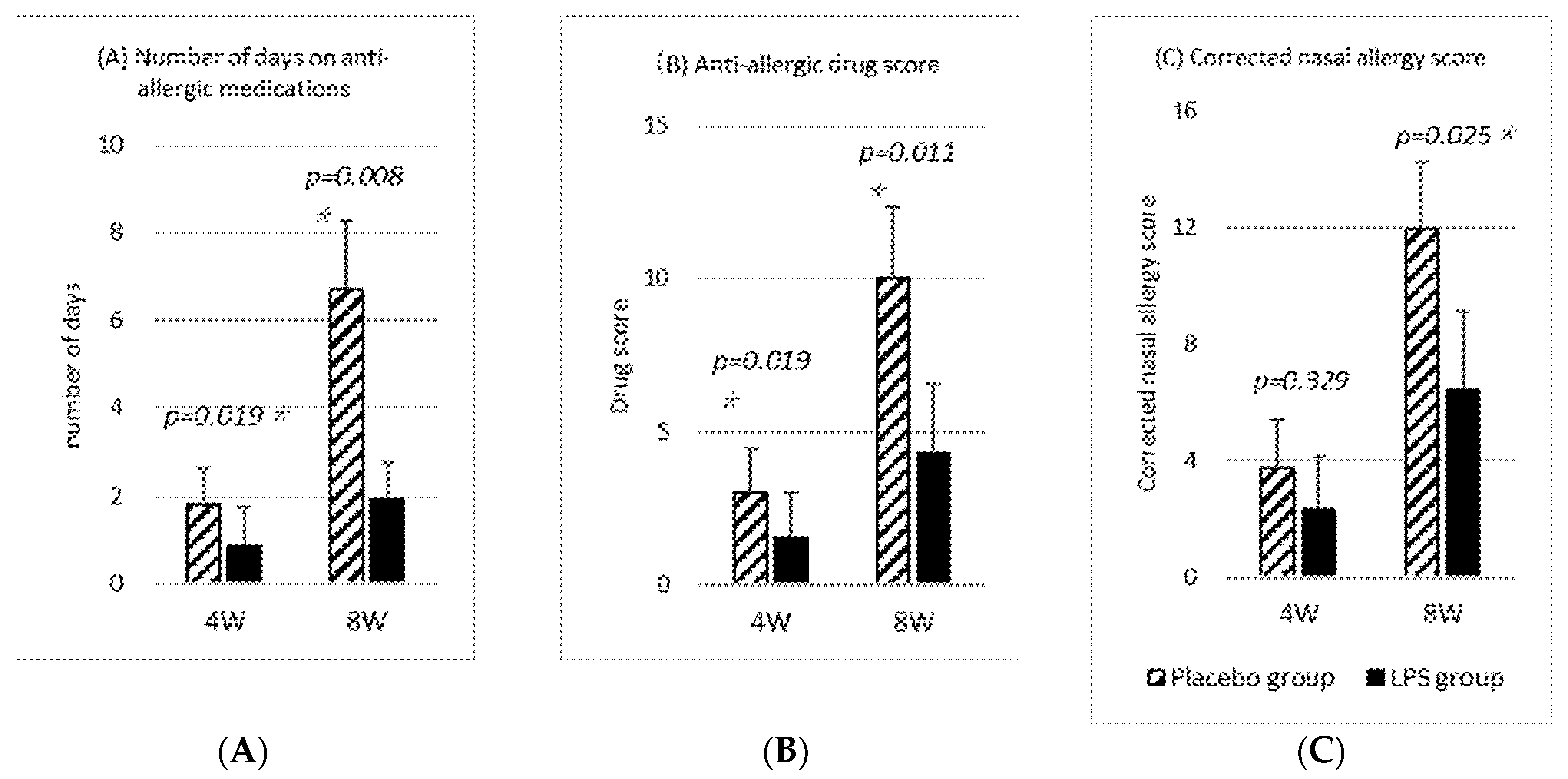
3.3. Analysis of Eye–Nose Allergic Symptoms Considering the Use of Antiallergic Drugs
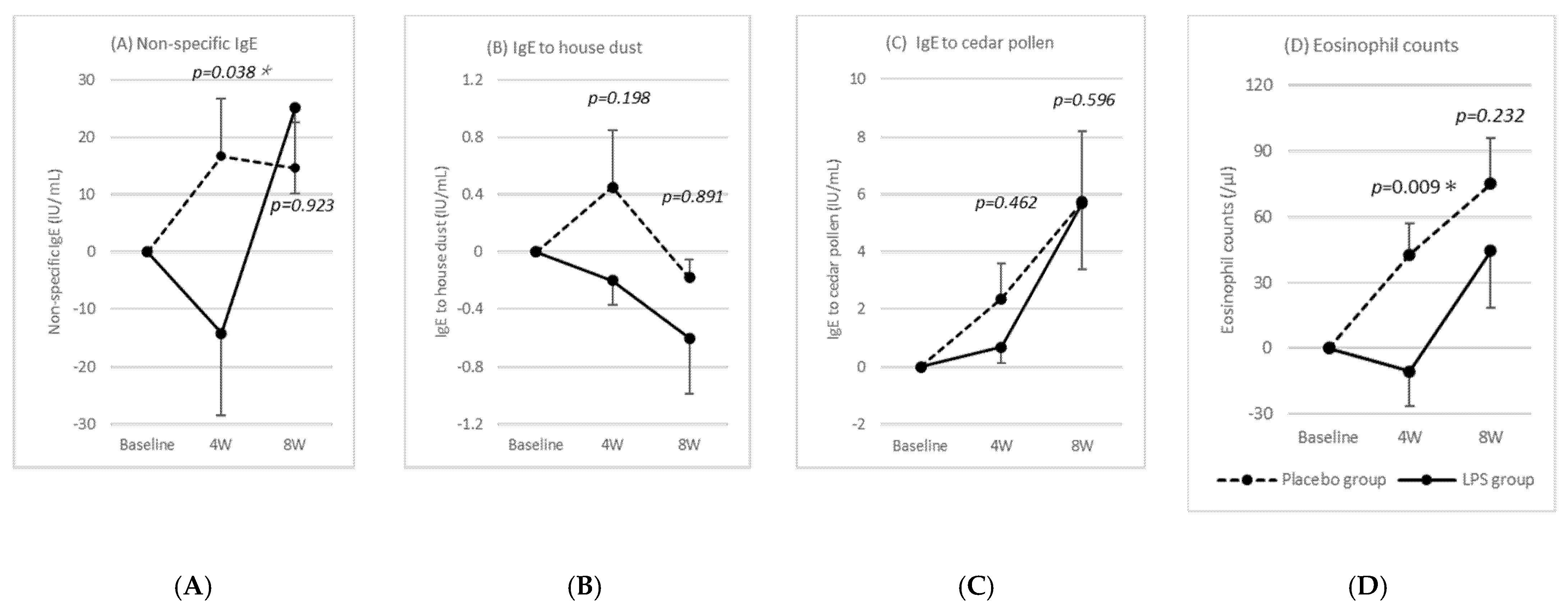
3.4. Changes in the IgE and Eosinophil Counts
3.5. Safety Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asako, M.; Okubo, K.; Ota, N.; Okano, M.; Kamijo, A.; Goto, M.; Sakasita, M.; Sakurai, D.; Terada, T.; Nakamaru, Y.; et al. Practical Guideline for the Management of Allergic Rhinitis in Japan, 9th ed.; Life Scirence: Tokyo, Japan, 2020. [Google Scholar]
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 299, 1259–1260. [Google Scholar] [CrossRef] [PubMed]
- Braun-Fahrlander, C.; Riedler, J.; Herz, U.; Eder, W.; Waser, M.; Grize, L.; Maisch, S.; Carr, D.; Gerlach, F.; Bufe, A.; et al. Environmental exposure to endotoxin and its relation to asthma in school-age children. N. Engl. J. Med. 2002, 347, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Inagawa, H.; Nishizawa, T.; Takagi, T.; Mizuno, D.-I.; Soma, G.-I. Protective effect by intradermal administration of Pantoea agglomerans LPS (LPSp) and oral administration of ONO-4007. Biotherapy 1997, 11, 464–466. [Google Scholar]
- Yoshioka, S.; Oe, M.; Kamijyo, F.; Shimada, K.; Okuyama, Y.; Nishiyama, H.; Matsuoka, R.; Masuda, Y.; Kanemitsu, T.; Enomoto, M. Acetic Acid Bacteria (Gluconacetobacter hansenii GK-1) Relieves Nasal Discomforts—A Randomized Double-blinded Placebo-controlled Study. Jpn. Pharmacol. Ther. 2019, 47, 461–467. [Google Scholar]
- Kamijyo, F.; Oe, M.; Yoshioka, S.; Kajiyama, D.; Shimada, K.; Okuyama, Y.; Matsuoka, R.; Masuda, Y.; Kanemitsu, T.; Enomoto, M. Acetic Acid Bacteria (Gluconacetobacter hansenii GK-1) Relieves Nasal Discomforts of Japanese Cedar Pollimpsis. Jpn. Pharmacol. Ther. 2019, 47, 1993–1999. [Google Scholar]
- Brigham, K.L.; Meyrick, B. Endotoxin and lung injury. Am. Rev. Respir. Dis. 1986, 133, 913–927. [Google Scholar] [PubMed]
- Daly, C.G.; Seymour, G.J.; Kieser, J.B. Bacterial endotoxin: A role in chronic inflammatory periodontal disease? J. Oral. Pathol. 1980, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.V.; Worgul, B.V.; Merriam, G.R., Jr. Endotoxin-induced uveitis in the rat. Albrecht Von. Graefes Arch. Klin. Exp. Ophthalmol. 1980, 213, 221–233. [Google Scholar] [CrossRef]
