
Does a Preoperative Carbohydrate Drink Reduce Postoperative Inflammation? A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Data Extraction
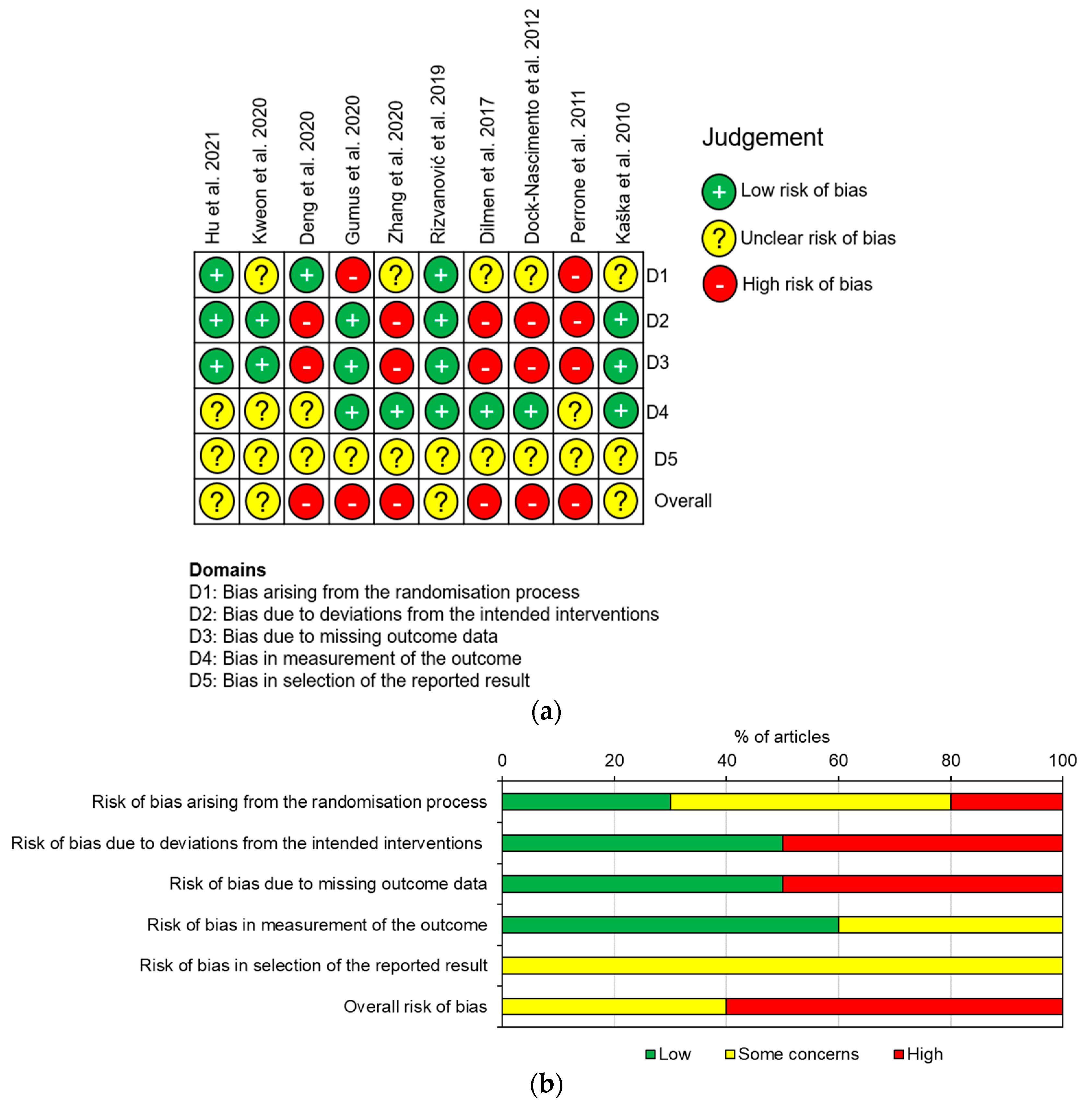
2.5. Risk of Bias
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
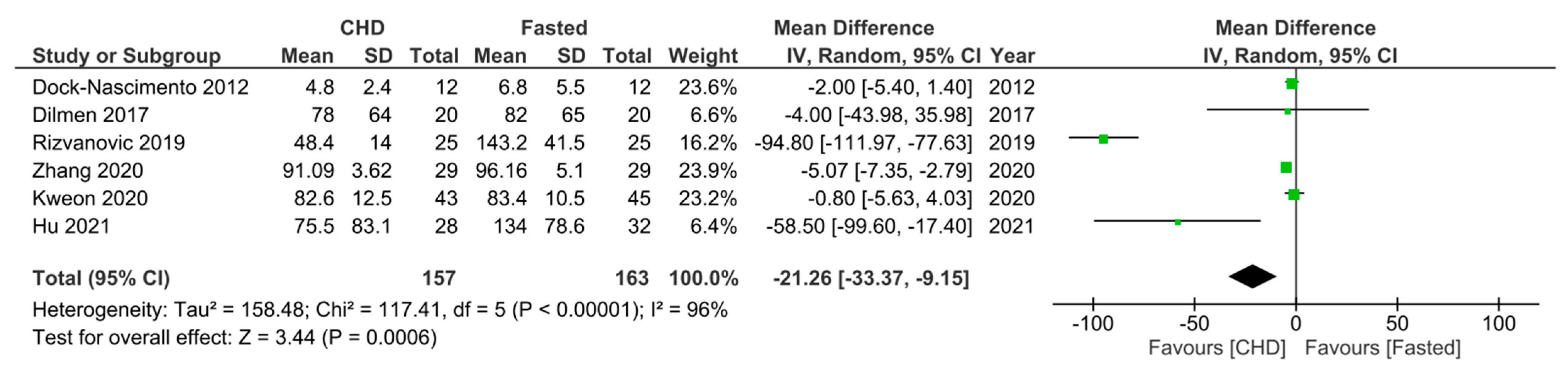
3.4. Primary Outcomes
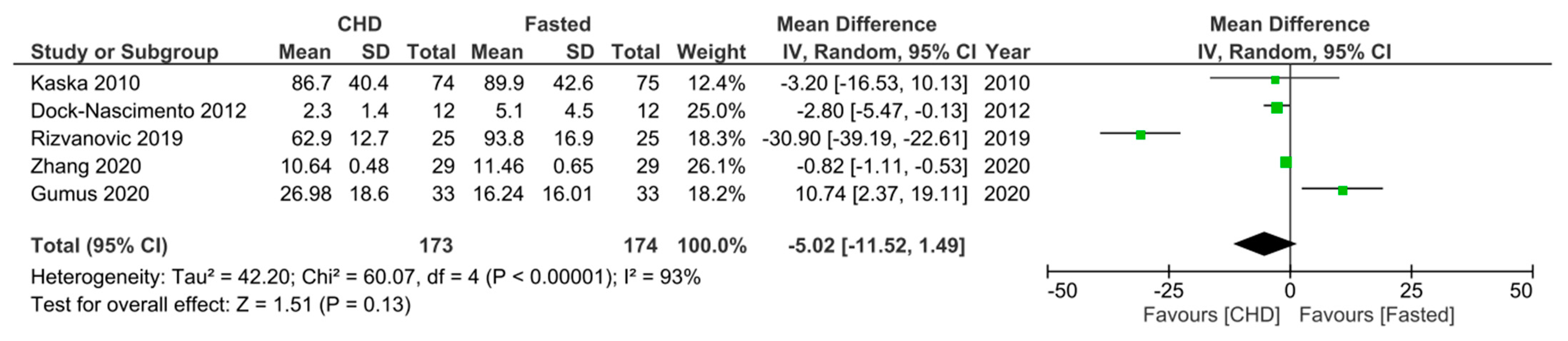
3.5. Secondary Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maltby, J.R. Fasting from midnight—The history behind the dogma. Best Pract. Res. Clin. Anaesthesiol. 2006, 20, 363–378. [Google Scholar] [CrossRef] [PubMed]
- Nygren, J.; Thorell, A.; Jacobsson, H.; Larsson, S.; Schnell, P.-O.; Hylén, L.; Ljungqvist, O. Preoperative gastric emptying. Effects of anxiety and oral carbohydrate administration. Ann. Surg. 1995, 222, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.N.; Hendry, P.O.; Rodrigues, G.; Marciani, L.; Totman, J.J.; Wright, J.W.; Preston, T.; Gowland, P.; Spiller, R.C.; Fearon, K.C.H. Gastric emptying of three liquid oral preoperative metabolic preconditioning regimens measured by magnetic resonance imaging in healthy adult volunteers: A randomised double-blind, crossover study. Clin. Nutr. ESPEN 2009, 28, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Brady, M.C.; Kinn, S.; Stuart, P.; Ness, V. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst. Rev. 2003, 4, CD004423. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Harsanyi, L.; Laviano, A.; Ljungqvist, O.; Soeters, P.; DGEM; Jauch, K.W.; Kemen, M.; Hiesmayr, J.M.; et al. ESPEN Guidelines on Enteral Nutrition: Surgery including Organ Transplantation. Clin. Nutr. ESPEN 2006, 25, 224–244. [Google Scholar] [CrossRef]
- Feldheiser, A.; Aziz, O.; Baldini, G.; Cox, B.P.B.W.; Fearon, K.C.H.; Feldman, L.S.; Gan, T.J.; Kennedy, R.H.; Ljungqvist, O.; Lobo, D.N.; et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 2: Consensus statement for anaesthesia practice. Acta Anaesthesiol. Scand. 2016, 60, 289–334. [Google Scholar] [CrossRef]
- Gustafsson, U.O.; Scott, M.J.; Schwenk, W.; Demartines, N.; Roulin, D.; Francis, N.; McNaught, C.E.; MacFie, J.; Liberman, A.S.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colonic Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2013, 37, 259–284. [Google Scholar] [CrossRef]
