Abstract
Pancreatic pseudocysts represent a complication of acute interstitial edematous pancreatitis with a frequency of about 10–20%, and most of these resolve spontaneously. Treatment is indicated only in patients who develop symptoms such as abdominal pain, gastric outlet obstruction, jaundice for compression of the biliary system, or in case of infection. Pancreatic pseudocysts’ complications include pseudocyst infection leading to sepsis, rupture with pancreatic ascites, bleeding or formation of pseudoaneurysm, and, rarely, fistulization to other viscera. The most common sites for fistulas are between cysts and the stomach, duodenum, and colon. Here, we present the case of a patient with severe acute pancreatitis who developed multiple infected fluid collections with a cysto-duodenum fistula that was successfully treated with endoscopic intervention.
1. Introduction
The clinical manifestation of acute pancreatitis can range from mild to severe. Most cases of acute pancreatitis are mild and resolve in a short period with supportive care. However, severe acute pancreatitis can lead to localized or systemic complications. The localized complications include pancreatic fluid collections (PFCs).
PFCs arise from the leakage of pancreatic juice to the peripancreatic area due to the disruption of pancreatic ducts. The revised Atlanta classification refers to collections based on the duration (more or less than four weeks) and nature of collections (necrotic or non-necrotic). These collections are further classified as sterile or infected [1].
Pancreatic pseudocysts (PPs) occur as complications of acute interstitial edematous pancreatitis, with a frequency ranging from 10% to 20% [2]. Asymptomatic PPs, even if of large dimension, do not require any treatment. Invasive management is indicated only in patients who develop symptoms such as abdominal pain, gastric outlet obstruction, jaundice for compression of the biliary system, or in case of infection [2].
Pancreatic pseudocysts’ complications include pseudocyst infection leading to sepsis, rupture with pancreatic ascites, bleeding or formation of pseudoaneurysm, and, rarely, fistula formation to other viscera. The most common sites for fistulas are between cysts and the stomach, duodenum, and colon [3].
Here, we present the case of a patient with severe acute pancreatitis who developed multiple infected fluid collections with a cysto-duodenum fistula that was treated with endoscopic intervention.
2. Case Report
A 73-year-old male patient arrived at the emergency department with severe epigastric pain that arose on the same day and was associated with nausea and vomiting. The patient had no history of alcohol abuse and had not taken any medications at the time of admission.
At admission, examination of peripheral blood yielded the following values: white blood cell (WBC) count of 14,920/mm3 (neutrophils: 80%); hemoglobin: 15.3 g/dL; C-reactive protein (CRP): 23.4 mg/L (normal value < 5 mg/L); procalcitonin: 4.21 ng/mL; total bilirubin: 2.84 mg/dL; direct bilirubin 1.56 mg/dl; aspartate aminotransferase (AST): 379 U/L (normal value < 38 U/L); alanine aminotransferase (ALT): 272 U/L (normal value < 41 U/L); gamma-glutamyl trans-peptidase: 705 IU/L (normal value < 61 U/L); amylase: 178 U/L; lipase: >3000 U/L (normal value < 60 U/L); amylase: > 1500 U/L (normal value < 95 U/L); and calcium: 8.8 mg/dL. Kidney function, coagulation, and cardio-respiratory function were preserved, and the patient did not present an alteration of cognitive status.
Abdominal computerized tomography (CT) revealed an edematous pancreatic gland with fluid collection in the peri-pancreatic area, mainly localized at the level of the tail. Lithiasis of the gallbladder was present. A diagnosis of moderately-severe pancreatitis due to biliary lithiasis complicated by sepsis was made.
The patient was treated according to guidelines with goal-directed fluid replacement, close monitoring, early enteral feeding, and antibiotic therapy. Eight days after the admission, the patient no longer complained of abdominal pain and had good overall health. The laboratory results were normalized. Cholecystectomy was recommended to prevent a recurrence.
