
Dental Stem Cell-Based Therapy for Glycemic Control and the Scope of Clinical Translation: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Process
2.3. Inclusion Criteria
- Animal studies, regardless of species, age, and gender, published in or before July 2023, were included.
- Studies in which the disease model was induced diabetes mellitus (Type 1 or Type 2), with any manner of disease induction, were included.
- Studies which included control groups with animals administered with saline or vehicle for comparison were included in the review.
- Studies which used dental stem cells, i.e., stem cells of dental origin, as the intervention were included, regardless of dose, timing, frequency, preparation, and route of administration. There were no restrictions regarding the source or portion of the tooth or its supporting tissues from which the DSCs were isolated.
- Studies using blood glucose and/or verifiable parameters of diabetic polyneuropathy, such as sensory and motor nerve conduction velocity (SNCV and MNCV), as outcome variables were included.
- Grey literature, such as preprints, dissertations, theses, unpublished manuscripts, and conference papers was also reviewed to determine if it met the inclusion criteria mentioned above.
2.4. Exclusion Criteria
- Animal studies which did not include diabetic models were not included in the review. In addition, animal studies which did not include diabetic controls administered with saline or vehicle for comparison with diabetic animals administered with DSCs were excluded.
- Studies in which diabetes mellitus was induced after DSC administration were excluded.
- Studies which did not use stem cells of dental origin were not included in the review.
- Studies which did not measure blood glucose and/or DPN parameters, or in which these variables were not measured using valid methods, were not included in the review.
- In vitro studies, surveys, and questionnaires were not included.
- Reviews and duplicate articles were excluded.
2.5. Data Extraction
2.6. Assessment of Internal Bias in Articles
2.7. Assessment of External Validity
2.8. Meta-Analysis
2.8.1. Subgroup Analysis
2.8.2. Publication Bias
3. Results
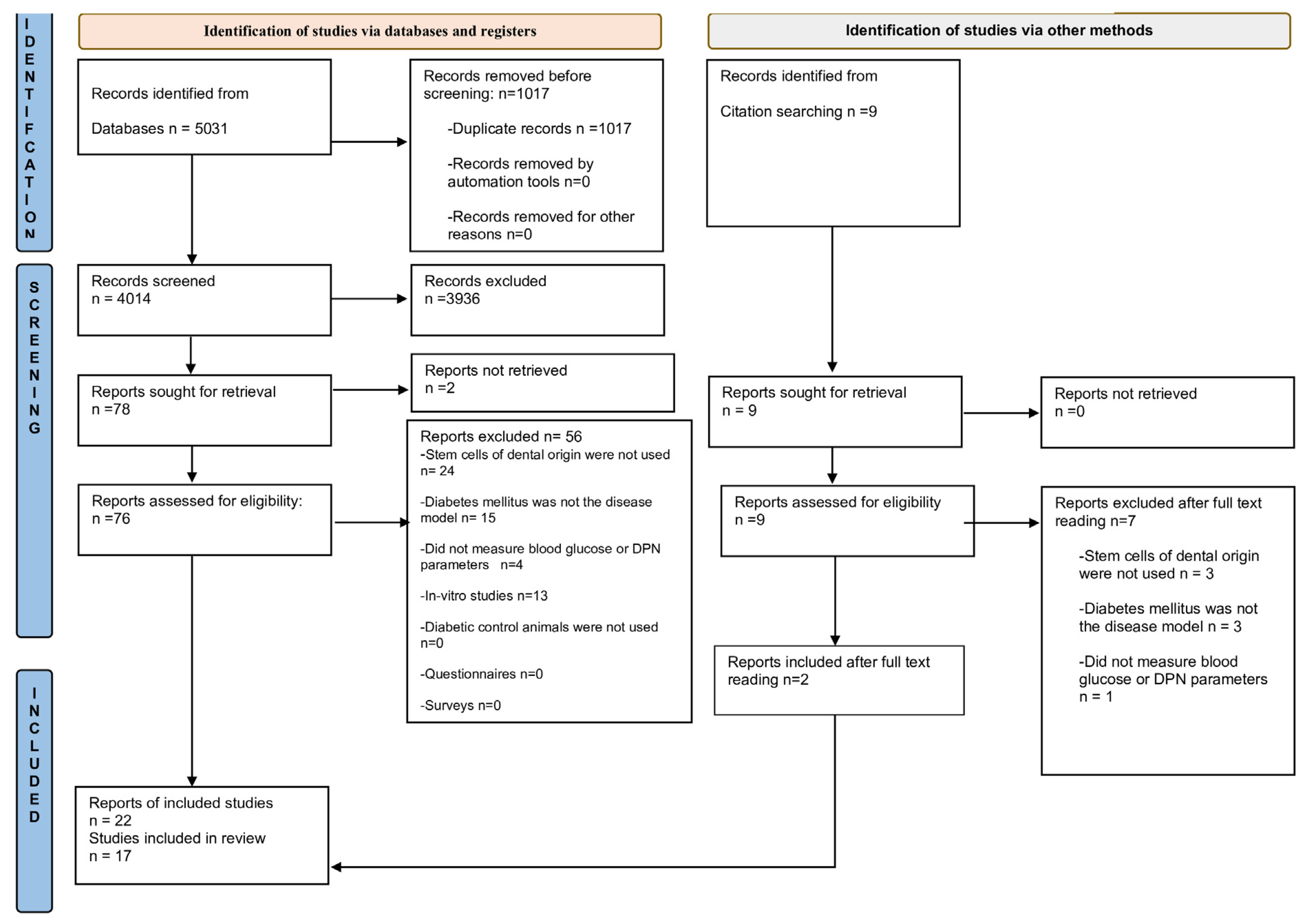