- Fearon, K.C.H.; Ljungqvist, O.; Von Meyenfeldt, M.; Revhaug, A.; Dejong, C.H.C.; Lassen, K.; Nygren, J.; Hausel, J.; Soop, M.; Andersen, J.; et al. Enhanced recovery after surgery: A consensus review of clinical care for patients undergoing colonic resection. Clin. Nutr. ESPEN 2005, 24, 466–477. [Google Scholar] [CrossRef]
- Nelson, G.; Fotopoulou, C.; Taylor, J.; Glaser, G.; Bakkum-Gamez, J.; Meyer, L.A.; Stone, R.; Mena, G.; Elias, K.M.; Altman, A.D.; et al. Enhanced recovery after surgery (ERAS®) society guidelines for gynecologic oncology: Addressing implementation challenges—2023 update. Gynecol. Oncol. 2023, 173, 58–67. [Google Scholar] [CrossRef]
- Bilku, D.K.; Dennison, A.R.; Hall, T.C.; Metcalfe, M.S.; Garcea, G. Role of preoperative carbohydrate loading: A systematic review. Ann. R. Coll. Surg. Engl. 2014, 96, 15–22. [Google Scholar] [CrossRef]
- Hausel, J.; Nygren, J.; Lagerkranser, M.; Hellström, P.M.; Hammarqvist, F.; Almström, C.; Lindh, A.; Thorell, A.; Ljungqvist, O. A Carbohydrate-Rich Drink Reduces Preoperative Discomfort in Elective Surgery Patients. Anesth. Analg. 2001, 93, 1344–1350. [Google Scholar] [CrossRef] [PubMed]
- Noblett, S.E.; Watson, D.S.; Huong, H.; Davison, B.; Hainsworth, P.J.; Horgan, A.F. Pre-operative oral carbohydrate loading in colorectal surgery: A randomized controlled trial. Colorectal Dis. 2006, 8, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Falconer, R.; Skouras, C.; Carter, T.; Greenway, L.; Paisley, A.M. Preoperative fasting: Current practice and areas for improvement. Updates Surg. 2014, 66, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Degeeter, T.; Demey, B.; Caelenberg, E.V.; Baerdemaeker, L.D.; Coppens, M. Prospective audit on fasting status of elective ambulatory surgery patients, correlated to gastric ultrasound. Acta Chir. Belg. 2023, 123, 43–48. [Google Scholar] [CrossRef]
- Nygren, J.; Soop, M.; Thorell, A.; Efendic, S.; Nair, K.S.; Ljungqvist, O. Preoperative oral carbohydrate administration reduces postoperative insulin resistance. Clin. Nutr. ESPEN 1998, 17, 65–71. [Google Scholar] [CrossRef]
- Rizvanović, N.; Adam, V.N.; Čaušević, S.; Dervišević, S.; Delibegović, S. A randomised controlled study of preoperative oral carbohydrate loading versus fasting in patients undergoing colorectal surgery. Int. J. Color. Dis. 2019, 34, 1551–1561. [Google Scholar] [CrossRef]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef]