- Herrmann, E.C., Jr.; Engle, C.; Perlman, P.L. Action of antiinflammatory agents on endotoxin-induced lung inflammation in mice. Am. J. Physiol. 1959, 197, 803–807. [Google Scholar] [CrossRef]
- Hopkins, R.W.; Damewood, C.A. Septic shock: Hemodynamics of endotoxin and inflammation. Am. J. Surg. 1974, 127, 476–483. [Google Scholar] [CrossRef]
- Howes, E.L.; Cruse, V.K.; Kwok, M.T. Mononuclear cells in the corneal response to endotoxin. Investig. Ophthalmol. Vis. Sci. 1982, 22, 494–501. [Google Scholar]
- Issekutz, A.C.; Bhimji, S. Role for endotoxin in the leukocyte infiltration accompanying Escherichia coli inflammation. Infect. Immun. 1982, 36, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Issekutz, A.C.; Megyeri, P.; Issekutz, T.B. Role for macrophage products in endotoxin-induced polymorphonuclear leukocyte accumulation during inflammation. Lab. Investig. 1987, 56, 49–59. [Google Scholar]
- Jacobs, D.R.; Cohen, H.B. The inflammatory role of endotoxin in rabbit gram-negative bacterial endophthalmitis. Investig. Ophthalmol. Vis. Sci. 1984, 25, 1074–1079. [Google Scholar]
- Meyrick, B.; Brigham, K.L. Repeated Escherichia coli endotoxin-induced pulmonary inflammation causes chronic pulmonary hypertension in sheep. Structural and functional changes. Lab. Investig. 1986, 55, 164–176. [Google Scholar] [PubMed]
- Movat, H.Z.; Cybulsky, M.I.; Colditz, I.G.; Chan, M.K.; Dinarello, C.A. Acute inflammation in gram-negative infection: Endotoxin, interleukin 1, tumor necrosis factor, and neutrophils. Fed. Proc. 1987, 46, 97–104. [Google Scholar]
- Pitts, D.L.; Williams, B.L.; Morton, T.H., Jr. Investigation of the role of endotoxin in periapical inflammation. J. Endod. 1982, 8, 10–18. [Google Scholar] [CrossRef]
- Rosenbaum, J.T.; Raymond, W. Monocyte chemotactic activity induced by intravitreal endotoxin. Investig. Ophthalmol. Vis. Sci. 1985, 26, 1267–1273. [Google Scholar]
- Young, R.S.; Yagel, S.K.; Towfighi, J. Systemic and neuropathologic effects of E. coli endotoxin in neonatal dogs. Pediatr. Res. 1983, 17, 349–353. [Google Scholar] [CrossRef]
