
The Influence of COVID-19 on Patient Mobilization and Injury Attributes in the ICU: A Retrospective Analysis of a Level II Trauma Center

 , ,
, ,
Abstract
1. Introduction
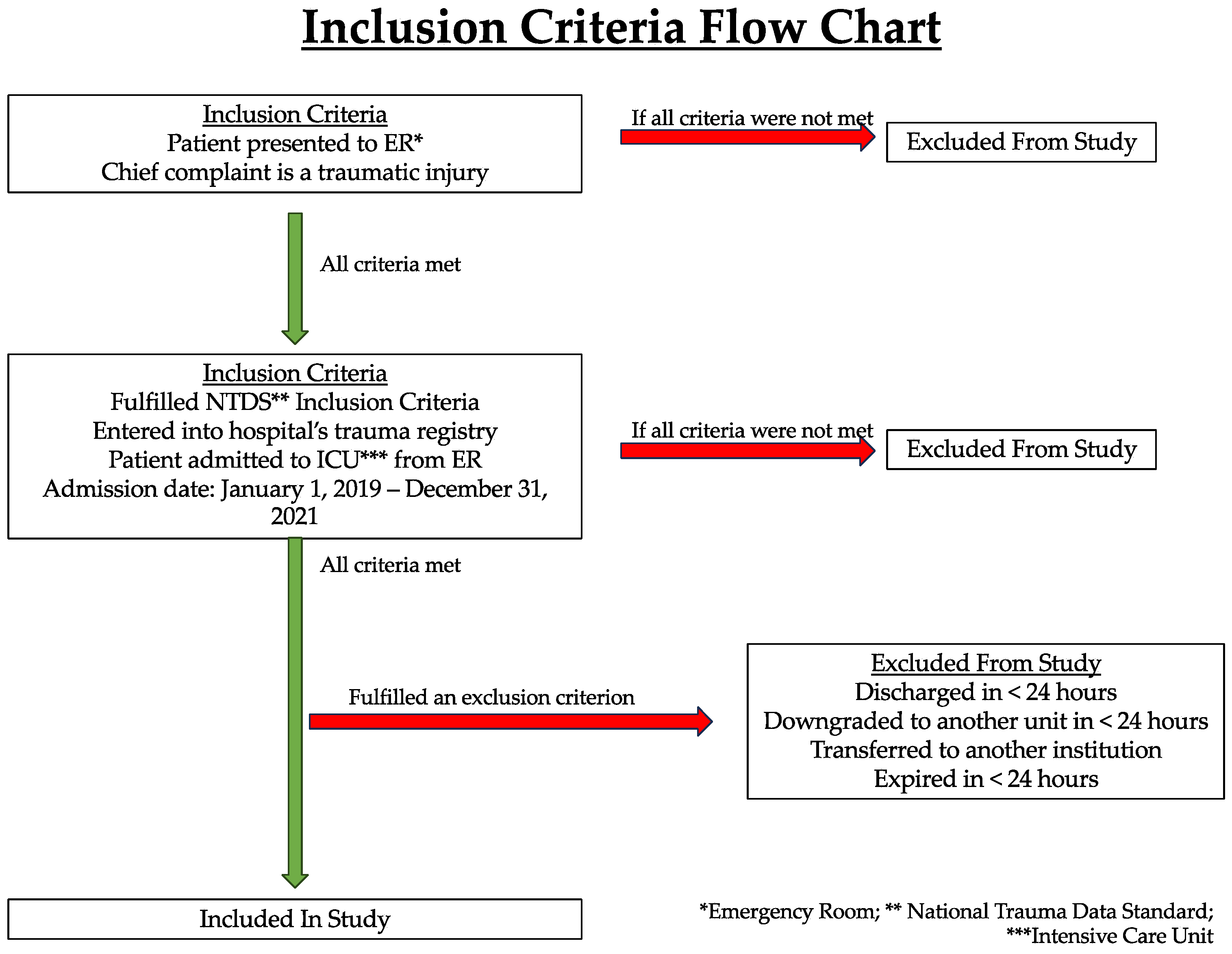
2. Methods
3. Results
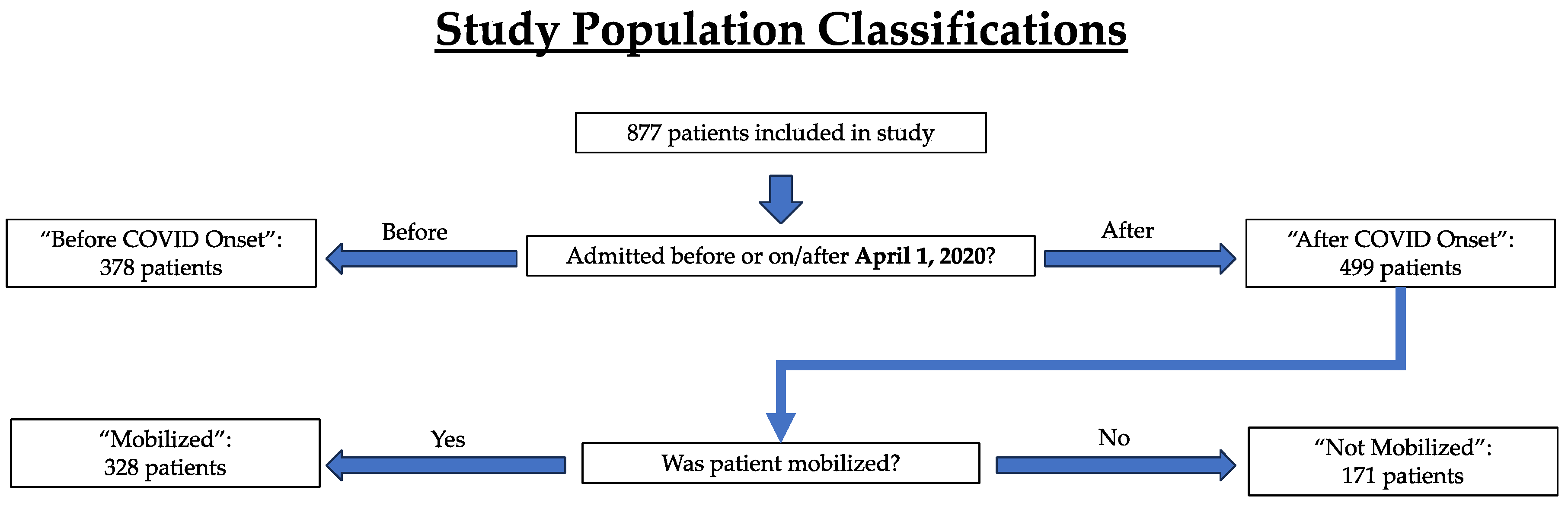
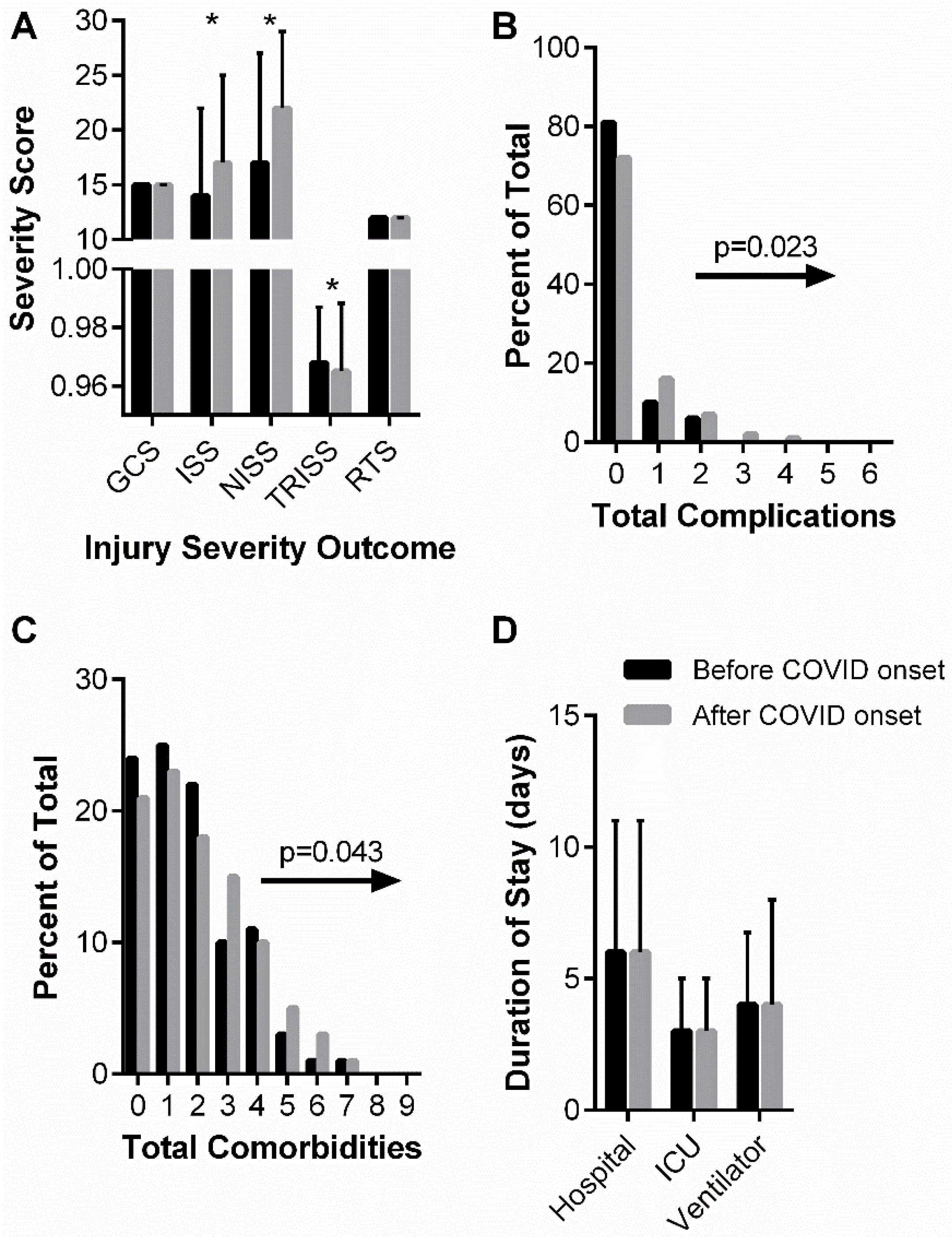
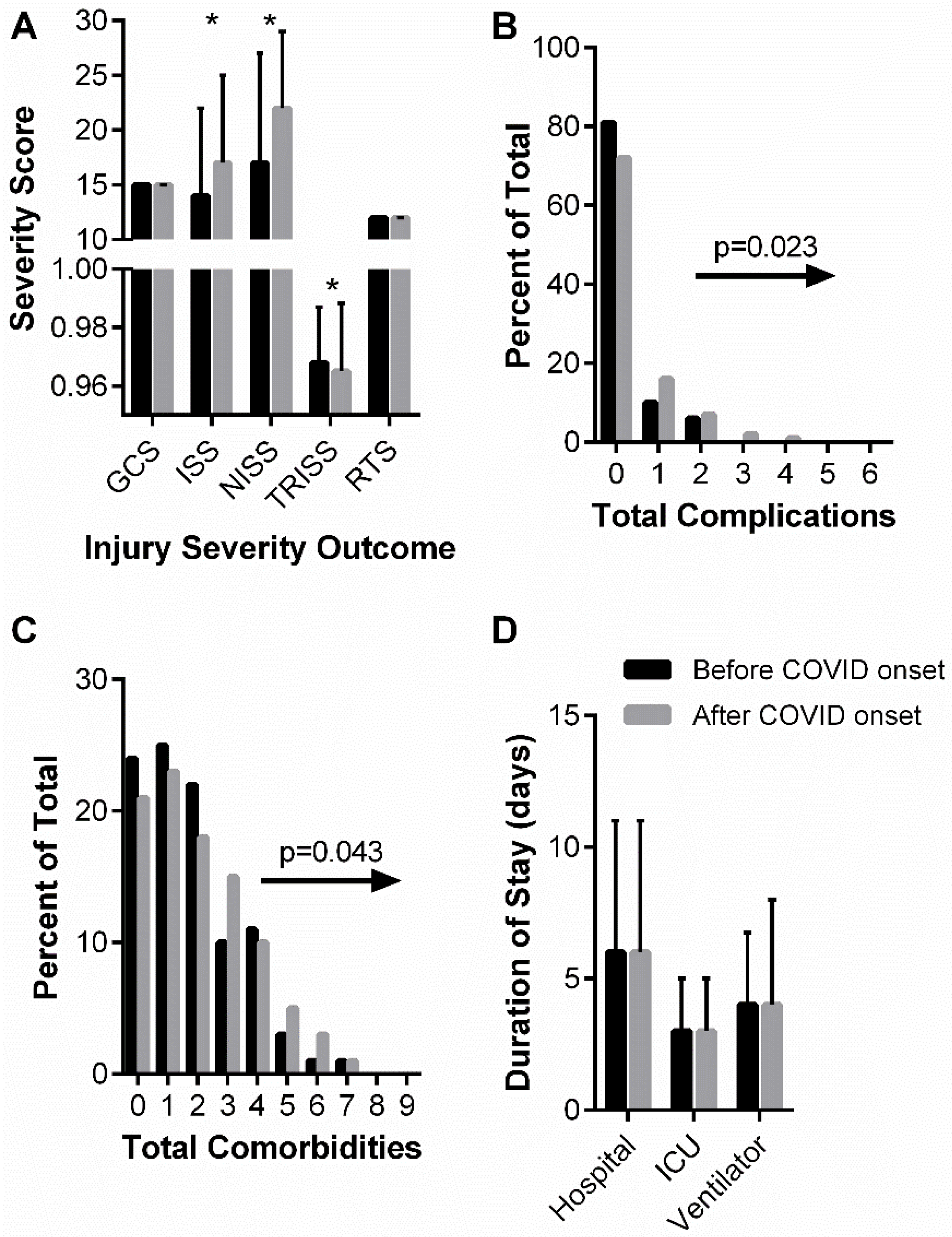
3.1. “Before and after COVID Onset” Patient Characteristics, Injury Attributes, and Mobilization
3.2. “After COVID Onset” Patient Characteristics, Injury Attributes, and Outcomes Stratified by Mobilization
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality: Systematic review and meta-analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact of the COVID-19 Pandemic on Hospital Admissions in the United States. Health Aff. 2020, 39, 2010–2017. [Google Scholar] [CrossRef] [PubMed]
- Hafner, K. Fear of COVID-19 leads other patients to decline critical treatment. The New York Times, 25 May 2020. [Google Scholar]
- Azuh, O.; Gammon, H.; Burmeister, C.; Frega, D.; Nerenz, D.; DiGiovine, B.; Siddiqui, A. Benefits of Early Active Mobility in the Medical Intensive Care Unit: A Pilot Study. Am. J. Med. 2016, 129, 866–871.e861. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, J.R.; Herbsman, J.M.; Bushnik, T.; Van Lew, S.; Stolfi, A.; Parkin, K.; McKenzie, A.; Hall, G.W.; Joseph, W.; Whiteson, J.; et al. Early Rehabilitation in the Medical and Surgical Intensive Care Units for Patients with and without Mechanical Ventilation: An Interprofessional Performance Improvement Project. PM R 2017, 9, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Chen, J.; Li, F.; Li-Tsang, C.W.; Liu, Q.; Ma, X.; Ao, M.; Chen, N.; Zhou, Y.; Zhong, X.; et al. Effects of mobility training on severe burn patients in the BICU: A retrospective cohort study. Burns 2016, 42, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Engel, H.J.; Tatebe, S.; Alonzo, P.B.; Mustille, R.L.; Rivera, M.J. Physical therapist-established intensive care unit early mobilization program: Quality improvement project for critical care at the University of California San Francisco Medical Center. Phys. Ther. 2013, 93, 975–985. [Google Scholar] [CrossRef]
- Engel, H.J.; Needham, D.M.; Morris, P.E.; Gropper, M.A. ICU early mobilization: From recommendation to implementation at three medical centers. Crit. Care Med. 2013, 41, S69–S80. [Google Scholar] [CrossRef]
- Lai, C.C.; Chou, W.; Chan, K.S.; Cheng, K.C.; Yuan, K.S.; Chao, C.M.; Chen, C.M. Early Mobilization Reduces Duration of Mechanical Ventilation and Intensive Care Unit Stay in Patients with Acute Respiratory Failure. Arch. Phys. Med. Rehabil. 2017, 98, 931–939. [Google Scholar] [CrossRef]
- McWilliams, D.; Weblin, J.; Atkins, G.; Bion, J.; Williams, J.; Elliott, C.; Whitehouse, T.; Snelson, C. Enhancing rehabilitation of mechanically ventilated patients in the intensive care unit: A quality improvement project. J. Crit. Care 2015, 30, 13–18. [Google Scholar] [CrossRef]
- Morris, P.E.; Goad, A.; Thompson, C.; Taylor, K.; Harry, B.; Passmore, L.; Ross, A.; Anderson, L.; Baker, S.; Sanchez, M.; et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit. Care Med. 2008, 36, 2238–2243. [Google Scholar] [CrossRef]