- de Aguilar-Nascimento, J.E.; Marra, J.G.; Slhessarenko, N.; Fontes, C.J.F. Efficacy of National Nosocomial Infection Surveillance score, acute-phase proteins, and interleukin-6 for predicting postoperative infections following major gastrointestinal surgery. Sao Paulo Med. J. 2007, 125, 34–41. [Google Scholar] [CrossRef]
- Hu, Z.; Liu, J.; Wang, F. Effects of Preoperative Carbohydrate Intake on Inflammatory Markers and Clinical Outcomes in Elderly Patients Undergoing Radical Prostatectomy: A Single-Centre, Double-Blind Randomised Controlled Trial. Front. Surg. 2021, 8, 744091. [Google Scholar] [CrossRef]
- Oka, Y.; Murata, A.; Nishijima, J.; Yasuda, T.; Hiraoka, N.; Ohmachi, Y.; Kitagawa, K.; Yasuda, T.; Toda, H.; Tanaka, N.; et al. Circulating interleukin 6 as a useful marker for predicting postoperative complications. Cytokine X 1992, 4, 298–304. [Google Scholar] [CrossRef]
- Mokart, D.; Capo, C.; Blache, J.L.; Delpero, J.R.; Houvenaeghel, G.; Martin, C.; Mege, J.L. Early postoperative compensatory anti-inflammatory response syndrome is associated with septic complications after major surgical trauma in patients with cancer. Br. J. Surg. 2002, 89, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Ricci, C.; Ingaldi, C.; Alberici, L.; Serbassi, F.; Pagano, N.; De Raffele, E.; Minni, F.; Pironi, L.; Sasdelli, A.S.; Casadei, R. Preoperative carbohydrate loading before elective abdominal surgery: A systematic review and network meta-analysis of phase II/III randomized controlled trials. Clin. Nutr. ESPEN 2022, 41, 313–320. [Google Scholar] [CrossRef]
- Tong, E.; Chen, Y.; Ren, Y.; Zhou, Y.; Di, C.; Zhou, Y.; Shao, S.; Qui, S.; Hong, Y.; Yang, L.; et al. Effects of preoperative carbohydrate loading on recovery after elective surgery: A systematic review and Bayesian network meta-analysis of randomized controlled trials. Front. Nutr. 2022, 9, 951676. [Google Scholar] [CrossRef]
