1. Introduction
Domestic, family, or intimate partner violence, referred to as
relational violence in this paper, varies in its definition. The widely accepted definition describes the violence between romantic partners and family members [
1]. However, more clinical definitions are becoming increasingly accepted. Finkelhor et al. (2007) [
2] describes domestic violence as “a pattern of assaultive and coercive behaviors, including physical, sexual, and psychological attacks, as well as economic coercion that adults or adolescents use against their intimate partners”. This definition is considered more accurate as it explains the pattern of control and coercion that often accompanies these relationships.
Despite social response systems focusing on the physical aspects of relational violence, it manifests in several forms, including “emotional, physical, sexual and economic abuse,” among others. Research shows that victims often experience multiple types of abuse, known as poly-victimization, in violent relationships. When this occurs, victims are more likely to have significant adverse mental health outcomes [
3]. Further, the concept of
coercive control, while not classified as an act of violence itself, has been shown to lie at the core of violent relationships and can actively predict violent relational events [
4]. Coercive control can be defined as the use of threats, humiliation, and/or intimidation to frighten or pressure a romantic partner or family member into a state of constant behavioral compliance with their abuser [
4]. It is a psychological assault on the autonomy of the abused partner and can manifest in a variety of manipulative contexts. Hester et al. (2011) [
5] identifies relationship violence as a “three-pronged attack,” which includes the use of control, threats, and violence. Scholars have established the connections between coercive control and traditional conceptualizations of domestic or interpersonal violence with this theoretical inclusion. This complex and multifaceted phenomenon involves people in every community around the world. A deeper investigation into relational violence is the key to developing a better understanding of the issue and advancing more successful interventions to increase safety, liberty, and autonomy for families and communities.
2. Scope of the Problem
Relational violence affects women, men, children, individuals, families, and communities and is present among all types and classifications of individuals. It is epidemic and affects countless families around the globe, reaching people of all cultures and socioeconomic statuses. There appears to be a link between those who experience greater structural inequality and intimate partner violence [
3]. However, women whose family annual income is less than USD 10,000 are more likely to experience intimate partner violence [
6]. Women of all races are equally likely to become victims of relational violence [
7]. However, multiracial women experience relational violence more often throughout their lifetimes compared to other ethnic groups [
8].
According to Black et al. [
9], a woman is assaulted or beaten every nine seconds in the United States. As reported by the U.S. Justice Department’s Bureau of Justice statistics, 21 percent (or about 1/5th) of all violence from 2003 to 2012 was in the form of relational violence [
1]. In the US, this adds up to more than 10 million victims of relational violence each year [
1]. A significant amount of relational violence is committed by a former intimate partner, and over 75% of reoccurring violence happens within the victim’s home. Only about half of relational violence reported on the National Crime Victimization Survey was reported to the police [
1]. The prevalence of relational violence shown through these statistics is staggering.
In addition to violence against women, which is at the center of this conversation, almost a quarter of men in the United States have reported experiencing relational violence, and for 1 out of every ten of those men, first-time victimization occurred before the age of 25. Many male victims first experience relational violence before the age of 18, and 97% of men who experienced rape, physical violence, or stalking by an intimate partner had only female perpetrators. Still, there is very little research on this matter [
10]. This is mainly because men fear they will not be believed if they report the abuse. A study of male victims of relational violence was conducted in the Netherlands in 2013, and it was shown that abuse is perpetrated by both men and women. The study found that male victims are abused by their partners both mentally and physically, with 54% of survivors in these cases having been physically abused. In the study, children were often used as weapons during psychological abuse, along with threats of blackmail and financial harm. The study found that men were more likely to report to police if they were physically attacked and less likely to report other types of abuse [
11].