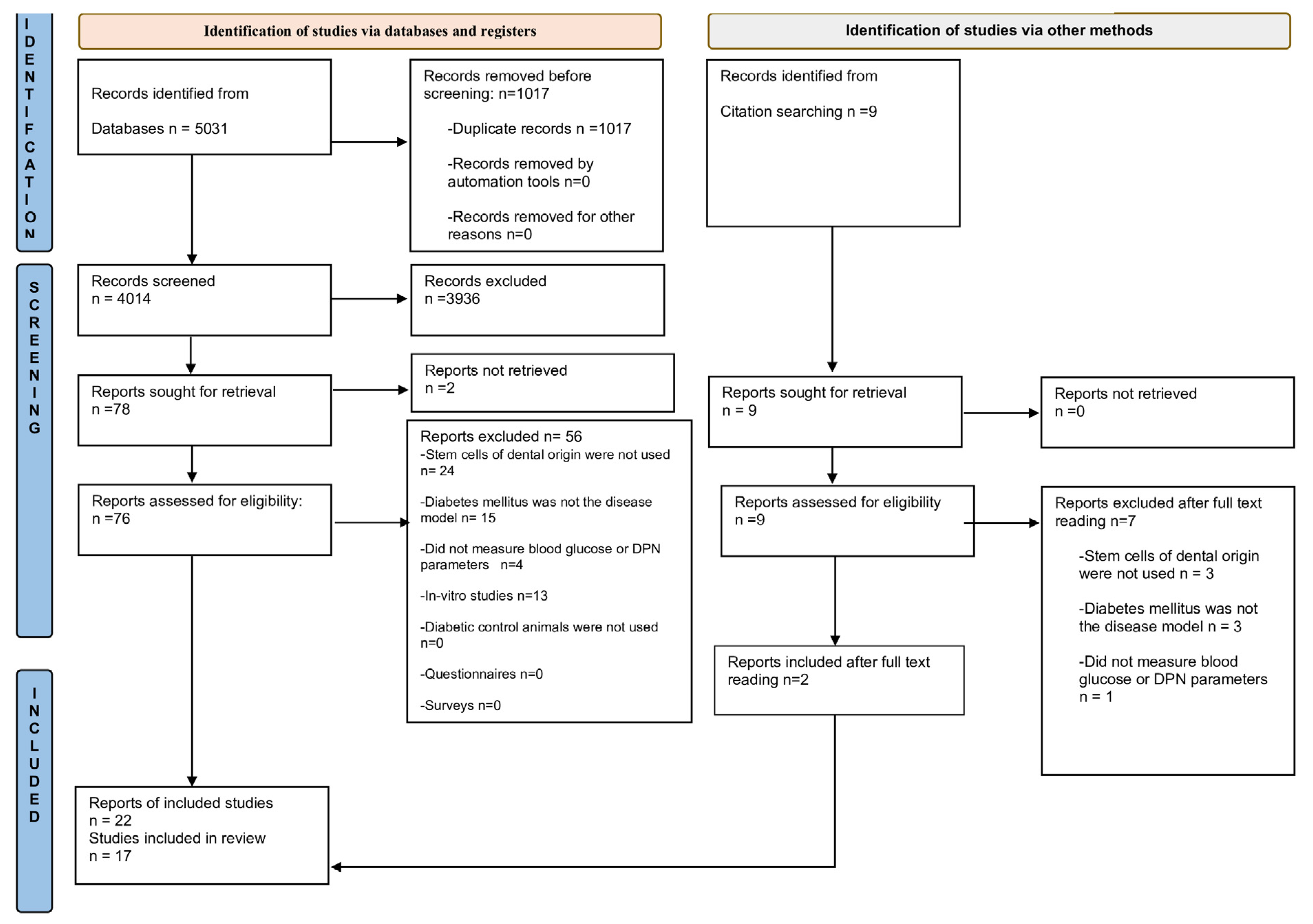
3.1. Study Selection
3.2. Characteristics of Animal Studies
3.2.1. Animal Model Characteristics
3.2.2. Dental Stem Cell Selection in Animal Studies
3.3. Effect of DSCs in Animals
3.4. Characteristics of the Clinical Study and Effects of DSCs in Humans
3.5. Internal Validity of Animal Studies
3.6. External Validity of Animal Studies
3.7. Meta-Analysis
3.7.1. Forest Plot Analysis
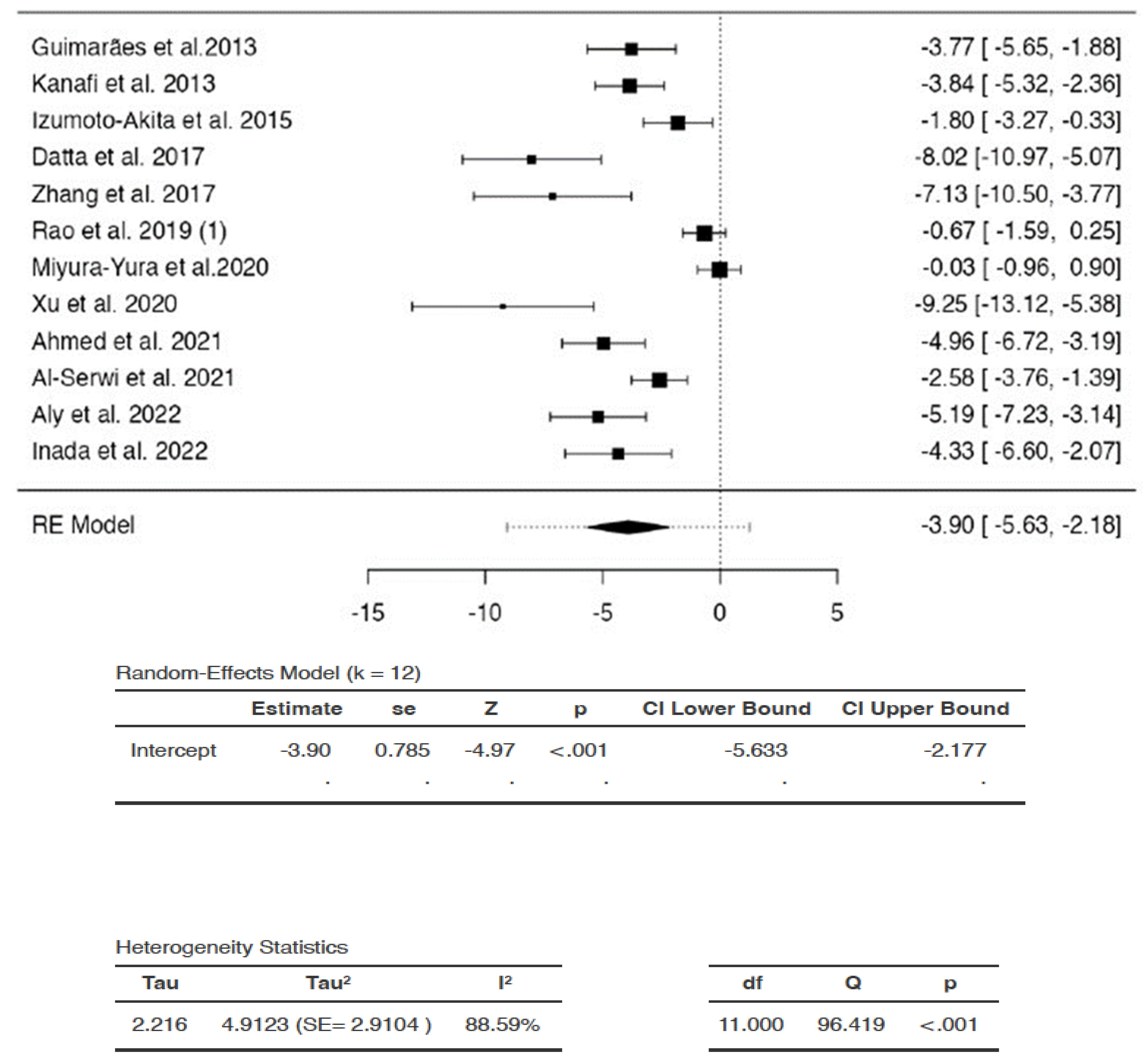
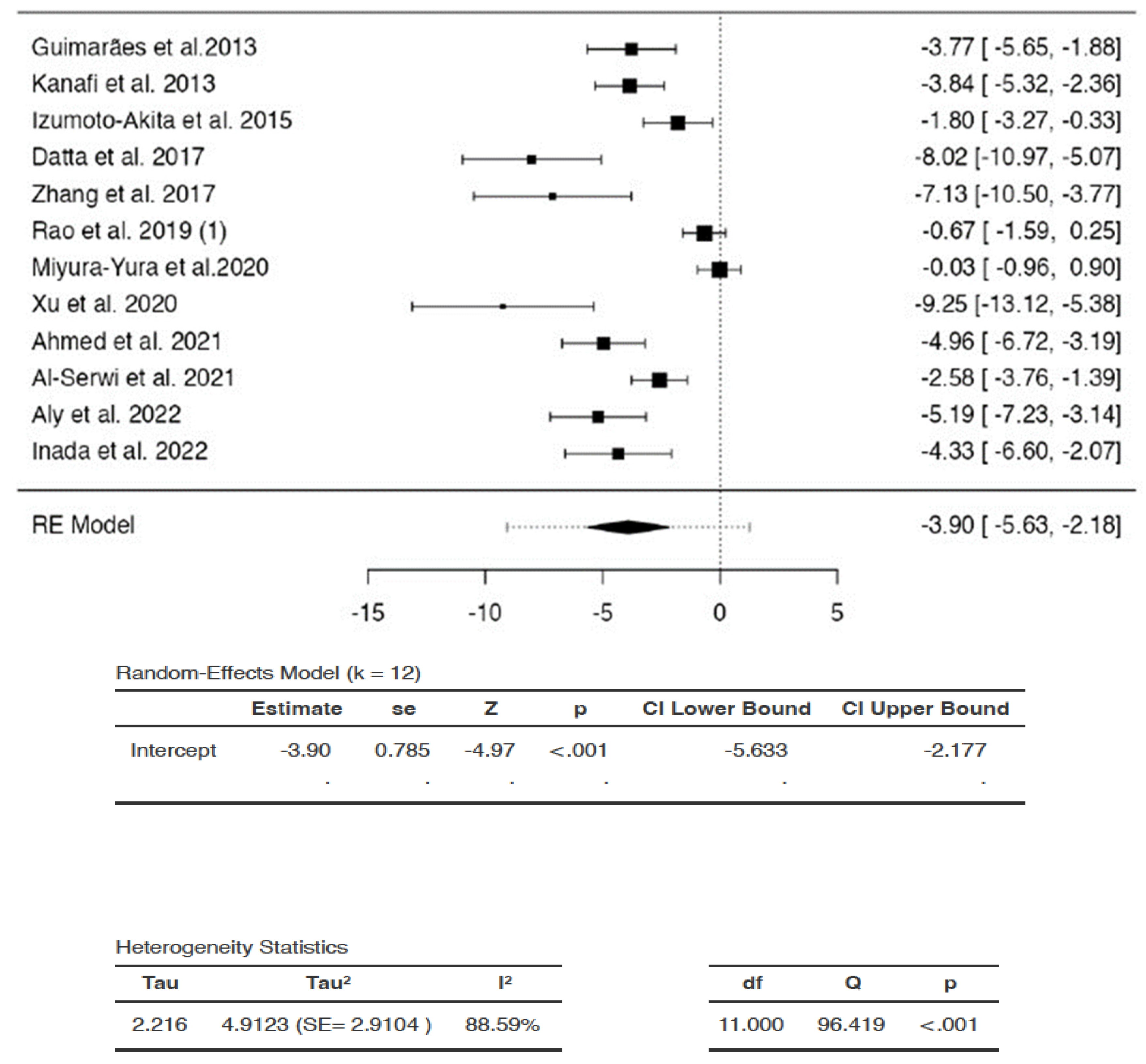
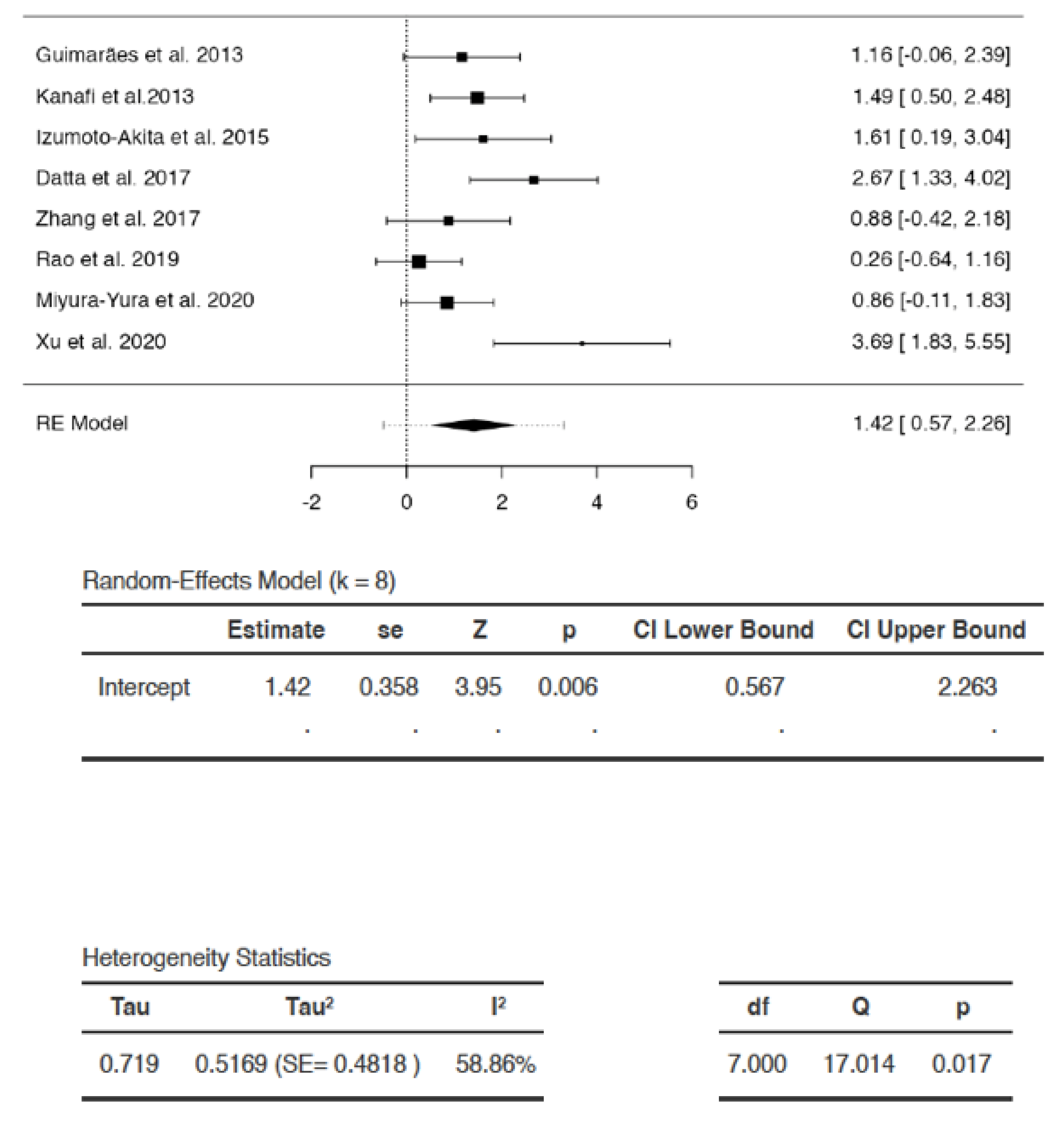
Effect of DSCs on Blood Glucose
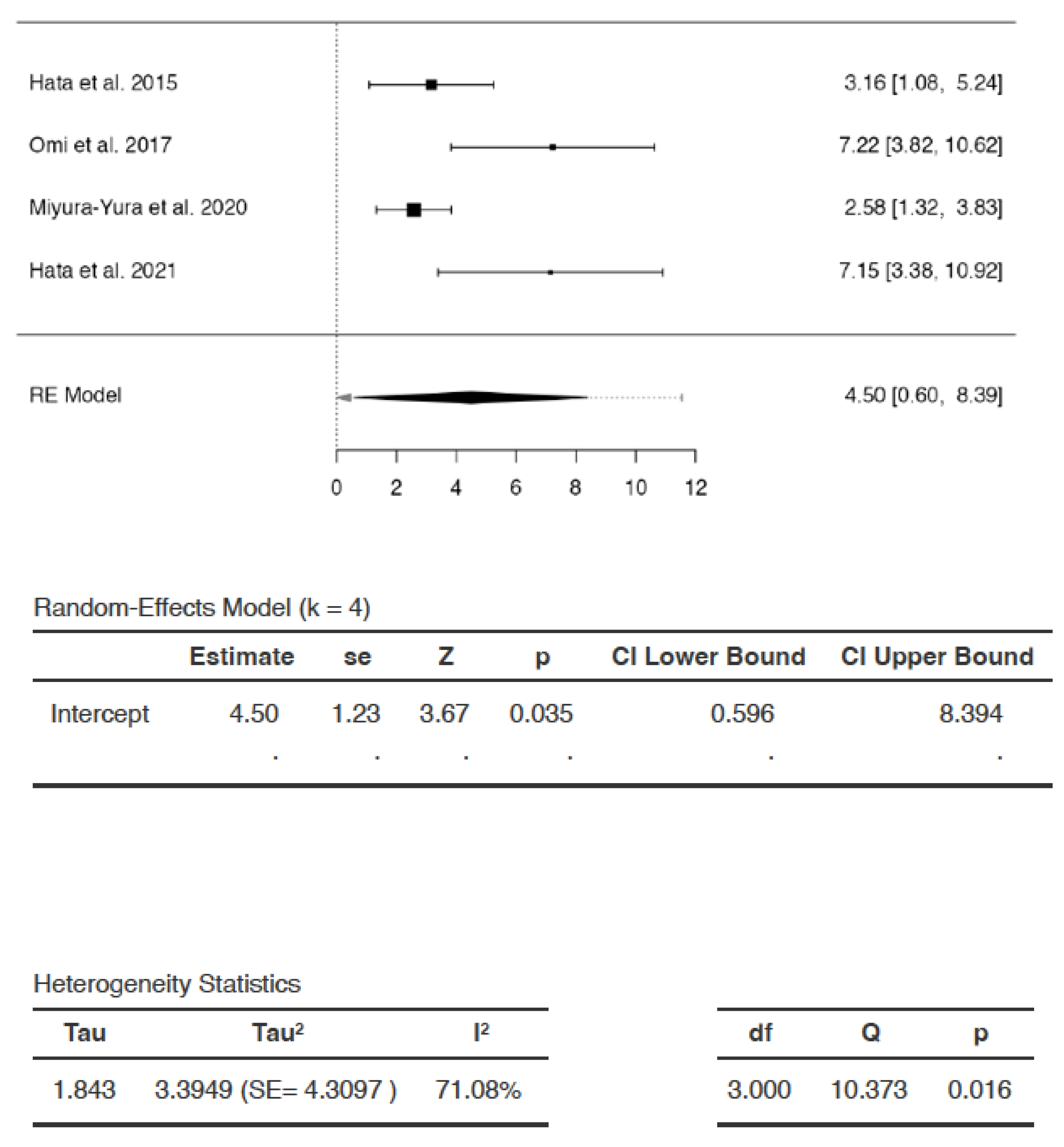
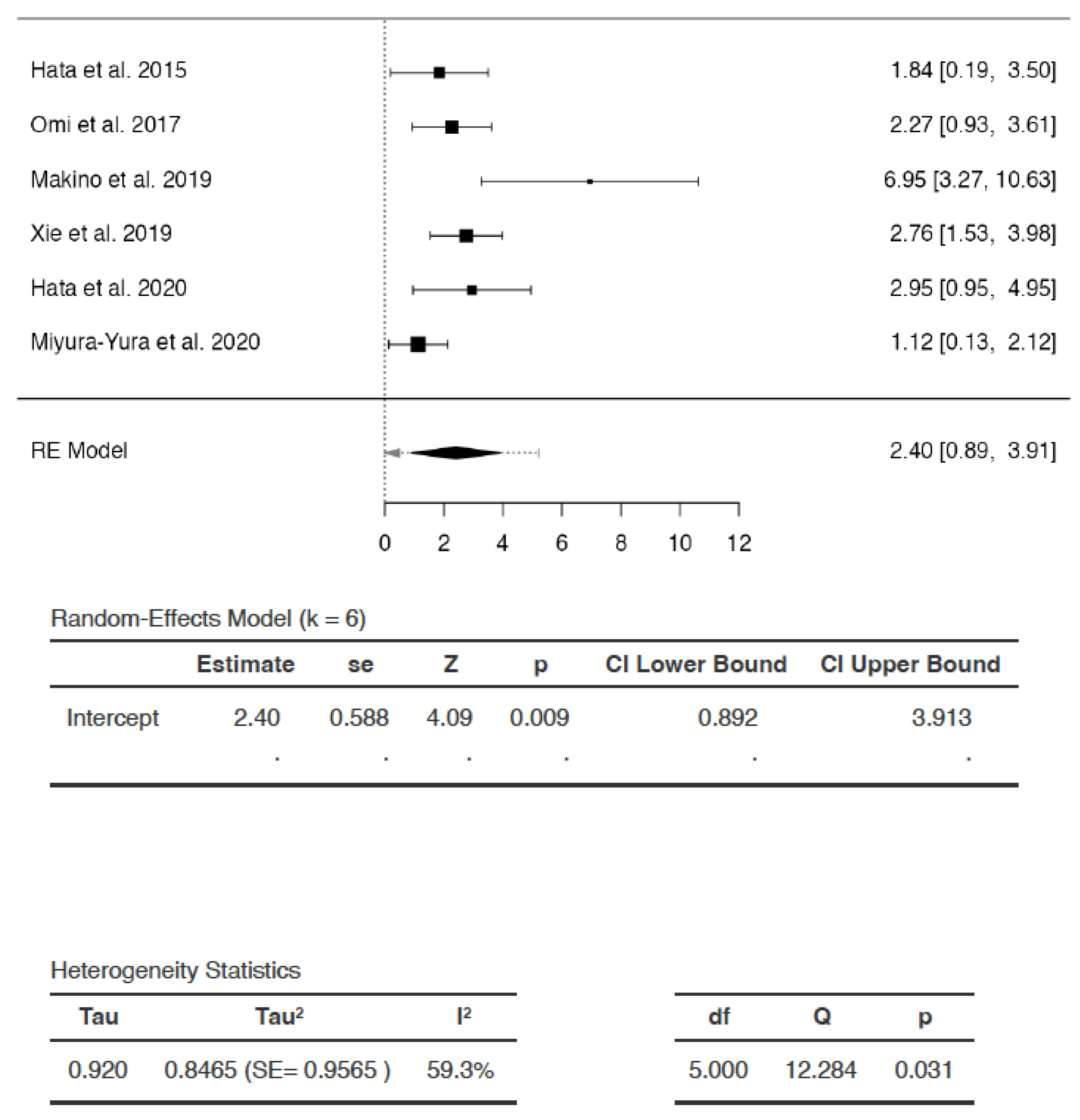
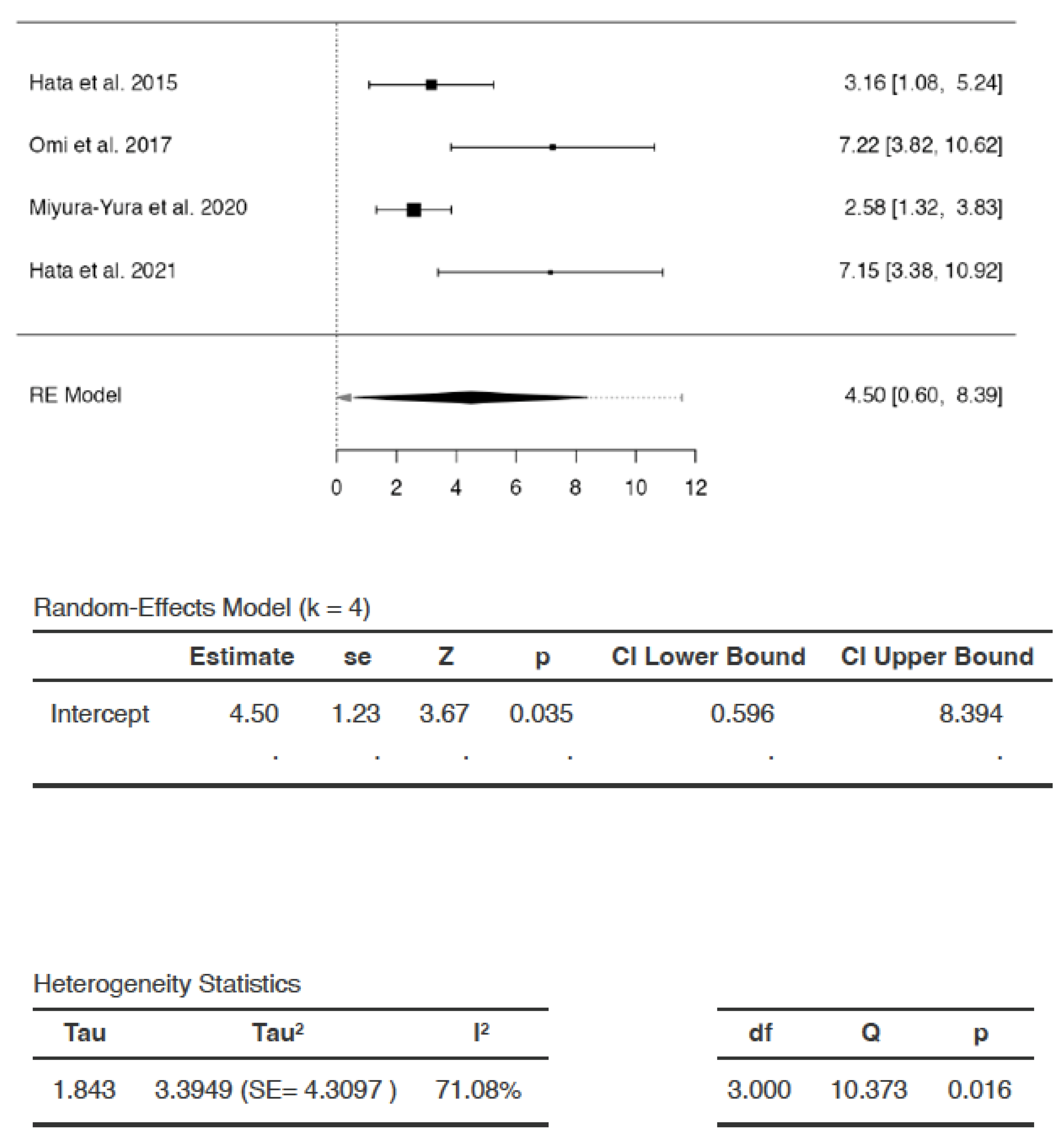
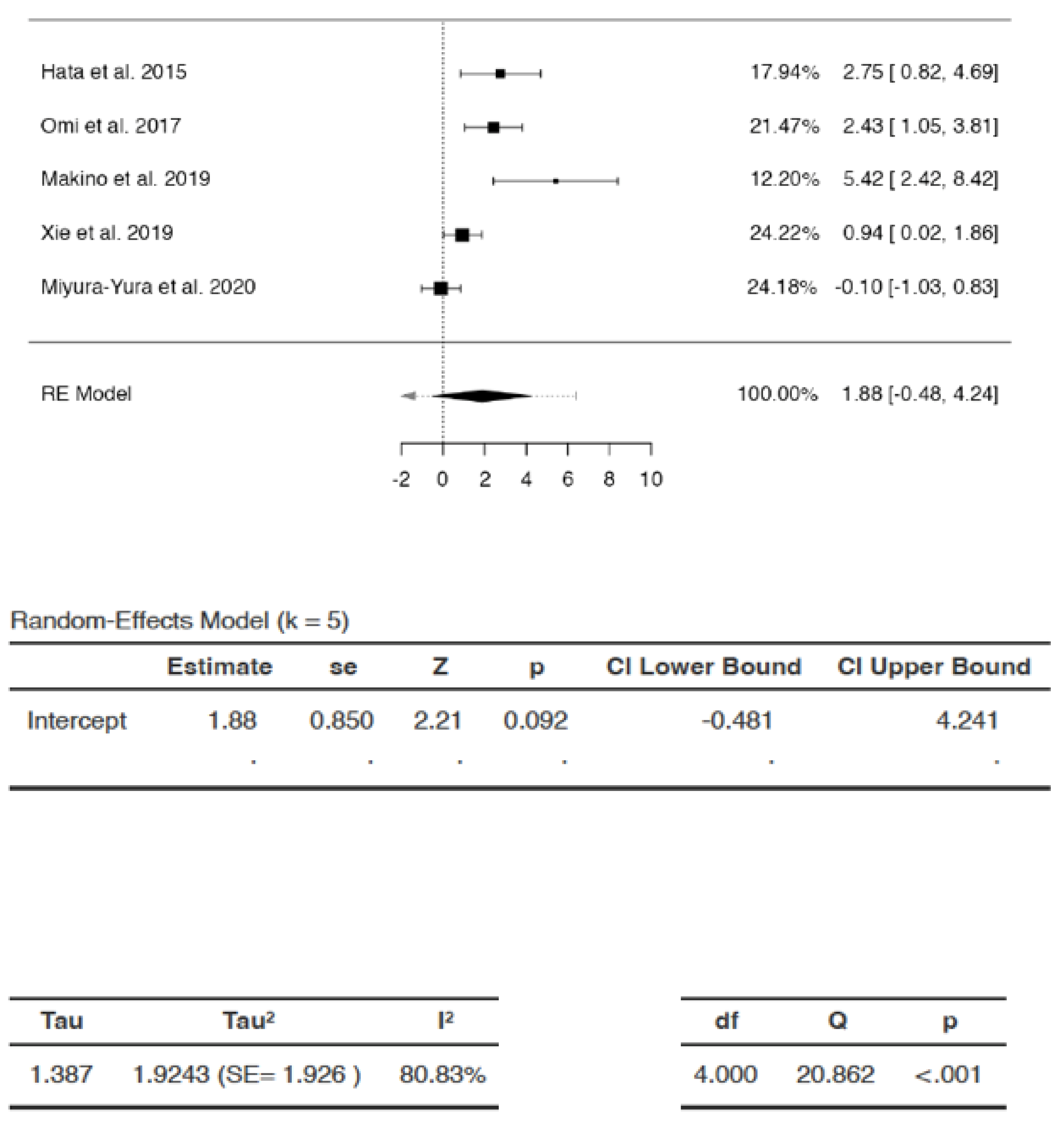
Effects of DSCs on SNCV
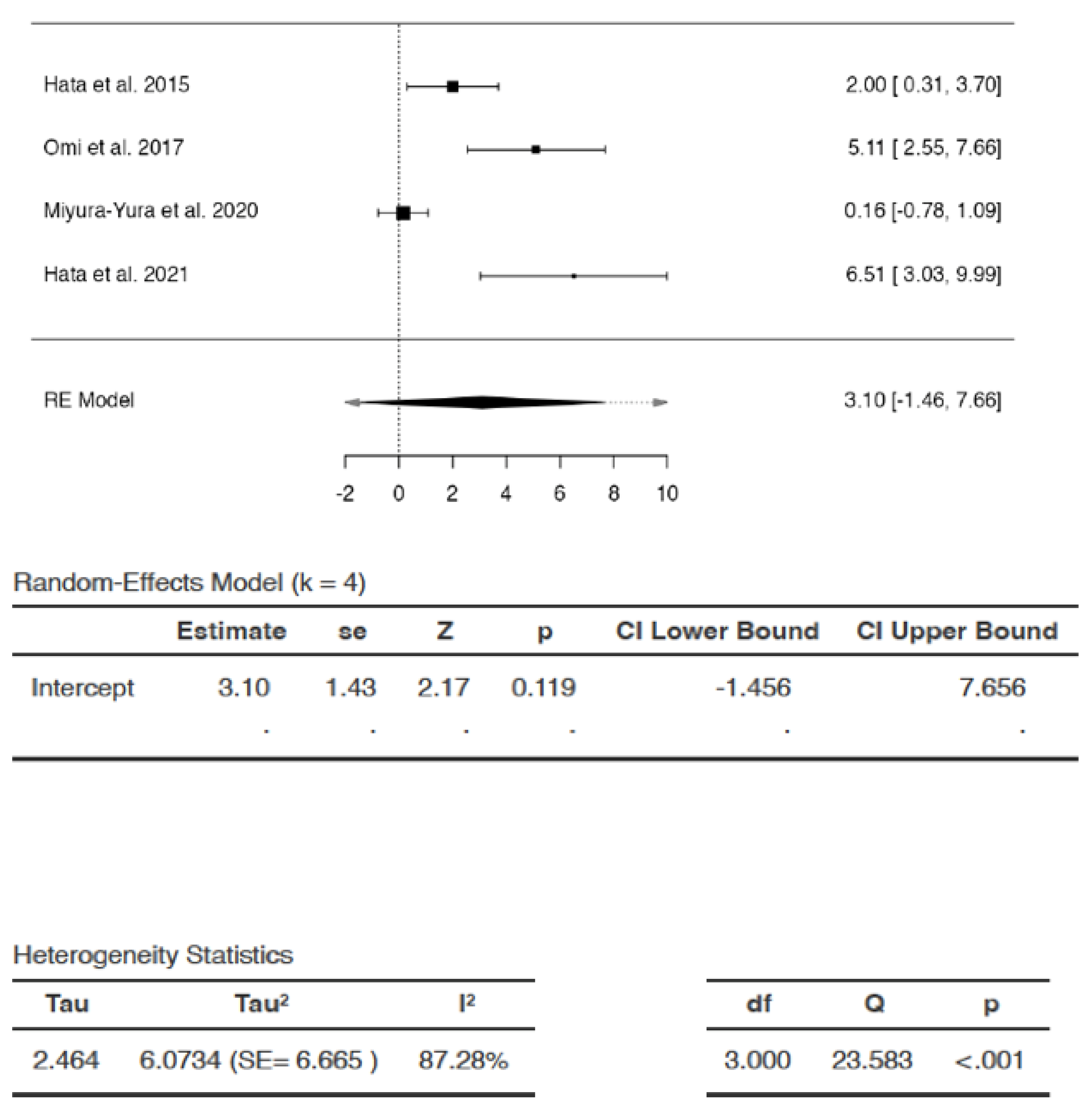
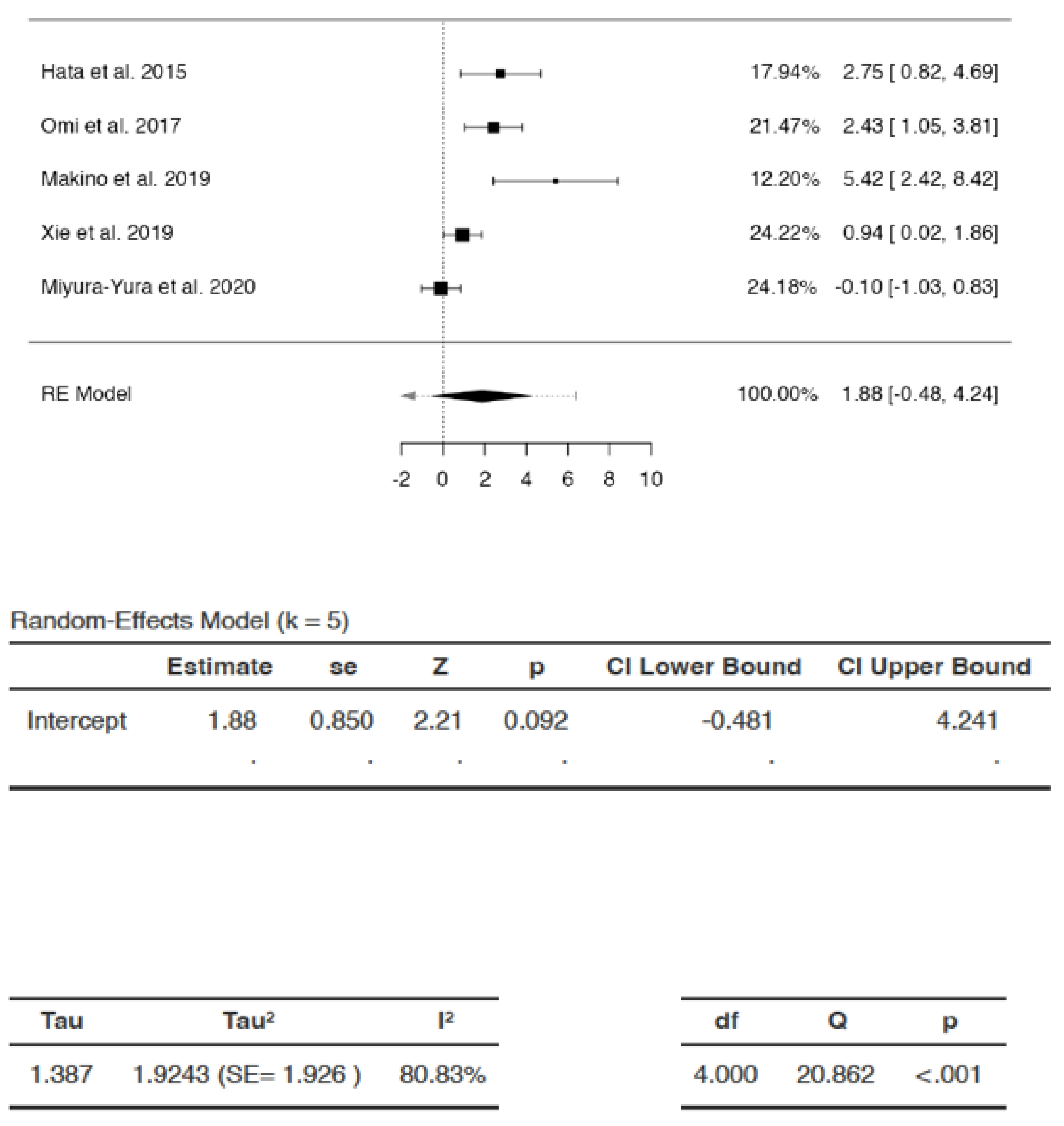
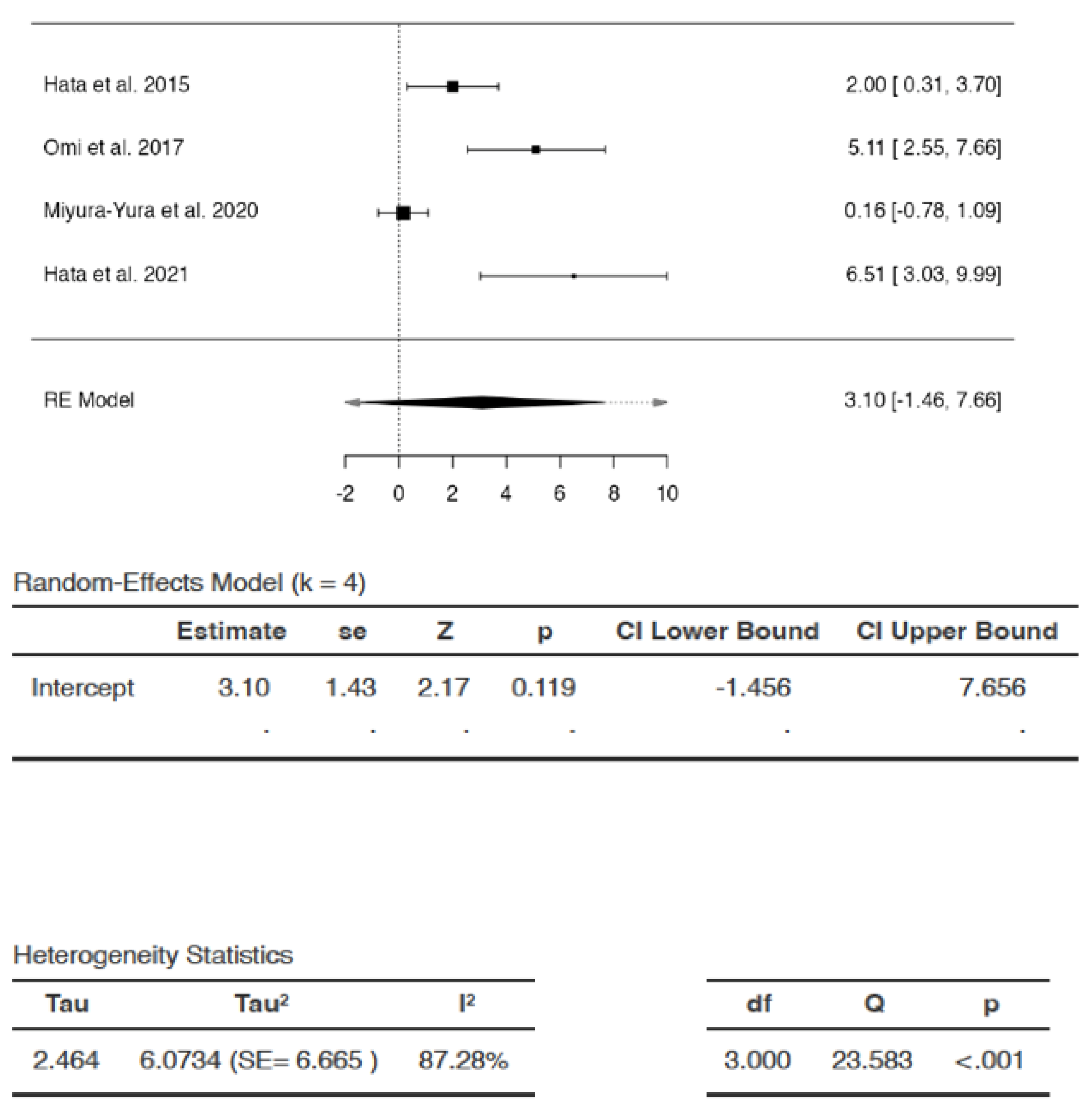
Effects of DSCs on MNCV
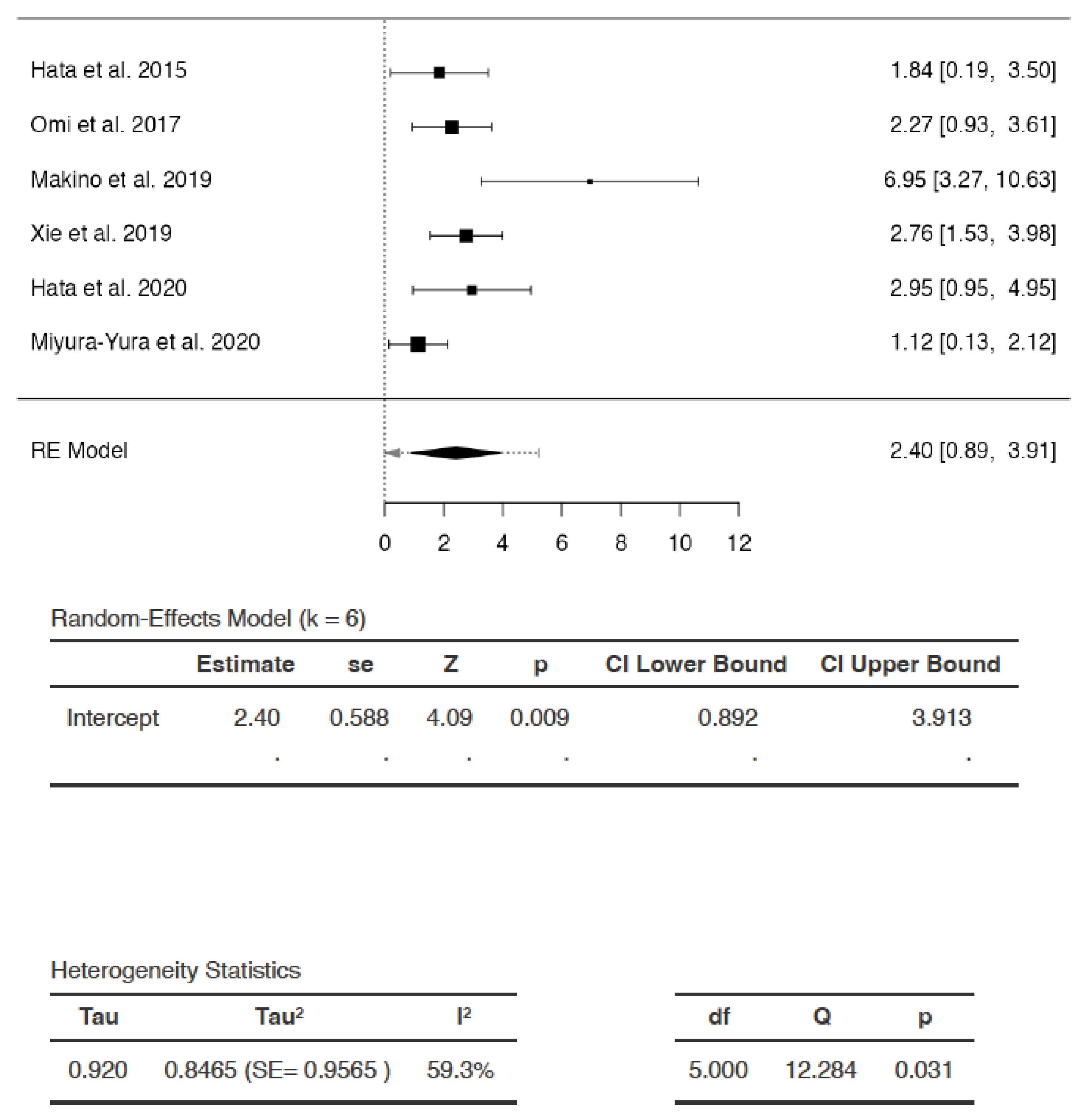
Effects of DSCs on Capillary–Muscle Ratio
Effects of DSCs on IENFD
Effect of DSCs on Body Weight
3.7.2. Subgroup Analysis
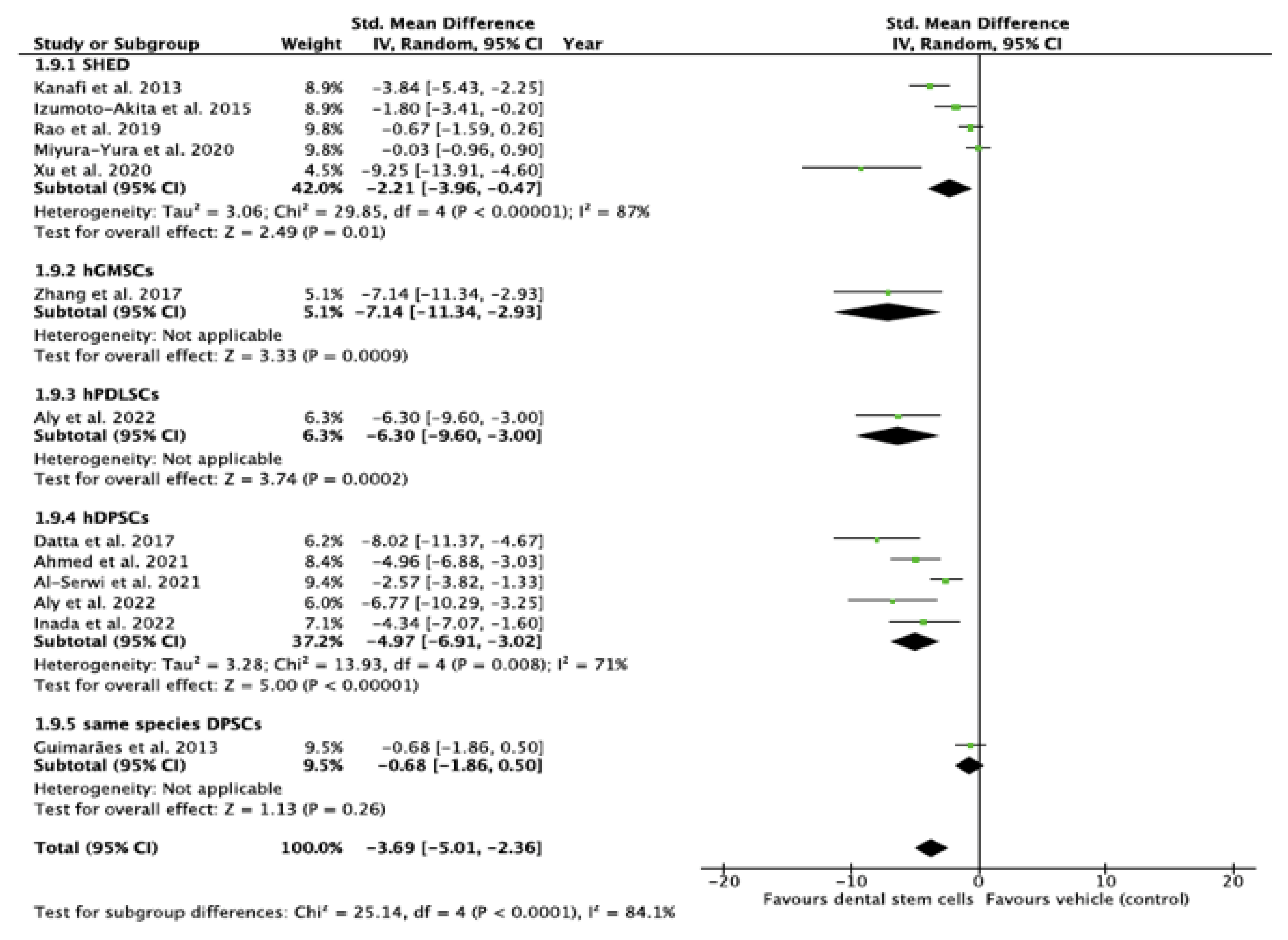
Subgroup Analysis of the Effect of DSC Type Used in the Study
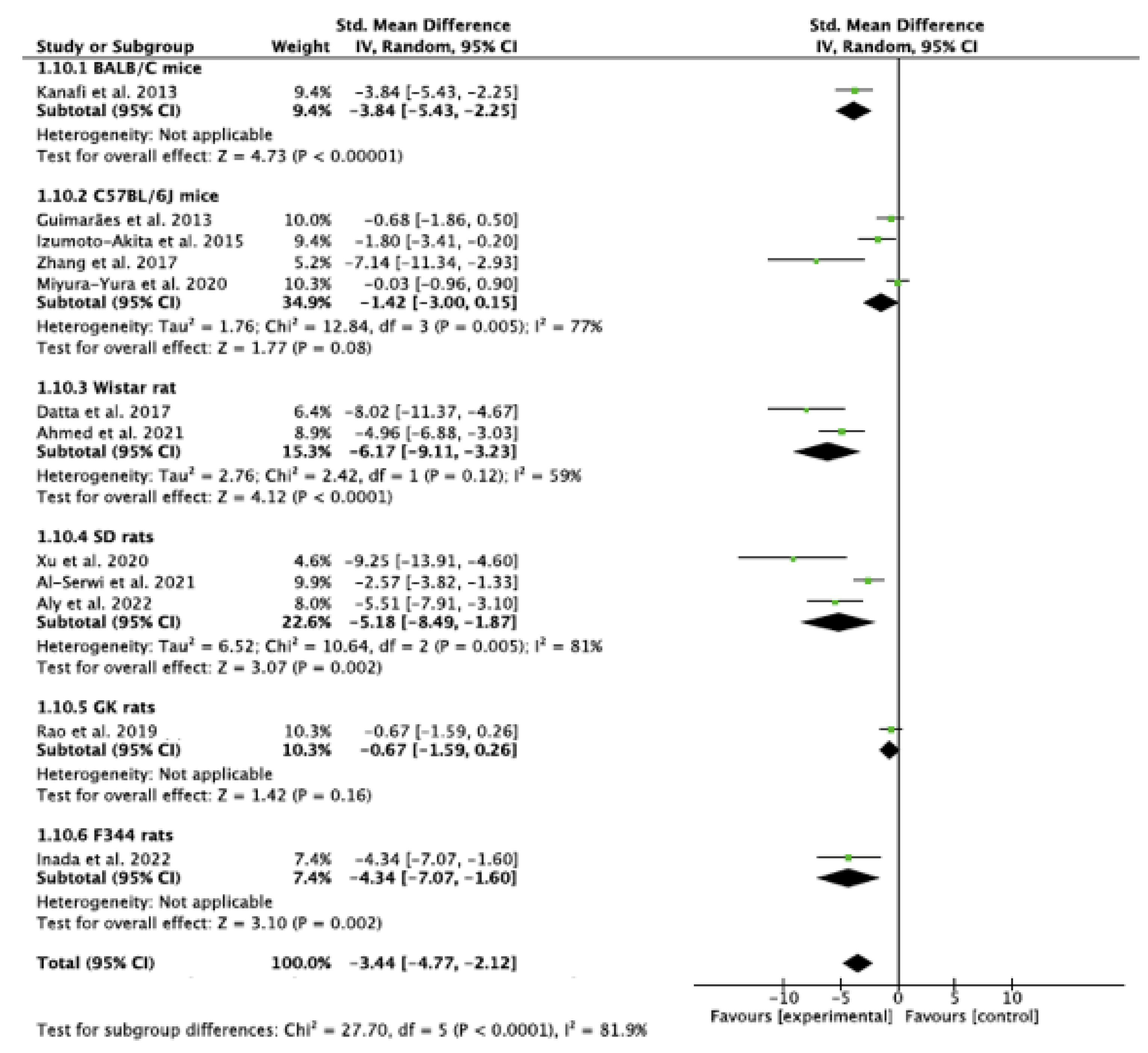
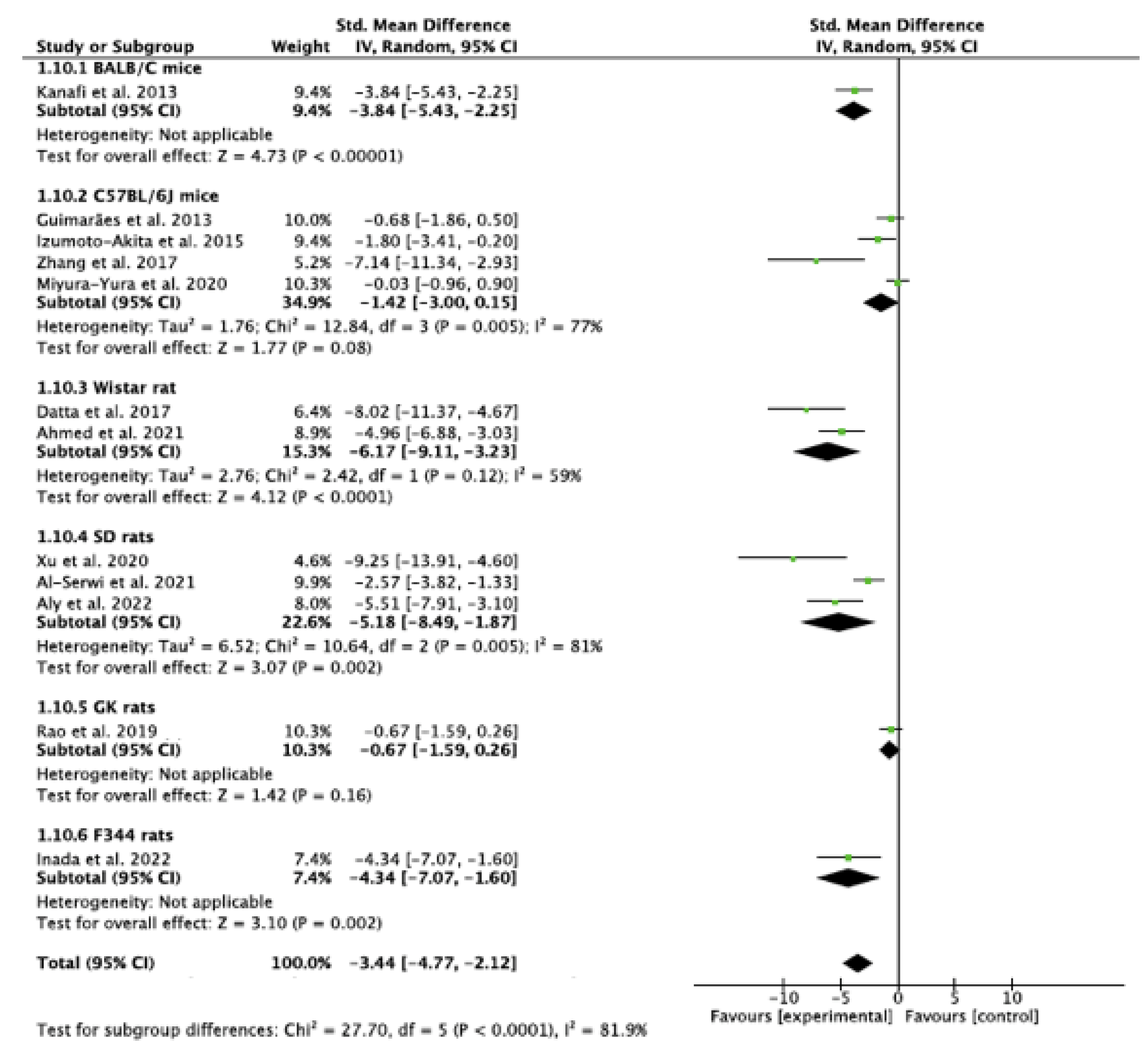
Subgroup Analysis of the Effect of Species Variations
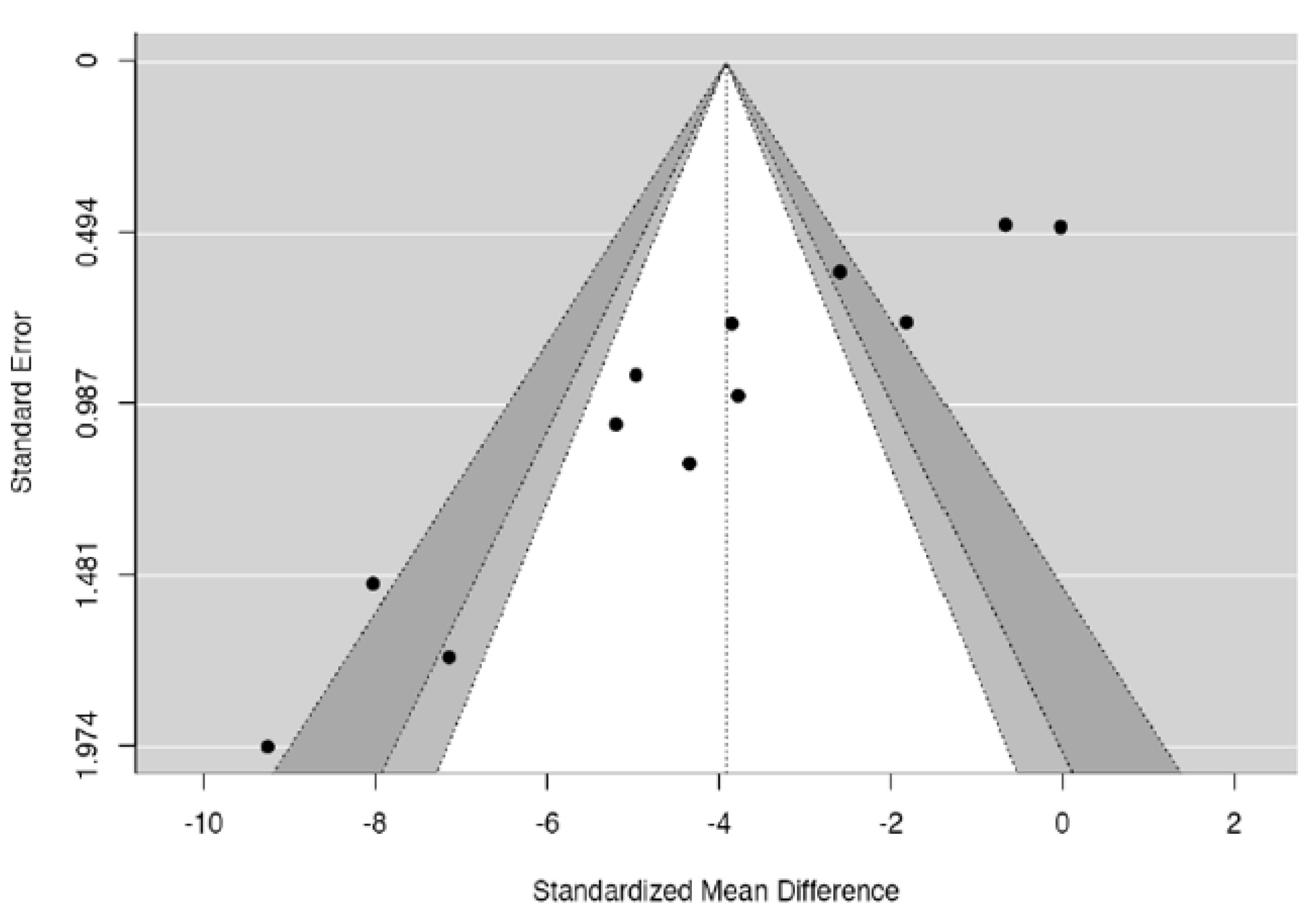
3.7.3. Funnel Plot Analysis and Publication Bias
4. Discussion
4.1. Scope of Translation of Dental Stem Cell-Based Therapy in Diabetes Mellitus
4.2. Publication Bias
4.3. Graft Rejection, Tumorigenesis, and Other Adverse Reactions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomas, E.D.; Lochte, H.L., Jr.; Lu, W.C.; Ferrebee, J.W. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957, 257, 491–496. [Google Scholar] [CrossRef]
- Henig, I.; Zuckerman, T. Hematopoietic stem cell transplantation—50 years of evolution and future perspectives. Rambam Maimonides Med. J. 2014, 5, e0028. [Google Scholar] [CrossRef]
- Friedenstein, A.J.; Petrakova, K.V.; Kurolesova, A.I.; Frolova, G.P. Heterotopic of bone marrow. Analysis of precursor cells for osteogenic and hematopoietic tissues. Transplantation 1968, 6, 230–247. [Google Scholar] [CrossRef]
- Caplan, A.I. Mesenchymal Stem Cells. J. Orthop. Res. 1991, 9, 641–650. [Google Scholar] [CrossRef]
