Hip Flexibility and Dynamic Balance Ability in Soccer Players with Functional Ankle Instability


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. CAI
2.3. Hip Joint Range of Motion (ROM)
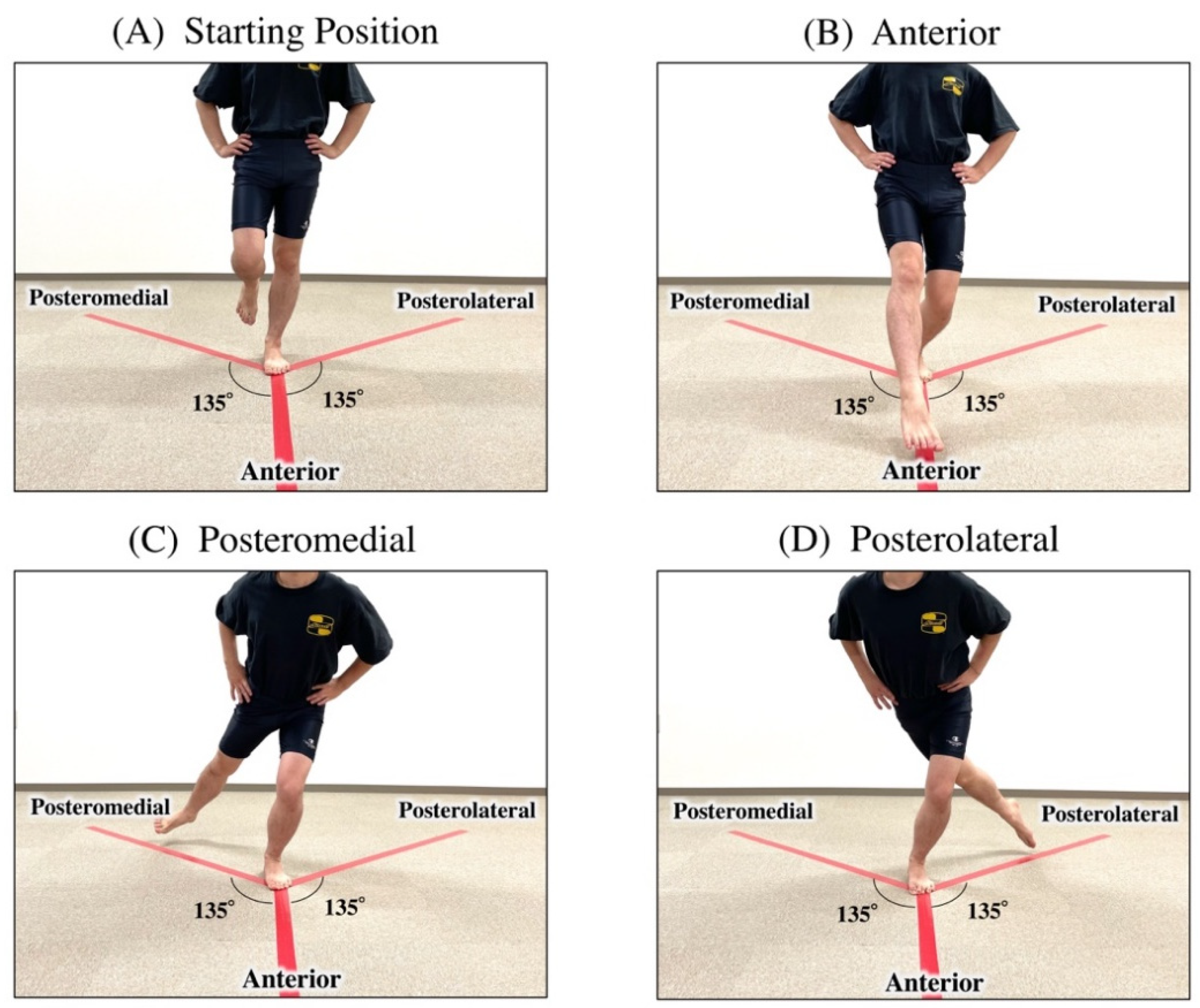
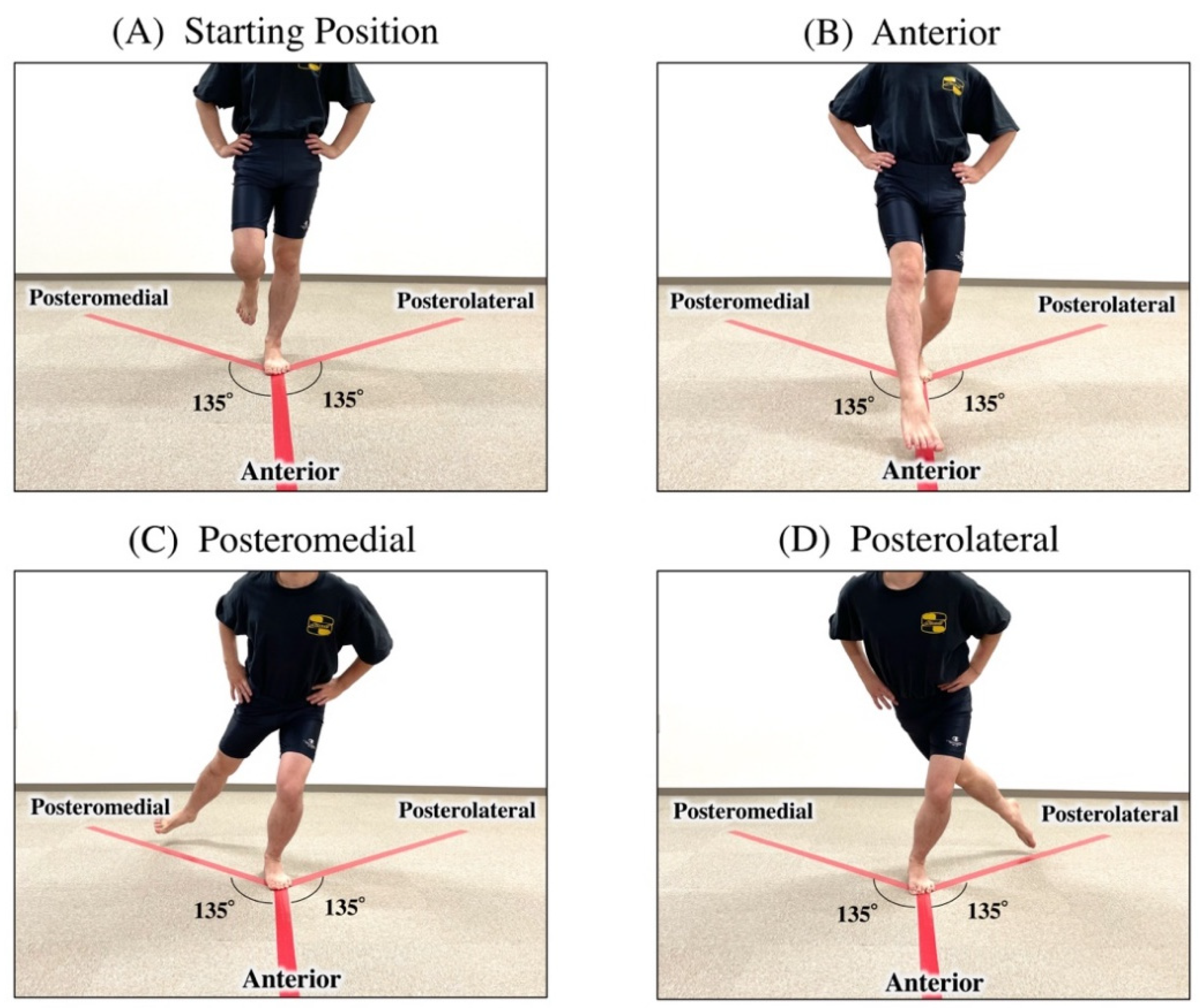
2.4. Dynamic Balance by the Modified SEBT
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swenson, D.M.; Collins, C.L.; Fields, S.K.; Comstock, R.D. Epidemiology of US High School Sports-Related Ligamentous Ankle Injuries, 2005/06–2010/11. Clin. J. Sport Med. 2013, 23, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Waldén, M.; Hägglund, M.; Ekstrand, J. Time-trends and circumstances surrounding ankle injuries in men’s professional football: An 11-year follow-up of the UEFA Champions League injury study. Br. J. Sports Med. 2013, 47, 748–753. [Google Scholar] [CrossRef] [Green Version]
- Woods, C.; Hawkins, R.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football: An analysis of ankle sprains. Br. J. Sports Med. 2003, 37, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walls, R.J.; Ross, K.; Fraser, E.J.; Hodgkins, C.W.; Smyth, N.A.; Egan, C.J.; Calder, J.; Kennedy, J.G. Football injuries of the ankle: A review of injury mechanisms, diagnosis and management. World J. Orthop. 2016, 7, 8–19. [Google Scholar] [CrossRef] [Green Version]
- Yeung, M.S.; Chan, K.M.; So, C.H.; Yuan, W.Y. An epidemiological survey on ankle sprain. Br. J. Sports Med. 1994, 28, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Tyler, T.F.; McHugh, M.P.; Mirabella, M.R.; Mullaney, M.J.; Nicholas, S.J. Risk Factors for Noncontact Ankle Sprains in High School Football Players. Am. J. Sports Med. 2006, 34, 471–475. [Google Scholar] [CrossRef]
- Jain, N.; Murray, D.; Kemp, S.; Calder, J. Frequency and trends in foot and ankle injuries within an English Premier League Football Club using a new impact factor of injury to identify a focus for injury prevention. Foot Ankle Surg. 2014, 20, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Kilbreath, S.; Refshauge, K. Chronic Ankle Instability: Evolution of the Model. J. Athl. Train. 2011, 46, 133–141. [Google Scholar] [CrossRef] [Green Version]
- Hiller, C.E.; Nightingale, E.J.; Lin, C.-W.C.; Coughlan, G.F.; Caulfield, B.; Delahunt, E. Characteristics of people with recurrent ankle sprains: A systematic review with meta-analysis. Br. J. Sports Med. 2011, 45, 660–672. [Google Scholar] [CrossRef]