In 2015, the US National Coalition of Anti-Violence Programs (NCAVP) published a report related to LGBTQ and HIV-affected intimate partner violence. They reported 13 homicides due to intimate partner violence; of the total 13 homicides, six were transgender women, four were cisgender men, and three were cisgender women. All six transgender women were transgender women of color, including four who were black and two who were Latinx. In total, they reported 1976 survivors of relational violence, with the majority identifying as gay or lesbian. Survivors who were transgender were two times more likely to report that they had experienced violence by a former or ex-partner than survivors who were cisgender [
12].
A survey conducted in the United States revealed that over 1.3 million women in the country had reported being physically assaulted by a romantic partner in the previous twelve months. Survivors in this study reported an average of 3.5 assaults per year. A total of 25.5% of respondents reported being victimized in at least one relational violence incident in their lifetime, which included an estimated 25 million women [
13]. Due to the often-complicated nature of relational violence, many professionals struggle with the non-physical aspects of the phenomenon. Specialists in a variety of intersectional professions such as social work, law enforcement, and the courts are working to address this, but much more is needed. Criminal justice systems are frequently tasked with addressing this social problem, but the limitations of these systems have been revealed due to their focus on acts of physical violence and their lack of ability to intervene in psychological and emotionally abusive situations [
5]. Other forms of coercion and control, such as emotional, financial, and psychological methods can be just as debilitating to survivors but are not typically the criminal justice system’s focus.
3. Impact on Survivors
3.1. Mental Health Impacts
Survivors of relational violence have higher rates of post-traumatic stress disorder (PTSD) and depression than those who have not experienced relational violence, and those who experience poly-victimization also experience higher rates of PTSD and depression than those who have not experienced poly-victimization (Black, et al., 2011; Fedovskiy et al., 2008) [
9,
14]. Research consistently demonstrates pervasive mental health diagnoses in victims of relational violence. Women who have experienced relational violence are more likely to have suicidal ideations and to attempt suicide compared to women who have not [
8,
15,
16,
17]. Men who are experiencing relational violence, both physical and non-physical, are most likely to present with PTSD and depression, while additional mental health concerns for this population include anxiety, insomnia, and social dysfunction [
18].
3.2. Physical Health Impacts
Research reliably illustrates the lifelong physical health effects of relational violence. A 2006 study found that relational violence took a significant physical toll on survivors. The women studied had an increased risk of stroke, heart disease, and asthma [
15]. Additional health consequences of relational violence for victims include chronic pain, gastrointestinal disorders, and chronic disease [
8]. Gynecological issues, including sexually transmitted infections, chronic pelvic pain, and urinary tract infections, are also common among survivors of relational violence [
18]. A 2009 study revealed a significant association between HIV infection and experiences or histories of relational violence in women [
19].
The various physical health consequences are present at the time of the assault but can continue far beyond the period of abuse. Relational violence survivors experience an increased prevalence of co-occurring conditions. Female victims of relational violence are 70% more likely to abuse alcohol than women who are not survivors of relational violence [
15]. It is not uncommon for survivors to struggle with mental health issues and physical and substance abuse issues.
3.3. Impact on Children and Families
Children living in homes where relational violence is prevalent experience many negative outcomes from witnessing the abuse. One study found that about 26% of children in the United States were exposed to family violence in their lifetime, which is equal to about 18 million children [
20]. Children exposed to family violence are more likely to be the victims of child abuse [
3]. The above-cited research suggests that children who experience multiple types of violence in the home tend to demonstrate lower levels of resilience and have a higher level of vulnerability towards negative behavioral, social, and health outcomes later in life.