- Battiwalla, M.; Hematti, P. Mesenchymal stem cells in hematopoietic stem cell transplantation. Cytotherapy 2009, 11, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Jiao, X.; Song, J.; Sui, B.; Guo, Z.; Zhao, Y.; Li, J.; Shi, S.; Huang, Q. Therapeutic potential of stem cells from human exfoliated deciduous teeth infusion into patients with type 2 diabetes depends on basal lipid levels and Islet function. Stem Cells Transl. Med. 2021, 10, 956–967. [Google Scholar] [CrossRef] [PubMed]
- Kot, M.; Baj-Krzyworzeka, M.; Szatanek, R.; Musiał-Wysocka, A.; Suda-Szczurek, M.; Majka, M. The Importance of HLA Assessment in “Off-the-Shelf” Allogeneic Mesenchymal Stem Cells Based-Therapies. Int. J. Mol. Sci. 2019, 20, 5680. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.T.-J.; Gronthos, S.; Shi, S. Mesenchymal stem cells derived from dental tissues vs. those from other sources: Their biology and role in regenerative medicine. J. Dent. Res. 2009, 88, 792–806. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhou, L.; Dang, J.; Zhang, X.; Wang, J.; Chen, Y.; Liang, J.; Li, D.; Ma, J.; Yuan, J.; et al. Human gingiva-derived mesenchymal stem cells ameliorate streptozoticin-induced T1DM in mice via suppression of T effector cells and up-regulating Treg subsets. Sci. Rep. 2017, 7, 15249. [Google Scholar] [CrossRef] [PubMed]
- Crotty, S. A brief history of T cell help to B cells. Nat. Rev. Immunol. 2015, 15, 185–189. [Google Scholar] [CrossRef]
- International Diabetes Federation. Diabetes Factors and Figures. 2021. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 9 July 2023).
- King, A.J. The use of animal models in diabetes research. Br. J. Pharmacol. 2012, 166, 877–894. [Google Scholar] [CrossRef] [PubMed]
- Omi, M.; Hata, M.; Nakamura, N.; Miyabe, M.; Ozawa, S.; Nukada, H.; Tsukamoto, M.; Sango, K.; Himeno, T.; Kamiya, H.; et al. Transplantation of dental pulp stem cells improves long-term diabetic polyneuropathy together with improvement of nerve morphometrical evaluation. Stem Cell Res. Ther. 2017, 8, 279. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Rao, N.; Zhai, Y.; Li, J.; Zhao, Y.; Ge, L.; Wang, Y. Therapeutic effects of stem cells from human exfoliated deciduous teeth on diabetic peripheral neuropathy. Diabetol. Metab. Syndr. 