- Tanen, L.; Docherty, C.L.; Van Der Pol, B.; Simon, J.; Schrader, J. Prevalence of Chronic Ankle Instability in High School and Division I Athletes. Foot Ankle Spéc. 2013, 7, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.A. Instability of the foot after injuries to the lateral ligament of the ankle. J. Bone Jt. Surg. Br. 1965, 47, 669–677. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J. Athl. Train. 2002, 37, 364–375. [Google Scholar]
- McKeon, P.O.; Hertel, J. Systematic review of postural control and lateral ankle instability, part I: Can deficits be detected with instrumented testing. J Athl. Train. 2008, 43, 293–304. [Google Scholar] [CrossRef] [Green Version]
- Boyle, J.; Negus, V. Joint position sense in the recurrently sprained ankle. Aust. J. Physiother. 1998, 44, 159–163. [Google Scholar] [CrossRef] [Green Version]
- Hintermann, B.; Boss, A.; Schäfer, D. Arthroscopic findings in patients with chronic ankle instability. Am. J. Sports Med. 2002, 30, 402–409. [Google Scholar] [CrossRef]
- Khalaj, N.; Vicenzino, B.; Smith, M.D. Hip and knee muscle torque and its relationship with dynamic balance in chronic ankle instability, copers and controls. J. Sci. Med. Sport. 2021, 24, 647–652. [Google Scholar] [CrossRef]
- McCann, R.S.; Terada, M.; Kosik, K.B.; Gribble, P.A. Landing kinematics and isometric hip strength of individuals with chronic ankle instability. Foot Ankle Int. 2019, 40, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Freke, M.; Kemp, J.; Semciw, A.; Sims, K.; Russell, T.; Singh, P.; Crossley, K. Hip Strength and Range of Movement Are Associated with Dynamic Postural Control Performance in Individuals Scheduled for Arthroscopic Hip Surgery. J. Orthop. Sports Phys. Ther. 2018, 48, 280–288. [Google Scholar] [CrossRef]
- Robinson, R.; Gribble, P. Kinematic predictors of performance on the Star Excursion Balance Test. J. Sport Rehabil. 2008, 17, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Endo, Y.; Sakamoto, M. Relationship between Lower Extremity Tightness and Star Excursion Balance Test Performance in Junior High School Baseball Players. J. Phys. Ther. Sci. 2014, 26, 661–663. [Google Scholar] [CrossRef] [Green Version]