- Perrone, F.; da-Silva-Filho, A.C.; Adôrno, I.F.; Anabuki, N.T.; Leal, F.S.; Colombo, T.; da Silva, B.D.; Dock-Nascimento, D.B.; Damião, A.; de Aguilar-Nascimento, J.E. Effects of preoperative feeding with a whey protein plus carbohydrate drink on the acute phase response and insulin resistance. A randomized trial. Nutr. J. 2011, 10, 66. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Kweon, S.-H.; Park, J.S.; Lee, Y.C. Oral Carbohydrate Administration in Patients Undergoing Cephalomedullary Nailing for Proximal Femur Fractures: An Analysis of Clinical Outcomes and Patient Satisfaction. Geriatr. Orthop. Surg. Rehabil. 2020, 11, 2151459320958609. [Google Scholar] [CrossRef]
- Deng, Y.; Fang, Y.; Li, H.; Chen, J.; An, J.; Qiao, S.; Wang, C. A preoperative whey protein and glucose drink before hip fracture surgery in the aged improves symptomatic and metabolic recovery. Asia Pac. J. Clin. Nutr. 2020, 29, 234–238. [Google Scholar] [CrossRef]
- Gumus, K.; Aydın, G. The Effect of Preoperative Nutrition on Postoperative CRP and Albumin Levels in Patients Undergoing Laparoscopic Surgery: A Surgical Nursing Perspective. J. Perianesth. Nurs. 2020, 35, 592–596. [Google Scholar] [CrossRef]
- Zhang, Y.; Min, J. Preoperative Carbohydrate Loading in Gynecological Patients Undergoing Combined Spinal and Epidural Anesthesia. J. Investig. Surg. 2020, 33, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Dilmen, O.K.; Yentur, E.; Tunali, Y.; Balci, H.; Bahar, M. Does preoperative oral carbohydrate treatment reduce the postoperative surgical stress response in lumbar disc surgery? Clin. Neurol. Neurosurg. 2017, 153, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Dock-Nascimento, D.B.; de Aguilar-Nascimento, J.E.; Faria, M.S.M.; Caporossi, C.; Slhessarenko, N.; Waitzberg, D.L. Evaluation of the Effects of a Preoperative 2-Hour Fast with Maltodextrine and Glutamine on Insulin Resistance, Acute-Phase Response, Nitrogen Balance, and Serum Glutathione After Laparoscopic Cholecystectomy. JPEN J. Parenter. Enteral. Nutr. 2012, 36, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Kaška, M.; Grosmanová, T.; Havel, E.; Hyšpler, R.; Petrová, Z.; Brtko, M.; Bareš, P.; Bareš, D.; Schusterová, B.; Pyszková, L.; et al. The impact and safety of preoperative oral or intravenous carbohydrate administration versus fasting in colorectal surgery—A randomized controlled trial. Wien. Klin. Wochenschr. 2010, 122, 23–30. [Google Scholar] [CrossRef]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How Many Studies Do You Need? A Primer on Statistical Power for Meta-Analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Li, L.; Wang, Z.; Ying, X.; Tian, J.; Sun, T.; Yi, K.; Zhang, P.; Jing, Z.; Yang, K. Preoperative carbohydrate loading for elective surgery: A systematic review and meta-analysis. Surg. Today 2012, 42, 613–624. [Google Scholar] [CrossRef]