Approximately two months after the hospitalization, they returned to the hospital with epigastric pain and fever (38 °C). Laboratory results showed a WBC count of 14,530/mm3 (neutrophils: 78%) and a CRP level of 163 mg/L (<5 mg/L), procalcitonin 0.14 ng/mL. Pancreatic enzymes and liver function test results were within the normal ranges. An abdominal CT scan showed the presence of multiple confluent fluid collections extending from the head to the tail along the entire pancreatic profile containing air (Figure 1). An endoscopic investigation and an endoscopic ultrasound (EUS) were performed. The upper endoscopy revealed the presence of a fistula opening of about 8 mm in diameter in the duodenum bulb with leakage of purulent material (Figure 2). EUS showed the presence of air in the fistula and a complex 5 cm fluid collection in the tail of the pancreas (Figure 3). An abdominal CT scan with gastrografin confirmed the fistulous channel originating from the first duodenal portion, which gives rise to two branches, anteriorly in the head of the pancreas and posteriorly in the tail. After a collegial reunion with clinicians, surgeons, radiologists, and gastroenterologists, it was decided to proceed with the drainage of the larger pancreatic collection in an attempt to heal the fistula with the duodenum. EUS-guided trans gastric drainage of the fluid collection was performed using a 16 × 20 mm lumen-apposing metal stent (LAMS, Hot-Spaxus, Taewoong Medical Co., Gimpo, Korea), obtaining drainage of copious purulent material in the stomach (Figure 4).
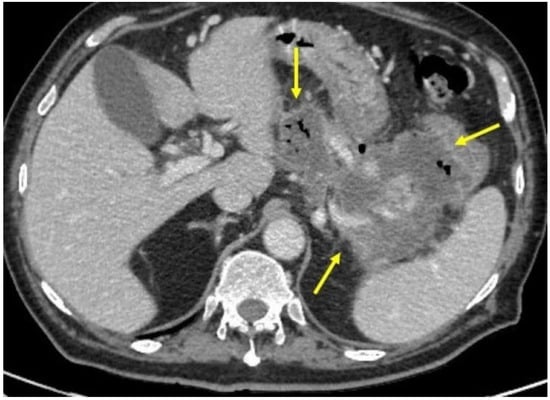
Figure 1.
Abdominal CT scan showing the presence of multiple confluent fluid collections extending from the head to the tail along the entire pancreatic profile (outlined from yellow arrow).
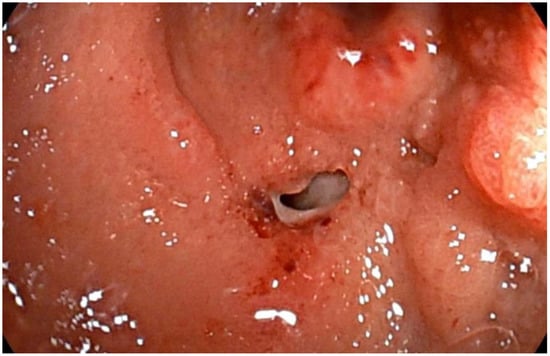
Figure 2.
Endoscopy view of fistula opening of about 8 mm in diameter in the duodenum bulb with leakage of purulent material.
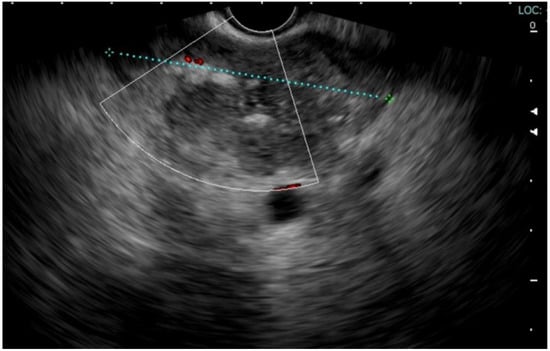
Figure 3.
EUS showed the presence of air in the fistula and a complex 5 cm fluid collection in the tail of the pancreas.
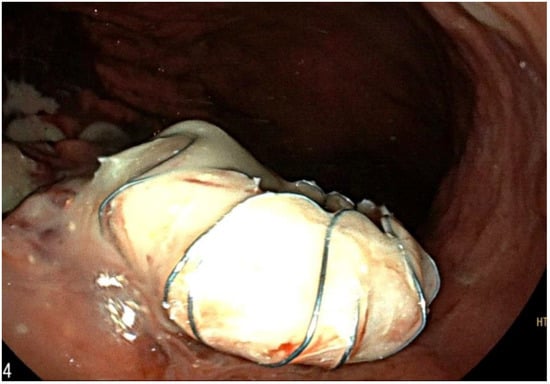
Figure 4.