- Gribble, P.A.; Kelly, S.E.; Refshauge, K.; Hiller, C.E. Interrater Reliability of the Star Excursion Balance Test. J. Athl. Train. 2013, 48, 621–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinzey, S.J.; Armstrong, C.W. The Reliability of the Star-Excursion Test in Assessing Dynamic Balance. J. Orthop. Sports Phys. Ther. 1998, 27, 356–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland Ankle Instability Tool: A Report of Validity and Reliability Testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Kunugi, S.; Masunari, A.; Noh, B.; Mori, T.; Yoshida, N.; Miyakawa, S. Cross-cultural adaptation, reliability, and validity of the Japanese version of the Cumberland ankle instability tool. Disabil. Rehabil. 2016, 39, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Noronha, M.; Refshauge, K.M.; Crosbie, J.; Kilbreath, S.L. Relationship Between Functional Ankle Instability and Postural Control. J. Orthop. Sports Phys. Ther. 2008, 38, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Roach, S.; Juan, J.S.; Suprak, D.N.; Lyda, M. Concurrent Validity of Digital Inclinometer and Universal Goniometer in Assessing Passive Hip Mobility in Healthy Subjects. Int. J. Sports Phys. Ther. 2013, 8, 680–688. [Google Scholar]
- Nussbaumer, S.; Leunig, M.; Glatthorn, J.F.; Stauffacher, S.; Gerber, H.; Maffiuletti, N.A. Validity and test-retest reliability of manual goniometers for measuring passive hip range of motion in femoroacetabular impingement patients. BMC Musculoskelet. Disord. 2010, 11, 194. [Google Scholar] [CrossRef] [Green Version]
- Yonemoto, K.; Ishigami, S.; Kondo, T. The method guidelines for range of motion measurement. Jpn. J. Rehabil. Med. 1995, 32, 207–217. [Google Scholar]
- Han, H.; Kubo, A.; Kurosawa, K.; Maruichi, S.; Ishizaka, M.; Sadakiyo, K.; Nomura, T.; Honzawa, K. Ipsilateral patterns of the rotational range of motion of the hip in healthy Japanese adults. J. Phys. Ther. Sci. 2016, 28, 2550–2555. [Google Scholar] [CrossRef] [PubMed]
- van Lieshout, R.; Reijneveld, E.A.; van den Berg, S.M.; Haerkens, G.M.; Koenders, N.H.; de Leeuw, A.J.; van Oorsouw, R.G.; Paap, D.; Scheffer, E.; Weterings, S.; et al. Reproducibility of the modified star excursion balance test composite and specific reach direction scores. Int. J. Sports Phys. Ther. 2016, 11, 356–365. [Google Scholar]
- Denehey, T.; Marshall, T.; Spaccarotella, K.; Andzel, W. The Impact of an External Load of Football Equipment on Dynamic Balance as Assessed by the Modified Star Excursion Balance Test. Int. J. Exerc. Sci. 2018, 11, 797–805. [Google Scholar]