- Smith, M.D.; McCall, J.; Plank, L.; Herbison, G.P.; Soop, M.; Nygren, J. Preoperative carbohydrate treatment for enhancing recovery after elective surgery. Cochrane Database Syst. Rev. 2014, 8, CD009161. [Google Scholar] [CrossRef]
- Amer, M.A.; Smith, M.D.; Herbison, G.P.; Plank, L.D.; McCall, J.L. Network meta-analysis of the effect of preoperative carbohydrate loading on recovery after elective surgery. Br. J. Surg. 2017, 104, 187–197. [Google Scholar] [CrossRef]
- Cheng, P.-L.; Loh, E.-W.; Chen, J.-T.; Tam, K.-W. Effects of preoperative oral carbohydrate on postoperative discomfort in patients undergoing elective surgery: A meta-analysis of randomized controlled trials. Langenbecks Arch. Surg. 2021, 406, 993–1005. [Google Scholar] [CrossRef]
- Sato, H.; Carvalho, G.; Sato, T.; Lattermann, R.; Matsukawa, T.; Schricker, T. The Association of Preoperative Glycemic Control, Intraoperative Insulin Sensitivity, and Outcomes after Cardiac Surgery. J. Clin. Endocrinol. Metab. 2010, 95, 4338–4344. [Google Scholar] [CrossRef]
- Wang, X.; Hu, Z.; Hu, J.; Du, J.; Mitch, W.E. Insulin Resistance Accelerates Muscle Protein Degradation: Activation of the Ubiquitin-Proteasome Pathway by Defects in Muscle Cell Signaling. Endocrinology 2006, 147, 4160–4168. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.; Bissolati, M.; Rocchetti, S.; Beneduce, A.; Pecorelli, N.; Carlo, V.D. Oral preoperative antioxidants in pancreatic surgery: A double-blind, randomized, clinical trial. Nutrition 2012, 28, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Pexe-Machado, P.A.; de Oliveira, B.D.; Dock-Nascimento, D.B.; de Aguilar-Nascimento, J.E. Shrinking preoperative fast time with maltodextrin and protein hydrolysate in gastrointestinal resections due to cancer. Nutrition 2013, 29, 1054–1059. [Google Scholar] [CrossRef] [PubMed]
- de Aguilar-Nascimento, J.E.; Dias, A.L.A.; Dock-Nascimento, D.B.; Correia, M.I.T.D.; Campos, A.C.L.; Portari-Filho, P.E.; Oliveira, S.S. Actual preoperative fasting time in Brazilian hospitals: The BIGFAST multicenter study. Ther. Clin. Risk Manag. 2014, 10, 107–112. [Google Scholar] [CrossRef]