- Phipps, K.R.; Sulaiman, C.; Simon, R.; Holalagoudar, S.; Kohchi, C.; Nakata, Y. Subchronic (90-day) toxicity assessment of Somacy-FP100, a lipopolysaccharide-containing fermented wheat flour extract from Pantoea agglomerans. J. Appl. Toxicol. 2020, 40, 1342–1352. [Google Scholar] [CrossRef]
- Kohchi, C.; Uehiro, M.; Yamashita, M.; Inagawa, H.; Soma, G.-I. Foods Containing Pantoea agglomerans LPS Reduce Eye-Nose Allergies—A Double-Blind, Placebo-Controlled, Randomized, Parallel-Group Comparative Pilot Study. Int. J. Transl. Med. 2023, 3, 299–309. [Google Scholar] [CrossRef]
- Nakata, K.; Nakata, Y.; Inagawa, H.; Nakamoto, T.; Yoshimura, H.; Soma, G. Pantoea agglomerans lipopolysaccharide maintains bone density in premenopausal women: A randomized, double-blind, placebo-controlled trial. Food Sci. Nutr. 2014, 2, 638–646. [Google Scholar] [CrossRef]
- Nakata, K.; Taniguchi, Y.; Yoshioka, N.; Yoshida, A.; Inagawa, H.; Nakamoto, T.; Yoshimura, H.; Miyake, S.; Kohchi, C.; Kuroki, M.; et al. A mixture of Salacia oblonga extract and IP-PA1 reduces fasting plasma glucose (FPG) and low-density lipoprotein (LDL) cholesterol levels. Nutr. Res. Pract. 2011, 5, 435–442. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nakata, Y.; Kohchi, C.; Ogawa, K.; Nakamoto, T.; Yoshimura, H.; Soma, G.I. Effects of 3 months continuous intake of supplement containing Pantoea agglomerans LPS to maintain normal bloodstream in adults: Parallel double-blind randomized controlled study. Food Sci. Nutr. 2018, 6, 197–206. [Google Scholar] [CrossRef]
- Durham, O.C. The volumetric incidence of atmospheric allergens; a proposed standard method of gravity sampling, counting, and volumetric interpolation of results. J. Allergy 1946, 17, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Kohchi, C.; Inagawa, H.; Nishizawa, T.; Yamaguchi, T.; Nagai, S.; Soma, G. Applications of lipopolysaccharide derived from Pantoea agglomerans (IP-PA1) for health care based on macrophage network theory. J. Biosci. Bioeng. 2006, 102, 485–496. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Yoshioka, N.; Nishizawa, T.; Inagawa, H.; Kohchi, C.; Soma, G. Utility and safety of LPS-based fermented flour extract as a macrophage activator. Anticancer Res. 2009, 29, 859–864. [Google Scholar]