- Uebayashi, K.; Akasaka, K.; Tamura, A.; Otsudo, T.; Sawada, Y.; Okubo, Y.; Hall, T. Characteristics of trunk and lower limb alignment at maximum reach during the Star Excursion Balance Test in subjects with increased knee valgus during jump landing. PLoS ONE 2019, 14, e0211242. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Single-leg drop landing movement strategies in participants with chronic ankle instability compared with lateral ankle sprain ‘copers’. Knee Surg. Sports Traumatol. Arthrosc. 2015, 24, 1049–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshino, Y.; Yamanaka, M.; Ezawa, Y.; Ishida, T.; Kobayashi, T.; Samukawa, M.; Saito, H.; Takeda, N. Lower limb joint motion during a cross cutting movement differs in individuals with and without chronic ankle instability. Phys. Ther. Sport 2014, 15, 242–248. [Google Scholar] [CrossRef]
- Inoue, K.; Nunome, H.; Sterzing, T.; Shinkai, H.; Ikegami, Y. Dynamics of the support leg in soccer instep kicking. J. Sports Sci. 2014, 32, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- McCann, R.S.; Crossett, I.D.; Terada, M.; Kosik, K.B.; Bolding, B.A.; Gribble, P.A. Hip strength and star excursion balance test deficits of patients with chronic ankle instability. J. Sci. Med. Sport 2017, 20, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Jaber, H.; Lohman, E.; Daher, N.; Bains, G.; Nagaraj, A.; Mayekar, P.; Shanbhag, M.; Alameri, M. Neuromuscular control of ankle and hip during performance of the star excursion balance test in subjects with and without chronic ankle instability. PLoS ONE 2018, 13, e0201479. [Google Scholar] [CrossRef] [Green Version]
- Theisen, A.; Day, J. Chronic Ankle Instability Leads to Lower Extremity Kinematic Changes During Landing Tasks: A Systematic Review. Int. J. Exerc. Sci. 2019, 12, 24–33. [Google Scholar]
- Augustus, S.; Mundy, P.; Smith, N. Support leg action can contribute to maximal instep soccer kick performance: An intervention study. J. Sports Sci. 2016, 35, 89–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew-Bullock, T.S.-Y.; Anderson, D.I.; Hamel, K.A.; Gorelick, M.L.; Wallace, S.A.; Sidaway, B. Kicking performance in relation to balance ability over the support leg. Hum. Mov. Sci. 2012, 31, 1615–1623. [Google Scholar] [CrossRef]
- Tropp, H. Commentary: Functional Ankle Instability Revisited. J. Athl. Train. 2002, 37, 512–515. [Google Scholar] [PubMed]

{kind=link}
| Q. Please Tick the One Statement in Each Question that Best Describes Your Ankles. |
|---|