2019, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Yasujima, M.; Yagihashi, S. Role of advanced glycation end products in diabetic neuropathy. Curr. Pharm. Des. 2008, 14, 953–961. [Google Scholar] [CrossRef]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diabetes Rep. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Datta, I.; Bhadri, N.; Shahani, P.; Majumdar, D.; Sowmithra, S.; Razdan, R.; Bhonde, R. Functional recovery upon human dental pulp stem cell transplantation in a diabetic neuropathy rat model. Cytotherapy 2017, 19, 1208–1224. [Google Scholar] [CrossRef]
- Honda, M.J.; Imaizumi, M.; Tsuchiya, S.; Morsceck, C. Dental follicle stem cells and tissue enjineering. J. Oral Sci. 2010, 52, 541–552. [Google Scholar] [CrossRef]
- Govindasamy, V.; Ronald, V.; Abdullah, A.; Nathan, K.G.; Aziz, Z.A.; Abdullah, M.; Musa, S.; Abu Kasim, N.; Bhonde, R. Differentiation of dental pulp stem cells into islet-like aggregates. J. Dent. Res. 2011, 90, 646–652. [Google Scholar] [CrossRef]
- Wu, W.; Zhou, J.; Xu, C.-T.; Zhang, J.; Jin, Y.-J.; Sun, G.-L. Derivation and growth characteristics of dental pulp stem cells from patients of different ages. Mol. Med. Rep. 2015, 12, 5127–5134. [Google Scholar] [CrossRef]
- Shi, X.; Mao, J.; Liu, Y. Pulp stem cells derived from human permanent and deciduous teeth: Biological characteristics and therapeutic applications. Stem Cells Transl. Med. 2020, 9, 445–464. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. Available online: http://www.prisma-statement.org/ (accessed on 7 June 2023). [CrossRef] [PubMed]
- Hooijmans, C.R.; Tillema, A.; Leenaars, M.; Ritskes-Hoitinga, M. Enhancing search efficiency by means of a search filter for finding all studies on animal experimentation in PubMed. Lab. Anim. 2010, 44, 170–175. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.M.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Review Manager (RevMan), Version 5.4; The Cochrane Collaboration: London, UK, 2020.
- The Jamovi Project. Jamovi [Computer Program]. Version 2.3. 2021. Available online: http://www.jamovi.org (accessed on 1 January 2020).