- Schaller, S.J.; Anstey, M.; Blobner, M.; Edrich, T.; Grabitz, S.D.; Gradwohl-Matis, I.; Heim, M.; Houle, T.; Kurth, T.; Latronico, N.; et al. Early, goal-directed mobilisation in the surgical intensive care unit: A randomised controlled trial. Lancet 2016, 388, 1377–1388. [Google Scholar] [CrossRef] [PubMed]
- Sigler, M.; Nugent, K.; Alalawi, R.; Selvan, K.; Tseng, J.; Edriss, H.; Turner, A.; Valdez, K.; Krause, D. Making of a Successful Early Mobilization Program for a Medical Intensive Care Unit. South Med. J. 2016, 109, 342–345. [Google Scholar] [CrossRef]
- Hanekom, S.D.; Louw, Q.; Coetzee, A. The way in which a physiotherapy service is structured can improve patient outcome from a surgical intensive care: A controlled clinical trial. Crit. Care 2012, 16, R230. [Google Scholar] [CrossRef]
- Klein, K.; Mulkey, M.; Bena, J.F.; Albert, N.M. Clinical and psychological effects of early mobilization in patients treated in a neurologic ICU: A comparative study. Crit. Care Med. 2015, 43, 865–873. [Google Scholar] [CrossRef]
- Pandullo, S.M.; Spilman, S.K.; Smith, J.A.; Kingery, L.K.; Pille, S.M.; Rondinelli, R.D.; Sahr, S.M. Time for critically ill patients to regain mobility after early mobilization in the intensive care unit and transition to a general inpatient floor. J. Crit. Care 2015, 30, 1238–1242. [Google Scholar] [CrossRef]
- Titsworth, W.L.; Hester, J.; Correia, T.; Reed, R.; Guin, P.; Archibald, L.; Layon, A.J.; Mocco, J. The effect of increased mobility on morbidity in the neurointensive care unit. J. Neurosurg. 2012, 116, 1379–1388. [Google Scholar] [CrossRef]
- Adler, J.; Malone, D. Early mobilization in the intensive care unit: A systematic review. Cardiopulm. Phys. Ther. J. 2012, 23, 5–13. [Google Scholar] [CrossRef]
- Bailey, P.; Thomsen, G.E.; Spuhler, V.J.; Blair, R.; Jewkes, J.; Bezdjian, L.; Veale, K.; Rodriquez, L.; Hopkins, R.O. Early activity is feasible and safe in respiratory failure patients. Crit. Care Med. 2007, 35, 139–145. [Google Scholar] [CrossRef]
- Burtin, C.; Clerckx, B.; Robbeets, C.; Ferdinande, P.; Langer, D.; Troosters, T.; Hermans, G.; Decramer, M.; Gosselink, R. Early exercise in critically ill patients enhances short-term functional recovery. Crit. Care Med. 2009, 37, 2499–2505. [Google Scholar] [CrossRef]
- Hodgson, C.L.; Bailey, M.; Bellomo, R.; Berney, S.; Buhr, H.; Denehy, L.; Gabbe, B.; Harrold, M.; Higgins, A.; Iwashyna, T.J.; et al. A Binational Multicenter Pilot Feasibility Randomized Controlled Trial of Early Goal-Directed Mobilization in the ICU. Crit. Care Med. 2016, 44, 1145–1152. [Google Scholar] [CrossRef]
- Laurent, H.; Aubreton, S.; Richard, R.; Gorce, Y.; Caron, E.; Vallat, A.; Davin, A.M.; Constantin, J.M.; Coudeyre, E. Systematic review of early exercise in intensive care: A qualitative approach. Anaesth. Crit. Care Pain Med. 2016, 35, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Needham, D.M.; Korupolu, R.; Zanni, J.M.; Pradhan, P.; Colantuoni, E.; Palmer, J.B.; Brower, R.G.; Fan, E. Early physical medicine and rehabilitation for patients with acute respiratory failure: A quality improvement project. Arch. Phys. Med. Rehabil. 2010, 91, 536–542. [Google Scholar] [CrossRef]