| 1. I have pain in my ankle Never (5), During sport (4), Running on uneven surfaces (3), Running on level surfaces (2), Walking on uneven surfaces (1), Walking on level surfaces (0) |
| 2. My ankle feels UNSTABLE Never (4), Sometimes during sport (not every time) (3), Frequently during sport (every time) (2), Sometimes during daily activity (1), Frequently during daily activity (0) |
| 3. When I make SHARP turns, my ankle feels UNSTABLE Never (3), Sometimes during running (2), Often when running (1), When walking (0) |
| 4. When going down the stairs, my ankle feels UNSTABLE Never (3), If I go fast (2), Occasionally (1), Always (0) |
| 5. My ankle feels UNSTABLE when standing on ONE leg Never (2), On the ball of my foot (1), With my foot fat (0) |
| 6. My ankle feels UNSTABLE when Never (3), I hop from side to side (2), I hop on the spot (1), When I jump (0) |
| 7. My ankle feels UNSTABLE when Never (4), I run on uneven surfaces (3), I jog on uneven surfaces (2), I walk on uneven surfaces (1), I walk on a fat surface (0) |
| 8. TYPICALLY, when I start to roll over (or “twist”) on my ankle, I can stop it Immediately (3), Often (2), Sometimes (1), Never (0), I have never rolled over on my ankle (3) |
| 9. After a TYPICAL incident of my ankle rolling over, my ankle returns to “normal” Almost immediately (3), Less than 1 day (2), 1–2 days (1), More than 2 days (0), I have never rolled over on my ankle (3) |
| Dominant Leg | Nondominant Leg | p-Value | Cohen’s d ES | |
|---|---|---|---|---|
| Mean (SD) 1 | Mean (SD) 1 | |||
| mSEBT (%LL) 2 | ||||
| Anterior | 75.6 (8.0) | 77.2 (7.9) | 0.46 | 0.20 |
| Posterolateral | 94.5 (11.7) | 98.0 (14.2) | 0.30 | 0.27 |
| Posteromedial | 104.4 (5.4) | 105.4 (7.5) | 0.72 | 0.15 |
| Composite | 91.5 (8.4) | 93.5 (9.9) | 0.49 | 0.22 |
| Range of Motion (deg) | ||||
| Hip Flexion | 123.6 (6.1) | 125.3 (5) | 0.25 | 0.30 |
| Hip Extension | 18.9 (2.9) | 18.1 (2.9) | 0.23 | 0.26 |
| Hip External Rotation | 41.6 (7.9) | 45.6 (6.9) | 0.12 | 0.54 |
| Hip Internal Rotation | 35.9 (9.4) | 36.7 (10.9) | 0.66 | 0.08 |
| Hip Abduction | 36.5 (4.5) | 36.9 (4.1) | 0.67 | 0.08 |
| Hip Adduction | 17.1 (12.7) | 18.5 (13.1) | 0.00 * | 0.11 |
| Trunk Flexion | 39.2 (4.8) | - | - | |
| Trunk Lt Rotation | 46.4 (5.1) | - | - | |
| Trunk Rt Rotation | 42.2 (4.8) | - | - | |
| Dominant Leg 1 | p-Value | Cohen’s d ES | Nondominant Leg 1 | p-Value | Cohen’s d ES | |||
|---|---|---|---|---|---|---|---|---|
| CAI (n = 7) | Non-CAI (n = 10) | CAI (n = 9) | Non-CAI (n = 8) | |||||