Studies have also found that children who experienced poly-victimization were at a greater risk of being victimized in adolescence and adulthood. They were also more likely to experience a substance abuse disorder in adolescence [
3,
21]. Finkelhor, Ormrod, and Turner [
2] describe this type of victimization in children as a “condition” rather than an event. This condition of victimization often includes intrafamily violence. The authors found poly-victimization to strongly correlate with psychological symptoms such as anxiety and depression. Children who witness domestic violence are more likely to have behavioral and cognitive challenges and long-term health issues. They are more likely to have anxiety, depression, problems with peers and anger/aggression, and low self-esteem. They are also more likely to be delayed in physical and cognitive skills and have trouble concentrating. The effects are not limited to behavioral and cognitive challenges; children who experience poly-victimization have a 3.7 times higher likelihood of suffering from chronic pain and developing gastrointestinal diseases, respiratory diseases and metabolic diseases, or musculoskeletal disorders [
22]. Furthermore, exposure to domestic violence is a risk factor on the adverse childhood experiences questionnaire for early death [
20].
Relational violence has a negative outcome on the entire family unit. A study in the United States has shown that witnessing relational violence as a child can cause negative health effects in future generations [
23]. Over the course of one year in the Unites States, approximately 20,000 children received residential domestic violence services, and an additional 23,000 adults received advocacy and support [
20]. Children are removed from their homes at alarming rates due to exposure to domestic violence. The risk of having children removed is an often-cited reason that survivors of relational violence are hesitant to seek help.
3.4. Impact on Communities
The effects of relational violence last for years, and the cost for children who witness it once they become adults is estimated to be around USD 50,000 per person [
24]. The damage of relational violence does not exist in a vacuum. Instead, the family, community, and even broader society suffer the impact. A 1995 study in the United States estimated the cost of medical, mental health services, and productivity loss due to relational violence to be about USD 5.8 billion each year. Relational violence is estimated to cost USD 4.1 billion in medical and mental health services alone. Private or group insurance and out-of-pocket costs make up most payments for relational violence victims [
13]. Compared to others, women experiencing relational violence are nine times more likely to receive health care services [
18]. Furthermore, survivors are more likely to require high-cost specialty care, such as an orthopedic surgeon [
8].
4. Current Models
There are currently two predominant models used to explain relational violence. Both models have been applied to studies of relational violence for over thirty years. They have experienced scrutiny over their ability to describe the complex nature of intimate partner violence realistically.
4.1. Cycle Theory of Domestic Violence
Lenore Walker developed the Cycle Theory of Violence in 1978 after interviewing 400 battered women. The study used forced-choice and open-ended questions and relied on remembered incidents of relational violence [
25,
26]. The Cycle Theory of Violence proposes that relational violence occurs predictably through three stages. These include tension-building, acute-battering incidents, and loving contrition [
25]. The tension-building stage begins the cycle with increasing interpersonal stress and tension about domestic issues. This tension continues to grow despite the survivors’ attempts to appease the batterer. Non-physical forms of abuse may occur during this phase [
25]. Physical violence occurs during the acute-battering incident phase. This cycle is short but poses the most significant risk to the survivor. Physical and sexual abuse, as well as physical injuries, are likely during this phase. The ending of this stage in the cycle marks a significant release of interpersonal tension [
25,
27]. Walker suggests that the final phase, loving contrition, consists of a “honeymoon” between the batterer and survivor. During this phase, the batterer apologizes, and there is a decrease in the abuse. Walker (1979) describes this last phase as a “respite” from the suffering. This stage, along with Walker’s theory of learned helplessness, is often used to explain why survivors remain in violent relationships [
21,
27].
4.2. Critique of Cycle Theory of Violence
The Cycle Theory of Violence is one of the most widely used models when training professionals in other disciplines to respond to families with violence in the home. This theory is viewed as problematic for many reasons. One study found that women were just as likely to resort to violence during conflict with intimate partners as men [
28]. Michael Johnson (2009) [
28] described three types of relational violence to standardize domestic violence statistics. Two of those types have the overarching theme of power and control, which the Cycle Theory of Violence explains. The third type, which Johnson calls situational couple violence, occurs when a particular situation provokes violence between a couple when neither person is otherwise trying to exert power or control in the relationship [
28]. Situational couple violence is believed to be the most common type of relational violence and cannot be described using the Cycle Theory of Violence [
28].