- Patman, S.M.; Dennis, D.M.; Hill, K. Exploring the capacity to ambulate after a period of prolonged mechanical ventilation. J. Crit. Care 2012, 27, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Schweickert, W.D.; Pohlman, M.C.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet 2009, 373, 1874–1882. [Google Scholar] [CrossRef]
- AOTR. AOTR Trauma Registry Resource Manual; AOTR: Columbus, OH, USA, 2020; p. 48. [Google Scholar]
- Strassle, P.D.; Ko, J.S.; Ponder, M.; Napoles, A.M.; Kinlaw, A.C.; Schiro, S.E. Impact of COVID-related policies on gunshot wound assault hospitalizations in the United States: A statewide time series analysis. Inj. Epidemiol. 2023, 10, 2. [Google Scholar] [CrossRef]
- Padubidri, A.A.; Rushing, A.; Ochenjele, G.; Sontich, J.; Napora, J.; Osborne, A.; Delozier, S.; Wetzel, R. Increase in gunshot wounds at a level 1 trauma center following the COVID19 pandemic. OTA Int. 2021, 4, e159. [Google Scholar] [CrossRef]
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V.; National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, 1 January 2019–30 May 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef]
- Oseran, A.S.; Nash, D.; Kim, C.; Moisuk, S.; Lai, P.Y.; Pyhtila, J.; Sequist, T.D.; Wasfy, J.H. Changes in hospital admissions for urgent conditions during COVID-19 pandemic. Am. J. Manag. Care 2020, 26, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Burgard, M.; Cherbanyk, F.; Nassiopoulos, K.; Malekzadeh, S.; Pugin, F.; Egger, B. An effect of the COVID-19 pandemic: Significantly more complicated appendicitis due to delayed presentation of patients! PLoS ONE 2021, 16, e0249171. [Google Scholar] [CrossRef]
- Yeates, E.O.; Grigorian, A.; Schellenberg, M.; Owattanapanich, N.; Barmparas, G.; Margulies, D.; Juillard, C.; Garber, K.; Cryer, H.; Tillou, A.; et al. Decreased hospital length of stay and intensive care unit admissions for non-COVID blunt trauma patients during the COVID-19 pandemic. Am. J. Surg. 2022, 224, 90–95. [Google Scholar] [CrossRef]
- Huang, G.S.; Chance, E.A.; Dunham, C.M. Influence of a Stay-At-Home Order on Trauma Volume and Injury Patterns at a Level I Trauma Center in Ohio. Am. Surg. 2021, 89, 31348211047488. [Google Scholar] [CrossRef] [PubMed]
- Bologheanu, R.; Maleczek, M.; Laxar, D.; Kimberger, O. Outcomes of non-COVID-19 critically ill patients during the COVID-19 pandemic: A retrospective propensity score-matched analysis. Wien. Klin. Wochenschr. 2021, 133, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Jung, K.; Kwon, J.; Moon, J.; Huh, Y.; Heo, Y.J.; Kang, B.H. Changes in the characteristics of trauma patients after the early COVID-19 outbreak: A retrospective study of a regional level 1 trauma center in Republic of Korea. Medicine 2022, 101, e28567. [Google Scholar] [CrossRef] [PubMed]
- Maman, Y.; Lee Goldstein, A.; Neeman, U.; Lessing, Y.; Orbach, L.; Sirhan, S.; Falk, E.; Lahat, G. The Impact of the COVID-19 Pandemic on an Israeli Acute Care Surgery Unit: Fewer Patients, More Disease. Am. Surg. 2022, 88, 2863–2870. [Google Scholar] [CrossRef]