- Wassenaar, T.M.; Zimmermann, K. Lipopolysaccharides in Food, Food Supplements, and Probiotics: Should We be Worried? Eur. J. Microbiol. Immunol. 2018, 8, 63–69. [Google Scholar] [CrossRef]
- Chung, S.H.; Choi, S.H.; Cho, K.J.; Joo, C.K. Toll-like receptor 4 signalling attenuates experimental allergic conjunctivitis. Clin. Exp. Immunol. 2011, 164, 275–281. [Google Scholar] [CrossRef]
- Debarry, J.; Garn, H.; Hanuszkiewicz, A.; Dickgreber, N.; Blumer, N.; von Mutius, E.; Bufe, A.; Gatermann, S.; Renz, H.; Holst, O.; et al. Acinetobacter lwoffii and Lactococcus lactis strains isolated from farm cowsheds possess strong allergy-protective properties. J. Allergy Clin. Immunol. 2007, 119, 1514–1521. [Google Scholar] [CrossRef]
- Looringh van Beeck, F.A.; Hoekstra, H.; Brunekreef, B.; Willemse, T. Inverse association between endotoxin exposure and canine atopic dermatitis. Vet. J. 2011, 190, 215–219. [Google Scholar] [CrossRef]
- Schuijs, M.J.; Willart, M.A.; Vergote, K.; Gras, D.; Deswarte, K.; Ege, M.J.; Madeira, F.B.; Beyaert, R.; van Loo, G.; Bracher, F.; et al. Farm dust and endotoxin protect against allergy through A20 induction in lung epithelial cells. Science 2015, 349, 1106–1110. [Google Scholar] [CrossRef]
- Wang, N.; McKell, M.; Dang, A.; Yamani, A.; Waggoner, L.; Vanoni, S.; Noah, T.; Wu, D.; Kordowski, A.; Kohl, J.; et al. Lipopolysaccharide suppresses IgE-mast cell-mediated reactions. Clin. Exp. Allergy 2017, 47, 1574–1585. [Google Scholar] [CrossRef]
- Wang, Y.; McCusker, C. Neonatal exposure with LPS and/or allergen prevents experimental allergic airways disease: Development of tolerance using environmental antigens. J. Allergy Clin. Immunol. 2006, 118, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Maggi, E. The TH1/TH2 paradigm in allergy. Immunotechnology 1998, 3, 233–244. [Google Scholar] [CrossRef]