The Cycle Theory of Violence attempts to simplify a complex issue. The theory is used by child welfare professionals, the judicial system, law enforcement officials, domestic violence shelters, and others educating the public about domestic violence. The Cycle model is problematic because it does not depict the reality of relational violence for many batterers and survivors. Many survivors never describe a “honeymoon” phase. Instead, they feel the near-constant presence of power and control in the relationship [
29]. The cycle also describes a relatively stable pattern where actions are repeated over and over again. Many survivors describe an escalating series of incidents in which the violence becomes more and more life-threatening. Professionals and others who may contact families impacted by relational violence must recognize the secretive nature and the impact of power and control on a survivor. Additionally, the Cycle Theory of Violence does not account for the “ongoing nature” of relational violence and the many non-physical forms of abuse present in controlling relationships [
30].
The Cycle Theory of Violence and Walker’s Battered Women’s Syndrome have received criticism from many social scientists, but they are especially controversial in the judicial system. As ordered in the Violence Against Women’s Act of 1994, Walker’s theory was studied in its effectiveness in defense trials for women who killed their abusers. This study found that many survivors’ stories did not align with the theory. The idea of a passive or helpless victim at times did more harm; professionals began to distance themselves from the theory [
29]. The Cycle Theory of Violence has made contributions to the field; however, there has been a need to develop a model that more closely resembles the experiences of those involved in relational violence. Assuming that there is a “honeymoon” among the violence infers that there is an opportunity for the victim to leave their abuser, when in fact, research consistently points to the continuation of control that leaves a victim trapped. The learned helplessness that Lenore Walker (1978) [
25] describes as the force that keeps women in violent relationships has been criticized and refuted in numerous studies [
31,
32,
33,
34].
4.3. The Duluth Power and Control Wheel
Another widely used model for explaining relational violence is the power and control wheel [
35]. The power and control wheel is used as part of the Duluth Method to describe the pervasive and coercive nature of control in relational violence. The wheel was developed in 1981 by the founders of the DAIP in Duluth, Minnesota. The project is a collaborative of community agencies aiming to address the problem of domestic violence. It is also the creator of some of the most widely used portions of batterers’ intervention programs in the United States [
36].
4.4. Critique of the Power and Control Wheel
Although it continues to experience popularity in batterers’ intervention programs across the country, advocates and social scientists have criticized the Power and Control Wheel. One of the major criticisms is the assumption made in the model of a male perpetrator and a female victim. New research highlights the neutrality of gender in relational violence. Both males and females are capable of perpetuating relational violence against their partner in heterosexual couples as well as same-sex couples [
36]. Similar to the criticism of the Cycle of Violence model, opposition to the Power and Control Wheel is typically related to the one size fits all approach of the model. Although power and control are prevalent in relational violence scenarios, there are varying degrees of enforcement. This picture further stereotypes the batterer as powerful and forceful and the survivor as passive and helpless. Advocates against the use of the Power and Control Wheel also condemn the model for listing all of the modes of power and control under the “violence” heading. Opponents say that misrepresents the subtle effect coercive control has in a relationship [
36]. Currently, the Duluth model is utilized in most batterers’ intervention programs across the United States [
37]. In 2003, a report released by the National Institute of Justice revealed two studies that did not support the utilization of the Duluth model in offender treatment [
37].
4.5. Reasoning for a New Model
A new model is necessary to educate the public and service delivery professionals about the complicated nature of violent intimate relationships. This new model needs to represent all possible batterers and survivors and needs to highlight coercive power and control. It also needs to display the continuous and escalating tendencies of control and violence. Most importantly, the new model needs to assist those who contact batterers or survivors plagued by relational violence to recognize patterns in families in crisis and have a practical application for survivors to identify and process their own experiences.