- Leichtle, S.W.; Rodas, E.B.; Procter, L.; Bennett, J.; Schrader, R.; Aboutanos, M.B. The influence of a statewide “Stay-at-Home” order on trauma volume and patterns at a level 1 trauma center in the united states. Injury 2020, 51, 2437–2441. [Google Scholar] [CrossRef]
- Dayananda, K.S.S.; Mercer, S.T.; Agarwal, R.; Yasin, T.; Trickett, R.W. A comparative review of 1,004 orthopaedic trauma patients before and during the COVID-19 pandemic. Bone Jt. Open 2020, 1, 568–575. [Google Scholar] [CrossRef]
- Yeung, E.; Brandsma, D.S.; Karst, F.W.; Smith, C.; Fan, K.F.M. The influence of 2020 coronavirus lockdown on presentation of oral and maxillofacial trauma to a central London hospital. Br. J. Oral. Maxillofac. Surg. 2021, 59, 102–105. [Google Scholar] [CrossRef]
- Pettke, A.; Stassen, W.; Laflamme, L.; Wallis, L.A.; Hasselberg, M. Changes in trauma-related emergency medical services during the COVID-19 lockdown in the Western Cape, South Africa. BMC Emerg. Med. 2023, 23, 72. [Google Scholar] [CrossRef]
- Shen, B.; Chen, B.; Li, K.; Cheng, W.; Mofatteh, M.; Regenhardt, R.W.; Wellington, J.; Liang, Z.; Tang, Q.; Chen, J.; et al. The Impact of COVID-19 Pandemic Lockdown on Emergency Department Visits in a Tertiary Hospital. Risk Manag. Healthc Policy 2023, 16, 1309–1316. [Google Scholar] [CrossRef]
- Sekadakis, M.; Katrakazas, C.; Michelaraki, E.; Kehagia, F.; Yannis, G. Analysis of the impact of COVID-19 on collisions, fatalities and injuries using time series forecasting: The case of Greece. Accid. Anal. Prev. 2021, 162, 106391. [Google Scholar] [CrossRef]
- Ronnebaum, J.A.; Weir, J.P.; Hilsabeck, T.A. Earlier Mobilization Decreases the Length of Stay in the Intensive Care Unit. Acute Care Phys. Ther. 2012, 3, 204–210. [Google Scholar] [CrossRef]
- Roychoudhury, S.; Das, A.; Sengupta, P.; Dutta, S.; Roychoudhury, S.; Choudhury, A.P.; Ahmed, A.B.F.; Bhattacharjee, S.; Slama, P. Viral Pandemics of the Last Four Decades: Pathophysiology, Health Impacts and Perspectives. Int. J. Environ. Res. Public Health 2020, 17, 9411. [Google Scholar] [CrossRef] [PubMed]
- Rubinson, L.; Mutter, R.; Viboud, C.; Hupert, N.; Uyeki, T.; Creanga, A.; Finelli, L.; Iwashyna, T.J.; Carr, B.; Merchant, R.; et al. Impact of the fall 2009 influenza A(H1N1)pdm09 pandemic on US hospitals. Med. Care 2013, 51, 259–265. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severity Scoring System | Determining Variables | Utility |
|---|---|---|
| Glasgow Coma Scale (GCS) Scale 3 (high severity) to 15 (low severity) | Eye response, verbal response, motor response | Higher scores correlate with better neurological function |
| Revised Trauma Score (RTS) Scale 0 (high severity) to 12 (low severity) | GCS, systolic pressure, respiratory rate | Higher scores correlate with greater survival rate and better outcome |
| Injury Severity Score (ISS) Scale 1 (low severity) to 75 (high severity) | Top 3 body region injuries | Higher scores correlate with low probability of survival |