- Deeks, J.; Higgins, J.P.T.; Altman, D.G.; on be half of the Cochrane Statistical Methods Group. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for SystematicReviews for Interventions Version 6.4; Cochrane: London, UK, 2023. [Google Scholar]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Hedges, L.V., Ed.; Academic Press: Cambridge, MA, USA, 1985. [Google Scholar]
- Hedges, L.V. Distrubution theory for Glass’ Estimator of effect sizes and related estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Neyman, J. On the problem of confidence intervals. Ann. Math. Stat. 1935, 6, 111–116. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Knapp, G.; Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 2003, 22, 2693–2710. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Skipa, G. The inclusion of the estimated inter-study variation into forest plots for random effects meta analysis a suggestion for a graphical representation (abstract). In Proceedings of the XIV Cochrane Colloquium, Program and Abstract Book, Dublin, Ireland, 23–26 October 2006; p. 134. [Google Scholar]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef]
- Pope, A.J. The Statistics of Residuals and the Detection of Outliers; U.S. Dept. of Commerce, National Oceanic and Atmospheric Administration, National Ocean Survey, Geodetic Research and Development Laboratory: Miami, FL, USA, 1976; 136p. [Google Scholar]
- Dunn, O.J. Multiple comparisons among means. J. Am. Stat. Assoc. 1961, 56, 52–64. [Google Scholar] [CrossRef]
- Cook, R.D. Detection of Influential Observation in Linear Regression. Technometrics 1977, 19, 15. [Google Scholar] [CrossRef]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Featherstone, R.; Littlewood, A.; Metzendorf, M.I.; Noel-Storr, A.; Paynter, R.; Rader, T.; Thomas, J.; et al. Chapter 4. Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4; Cochrane: London, UK, 2023; Available online: https://www.training.cochrane.org/handbook (accessed on 1 August 2023).
- Higgins, J.P.T.; Eldridge, S.; Li, T. Chapter 23. Including variants on randomized trials. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4; (updated August 2023); Cochrane: London, UK, 2023; Available online: https://www.training.cochrane.org/handbook (accessed on 1 August 2023).