5. Materials and Methods
Two primary conceptual mechanisms were used in the development and refinement of the Model of Systemic Relational Violence. Original ideas for the model resulted from quantitative data analysis and a literature review investigating the coercive control perspective of domestic violence. From this paradigm, particular attention was paid to the presence of emotional, psychological, and expressed coercion and control, which manifests as threats and demands from an abusive partner. These threats and demands are placed on the marginalized partner in a relationship for the express purpose of reducing their autonomy and controlling their behavior across multiple domains of their day-to-day lives. Recent research has suggested that even when these controlling behaviors may not fit the criteria for traditional conceptualizations of relational violence, they are connected to traditionally recognized abusive behavior patterns. This is expressed when one romantic partner diminishes the autonomy of the other and enforces their control through enacted physical and sexual violence in the relationship. As was seen in the data and is theoretically postulated in Stark’s theory of coercive control, from this perspective, the traditional conceptualizations of a honeymoon phase do not exist. Instead, what may have been previously identified as a honeymoon phase in the cycle of violence may be more accurately represented as a period of manipulation or a lack of overt aggression. Preceding the period of manipulation and lack of overt aggression, the abusive partner enforces their control over their partner by expressing physical, sexual, or other types of violence. As a result, additional enforcement behaviors to maintain control of the abused partner are unnecessary. During this time, the abused partner and/or other external observers have the highest potential for failing to recognize the presence of the abusive partner’s continued domination in the relationship
To further develop this portrayal of intimate partner violence and to develop a visual, conceptual model, collaborative focus groups were conducted in cooperation with the state-level domestic and sexual violence task force (n = 17) in the central United States. The task force, and subsequent focus group participants, consisted of experienced agency leadership from an array of domestic violence service delivery programs in rural and urban areas across the state. Participants were among the most knowledgeable and accomplished domestic violence service providers in the state. Before the focus groups, a base-level version of the Model of Systemic Relational Violence was developed based on the aforementioned data. In addition, the model was built upon the state of the literature, which expanded traditional conceptualizations focused on physical markers of domestic violence to include manipulation, threats, demands, and emotional and psychological abuse. This version of the model was given to all participants who were asked to heavily critique it and provide suggestions on how it could better describe their experiences with the client populations they serve. In addition to this, participants were given four specific questions to consider on their own. These questions focused on the experiences these leaders in domestic violence service provision had observed in their agency settings and assessed to what degree the visual representation of the model aligned with these experiences. Specific attention was paid to what factors or components may be missing from the model and how to adapt included concepts.
Participants were asked to work independently, examine the preliminary model they were provided with, and work through their critique of the model on their own. Each participant provided written feedback on this work to be analyzed. After the independent work, a focus group was conducted. The participants explored their answers to the provided questions and expanded on general perspectives on improving the visual model and developing its components. The group engaged in a collaborative process as the model was amended and provided feedback to ensure consensus and clarity in interpreting their feedback. This process was conducted regarding both the visual model development and the assessment and interpretation of their verbal feedback. Copious notes were taken by the facilitator detailing the process. Later, the facilitator and two additional university researchers independently assessed all the written feedback, critiques, and constructions provided by the focus group participants. Qualitative content analysis was performed using open coding to identify themes, a methodology validated by Esterberg (2002) [
38]. After each of the three researchers independently performed the initial coding process, a
consensus procedure was used to debate and clarify the codes and collectively agree on how they should be interpreted and utilized in the model refinement process [
39]. Facilitator notes from the focus group were also used during the consensus procedure process to help establish participant context and align the interpretation of the codes. Preliminary findings and code interpretations were then shared with agency and field leaders in domestic violence work and verified as accurate expressions of the phenomenon described and as helpful tools to better explain the phenomenon they experienced in practice [
40]. These methods of utilizing multiple independent analysts and points of checks and balances in a collaborative process contributed to a triangulation process which is considered to enhance the confirmability of the findings and the trustworthiness of the process [
41].