- Moverare, R.; Elfman, L.; Stalenheim, G.; Bjornsson, E. Study of the Th1/Th2 balance, including IL-10 production, in cultures of peripheral blood mononuclear cells from birch-pollen-allergic patients. Allergy 2000, 55, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, S. T-cell subsets (Th1 versus Th2). Ann. Allergy Asthma Immunol. 2000, 85, 9–18, quiz 18, 21. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Y.; Gu, W.; He, L.; Sun, B. Th1/Th2 cell’s function in immune system. Adv. Exp. Med. Biol. 2014, 841, 45–65. [Google Scholar]
- Coyle, A.J.; Tsuyuki, S. Th2 cells and cytokine networks in allergic inflammation of the lung. Mediat. Inflamm. 1995, 4, 239–247. [Google Scholar] [CrossRef]
- Hamilos, D.L.; Leung, D.Y.; Wood, R.; Cunningham, L.; Bean, D.K.; Yasruel, Z.; Schotman, E.; Hamid, Q. Evidence for distinct cytokine expression in allergic versus nonallergic chronic sinusitis. J. Allergy Clin. Immunol. 1995, 96, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Makino, S.; Fukuda, T. Eosinophils and allergy in asthma. Allergy Proc. 1995, 16, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, G.; Bianco, A.; Catena, E.; De Palma, R.; Abbate, G.F. Th1/Th2 lymphocyte polarization in asthma. Allergy 2000, 55 (Suppl. S61), 6–9. [Google Scholar] [CrossRef] [PubMed]
- Mudde, G.C.; Bheekha, R.; Bruijnzeel-Koomen, C.A. Consequences of IgE/CD23-mediated antigen presentation in allergy. Immunol. Today 1995, 16, 380–383. [Google Scholar] [CrossRef]
- Sampson, H.A. Mechanisms in adverse reactions to food. The skin. Allergy 1995, 50, 46–51. [Google Scholar] [CrossRef]
- Colavita, A.M.; Reinach, A.J.; Peters, S.P. Contributing factors to the pathobiology of asthma. The Th1/Th2 paradigm. Clin. Chest Med. 2000, 21, 263–277, viii. [Google Scholar] [CrossRef] [PubMed]
- Shirafuji, Y.; Matsuura, H.; Sato, A.; Kanzaki, H.; Katayama, H.; Arata, J. Hyperimmunoglobin E syndrome: A sign of TH1/TH2 imbalance? Eur. J. Dermatol. 1999, 9, 129–131. [Google Scholar]
- Kawai, T.; Akira, S. Toll-like receptors and their crosstalk with other innate receptors in infection and immunity. Immunity 2011, 34, 637–650. [Google Scholar] [CrossRef]
- Palomares, O.; Yaman, G.; Azkur, A.K.; Akkoc, T.; Akdis, M.; Akdis, C.A. Role of Treg in immune regulation of allergic diseases. Eur. J. Immunol. 2010, 40, 1232–1240. [Google Scholar] [CrossRef]