- Johnson, A.; Sandford, J.; Tyndall, J. Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home. Cochrane Database Syst. Rev. 2003, 4, CD003716. [Google Scholar] [CrossRef]
- de Putte, P.V.; Vernieuwe, L.; Jerjir, A.; Verschueren, L.; Tacken, M.; Perlas, A. When fasted is not empty: A retrospective cohort study of gastric content in fasted surgical patients. Br. J. Anaesth. 2017, 118, 363–371. [Google Scholar] [CrossRef]
- Delgado-Rodríguez, M.; Llorca, J. Bias. J. Epidemiol. Community Health 2004, 58, 635–641. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Adults ≥ 18 years, elective surgical patients | Children < 18 years, animals, non-elective surgical patients, diabetes patients |
| Intervention | CHD 2–3 h preoperatively | Lack of CHD 2–3 h preoperatively, non-carbohydrate-containing drink, additional interventions alongside CHD |
| Comparison | Fasting ≥ 6 h, non-carbohydrate-containing PD | Carbohydrate-containing PD, No fasting or PD comparator |
| Outcomes | IL-6 and/or CRP and/or serum albumin levels 10–24 h postoperatively, mean levels available with CIs | IL-6 or CRP or serum albumin levels not within this time frame, lack of these inflammatory markers, mean levels with CIs not available |
| Study Design | RCTs | Other study designs |
| Study | Date | Country | Type of Surgery | Sample Size (M/F) | Relevant Cohorts | Contents of CHD | Volume and Timing of Drink(s) and Fasting | Outcomes Measured |
|---|---|---|---|---|---|---|---|---|
| Hu et al. [19] | 2021 | China | Prostatectomy | 90 (90/0) | (1) CHD (2) Fasting (3) Placebo | 12.6% carbohydrate solution | Drinks—400 m 2–3 h preop, Fasting—6 h preop | IL-6 |
| Kweon et al. [28] | 2020 | Korea | Femur fracture nailing | 88 (28/60) | (1) CHD (2) Fasting | 12.8% carbohydrate solution (vitamin A, B, C, D, E, and K, carbohydrate 15 g, fat 3 g, protein 4 g, vitamin A 75 ug, B1 0.13 mg, B2 0.15 mg, B6 0.15 mg, C 14 mg, D 1 ug, E 1.5 mg, K 7.5 ug per 100 mL) | Drink—400 mL 2 h preop, Fasting—7–8 h preop | IL-6 |
| Deng et al. [29] | 2020 | China | Hip fracture surgery | 40 (12, 28) | (1) CHD (3) Placebo | 10% carbohydrate solution (14% whey protein) | Drinks—200 mL 3 h preop | CRP, Serum Albumin |