| New Injury Severity Score (NISS) Scale 1 (low severity) to 75 (high severity) | Top 3 injuries regardless of body region | Higher scores correlate with low probability of survival |
| Trauma and Injury Severity Score (TRISS) Scale 0 (high severity) to 1 (low severity) | RTS and ISS | Higher scores correlate with high probability of survival |
| Patient Characteristics | Before COVID Onset (n = 378) | After COVID Onset (n = 499) | p Value |
|---|---|---|---|
| Age at Admission, years (IQR) | 50 (42.25) | 55 (40) | 0.70 |
| Gender, n (%) | 0.86 | ||
| Male | 244 (64.6%) | 325 (65.1%) | |
| Female | 134 (35.4%) | 174 (34.9%) | |
| Ethnicity, n (%) | 0.46 | ||
| Hispanic or Latino | 16 (4.0%) | 24 (4.8%) | |
| Not Hispanic or Latino | 361 (96.0%) | 475 (95.2%) | |
| Race, n (%) | 0.016 | ||
| White or Caucasian | 305 (80.7%) | 368 (73.8%) | |
| Other (Asian, Black/African American, Native Hawaiian, Pacific Islander, Refused) | 73 (19.3%) | 131 (26.2%) | |
| Vitals | |||
| Height, meters (IQR) | 1.73 (0.15) | 1.73 (0.15) | 1.73 (0.15) |
| Weight, kilograms (IQR) | 79.9 (27.03) | 80.45 (29.88) | 80.45 (29.88) |
| Body Mass Index (IQR) | 26.89 (8.58) | 26.65 (8.40) | 26.65 (8.40) |
| Systolic Blood Pressure (IQR) | 132 (36.25) | 132 (34) | 132 (34) |
| Diastolic Blood Pressure (IQR) | 81 (22.25) | 81 (22) | 81 (22) |
| Pulse (IQR) | 89 (29) | 87 (30) | 87 (30) |
| Respiratory Rate (IQR) | 18 (4) | 18 (6) | 18 (6) |
| SpO2 (IQR) | 97 (5) | 97 (4) | 97 (4) |
| Injury type, n (%) | 0.29 | ||
| Blunt | 349 (92.3%) | 447 (89.6%) | |
| Penetrating | 29 (7.7%) | 51 (10.2%) | |
| Other (thermal, not applicable) | 0 | 1 (0.2%) | |
| Chief mechanisms of injury, n (%) | 0.046 | ||
| Fall | 161 (42.6%) | 176 (35.3%) | |
| Gunshot wound | 17 (4.5%) | 41 (8.2%) | |
| Motor vehicle crash | 177 (46.8%) | 250 (50.1%) | |
| Other (assault, bicycle, burn, knife, pedestrian, puncture wound, other blunt mechanism, other penetrating mechanism, struck by object or person, unknown) | 23 (6.1%) | 32 (6.4%) | |
| Injury severity | |||
| Severe ISS, n (%) | 177 (46.83%) | 292 (58.52%) | 0.001 |
| TRISS (IQR) | 0.968 (0.044) | 0.965 (0.068) | 0.014 |
| ISS (IQR) | 14 (13) | 17 (15) | <0.001 |
| NISS (IQR) | 17 (16) | 22 (16) | <0.001 |
| RTS (IQR) | 12 (1) | 12 (1) | 0.21 |
| Comorbidities (%) | Before COVID Onset (n = 378) | After COVID Onset (n = 499) | p Value |
|---|---|---|---|
| Total comorbidities (IQR) | 1 (2.25) | 2 (2) | 0.0067 |
| Currently receiving chemotherapy | 2 (0.53%) | 5 (1.00%) | 0.44 |
| Congenital anomalies | 3 (0.79%) | 2 (0.40%) | 0.44 |
| Congestive heart failure | 29 (7.67%) | 52 (10.42%) | 0.16 |
| Smoker | 91 (24.07%) | 136 (27.25%) | 0.29 |
| Renal failure | 29 (7.67%) | 45 (9.02%) | 0.48 |
| Prior cerebral vascular accident | 23 (6.08%) | 48 (9.62%) | 0.057 |
| Diabetes | 77 (20.37%) | 83 (16.63%) | 0.16 |
| Disseminated cancer | 2 (0.53%) | 30 (6.01%) | <0.0001 |
| Advanced directive limiting care | 8 (2.12%) | 63 (12.63%) | <0.0001 |
| History of angina | 1 (0.26%) | 1 (0.20%) | 0.84 |
| Prior myocardial infarction | 16 (4.23%) | 31 (6.21%) | 0.20 |
| Peripheral vascular disease | 19 (5.03%) | 28 (5.61%) | 0.70 |
| Hypertension | 161 (42.59%) | 204 (40.88%) | 0.61 |