- Lewkowicz, N.; Klink, M.; Mycko, M.P.; Lewkowicz, P. Neutrophil--CD4+CD25+ T regulatory cell interactions: A possible new mechanism of infectious tolerance. Immunobiology 2013, 218, 455–464. [Google Scholar] [CrossRef]
- Caramalho, I.; Lopes-Carvalho, T.; Ostler, D.; Zelenay, S.; Haury, M.; Demengeot, J. Regulatory T cells selectively express toll-like receptors and are activated by lipopolysaccharide. J. Exp. Med. 2003, 197, 403–411. [Google Scholar] [CrossRef]
- Lewkowicz, N.; Mycko, M.P.; Przygodzka, P.; Cwiklinska, H.; Cichalewska, M.; Matysiak, M.; Selmaj, K.; Lewkowicz, P. Induction of human IL-10-producing neutrophils by LPS-stimulated Treg cells and IL-10. Mucosal Immunol. 2016, 9, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Lewkowicz, P.; Lewkowicz, N.; Sasiak, A.; Tchorzewski, H. Lipopolysaccharide-activated CD4+CD25+ T regulatory cells inhibit neutrophil function and promote their apoptosis and death. J. Immunol. 2006, 177, 7155–7163. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placebo Food (/Tablet) | Test Food (/Tablet) | |
|---|---|---|
| Energy (kcal) | 1 | 1 |
| Protein (g) | <0.1 | <0.1 |
| Fat (g) | <0.1 | <0.1 |
| Carbohydrates (g) | 0.2 | 0.2 |
| Salt equivalent (g) | 0 | 0 |
| Placebo Group (n = 32) Mean ± SD | LPS Group (n = 31) Mean ± SD | p-Value | |
|---|---|---|---|
| Men: Women (n) | 9:23 | 8:23 | 0.683 |
| Age (years) | 47.4 ± 9.6 | 45.4 ± 10.0 | 0.504 |
| Eye–nose allergy scores | 4.09 ± 0.61 | 5.97 ± 0.73 | 0.061 |
| IgE to house dust | 5.14 ± 1.86 | 8.69 ± 3.83 | 0.967 |
| IgE to cedar pollen | 12.15 ± 3.42 | 8.58 ± 2.32 | 0.670 |
| After 4 Weeks | After 8 Weeks | |||||
|---|---|---|---|---|---|---|
| Placebo Group (n = 32) Mean ± SE | LPS Group (n = 31) Mean ± SE | p-Value | Placebo Group (n = 32) Mean ± SE | LPS Group (n = 31) Mean ± SE | p-Value | |
| Eye–nose allergy scores | 1.34 ± 0.80 | 1.39 ± 0.77 | 0.961 | 3.03 ± 0.98 | 3.90 ± 1.24 | 0.962 |
| Nasal allergy score | 0.75 ± 0.54 | 0.84 ± 0.61 | 0.901 | 1.91 ± 0.71 | 2.19 ± 0.81 | 0.874 |
| Watery | 0.34 ± 0.20 | 0.26 ± 0.19 | 0.948 | 0.53 ± 0.25 | 0.42 ± 0.26 | 0.799 |
| Sneezing | 0.22 ± 0.14 | 0.19 ± 0.18 | 0.950 | 0.59 ± 0.23 | 0.74 ± 0.25 | 0.989 |
| Stuffy | 0.09 ± 0.16 | 0.32 ± 0.21 | 0.491 | 0.34 ± 0.18 | 0.42 ± 0.22 | 0.829 |