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin. Epidemiol. Glob. Health 2019, 7, 192–198. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis, 2nd ed.; John Wiley & Sons: Chichester, UK, 2009. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Hata, M.; Omi, M.; Kobayashi, Y.; Nakamura, N.; Tosaki, T.; Miyabe, M.; Kojima, N.; Kubo, K.; Ozawa, S.; Maeda, H.; et al. Transplantation of cultured dental pulp stem cells into the skeletal muscles ameliorated diabetic polyneuropathy: Therapeutic plausibility of freshly isolated and cryopreserved dental pulp stem cells. Stem Cell Res. Ther. 2015, 6, 162. [Google Scholar] [CrossRef]
- Omi, M.; Hata, M.; Nakamura, N.; Miyabe, M.; Kobayashi, Y.; Kamiya, H.; Nakamura, J.; Ozawa, S.; Tanaka, Y.; Takebe, J.; et al. Transplantation of dental pulp stem cells suppressed inflammation in sciatic nerves by promoting macrophage polarization towards anti-inflammation phenotypes and ameliorated diabetic polyneuropathy. J. Diabetes Investig. 2016, 7, 485–496. [Google Scholar] [CrossRef]
- Hata, M.; Omi, M.; Kobayashi, Y.; Nakamura, N.; Miyabe, M.; Ito, M.; Ohno, T.; Imanishi, Y.; Himeno, T.; Kamiya, H.; et al. Sustainable Effects of Human Dental Pulp Stem Cell Transplantation on Diabetic Polyneuropathy in Streptozotocine-Induced Type 1 Diabetes Model Mice. Cells 2021, 10, 2473. [Google Scholar] [CrossRef] [PubMed]
- Hata, M.; Omi, M.; Kobayashi, Y.; Nakamura, N.; Miyabe, M.; Ito, M.; Makino, E.; Kanada, S.; Saiki, T.; Ohno, T.; et al. Transplantation of human dental pulp stem cells ameliorates diabetic polyneuropathy in streptozotocin-induced diabetic nude mice: The role of angiogenic and neurotrophic factors. Stem Cell Res. Ther. 2020, 11, 236. [Google Scholar] [CrossRef] [PubMed]
- Miura-Yura, E.; Tsunekawa, S.; Naruse, K.; Nakamura, N.; Motegi, M.; Nakai-Shimoda, H.; Asano, S.; Kato, M.; Yamada, Y.; Izumoto-Akita, T.; et al. Secreted factors from cultured dental pulp stem cells promoted neurite outgrowth of dorsal root ganglion neurons and ameliorated neural functions in streptozotocin-induced diabetic mice. J. Diabetes Investig. 2020, 11, 28–38. [Google Scholar] [CrossRef]
- Izumoto-Akita, T.; Tsunekawa, S.; Yamamoto, A.; Uenishi, E.; Ishikawa, K.; Ogata, H.; Iida, A.; Ikeniwa, M.; Hosokawa, K.; Niwa, Y.; et al. Secreted factors from dental pulp stem cells improve glucose intolerance in streptozotocin-induced diabetic mice by increasing pancreatic β-cell function. BMJ Open Diabetes Res. Care 2015, 3, e000128. [Google Scholar] [CrossRef] [PubMed]
- Makino, E.; Nakamura, N.; Miyabe, M.; Ito, M.; Kanada, S.; Hata, M.; Saiki, T.; Sango, K.; Kamiya, H.; Nakamura, J.; et al. Conditioned media from dental pulp stem cells improved diabetic polyneuropathy through anti-inflammatory, neuroprotective and angiogenic actions: Cell-free regenerative medicine for diabetic polyneuropathy. J. Diabetes Investig. 2019, 10, 1199–1208. [Google Scholar] [CrossRef]
- Kanada, S.; Makino, E.; Nakamura, N.; Miyabe, M.; Ito, M.; Hata, M.; Yamauchi, T.; Sawada, N.; Kondo, S.; Saiki, T.; et al. Direct Comparison of Therapeutic Effects on Diabetic Polyneuropathy between Transplantation of Dental Pulp Stem Cells and Administration of Dental Pulp Stem Cell-Secreted Factors. Int. J. Mol. Sci. 2020, 21, 6064. [Google Scholar] [CrossRef] [PubMed]
- Inada, R.; Mendoza, H.Y.; Tanaka, T.; Horie, T.; Satomi, T. Preclinical study for the treatment of diabetes mellitus using β-like cells derived from human dental pulp stem cells. Regen. Med. 2022, 17, 905–913. [Google Scholar] [CrossRef]
- Rao, N.; Wang, X.; Xie, J.; Li, J.; Zhai, Y.; Li, X.; Fang, T.; Wang, Y.; Zhao, Y.; Ge, L. Stem Cells from Human Exfoliated Deciduous Teeth Ameliorate Diabetic Nephropathy In Vivo and In Vitro by Inhibiting Advanced Glycation End Product-Activated Epithelial-Mesenchymal Transition. Stem Cells Int. 2019, 2019, 2751475. [Google Scholar] [CrossRef] [PubMed]
- Rao, N.; Wang, X.; Zhai, Y.; Li, J.; Xie, J.; Zhao, Y.; Ge, L. Stem cells from human exfoliated deciduous teeth ameliorate type II diabetic mellitus in Goto-Kakizaki rats. Diabetol. Metab. Syndr. 2019, 11, 22. [Google Scholar] [CrossRef]
- Xu, Y.; Chen, J.; Zhou, H.; Wang, J.; Song, J.; Xie, J.; Guo, Q.; Wang, C.; Huang, Q. Effects and mechanism of stem cells from human exfoliated deciduous teeth combined with hyperbaric oxygen therapy in type 2 diabetic rats. Clinics 2020, 75, e1656. [Google Scholar] [CrossRef]
- Al-Serwi, R.H.; El-Khersh, A.O.F.O.; El-Akabawy, G. Human dental pulp stem cells attenuate streptozotocin-induced parotid gland injury in rats. Stem Cell Res. Ther. 2021, 12, 577. [Google Scholar] [CrossRef]
- El-Kersh, A.O.F.O.; El-Akabawy, G.; Al-Serwi, R.H. Transplantation of human dental pulp stem cells in streptozotocin-induced diabetic rats. Anat. Sci. Int. 2020, 95, 523–539. [Google Scholar] [CrossRef]
- 60Ahmed, H.H.; Aglan, H.A.; Mahmoud, N.S.; Aly, R.M. Preconditioned human dental pulp stem cells with Cetrium and yttrium oxide nanoparticles effectively ameliorate diabetes hyperglycemia while combating hypoxia. Tissue Cell 2021, 73, 101661. [Google Scholar]
- Aly, R.M.; Aglan, H.A.; Eldeen, G.N.; Mahmoud, N.S.; Aboul-Ezz, E.H.; Ahmed, H.H. Efficient generation of functional pancreatic β cells from dental-derived stem cells via laminin-induced differentiation. J. Genet. Eng. Biotechnol. 2022, 20, 85. [Google Scholar] [CrossRef]
- Kanafi, M.M.; Rajeshwari, Y.B.; Gupta, S.; Dadheech, N.; Nair, P.D.; Gupta, P.K.; Bhonde, R.R. Transplantation of islet-like cell clusters derived from human dental pulp stem cells restores normoglycemia in diabetic mice. Cytotherapy 2013, 15, 1228–1236. [Google Scholar] [CrossRef]
- Guimarães, E.T.; da Silva Cruz, G.; De Almeida, T.F.; de Freitas Souza, B.S.; Kaneto, C.M.; Vasconcelos, J.F.; Dos Santos, W.L.C.; Ribeiro-Dos-Santos, R.; Villarreal, C.F.; Soares, M.B.P. Transplantation of stem cells obtained from murine dental pulp improves pancreatic damage, renal function, and painful diabetic neuropathy in diabetic type 1 mouse model. Cell Transplant. 2013, 22, 2345–2354. [Google Scholar] [CrossRef]
- Tsai, A.I.; Hong, H.-H.; Lin, W.-R.; Fu, J.-F.; Chang, C.-C.; Wang, I.-K.; Huang, W.-H.; Weng, C.-H.; Hsu, C.-W.; Yen, T.-H. Isolation of Mesenchymal Stem Cells from Human Deciduous Teeth Pulp. BioMed Res. Int. 2017, 2017, 2851906. [Google Scholar] [CrossRef] [PubMed]
- Pound, P.; Ritskes-Hoitinga, M. Is it possible to overcome issues of external validity in preclinical animal research? Why most animal models are bound to fail. J. Transl. Med. 2018, 16, 304. [Google Scholar] [CrossRef]
- van der Worp, H.B.; Howells, D.W.; Sena, E.S.; Porritt, M.J.; Rewell, S.; O’Collins, V.; Macleod, M.R. Can animal models of disease reliably inform human studies? PLoS Med. 2010, 7, e1000245. [Google Scholar] [CrossRef]
- Mitchell, S.J.; Scheibye-Knudsen, M.; Longo, D.L.; de Cabo, R. Animal models of aging research: Implications for human aging and age-related diseases. Annu. Rev. Anim. Biosci. 2015, 3, 283–303. [Google Scholar] [CrossRef]
- Jackson, S.J.; Andrews, N.; Ball, D.; Bellantuono, I.; Gray, J.; Hachoumi, L.; Holmes, A.; Latcham, J.; Petrie, A.; Potter, P.; et al. Does age matter? The impact of rodent age on study outcomes. Lab. Anim. 2017, 51, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Tesch, G.H.; Allen, T.J. Rodent Models of Streptozotocin-Induced Diabetic Nephropathy. Nephrology 2007, 12, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Sui, B.; Xiang, L.; Yan, X.; Wu, D.; Shi, S.; Hu, X. Emerging understanding of apoptosis in mediating mesenchymal stem cell therapy. Cell Death Dis. 2021, 12, 596. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Baust, J.M. Cryopreservation: An emerging paradigm change. Organogenesis 2009, 5, 90–96. [Google Scholar] [CrossRef]
- Gale, E.A.; Gillespie, K.M. Diabetes and gender. Diabetologia 2001, 44, 3–15. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, R.; Fried, M.W.; Sallie, R.; Conjeevaram, H.; Di Bisceglie, A.M.; Park, Y.; Savarese, B.; Kleiner, D.; Tsokos, M.; Luciano, C.; et al. Hepatic Failure and Lactic Acidosis Due to Fialuridine (FIAU), an Investigational Nucleoside Analogue for Chronic Hepatitis B. N. Engl. J. Med. 1995, 333, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Lontchi-Yimagou, E.; Sobngwi, E.; Matsha, T.E.; Kengne, A.P. Diabetes mellitus and inflammation. Curr. Diabetes Rep. 2013, 13, 435–444. [Google Scholar] [CrossRef]
- Hentze, H.; Soong, P.L.; Wang, S.T.; Phillips, B.W.; Putti, T.C.; Dunn, N.R. Teratoma formation by human embryonic stem cells: Evaluation of essential parameters for future safety studies. Stem Cell Res. 2009, 2, 198–210. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Animal Used in Study/ Method of Disease Induction/Source of Stem Cells | Age of Animal at Start of Experiment | Time of Sacrifice | Route/Mode of Stem Cell Administration | Parameters Assessed | Results | Additional Comments |
|---|---|---|---|---|---|---|---|
| SUBSET 1 Stem cells from human exfoliated deciduous teeth (SHED) | |||||||
| Kanafi et al., 2013 [62] | Male BALB/c mice. T1DM was induced by intraperitoneal dose of STZ. SHED from deciduous teeth. Dental pulp stem cells (DPSCs) from extracted teeth of human adults for in vitro experiments. | 6–8 weeks old. | 10 weeks after transplantation of islet-like cell clusters (ICCs) from SHED; 2 weeks after graft removal. | Subcutaneous (SC) transplantation of macro capsules. 8 weeks following transplantation, macro capsules were removed to assess effect of removal. 1000 SHED cells packed in each macro capsule. | In vitro: flow cytometry following isolation of DPSCs and SHED from human teeth; adipogenic and osteogenic differentiation, rate of proliferation, insulin release. Immunohistochemistry, reverse transcriptase polymerase chain reaction. In vivo: blood and urine glucose, body weight (BW) every 48 hours; histopathology of pancreas following sacrifice. | In vitro: Both DPSCs, SHED showed adipogenic and osteogenic differentiation; positive for stromal markers (CD34, CD90 etc.). Proliferative ability greater in SHED than DPSC. Increased expression of insulin on 10th day. In vivo: No graft rejection in any mouse. Diabetic mice with islet-like cell (ICC) transplantation returned to normoglycemia and normal level of glucose in urine by second week of transplantation, which was maintained for 10 weeks after transplantation and 2 weeks after graft removal. BW improved. Morphology of islets of Langerhans cells improved. Diabetic mice without SHED transplantation showed hyperglycemia and reduced BW. | In vitro experiment demonstrated that SHED showed greater differentiation and proliferative ability than DPSCs. In vivo experiment was conducted with ICCs from SHED only. |
| Izumoto-Akita T et al., 2015 [51] | Male C57BL/6J mice induced T1DM by daily intraperitoneal injection of Streptozotocin (STZ) for 5 days,or a single high dose of STZ. SHED from 6–12-year-old patients. Bone marrow mesenchymal stem cells (BMMSCs) from 20–22-year-old patients. | 10 weeks old. | 3 weeks after treatment ended, 5 weeks from 1st STZ dose. | Intravenous (IV) administration of 1 mL twice daily dose of conditioned medium, i.e., SHED-CM (or 1 mL BMMSC-CM or 24 nmol/kg exendin-4 (Ex-4) -type of incretin that reduces glucose and stimulates insulin production) for 5 days during STZ administration; Thereafter, intraperitoneal administration for 9 days (14 days total) or 3 days following a single high dose of STZ. | In vitro: immunofluorescence studies on the effect of SHED-CM on mouse. pancreatic B cells; insulin secretion assay. In vivo: random plasma glucose at the same time every day for 14 days. Intraperitoneal glucose tolerance test (IPGTT) on 27th day after16 h fasting; BW, histopathology of pancreas following sacrifice 3 weeks after treatment. | In vitro: number of necrotic pancreatic cells reduced when treated with SHED-CM; significantly greater effect noted in SHED-CM compared to that of BMMSC-CM and Ex-4. In vivo: random plasma glucose was reduced on 12th day of treatment; IPGTT showed insulin increased in mice treated with SHED-CM. No change in BW. Number of insulin-producing β-cells increased with SHED-CM administration. | Despite the high dose of SHED-CM administered, no hematuria or animal deaths caused by administration were reported to occur. The authors suggested that secreted factors of SHED resulted in fewer complications than transplantation of whole SHED cells and required no immunosuppressive agents. |
| Rao et al., 2019 [55] | Male Goto-Kakizaki (GK) rats. as test group; Male Wistar rats as controls. T2DM induced by high fat diet for 2–4 weeks. SHED from 6–8-year-old patients. BMMSCs from 16–20-year-old patients from bone marrow aspirate following 3rd molar extractions. 6 rats were transplanted with green fluorescence protein (GFP) GFP-SHED or GFP-BMMSCs for cell tracking in kidneys. | 12 weeks old. | For GK rats: 8 weeks after administration of stem cells (i.e., 8–10 weeks from start of experiment); for GFP-SHED and GFP-BMMSC rats: 2, 4, and 8 weeks after administration of SHED or BMMSCs; for Wistar rats: 10 weeks from baseline. | Administered 4 × 106 cells (SHED or BMMSCs) per animal via tail vein. | In vitro: flow cytometry for surface marker profiles; adipogenic and osteogenic differentiation. Effect of SHED and BMMSCs on epithelial— mesenchymal transition (EMT) caused by advanced glycation end products (AGE). In vivo: BW, fasting, and non-fasting glucose every week; serum triglycerides, IL1, IL10, TNF-α, Hepatocyte growth factor (HGF); renal function tests, renal histological and immunohistochemistry following sacrifice. | In vitro: SHED and BMMSCs showed fibroblast-like morphology. Both showed adipogenic and osteogenic differentiation. In vivo: fasting glucose decreased with SHED and BMMSCs; non-fasting reduced at 2 weeks with BMMSCs, and at 2,3, and 7 weeks in SHED group. Serum triglycerides, urinary albumin, and kidney to body weight ratio remained stable with SHED and BMMSCs as compared to diabetic group with no SC treatment. IL1,TNF-α reduced in both the SHED and BMMSC group; IL10, and HGF increased in both groups compared to the no treatment group; improved renal morphology such as reduced glomerulosclerosis and tubular dilatation seen in treatment with both types of SCs. | Results suggest that both BMMSCs and SHED are effective in treating diabetic nephropathy, although SHED appeared to have more sustained long-lasting effects than BMMSCs. Authors attributed the improvement in renal morphology and local inflammation to the local engraftment (homing) of SHED in kidneys. Study used GK rats, a lean Type II DM model characterized by glucose intolerance. |