| COPD | 30 (7.94%) | 35 (7.01%) | 0.61 |
| Steroid use | 0 (0%) | 5 (1.00%) | 0.051 |
| Cirrhosis | 9 (2.38%) | 12 (2.40%) | 0.98 |
| Other major non-psychiatric disorder | 1 (0.27%) | 4 (0.8%) | 0.30 |
| EtOH use disorder | 37 (9.79%) | 59 (11.82%) | 0.34 |
| Other substance use disorder | 41 (10.85%) | 68 (13.63%) | 0.22 |
| Dementia | 19 (5.03%) | 18 (3.61%) | 0.30 |
| ADHD | 10 (2.65%) | 9 (1.80%) | 0.40 |
| Other major psychiatric disorder | 65 (17.20%) | 112 (22.44%) | 0.0551 |
| Complications (%) | Before COVID Onset (n = 378) | After COVID Onset (n = 499) | p Value |
|---|---|---|---|
| Total complications (IQR) | 0 (0) | 0 (1) | 0.0046 |
| Deep surgical infection | 4 (1.06%) | 5 (1.00%) | 0.93 |
| Drug/EtOH substance use disorder | 4 (1.06%) | 8 (1.06%) | 0.49 |
| Deep venous thrombosis (DVT) | 15 (3.97%) | 21 (4.21%) | 0.86 |
| Compartment syndrome | 1 (0.26%) | 2 (0.40%) | 0.73 |
| Graft/prosthesis/flap failure | 0 (0%) | 1 (0.20%) | 0.38 |
| Myocardial infarction | 0 (0%) | 2 (0.40%) | 0.22 |
| Organ space infection | 0 (0%) | 2 (0.40%) | 0.22 |
| Osteomyelitis | 4 (1.06%) | 1 (0.20%) | 0.095 |
| Pneumonia | 43 (11.38%) | 58 (11.62%) | 0.91 |
| Pulmonary embolism | 3 (0.79%) | 7 (1.40%) | 0.40 |
| Sepsis | 16 (4.23%) | 23 (6.81%) | 0.10 |
| Stroke/cerebral vascular accident | 2 (0.53%) | 12 (2.40%) | 0.028 |
| Superficial infection | 3 (0.79%) | 5 (1.00%) | 0.75 |
| Urinary tract infection | 11 (2.91%) | 14 (2.81%) | 0.93 |
| Hospital Stay Characteristics | Before COVID Onset (n = 378) | After COVID Onset (n = 499) | p Value |
|---|---|---|---|
| Weekend vs. Weekday Admission, n (%) | 0.66 | ||
| Weekday | 263 (69.6%) | 354 (70.9%) | |
| Weekend | 115 (30.4%) | 145 (29.1%) | |
| Day of the Week Admission, n (%) | 0.51 | ||
| Sunday | 48 (12.7%) | 71 (14.2%) | |
| Monday | 57 (15.1%) | 71 (14.2%) | |
| Tuesday | 53 (14.0%) | 58 (11.6%) | |
| Wednesday | 42 (11.1%) | 75 (15.0%) | |
| Thursday | 56 (14.8%) | 72 (14.4%) | |
| Friday | 55 (14.6%) | 78 (15.6%) | |
| Saturday | 67 (17.7%) | 74 (14.8%) | |
| Received PT, n (%) | 215 (56.9%) | 302 (60.6%) | 0.97 |
| PT Time to Mobilization, day (IQR) | 4 (4) | 3 (3.25) | 0.86 |
| Discharge Status, n (%) | 0.001 | ||
| Alive | 360 (95.2%) | 445 (89.2%) | |
| Expired | 18 (4.8%) | 54 (10.8%) | |
| Readmission | |||
| Patients Readmitted, n (%) | 23 (6.08%) | 70 (14.03%) | 0.0003 |
| Days Post ED Before Readmission, days (IQR) | 23.92 (37.47) | 42.00 (83.21) | 0.04 |
| Length of Readmission Stay, days (IQR) | 5 (10) | 2 (3.92) | 0.03 |
| Patient Characteristics | Not Mobilized (n = 171) | Mobilized (n = 328) | p Value |
|---|---|---|---|
| Age at Admission, years (IQR) | 50 (38) | 57 (41) | 0.005 |
| Gender, n (%) | 0.004 | ||
| Male | 126 (73.7%) | 199 (60.7%) | |
| Female | 45 (26.3%) | 129 (39.3%) | |
| Ethnicity, n (%) | 0.57 | ||
| Hispanic or Latino | 6 (3.5%) | 13 (4.0%) | |
| Not Hispanic or Latino | 164 (96.5%) | 309 (96.0%) | |
| Race, n (%) | 0.51 | ||
| White or Caucasian | 123 (71.9%) | 245 (74.7%) | |
| Other (Asian, Black/African American, Native Hawaiian, Pacific Islander, Refused) | 48 (28.1%) | 83 (25.3%) | |