| Anterior (%LL) | 75.6 (8) | 77.2 (7.9) | 0.46 | 0.20 | 77.9 (7.6) | 76.5 (8.8) | 0.74 | 0.17 |
| Posterolateral (%LL) | 94.5 (11.7) | 98.0 (14.2) | 0.30 | 0.27 | 91.7 (13.7) | 105.1 (11.7) | 0.046 * | 1.05 |
| Posteromedial (%LL) | 104.4 (5.4) | 105.4 (7.5) | 0.72 | 0.15 | 105.9 (6) | 104.9 (9.3) | 0.80 | 0.12 |
| Composite Score (%) | 91.5 (8.4) | 93.5 (9.9) | 0.49 | 0.22 | 91.8 (9.1) | 95.5 (9.9) | 0.53 | 0.10 |
| Dominant Leg 1 | p-Value | Cohen’s d ES | Nondominant Leg 1 | p-Value | Cohen’s d ES | |||
|---|---|---|---|---|---|---|---|---|
| CAI (n = 7) | Non-CAI (n = 10) | CAI (n = 9) | Non-CAI (n = 8) | |||||
| Hip Flexion | 122.6 (8.2) | 123.6 (4.4) | 0.56 | 0.16 | 123.8 (5.9) | 127.0 (3.2) | 0.19 | 0.68 |
| Hip Extension | 17.7 (1.7) | 19.5 (3.4) | 0.17 | 0.69 | 19.4 (3.0) | 16.6 (2.0) | 0.04 * | 1.11 |
| Hip External Rotation | 42.1 (6.0) | 41.7 (9.3) | 0.84 | 0.05 | 45.8 (4.5) | 45.5 (9.2) | 0.94 | 0.04 |
| Hip Internal Rotation | 34.1 (10.1) | 37.1 (9.2) | 0.54 | 0.31 | 41.6 (6.4) | 31.3 (12.6) | 0.047 * | 1.03 |
| Hip Abduction | 35.3 (4.3) | 37.4 (4.6) | 0.35 | 0.47 | 35.6 (4.1) | 38.4 (3.7) | 0.16 | 0.72 |
| Hip Adduction | 17.4 (16.6) | 16.5 (10.1) | 0.92 | 0.06 | 14.4 (1.1) | 23.1 (18.6) | 0.18 | 0.66 |
| Trunk Flexion | 38.4 (2.6) | 39.5 (5.9) | 0.58 | 0.24 | 39.6 (4.3) | 38.9 (5.5) | 0.78 | 0.14 |
| Trunk Lt Rotation | 48.6 (3.6) | 44.5 (5.5) | 0.14 | 0.88 | 47.3 (4.0) | 45.3 (6.2) | 0.42 | 0.40 |
| Trunk Rt Rotation | 42.3 (3.7) | 42.0 (5.6) | 0.97 | 0.06 | 42.4 (3.2) | 42.0 (6.3) | 0.85 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamura, A.; Shimura, K.; Inoue, Y. Hip Flexibility and Dynamic Balance Ability in Soccer Players with Functional Ankle Instability. Trauma Care 2021, 1, 206-214. https://doi.org/10.3390/traumacare1030018
Tamura A, Shimura K, Inoue Y. Hip Flexibility and Dynamic Balance Ability in Soccer Players with Functional Ankle Instability. Trauma Care. 2021; 1(3):206-214. https://doi.org/10.3390/traumacare1030018
Chicago/Turabian StyleTamura, Akihiro, Keita Shimura, and Yuri Inoue. 2021. "Hip Flexibility and Dynamic Balance Ability in Soccer Players with Functional Ankle Instability" Trauma Care 1, no. 3: 206-214. https://doi.org/10.3390/traumacare1030018
APA StyleTamura, A., Shimura, K., & Inoue, Y. (2021). Hip Flexibility and Dynamic Balance Ability in Soccer Players with Functional Ankle Instability. Trauma Care, 1(3), 206-214. https://doi.org/10.3390/traumacare1030018