| Itchy nose | 0.09 ± 0.16 | 0.06 ± 0.17 | 0.953 | 0.44 ± 0.22 | 0.61 ± 0.21 | 0.338 |
| Eye allergy score | 0.59 ± 0.31 | 0.55 ± 0.26 | 0.715 | 1.13 ± 0.32 | 1.71 ± 0.48 | 0.746 |
| Itchy eye | 0.25 ± 0.16 | 0.35 ± 0.18 | 0.832 | 0.66 ± 0.18 | 0.90 ± 0.28 | 0.746 |
| Watery eyes | 0.34 ± 0.17 | 0.19 ± 0.13 | 0.340 | 0.47 ± 0.17 | 0.81 ± 0.23 | 0.502 |
| QOL | 3.13 ± 2.20 | 2.23 ± 2.04 | 0.581 | 6.75 ± 2.63 | 6.84 ± 3.18 | 0.234 |
| Summative status score | −0.25 ± 0.18 | 0.03 ± 0.16 | 0.193 | 0.16 ± 0.19 | 0.52 ± 0.24 | 0.727 |
| Placebo Group (n = 32) | LPS Group (n = 31) | |
|---|---|---|
| Number of people taking antiallergic medication | 16 | 6 |
| 1–4 w | 8 | 1 |
| 5–8 w | 16 | 6 |
| Evaluation Item | Reference Value | Placebo gr. (n = 32) LPS gr. (n = 31) | Baseline Mean ± SE | After 8 Weeks | p-Value |
|---|---|---|---|---|---|
| White blood cell (μL) | Men: 3300~8600 Women: 3300~8600 | Placebo group | 4928 ± 203 | 5206 ± 272 | 0.132 |
| LPS group | 5061 ± 221 | 5045 ± 238 | 0.530 | ||
| Neutrophil (%) | Men: 45.2~68.8 Women: 49.7~72.7 | Placebo group | 53.87 ± 1.57 | 54.00 ± 1.48 | 0.874 |
| LPS group | 55.14 ± 1.24 | 54.46 ± 1.24 | 0.530 | ||
| Eosinophil (%) | Men: 0.0~10.0 Women: 0.0~5.0 | Placebo group | 2.83 ± 0.43 | 4.07 ± 0.57 | 0.000 * |
| LPS group | 3.90 ± 0.53 | 4.76 ± 0.67 | 0.057 | ||
| Basophil (%) | Men: 0.0~5.0 Women: 0.0~3.0 | Placebo group | 0.75 ± 0.06 | 0.90 ± 0.06 | 0.010 * |
| LPS group | 0.75 ± 0.07 | 0.76 ± 0.07 | 0.838 | ||
| Monocyte (%) | Men: 2.7~7.9 Women: 1.7~8.7 | Placebo group | 5.62 ± 0.23 | 5.73 ± 0.21 | 0.496 |
| LPS group | 5.83 ± 0.30 | 5.52 ± 0.21 | 0.196 | ||
| Lymphocyte (%) | Men: 26.8~43.8 Women: 24.5~38.9 | Placebo group | 36.93 ± 1.35 | 35.30 ± 1.25 | 0.161 |
| LPS group | 34.38 ± 1.07 | 34.50 ± 1.22 | 0.977 | ||
| Red blood cell (×104/μL) | Men: 435~555 Women: 386~492 | Placebo group | 462 ± 7 | 453 ± 7 | 0.014 * |
| LPS group | 463 ± 8 | 458 ± 9 | 0.038 * | ||
| Hemoglobin (g/dL) | Men: 13.7~16.8 Women: 11.6~14.8 | Placebo group | 13.9 ± 0.2 | 13.7 ± 0.2 | 0.031 * |
| LPS group | 13.6 ± 0.3 | 13.4 ± 0.3 | 0.135 | ||
| Hematocrit (%) | Men: 40.7~50.1 Women: 35.1~44.4 | Placebo group | 42.3 ± 0.6 | 41.6 ± 0.6 | 0.032 * |