| Vitals | |||
| Height, meters (IQR) | 1.75 (0.15) | 1.727 (0.17) | 0.071 |
| Weight, kilograms (IQR) | 81.6 (29.7) | 79.5 (30.7) | 0.95 |
| Body Mass Index (IQR) | 26.75 (8.81) | 26.63 (8.32) | 0.57 |
| Systolic Blood Pressure (IQR) | 131 (47) | 132.5 (32.49) | 0.78 |
| Diastolic Blood Pressure (IQR) | 81 (24) | 81 (21.75) | 0.091 |
| Pulse (IQR) | 88 (27) | 86.5 (32) | 0.25 |
| Respiratory Rate (IQR) | 18 (6) | 18 (6) | 0.79 |
| SpO2 (IQR) | 98 (5) | 97 (4) | 0.33 |
| Injury Type, n (%) | <0.001 | ||
| Blunt | 141 (82.4%) | 305 (93.3%) | |
| Penetrating | 30 (17.5%) | 21 (6.4%) | |
| Other (thermal, not applicable) | 0 (0%) | 1 (0.3%) | |
| Chief Mechanisms of Injury, n (%) | <0.001 | ||
| Fall | 53 (30.1%) | 123 (37.5%) | |
| Gunshot wound | 26 (15.2%) | 15 (4.6%) | |
| Motor vehicle crash | 76 (44.4%) | 174 (53.0%) | |
| Other (assault, bicycle, burn, knife, pedestrian, puncture wound, other blunt mechanism, other penetrating mechanism, struck by object or person, unknown) | 16 (9.4%) | 16 (4.9%) | |
| Injury Severity | |||
| Severe ISS, n (%) | 99 (33.9%) | 193 (66.1%) | <0.001 |
| TRISS (IQR) | 0.97 (0.0985) | 0.97 (0.056) | 0.27 |
| ISS (IQR) | 17 (16) | 17 (14) | 0.73 |
| NISS (IQR) | 22 (22) | 22 (15) | 0.028 |
| RTS (IQR) | 12 (2) | 2 (0.75) | <0.001 |
| Comorbidities (%) | Not Mobilized (n = 171) | Mobilized (n = 328) | p Value |
|---|---|---|---|
| Total comorbidities (IQR) | 2 (3) | 2 (2) | 0.089 |
| Currently receiving chemotherapy | 3 (1.75%) | 2 (0.61%) | 0.22 |
| Congenital anomalies | 1 (0.58%) | 1 (0.30%) | 0.64 |
| Congestive heart failure | 18 (10.53%) | 34 (10.37%) | 0.96 |
| Smoker | 53 (30.99%) | 83 (25.30%) | 0.18 |
| Renal failure | 15 (8.77%) | 30 (9.15%) | 0.89 |
| Prior cerebral vascular accident | 17 (9.94%) | 31 (9.45%) | 0.86 |
| Diabetes | 32 (18.71%) | 51 (15.55%) | 0.37 |
| Disseminated cancer | 12 (7.02%) | 18 (5.49%) | 0.50 |
| Advanced directive limiting care | 42 (24.56%) | 21 (6.40%) | <0.0001 |
| History of angina | 0 (0%) | 1 (0.30%) | 0.47 |
| Prior myocardial infarction | 10 (5.85%) | 21 (6.40%) | 0.81 |
| Peripheral vascular disease | 11 (6.43%) | 17 (5.18%) | 0.56 |
| Hypertension | 61 (35.67%) | 143 (43.60%) | 0.087 |
| COPD | 11 (6.43%) | 24 (7.32%) | 0.71 |
| Steroid use | 0 (0%) | 5 (1.52%) | 0.10 |
| Cirrhosis | 8 (4.68%) | 4 (1.22%) | 0.017 |
| Other major non-psychiatric disorder | 2 (1.17%) | 2 (0.61%) | 0.51 |
| EtOH use disorder | 25 (14.62%) | 34 (10.37%) | 0.16 |
| Other substance use disorder | 29 (16.96%) | 39 (11.89%) | 0.12 |
| Dementia | 7 (4.09%) | 11 (3.35%) | 0.67 |
| ADHD | 3 (1.75%) | 6 (1.83%) | 0.95 |
| Other major psychiatric disorder | 33 (19.30%) | 79 (24.09%) | 0.22 |
| Complications (%) | Not Mobilized (n = 171) | Mobilized (n = 328) | p Value |
|---|---|---|---|
| Total complications (IQR) | 0 (1) | 0 (1) | 0.5775 |
| Deep surgical infection | 0 (0%) | 5 (1.52%) | 0.10 |
| Drug/EtOH substance use disorder | 2 (1.17%) | 6 (1.83%) | 0.58 |
| Deep venous thrombosis (DVT) | 8 (4.68%) | 13 (3.96%) | 0.71 |
| Compartment syndrome | 0 (0%) | 2 (0.61%) | 0.31 |
| Graft/prosthesis/flap failure | 0 (0%) | 1 (0.30%) | 0.47 |