| └ Rao et al., 2019 [56] | Male GK rats as test group, 8 Male Wistar rats as controls. T2DM induced by high -fat diet. SHED from 6–8- year-old patients. Study does not mention if teeth were carious/infected and extracted. Human BMMSCs from commercially available source. | 12 weeks old. | 8 weeks after SC administration. 12 weeks from start of experiment. | Administered 4 × 106 cells (SHED/BMMSCs) per animal via tail vein. | In vitro: adipogenic and osteogenic differentiation. In vivo: BW, fasting, and non-fasting blood glucose, insulin release test (IRT), homeostatic model assessment for insulin resistance (HOMA-IR). Pancreatic histology and immunohistochemistry. Liver histology and presence of SCs in liver. Quantitative real time (RT-PCR) and Western blotting of liver. | SHED differentiated into adipogenic and osteogenic cells. BW increased during and after treatment but was less than that in normal rats. FBG and non-FBG were less in treatment groups than in PBS group but higher than in normal (non-diabetic) group. No difference b/w SHED and BMMSC groups. HOMA-IR increased in SHED and BMMSC groups. Morphology of pancreatic islet cells improved with SHED as well as BMMSC treatment as compared to vehicle group. Glycogen storage improved in liver with stem cell treatment, whereas in vehicle group, glycogen reduced as compared to normal hepatic cell morphology. PBS group had lower pancreatic beta function values than normal group, which improved in SC groups. SHED and human BMMSCs found in liver in SC groups. RT-PCR showed that T2DM-induced increase in enzymes was reversed with SC administration. | Homing of SCs were found in liver but not in pancreas, suggesting that IV form of administration and impaired liver may cause migration of SCs to distant organs other than the pancreas. Authors suggest that DSCs may cause improvement in parameters by improving B-cell function. |
| Xie et al., 2019 [14] | GK male rats as test group, male Wistar rats as controls. T2DM induced by high-fat diet. Retained deciduous teeth extracted from 6–10 year old patients. | 10 weeks old. | 12 weeks after administration of SHED, about 20 weeks from start of experiment. | 1 × 107 SHED transplanted into caudal vein by IV infusion, and repeated once after 2 weeks. | In vitro: flow cytometry for surface markers; differentiation into multiple cell lineage. In vivo: mechanical hyperalgesia by calculating Paw Withdrawal Mechanical Threshold (PWMT) using Dixon’s up and down method and Von Frey hairs (VFH) on hind paw; capillary- muscle ratio in soleus muscle, intra-epidermal fiber density (IENFD) in foot pads. Protein expression in skeletal muscle after sacrifice. | In vitro: lack of CD45 surface marker (characteristic of hematopoietic cells), differentiated into osteoblasts, chondroblasts, and odontoblasts. In vivo: SHED found around skeletal muscle bundles. PWMT values increased after 6 weeks in SHED group and were sustained for 2 weeks thereafter; IENFD and morphology of sciatic nerve fibers improved; increase in skeletal muscle capillary density with SHED treatment compared to saline administration group. | Source of stem cells were extracted deciduous teeth. Authors attributed amelioration of diabetic neuropathy to IV infusion for successful homing in skeletal muscles. |
| Miyura- Yura et al., 2020 [50] | Male C57BL/6 Mice. Induced T1DM by 150 mg/kg intraperitoneal injection of STZ. SHED from 6–12 -year-old patients. | 5 weeks old for induced DM study. Dorsal root ganglions from healthy 4–6-week-old mice. | 4 weeks after SHED-CM treatment, 16 weeks after induction of DM. | 100 μL SHED-CM administered into unilateral soleus muscle 12 weeks after DM induction, twice a week for 4 weeks. | In vitro: neurite outgrowth in dorsal root ganglion of mice; SHED effect on cell viability of human umbilical vein endothelial cells (HUVECs from cell bank). In vivo: BW, blood glucose; thermal plantar test, motor and sensory nerve conduction velocity (MNCV, SNCV), intra-epidermal nerve fiber ratio (IENFD), blood flow sciatic nerve (SNBF), capillary -muscle fiber ratio. | Dorsal root ganglion neurites were longer with SHED in vitro. SHED-CM did not affect glucose levels or body weight of diabetic mice. Von Frey tests showed that thermal sensitivity did not reduce with SHED-CM. SNCV was ameliorated, but MNCV, IENFD did not improve with SHED-CM. SHED-CM increased capillary-muscle density ratio and improved blood flow in treated side as compared to untreated side of diabetic mice. | Study suggests soluble factors from SHED caused neurite outgrowths, increased number of capillaries, and blood flow in skeletal muscle, which improved neural function. Treatment with SHED started after 12 weeks of DM with advanced stages of neuropathy, resulting in no improvement in thermal sensitivity, MNCV and IENFD, indicating that early intervention might be more effective. Study suggests that stem cells may not be as effective in animals of a different species. |
| Xu et al., 2020 [57] | Male Sprague Dawley (SD) rats. T2DM was induced in rats which were fed with high-fat diet for 8 weeks, and then administered with a single intraperitoneal dose of STZ. Rats were divided into five groups: stem cell therapy only (SC); stem cells and hyperbaric oxygen (SC+ HBO); hyperbaric oxygen only (HBO); diabetic control group (DM); and non-diabetic normal rats (NC). | Age of rats at start of experiment was unclear. | 6 weeks after treatment with either SHED or hyperbaric oxygen (HBO) or combined SHED and HBO treatment. | Rats administered 0.5 mL SHED through caudal veins in first and third week after induction of T2DM. Fourth group consisted of normal rats on a normal diet. Rats in normal control and HBO groups were transfused with equal volumes of sodium chloride. HBO treatment with pure oxygen administered for 1 hour daily for 28 days to rats in HBO or combined SC and HBO groups. | BW, blood glucose serum insulin, HOMA-IR, serum lipid panel. Insulin and glucagon in pancreatic islets following treatment. Inflammation; apoptosis in pancreatic cells. Mental state of rats. | Frequency of urination reduced, BW increased in SC+HBO and SC groups. Blood glucose reduced and serum insulin increased in SC+HBO and SC groups. Serum LDL, serum TNF-alpha reduced in these groups as compared to DM control group. Inflammation and apoptosis was reduced in pancreatic cells in SC+HBO and SC groups. Mental state of rats was better in SC+HBO and SC groups than in DM groups. | Study showed that SHED caused a decrease in serum lipids, and the change was demonstrated to be earlier in combination with HBO. |
| SUBSET 2 DPSCs derived from humans (hDPSCs) | |||||||
| Datta et al., 2017 [17] | Male Wistar rats induced with DM by single intraperitoneal injection with 55 mg/kg STZ. hDPSCs from healthy third molars from 18–40-year-old patients. | 16 weeks old. | 4 weeks and 8 weeks after hDPSC treatment; 10 weeks and 14 weeks after STZ administration. | 6 weeks after DM induction, 1 × 106 hDPSCs administered IV via lateral tail vein or IM through soleus muscle once or with a second dose 4 weeks after the first dose. | In vitro: adipogenic and osteogenic differentiation. In vivo: blood glucose, BW, thermal hyperalgesia by tail immersion test; grip strength; sciatic nerve conduction; immunohistochemistry following sacrifice; plasma proteins. | Positive for stromal cell markers; adipogenic and osteogenic differentiation. In vivo: decrease in BW in diabetic rats, BW increased with hDPSC treatment, but decreased after 6 weeks of IV treatment; blood glucose levels were reduced to normal with IM and IV administrations of hDPSCs. Tail flick test showed thermal sensitivity was reduced with treatment across groups treated with hDPSCs. Grip strength improved more in IV than IM groups, although with IM repeat doses, the grip strength increased more than with a single dose at 8 weeks. | DPSCs caused a reduction of IL-6, TNF-α and increased TGF-β. Repeat IM doses of hDPSCs caused an increase in arachidonic acid. The study suggests that repeat doses of IM transplantation are a more effective long-term option to treat DPN, which may be attributed to the presence of SCs within the soleus muscle. |
| Al-Serwy et al., 2021 [58] | Male Spraque Dawley (SD) rats. T1DM induced by STZ by intraperitoneal route. hDPSCs from adult human impacted third molars. | 6–8 weeks old. | 28 days after hDPSC transplantation. | Group 1: normal control rats. Group 2: untreated diabetes induced rats. Group 3: diabetic rats treated with 1x 106 DPSCs by IV administration. | Fasting blood glucose, glucose tolerance test, parotid gland weight and histology, salivary flow rate, caspase-3. | Blood glucose reduced with DPSC transplantation. Parotid gland weight and salivary flow improved with DPSCs. Caspase-3 reduced and VEGF upregulated with DPSCs. | Presence of transplanted DPSCs in STZ-injured parotid gland demonstrates the migratory ability of stem cells towards injured tissue. |
| └ El-Kersh et al., 2020 [59] | Male SD rats. Healthy impacted third molars from adult patients. T1DM induced by intraperitoneal injection of STZ. | 6 weeks old. | 4 weeks after transplantation; 5 weeks after DM induction. | Rats were divided into four groups: non diabetic rats, diabetic rats that were given buffer; DM rats that were treated with 1 × 106 DPSCs by IV; and DM rats that were treated with 1 × 106 DPSCs via intrapancreatic administration. For IV group, DPSCs administered into tail vein; for intrapancreatic group DPSC suspension administered into pancreas. | Insulin and C-peptide assay, blood glucose. Pancreatic immuno -histochemical and histological analyses. | Blood glucose levels in IV group reduced by 7th day following transplantation; in intrapancreatic group, the blood glucose levels were reduced by 14th day after DPSC treatment. Glucose homeostasis was maintained as established by glucose tolerance tests after 4 weeks of DPSC treatment in both IV and intrapancreatic groups. Insulin and C-peptide levels were higher in the DPSC treated groups than in the non-treated group. Pancreatic islet morphology and angiogenesis improved in both intrapancreatic and IV groups . | The study demonstrated that pancreatic function was re- established and maintained for 4 weeks following DPSC treatment. The study showed that intrapancreatic and IV administrations have comparable therapeutic results in an experimental T1DM model. |
| Hata et al., 2021 [48] | BALB/cAJcl-nu/nu nude male mice. hDPSCs from impacted third molars from human adults aged 13–23 years. T1DM induced by single dose of intraperitoneal injection of STZ. Mice that were not treated with STZ were normal controls. | 6 weeks old. | 16 weeks following transplantation of hDPSCs; 24 weeks after induction of DM. | Intramuscular (IM) transplantation of hDPSCs in saline injected in 10 separate sites in the hind- limb on one side. Saline was injected into the opposite hind limb on the control side. | Neurite outgrowth of mouse dorsal root ganglion (DRG) in vitro. Blood glucose; body weight (BW). 4 and 16 weeks after transplantation, SNCV, sciatic blood flow, current perception threshold (CPT). Location of transplanted hDPSCs in gastrocnemius muscle. | BW was reduced in DM mice than in normal control mice, blood glucose was significantly increased in DM mice than in normal control mice. hDPSCs promoted DRG neurite outgrowth in vitro. MNCV and SNCV and sciatic blood flow reduced in DM mice in saline injected sides; however, they significantly improved in hDPSC sides at 4 weeks, and were maintained upto 16 weeks post- transplantation. CPT significantly improved in hDPSC injected side at 4 weeks up to 16 weeks post-transplantation. hDPSCs were found around muscle bundles of gastrocnemius muscle in hDPSC side and not in saline injected sides 16 weeks post- transplantation. | Longer duration effects of DSCs on DPN were highlighted in this study. |
| └ Hata et al., 2020 [49] | Male nude mice (BALB/cAJcl-nu/nu). hDPSCs from impacted third molars extracted from humans 13–23 years of age. DM induced by intraperitoneal injection of STZ. Mice that did not receive STZ were normal controls. | 6 weeks old. | 4 weeks following hDPSC trans plantation, 12 weeks after induction of DM. | 8 weeks after STZ administration, hDPSCs in saline injected in 10 separate sites in unilateral right hind limb skeletal muscle of all mice. Saline was injected into the left hind limb muscle on the opposite side as controls. | Body weight (BW), blood glucose. MNCV, SNCV, SNBF, CPT Characterization of transplanted hDPSCs. Capillary-muscle density ratio in gastrocnemius muscle. Effect of human VEGF and NGF antibodies on hDPSC treatment. | CPT increased in saline injected sides and improved in hDPSC injected sides of mice. All diabetic mice showed reduced BW and increased blood glucose at the end of experiment. MNCV, SNCV, and SNBF reduced in saline -injected sides of DM mice compared to normal mice, but were significantly improved in hDPSC-treated sides of diabetic mice. hDPSCs were found localized around muscles 4 weeks after transplantation, whereas the saline injected sides did not show any hDPSCs. Human VEGF, NGF expressed in hDPSC sides only in normal and diabetic mice. VEGF and NGF antibodies suppressed hDPSC effects in MNCV and SNCV in hDPSC transplanted sides of mice. Capillary-muscle ratio reduced in DM mice in vehicle side, but improved significantly in hDPSC side of diabetic mice. | Suppressing effect of human VEGF and NGF antibodies on hDPSCs in DM mice shows that angiogenic and neurotrophic factors are important for hDPSC treatment. Potential cross effects of human VEGF and NGF antibodies on mouse VEGF and NGF may be present. |
| Ahmed et al., 2021 [60] | Adult male Wistar rats. Insulin producing cells (IPCs) from hDPSCs derived from human adult teeth. T1DM induced by single dose of SC injection of STZ. Normal controls were not treated with STZ. | Age of rats unclear. | 28 days following IPC transplantation. | Group 1: 10 rats— normal controls. Group 2: 10 rats— untreated diabetic rats. Group 3: 10 rats– diabetic rats treated with IPCs from DPSCs generated in the presence of cerium nanoparticles by IV administration (tail vein). Group 4: 10 rats—diabetic rats treated with IPCs from DPSCs generated in the presence of yttrium nanoparticles by IV. | Blood glucose, serum insulin (INS), hepatic hexokinase, glucose 6 phosphate dehydrogenase (G6PD), location of labeled IPCs in body following transplantation. | Blood glucose reduced and INS increased following IPC administration in both treated diabetic groups compared to diabetic controls. Hepatic hexokinase and G6PD, which were reduced in induced diabetes, increased in Group 3 compared to untreated diabetic rats. Group 3 and 4 showed increase in G6PD in diabetic rats; however, Group 3 generated greater G6PD activity than Group 4. Transplanted IPCs were located in the pancreas and improved pancreatic morphology. | Conditioned IPCs underwent hypoxia prior to transplantation. |