| LPS group | 41.7 ± 0.7 | 41.3 ± 0.8 | 0.141 | ||
| Platelet (×104/μL) | Men: 15.8~34.8 Women: 15.8~34.8 | Placebo group | 24.6 ± 0.8 | 25.1 ± 0.9 | 0.121 |
| LPS group | 25.8 ± 0.9 | 26.3 ± 1.3 | 0.804 | ||
| AST (U/L) | Men: 13~30 Women: 13~30 | Placebo group | 20.9 ± 0.7 | 20.7 ± 0.6 | 0.551 |
| LPS group | 21.3 ± 1.2 | 19.9 ± 1.0 | 0.064 | ||
| ALT (U/L) | Men: 10~42 Women: 7~23 | Placebo group | 19.7 ± 1.5 | 19.1 ± 1.3 | 0.433 |
| LPS group | 20.3 ± 1.8 | 18.3 ± 1.7 | 0.034 * | ||
| Creatinine (mg/dL) | Men: 0.65~1.07 Women: 0.46~0.79 | Placebo group | 0.67 ± 0.03 | 0.67 ± 0.03 | 0.603 |
| LPS group | 0.68 ± 0.03 | 0.66 ± 0.03 | 0.251 | ||
| CRP (mg/dL) | Men: ≤0.14 Women: ≤0.14 | Placebo group | 0.08 ± 0.03 | 0.18 ± 0.11 | 0.321 |
| LPS group | 0.06 ± 0.01 | 0.10 ± 0.02 | 0.188 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohchi, C.; Uehiro, M.; Fukaya, T.; Watanabe, N.; Inagawa, H.; Soma, G.-I. Pantoea agglomerans Lipopolysaccharide Controls Nasal Discomfort—A Placebo-Controlled, Randomized, Double-Blind, Parallel-Group Comparison Trial. Int. J. Transl. Med. 2024, 4, 126-139. https://doi.org/10.3390/ijtm4010006
Kohchi C, Uehiro M, Fukaya T, Watanabe N, Inagawa H, Soma G-I. Pantoea agglomerans Lipopolysaccharide Controls Nasal Discomfort—A Placebo-Controlled, Randomized, Double-Blind, Parallel-Group Comparison Trial. International Journal of Translational Medicine. 2024; 4(1):126-139. https://doi.org/10.3390/ijtm4010006
Chicago/Turabian StyleKohchi, Chie, Miyuki Uehiro, Taisuke Fukaya, Norikazu Watanabe, Hiroyuki Inagawa, and Gen-Ichiro Soma. 2024. "Pantoea agglomerans Lipopolysaccharide Controls Nasal Discomfort—A Placebo-Controlled, Randomized, Double-Blind, Parallel-Group Comparison Trial" International Journal of Translational Medicine 4, no. 1: 126-139. https://doi.org/10.3390/ijtm4010006
APA StyleKohchi, C., Uehiro, M., Fukaya, T., Watanabe, N., Inagawa, H., & Soma, G.-I. (2024). Pantoea agglomerans Lipopolysaccharide Controls Nasal Discomfort—A Placebo-Controlled, Randomized, Double-Blind, Parallel-Group Comparison Trial. International Journal of Translational Medicine, 4(1), 126-139. https://doi.org/10.3390/ijtm4010006