EUS-guided trans-gastric drainage of the fluid collection using a 16 × 20 mm lumen-apposing metal stent (LAMS, Hot-Spaxus, Taewoong Medical Co, Gimpo, Korea).
After a few days, the patient no longer complained of abdominal pain, had no more fever, and laboratory exams showed amelioration of CRP. After six days, due to complaints of nausea and malaise while eating, a feeding tube for enteral nutrition was placed with the distal head at the level of Treitz, and a revision of the drainage was made, showing necrotic material and granulation tissue in the lumen of the stent (Figure 5). The patient was discharged from the hospital in good health.

Figure 5.
Endoscopic view of the drainage showing necrotic material and granulation tissue in the lumen of the stent.
After four weeks, the patient was in good clinical condition, asymptomatic. An abdominal CT scan showed a reduction of the overall pseudocysts (Figure 6). The laboratory exams showed CRP, amylase, lipase, transaminases, and cholestatic exam results within the normal ranges.
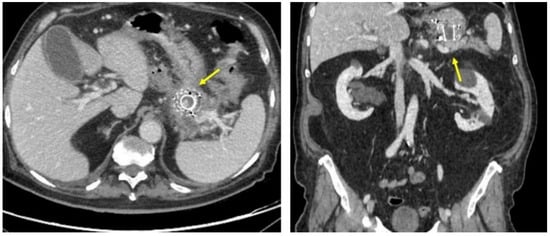
Figure 6.
Abdominal CT scan showing a reduction of the overall pseudocysts (yellow arrow).
After detecting by upper endoscopy the resolution of necrosis through the lumen of the stent (Figure 7) and the healing of the previous opening fistula (Figure 8), the LAMS was removed without any complication. The patient is currently under outpatient follow-up with subclinical conditions.
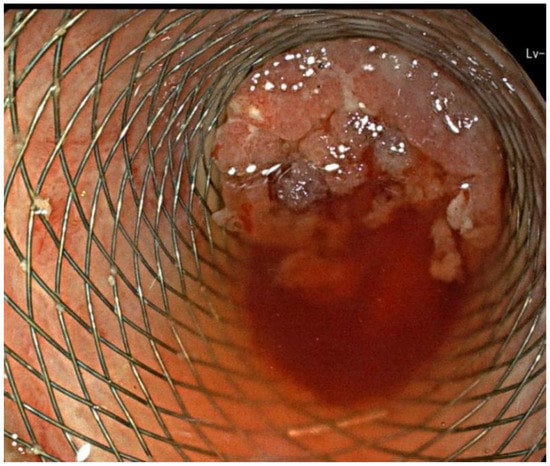
Figure 7.
Endoscopic view of the resolution of necrosis through the lumen of the stent.
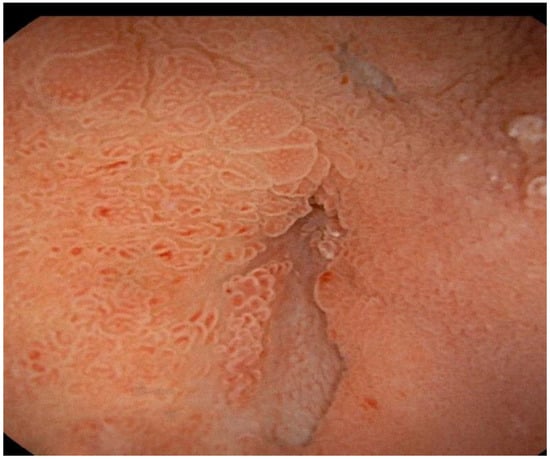
Figure 8.
Endoscopic view of the healing of the previous opening fistula.
3. Discussion
The drainage of complicated PFCs could be made through surgical, percutaneous, or endoscopic approaches. The endoscopic approach, due to its lower morbidity rate compared to the surgical and percutaneous ones, is the preferred first-line approach for managing PFCs [4,5]. Endoscopic ultrasound (EUS)-guided drainage represents the favorited method of draining PFCs because of the possibility of distinguishing PFCs from cystic tumors, determining the content of the PFC, and identifying interposed blood vessels, reducing the risk of bleeding [6].