| Inada et al., 2022 [54] | 40 Male nude F344-NJCl-rnu/rnu rats. T1DM induced by STZ via intraperitoneal route. hDPSCs from adult teeth. Human BMMSCs (hBMMSCs) obtained from SC bank. Tacrolimus was injected in diabetic group rats, along with transplants. Insulin implants were placed in diabetic rats at 12 weeks of age and removed at 16 weeks of age. | 9 weeks old. | 4 weeks after hDPSC transplantation and at 18 weeks of age. | Group 1: normal control rats. Group 2: diabetic control rats. Group 3: rats transplanted with hBMMSCs. Group 4: rats transplanted with 2D hBMMSCs. Group 5: 3D hBMMSCs transplanted rats. Group 6: hDPSC transplanted rats. Group 7: 2D hDPSC transplanted rats. Group 8: 3D hDPSC transplanted rats. Transplants of IPCs from SCs were placed in capsules of the left kidney of each animal; the cells were 5 × 106 per animal. | Non-fasting blood glucose, glucose tolerance test. Water consumption. Immunohistochemistry of kidneys. Serum human and rat insulin, serum urea, and creatinine. | After insulin implant was removed, water consumption increased in all except the 3D hDPSC group. All groups except for the 3D HDPSC group showed an increase in blood glucose after insulin implants were removed. Human as well as rat insulin increased in the 3D-hDPSC group. | After measuring serum urea and creatinine levels, it was found that there were no differences between diabetic rats and normal controls. The authors concluded that there were no effects of stem cells on the kidneys. Since rat as well as human insulin increased in the 3D hDPSC group, it was determined that transplanted IPCs performed an endocrine function and also aided in regeneration of host islet cells. |
| SUBSET 3 human gingival stem cells (hGMSCs) | |||||||
| Zhang et al., 2017 [9] | Wild type C57BL/6-foxgfb male mice. Induced with T1DM by multiple doses of STZ 40 mg/kg via intraperitoneal route for 5 days. Healthy gingival tissue from third molar extraction sites of Asian male or female patients aged 20–30 yrs. old. | 6–8 weeks old. | 10 days and 30 days after STZ administration. | 1 × 106 GMSCs (test group) or dermal fibroblasts (group 2) administered via intraperitoneal route at 0, 7, 14, 21, and 28 days after STZ administration. | In vitro: suppressive assay; murine CD4+T cell differentiation. In vivo: non-fasting blood glucose twice a week for 30 days following STZ administration. Histology and Immunohistochemistry of pancreas following sacrifice. | GMSCs have similar morphology to fibroblasts. CD4+T cell differentiation was reduced; GMSCs expressed CD39 and CD73 molecules. DM was delayed with GMSC administration; blood glucose was reduced more than with fibroblasts; DM was not prevented completely with GMSCs. More islet cells stained positive for insulin in the GMSC group, and insulitis was reduced significantly more than with fibroblasts. IL-17 and interferon-γ reduced after GMSC administration. | The study suggests the immunomodulatory mechanism of GMSCs is through CD39 or CD73 signals. T1DM was suppressed due to IL17 inhibition by GMSCs. GMSCs were found homed in pancreas and pancreatic lymph nodes, possibly attributed to intraperitoneal route. |
| SUBSET 4 Stem cells derived from human PDL (hPDLSCs) | |||||||
| Aly et al., 2022 [61] | Adult male Spraque Dawley (SD) rats. IPCs from PDLSCs from healthy impacted human third molars and from human DPSCs from third molars (aged 16–24 years). Differentiation into IPCs was induced by Laminin 411. T1DM induced with single SC dose of STZ. | Age of rats unclear. | 28 days after transplantation. | Group 1: normal controls. Group 2: untreated diabetic controls. Group 3: diabetic rats treated with 5 × 106 IPCs from human DPSCs by IV route. Group 4: diabetic rats treated with 5 × 106 IPCs from human PDLSCs by IV route. | Blood glucose, serum insulin (INS), C-Peptide (CP) | Blood glucose reduced with IPC transplantation from both human DPSCs and PDLSCs. INS and CP increased with IPCs from both sources. | The study demonstrates the efficacy of IPCs from PDLSCs, as well as DPSCs in regulating glucose and insulin in diabetic rats. |
| SUBSET 5 DPSCs derived from teeth of rats (rDPSCs) | |||||||
| Hata et al., 2015 [46] | Male SD rats induced with T1DM by a single dose of 60 mg/kg STZ intraperitoneal injection. DPSCs from incisors of 6-week-old male SD rats or green fluorescent protein (GFP) SD rats. | 6 weeks old. | 4 weeks after transplantation of rDPSCs; 12 weeks from time of DM induction. | 1 × 106 cells per limb (either freshly isolated or partly frozen for 6 months) of DPSCs injected into the unilateral skeletal muscle of hind limb while 1 mL saline administered similarly in the other hind limb, 8 weeks following induction of T1DM. | In vitro: assessment of cell surface markers CD34, CD49d, and CD45. Differentiation of fresh and frozen DPSCs. In vivo: 4 weeks after DPSC administration, MNCV, SNCV SNBF; IENFD, capillary -muscle fiber ratio, and location of DPSCs from GFP rats. | DPSCs were spindle shaped and expressed CD29 and CD90. Both fresh and cryopreserved DPSCs showed adipogenic and osteogenic differentiation. DPSCs expressed VEGF and bFGF. MNCV, SNCV, SNBF and IENFD increased in fresh as well as in cryopreserved DPSC injected hind limbs; vascular endothelial cell - muscle ratio increased with DPSCs; DPSC engrafted around skeletal muscle and did not differentiate into adipocytes or osteoblasts. | Transplanted DPSCs differentiated into PECAM-1 positive vascular endothelial cells, as indicated by GFP stained cells. The study showed that the proliferative ability of frozen DPSCs was similar to that of freshly isolated DPSCs. |
| └ Omi et al., 2016 [47] | Male SD rats induced with T1DM by intraperitoneal injection of 60 mg/kg STZ. DPSCs from mandibular incisors of 6- week-old normal male SD rats or GFP transgenic SD rats. | 6 weeks old. | 4 weeks after transplantation of DPSCs; 12 weeks from induction of DM. | 8 weeks following induction of DM, administration into unilateral hind limb with 1 × 106 DPSCs and 1 mL saline in opposite hind limb. | In vitro: morphology and characterization of DPSCs; adipogenic and osteogenic differentiation. In vivo: MNCV, SNCV, SNBF; histology following sacrifice; no monocytes or macrophages in sciatic nerves; IL10, VEGF, bFGF. | In vitro: DPSCs expressed angiogenic factors such as VEGF, BFGF, NGF. In vivo: BW, blood glucose was not affected by DPSC treatment. Monocytes/ macrophage numbers were reduced; delayed MNCV, SNCV, and SNBF was improved with DPSCs in treated hind limb; TNF-α was reduced and IL10 increased in sciatic nerve in treated side. | The study suggests that DPN could be related to inflammatory processes, as reduction of macrophages and pro inflammatory factors TNF-α, and an increase in 1L-10 occurred with concomitant amelioration of DPN following DPSC administration. The study showed that angiogenic factors may also play a role in the treatment of DPN. |
| Omi et al., 2017 [13] | Male SD rats induced with T1DM by intra- peritoneal injection of STZ 60 mg/kg. DPSCs harvested from incisors of 6-week-old SD rats. Dorsal root ganglions (DRG) from 8-week- old mice. | 6 weeks old. | 4 weeks after DPSC administration; 52 weeks after induction of DM. | 48 weeks following DM induction, 1 ×106 DPSCs administered into unilateral hind limb; saline was injected on opposite hind limb as the control. | In vitro: differentiation potential, neurite outgrowth of DRG, Schwann cell viability. In vivo: MNCV, SNCV, SNBF, current perception threshold (CPT); capillary density, nerve fiber density following sacrifice. | DPSCs differentiated into adipocytes and osteocytes and chondrocytes, promoted neurite outgrowth of DRG Schwann cell viability and myelin growth. MNCV, SNCV, SNBF, IENFD, and CPT improved in DPSC treated limb, DPSCs caused increase in the expression of NGF, bFGF; capillary density and myelin thickness of sural nerve was increased in treated side. | The experiment was conducted in rats which were induced with long-term DM (48 weeks). The study suggests that DPN was reduced due to the effects of DPSCs on myelin thickness of nerves. |
| Makino et al., 2019 [52] | Male SD rats induced with T1DM by intra- peritoneal injection of STZ 60 mg/kg. Conditioned medium of DPSCs (DPSC-CM) derived from incisors of 6-week -old SD rats after sacrifice. | 6 weeks old. | 4 weeks after DPSC administration; 12 weeks after DM induction. | 8 weeks after DM induction by STZ, 1 × 106 DPSC-CM administered in unilateral hind limb; 1.0 mL/rat saline injected in opposite hind limb. | In vitro: cell proliferation assay with human umbilical vein endothelial cells (HUVEC); differentiation potential. In vivo: Body weight (BW), blood glucose, MNCV, SNCV, SNBF, IENFD, and immune- histochemistry following sacrifice. | Increased proliferation of HUVECs. No changes in BW and blood glucose. MNCV, SNCV, SNBF, nerve density increased on DPSC-CM injected hind limb; number of macrophages reduced in sciatic nerve of DPSC-CM treated limb; capillary density in skeletal muscle increased with DPSC-CM, but was unaffected in sciatic nerves in hind limb. | DPSC-CM contains VEGF; hence, its use may be contra-indicated in patients with risk of diabetic retinopathy. |
| └ Kanada et al., 2020 [53] | Male SD rats. DPSCs harvested from incisors of 6-week-old male green fluorescent protein GFB transgenic SD rats. Intraperitoneal injection of STZ used to induce DM. | 6 weeks old. | 4 weeks after DPSC administration; 12 weeks after DM induction. | DM induced rats were either injected with saline, DPSCs or secretory factors of DPSCs (DPSC-SF) in the skeletal muscles of unilateral hind limb. Rats that were not induced with DM were included in the normal control group. | BW, blood glucose. SNCV, MNCV SNBF, intraepidermal nerve fiber density (IEFND). Capillary-muscle ratio in skeletal hind limbs. Characterization of secretory factors of DPSCs used in the study. | DM-induced rats showed lower BW and higher blood glucose levels than non-DM rats. Neither DPSCs nor DPSC-SF showed significant improvement in the BW or blood glucose values in DM rats. DPSCs and DPSC-SF improved SNCV, MNCV, sciatic nerve blood flow and IENFD values in the hind limbs that were treated as compared to saline injected DM rats. Muscle volume and capillary-muscle ratio improved with DPSC and DPSC-SF administration. | No significant difference between the effects of DPSCs and DPSC-SF administration. The study design demonstrated that SC administration results were limited to at or near the site of administration. VEGF, NGF, and IL-1 β were identified as some of the secretory factors of DPSCs. |
| SUBSET 6 DPSCs derived from teeth of mice (mDPSCs) | |||||||
| Guimarães et al., 2013 [63] | Female C57BL/6 mice induced T1DM by 3 daily intraperitoneal injections of 80mg/kg STZ. DPSCs from mandibular incisors of male enhanced GFP C57BL/6 mice. | 8 weeks old. | 30 days and 90 days after first STZ dose. | 10 days after first STZ induction of DM, administration of 1 × 106 DPSCs in each mouse via orbital plexus injection. | BW, weekly blood glucose, proteinuria, glycosuria, urea, histopathological assessment of pancreas and kidneys following sacrifice 30 days after DM induction; tail flick test up to 90 days after 1st STZ dose. | At 21 days after DPSC treatment, blood glucose levels were reduced in diabetic mice; BW was normalized. Increase in insulin producing pancreatic cells was seen with DPSC treatment. Engraftment of stem cells in the pancreas was observed. Reduced glucose, protein and increased urea levels were found in the urine. Morphologic changes in the kidneys, which were found in non-treatment diabetic mice, such as the loss of the epithelial brush border, were not seen in DPSC-treated mice, and less deposition of glycogen in the tubules was noted in DPSC-treated mice. Mice developed nociceptive values comparable to those of non-diabetic mice 3 days after DPSC treatment, a result that was maintained throughout the study. | The study showed that DPSCs improved kidney function. C57BL/6 mice are known to be relatively resistant to nephropathy. Blood glucose levels increased gradually, in spite of DPSC treatment, suggesting that repeat doses of DPSCs may be required. Donor mice stem cells secreting insulin were found engrafted in the pancreas. |
| Study | Selection Bias— Sequence Generation | Selection Bias— Baseline Characteristics | Selection Bias— Allocation Concealment | Performance Bias— Random Housing | Performance Bias— Blinding | Detection Bias— Random Outcome Assessment | Detection Bias— Blinding | Attrition Bias— Incomplete Outcome Data | Reporting Bias— Selective Outcome Reporting | Other— Other Types of Bias |
|---|---|---|---|---|---|---|---|---|---|---|
| Guimerães et al., 2013 [63] | U | Low | U | U | U | U | U | U | Low | U |
| Kanafi et al., 2013 [62] | U | Low | U | U | U | U | U | U | U | U |
| Hata et al., 2015 [46] | ||||||||||
| └ Omi et al., 2016 [47] | U | U | U | U | U | U | U | U | U | High *** |
| Izumoto-Akita et al., 2015 [51] | U | Low | Low | U | High * | U | U | Low | U | U |
| Omi et al., 2017 [13] | U | Low | U | U | U | U | U | U | U | High ^*** |
| Datta et al., 2017 [17] | U | Low | U | U | U | U | U | Low | U | High ^ |
| Zhang et al., 2017 [9] | U | Low | U | U | U | U | U | U | Low | Low |
| Rao et al., 2019 [55] | ||||||||||
| └ Rao et al., 2019 [56] | U | Low | U | U | High * | U | U | Low | Low | Low |
| Makino et al., 2019 [52] | ||||||||||
| └ Kanada et al., 2020 [53] | U | Low | U | U | High * | U | U | U | U | U |
| Xie et al., 2019 [14] | Low | Low | U | U | High * | U | U | Low | U | Low |
| El-Kersh et al., 2020 [59] | ||||||||||
| └ Al-Serwy et al., 2021 [58] | U | Low | U | U | High * | U | U | Low | High ** | U |
| Miyura Yura et al., 2020 [50] | U | U | U | U | U | U | U | U | U | U |
| Hata et al., 2021 [48] | U | Low | U | U | High * | U | U | U | U | High *** |
| └ Hata et al., 2020 [49] | ||||||||||
| Xu et al., 2020 [57] | U | Low | U | U | High * | U | U | U | U | U |
| Ahmed et al., 2021 [60] | U | Low | U | U | U | U | U | Low | High ** | U |
| Aly et al., 2022 [61] | U | Low | U | U | U | U | U | U | High ** | U |
| Inada et al., 2022 [54] | U | U | U | U | U | U | U | U | High ** | U |
| Test | Value | p |
|---|---|---|
| Egger’s regression | −7.831 | p < 0.0001 |
| Begg and Mazumdar rank correlation | −0.667 | p = 0.0018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonsekar, P.; Tonsekar, V.; Jiang, S.; Yue, G. Dental Stem Cell-Based Therapy for Glycemic Control and the Scope of Clinical Translation: A Systematic Review and Meta-Analysis. Int. J. Transl. Med. 2024, 4, 87-125. https://doi.org/10.3390/ijtm4010005
Tonsekar P, Tonsekar V, Jiang S, Yue G. Dental Stem Cell-Based Therapy for Glycemic Control and the Scope of Clinical Translation: A Systematic Review and Meta-Analysis. International Journal of Translational Medicine. 2024; 4(1):87-125. https://doi.org/10.3390/ijtm4010005
Chicago/Turabian StyleTonsekar, Pallavi, Vidya Tonsekar, Shuying Jiang, and Gang Yue. 2024. "Dental Stem Cell-Based Therapy for Glycemic Control and the Scope of Clinical Translation: A Systematic Review and Meta-Analysis" International Journal of Translational Medicine 4, no. 1: 87-125. https://doi.org/10.3390/ijtm4010005
APA StyleTonsekar, P., Tonsekar, V., Jiang, S., & Yue, G. (2024). Dental Stem Cell-Based Therapy for Glycemic Control and the Scope of Clinical Translation: A Systematic Review and Meta-Analysis. International Journal of Translational Medicine, 4(1), 87-125. https://doi.org/10.3390/ijtm4010005