| Gumus et al. [30] | 2020 | Turkey | Cholecystectomy | 66 (12, 54) | (1) CHD (2) Fasting | 12.5% carbohydrate solution | Drink—400 m 2 h proper, Fasting—12 h preop | CRP, Serum Albumin |
| Zhang et al. [31] | 2020 | China | Gynaecological surgery | 58 (0, 58) | (1) CHD (2) Fasting | 12.5% carbohydrate solution | Drink—400 mL 2 h preop, Fasting—8 h preop | IL-6, CRP |
| Rizvanović et al. [16] | 2019 | Bosnia and Herzegovina | Colorectal surgery | 50 (27, 23) | (1) CHD (2) Fasting | 12.5% carbohydrate solution | Drink—200 mL 2 h preop, Fasting—8 h preop | IL-6, CRP, Serum Albumin |
| Dilmen et al. [32] | 2017 | Turkey | Lumbar discectomy or laminectomy | 40 (20, 20) | (1) CHD (2) Fasting | 12.5% carbohydrate solution | Drink—400 mL 2 h preop, Fasting—8 h preop | IL-6 |
| Dock-Nascimento et al. [33] | 2012 | Brazil | Cholecystectomy | 48 (0, 48) | (1) CHD (2) Fasting (3) Placebo | 12.5% carbohydrate solution | Drinks—200 mL 2 h preop, Fasting—8 h preop | IL-6, CRP, Serum Albumin |
| Perrone et al. [24] | 2011 | Brazil | Cholecystectomy or inguinal hernia repair | 17 (6, 11) | (1) CHD (3) Placebo | 86% carbohydrate solution (14% whey protein) | Drinks—237 mL 3 h preop | CRP, Serum Albumin |
| Kaška et al. [34] | 2010 | Czech Republic | Colorectal surgery | 221 (122, 99) | (1) CHD (2) Fasting | 12.6% carbohydrate solution (Na 50 mg, K 122 mg, Cl 6 mg, Ca 6 mg, P 1 mg, Mg 1 mg) | Drink—400 mL 2 h preop, Fasting—6–12 h preop | CRP |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, K.Z.; Ahmed, Z. Does a Preoperative Carbohydrate Drink Reduce Postoperative Inflammation? A Systematic Review and Meta-Analysis. Trauma Care 2023, 3, 294-307. https://doi.org/10.3390/traumacare3040025
Haider KZ, Ahmed Z. Does a Preoperative Carbohydrate Drink Reduce Postoperative Inflammation? A Systematic Review and Meta-Analysis. Trauma Care. 2023; 3(4):294-307. https://doi.org/10.3390/traumacare3040025
Chicago/Turabian StyleHaider, Khasim Zakaria, and Zubair Ahmed. 2023. "Does a Preoperative Carbohydrate Drink Reduce Postoperative Inflammation? A Systematic Review and Meta-Analysis" Trauma Care 3, no. 4: 294-307. https://doi.org/10.3390/traumacare3040025
APA StyleHaider, K. Z., & Ahmed, Z. (2023). Does a Preoperative Carbohydrate Drink Reduce Postoperative Inflammation? A Systematic Review and Meta-Analysis. Trauma Care, 3(4), 294-307. https://doi.org/10.3390/traumacare3040025