| Myocardial infarction | 2 (1.17%) | 0 (0%) | 0.05 |
| Organ space infection | 0 (0%) | 2 (0.61%) | 0.31 |
| Osteomyelitis | 0 (0%) | 1 (0.30%) | 0.47 |
| Pneumonia | 20 (11.70%) | 38 (11.59%) | 0.97 |
| Pulmonary embolism | 0 (0%) | 7 (2.13%) | 0.054 |
| Sepsis | 11 (6.43%) | 23 (7.01%) | 0.81 |
| Stroke/cerebral vascular accident | 6 (3.51%) | 6 (1.83%) | 0.25 |
| Superficial infection | 0 (0%) | 5 (1.52%) | 0.10 |
| Urinary tract infection | 2 (1.17%) | 12 (3.66%) | 0.11 |
| Hospital Stay Characteristics | Not Mobilized (n = 171) | Mobilized (n = 328) | p Value |
|---|---|---|---|
| Weekend vs. Weekday Admission, n (%) | 0.785 | ||
| Weekday | 120 (70.2%) | 234 (71.3%) | |
| Weekend | 51 (29.8%) | 94 (28.6%) | |
| Day of the Week Admission, n (%) | 0.292 | ||
| Sunday | 20 (11.7%) | 51 (15.5%) | |
| Monday | 25 (14.6%) | 46 (14.0%) | |
| Tuesday | 18 (10.5%) | 40 (12.2%) | |
| Wednesday | 21 (12.3%) | 54 (16.5%) | |
| Thursday | 31 (18.1%) | 41 (12.5%) | |
| Friday | 25 (14.6%) | 53 (16.2%) | |
| Saturday | 31 (18.1%) | 43 (13.1%) | |
| PT Time to Mobilization, day (IQR) | - | 3 (3.25) | - |
| Hospital Days, day (IQR) | 3 (4) | 8 (8) | <0.001 |
| Intensive Care Unit Days, day (IQR) | 2 (2) | 3 (3) | 0.053 |
| Ventilatory Days, day (IQR) | 3 (4) | 4 (8) | 0.076 |
| Total Complications, n (IQR) | 0 (1) | 0 (1) | 0.578 |
| Discharge Status, n (%) | <0.001 | ||
| Alive | 124 (72.5%) | 321 (97.9%) | |
| Expired | 47 (27.5%) | 7 (2.1%) | |
| Readmission | |||
| Readmission | 0.001 | ||
| No Patient Readmission, n (%) | 161 (94.2%) | 268 (81.7%) | |
| Patients Readmission, n (%) | 10 (5.8%) | 60 (18.3%) | |
| Days Post ED Before Readmission, days (IQR) | 68.76 (91.05) | 34.68 (87.52) | 0.908 |
| Length of Readmission Stay, days (IQR) | 2 (4.69) | 3 (3.46) | 0.781 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro, Y.; Huang, E.; Johnson, C.; Clark, F.; Coppola, S.; Modi, S.; Warren, G.L.; Call, J.A. The Influence of COVID-19 on Patient Mobilization and Injury Attributes in the ICU: A Retrospective Analysis of a Level II Trauma Center. Trauma Care 2024, 4, 44-59. https://doi.org/10.3390/traumacare4010005
Navarro Y, Huang E, Johnson C, Clark F, Coppola S, Modi S, Warren GL, Call JA. The Influence of COVID-19 on Patient Mobilization and Injury Attributes in the ICU: A Retrospective Analysis of a Level II Trauma Center. Trauma Care. 2024; 4(1):44-59. https://doi.org/10.3390/traumacare4010005
Chicago/Turabian StyleNavarro, Yelissa, Elizabeth Huang, Chandler Johnson, Forrest Clark, Samuel Coppola, Suraj Modi, Gordon L. Warren, and Jarrod A. Call. 2024. "The Influence of COVID-19 on Patient Mobilization and Injury Attributes in the ICU: A Retrospective Analysis of a Level II Trauma Center" Trauma Care 4, no. 1: 44-59. https://doi.org/10.3390/traumacare4010005
APA StyleNavarro, Y., Huang, E., Johnson, C., Clark, F., Coppola, S., Modi, S., Warren, G. L., & Call, J. A. (2024). The Influence of COVID-19 on Patient Mobilization and Injury Attributes in the ICU: A Retrospective Analysis of a Level II Trauma Center. Trauma Care, 4(1), 44-59. https://doi.org/10.3390/traumacare4010005