LAMSs are recently designed stents with a bi-flanged shape. These are the stents of choice for endoscopic drainage of PFCs. This is due to the easy-to-use sorting procedure time and direct debridement access [7]. Several studies demonstrated that LAMSs have better efficacy and safety than plastic stents for PFC [8]. There is a reduced risk of leakage with the LAMS compared to plastic stents mainly due to dual flange anchors and the fully covered nature of the LAMS [9]; however, cases of bleeding perforation and stent migration are still reported in LAMS utilization.
A rare complication of PPs is the formation of a fistula within the gastrointestinal tract. Pseudocysts’ fistulas occur in one-third of all cases in the gastric cavity, followed by the colon and duodenum communication. The pathogenesis of fistula formation is thought to be due to elevated internal pressure of the PP caused by the accumulation of the pancreatic liquid. Due to this pressure, the fluid invades peripancreatic tissue and organs or vessels, inducing ischemic damage that enables penetration of the walls’ organs and the formation of a fistula [10]. Most pseudocyst-enteric fistulas that form in the upper gastrointestinal tract can be treated conservatively and have a relatively good prognosis. However, sometimes the fistula cannot drain all the pseudocysts’ content.
4. Conclusions
Here we presented the case of a complicated pseudocyst that cannot be entirely drained from the duodenum fistula and needed endoscopic drainage of the major fluid collection. From a clinical point of view, this case suggests that sometimes, in the case of multiloculated pseudocysts, combining the endoscopic drainage with the natural formation of the fistula can be decisive for the resolution of symptoms.
Author Contributions
B.L.: study concept and design, acquisition of data, manuscript preparation; M.B.: study concept and design, final drafting of the manuscript, critical discussion and support, revision of the manuscript for important intellectual content; I.F. and E.P.: critical discussion and support. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are present in clinical record of the patient at policlinico casilino hospital of rome.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S.; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis—2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Nabi, Z.; Basha, J.; Reddy, D.N. Endoscopic management of pancreatic fluid collections-revisited. World J. Gastroenterol. 2017, 23, 2660–2672. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.K.; Tiwary, S.K.; Kumar, P. Pancreatic pseudocyst: Therapeutic dilemma. Int. J. Inflam. 2012, 2012, 279476. [Google Scholar] [CrossRef] [PubMed]
- Seewald, S.; Ang, T.L.; Kida, M.; Teng, K.Y.; Soehendra, N.; EUS 2008 Working Group. EUS 2008 Working Group document: Evaluation of EUS-guided drainage of pancreatic-fluid collections (with video). Gastrointest. Endosc. 2009, 69, S13–S21. [Google Scholar] [CrossRef] [PubMed]
- Tyberg, A.; Karia, K.; Gabr, M.; Desai, A.; Doshi, R.; Gaidhane, M.; Sharaiha, R.Z.; Kahaleh, M. Management of pancreatic fluid collections: A comprehensive review of the literature. World J. Gastroenterol. 2016, 22, 2256–2270. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, C.; Luigiano, C.; Maimone, A.; Polifemo, A.M.; Tarantino, I.; Cennamo, V. Endoscopic ultrasound-guided drainage of pancreatic fluid collections. World J. Gastrointest. Endosc. 2012, 4, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.E.; Benrajab, K.; Mardini, H.; Su, L.; Gabr, M.; Frandah, W.M. Anchoring lumen-apposing metal stent with coaxial plastic stent for endoscopic ultrasound-guided drainage of pancreatic fluid collections: Any benefit? Ann. Gastroenterol. 2019, 32, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Hammad, T.; Khan, M.A.; Alastal, Y.; Lee, W.; Nawras, A.; Ismail, M.K.; Kahaleh, M. Efficacy and safety of lumen-apposing metal stents in management of pancreatic fluid collections: Are they better than plastic stents? A systematic review and meta-analysis. Dig. Dis. Sci. 2018, 63, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, P.; Hsueh, W.; Nasr, J. Use of lumen-apposing stents for the treatment of postsurgical fluid collections: A case series and a review of literature. Case Rep. Gastrointest. Med. 2019, 2019, 7656950. [Google Scholar] [CrossRef] [PubMed]
- Shatney, C.H.; Sosin, H. Spontaneous perforation of a pancreatic pseudocyst into the colon and duodenum. Am. J. Surg. 1973, 126, 433–438. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).