6. Results
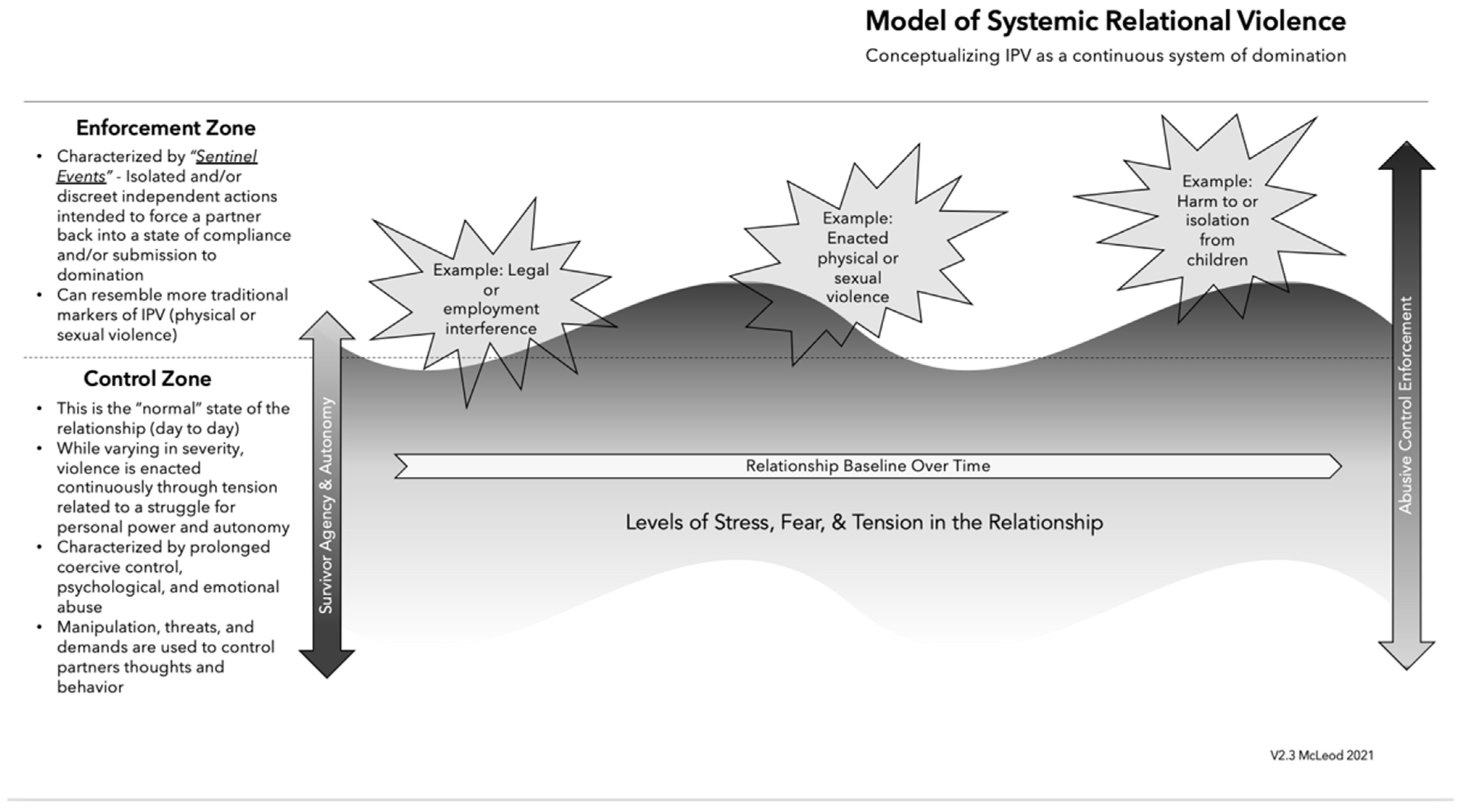
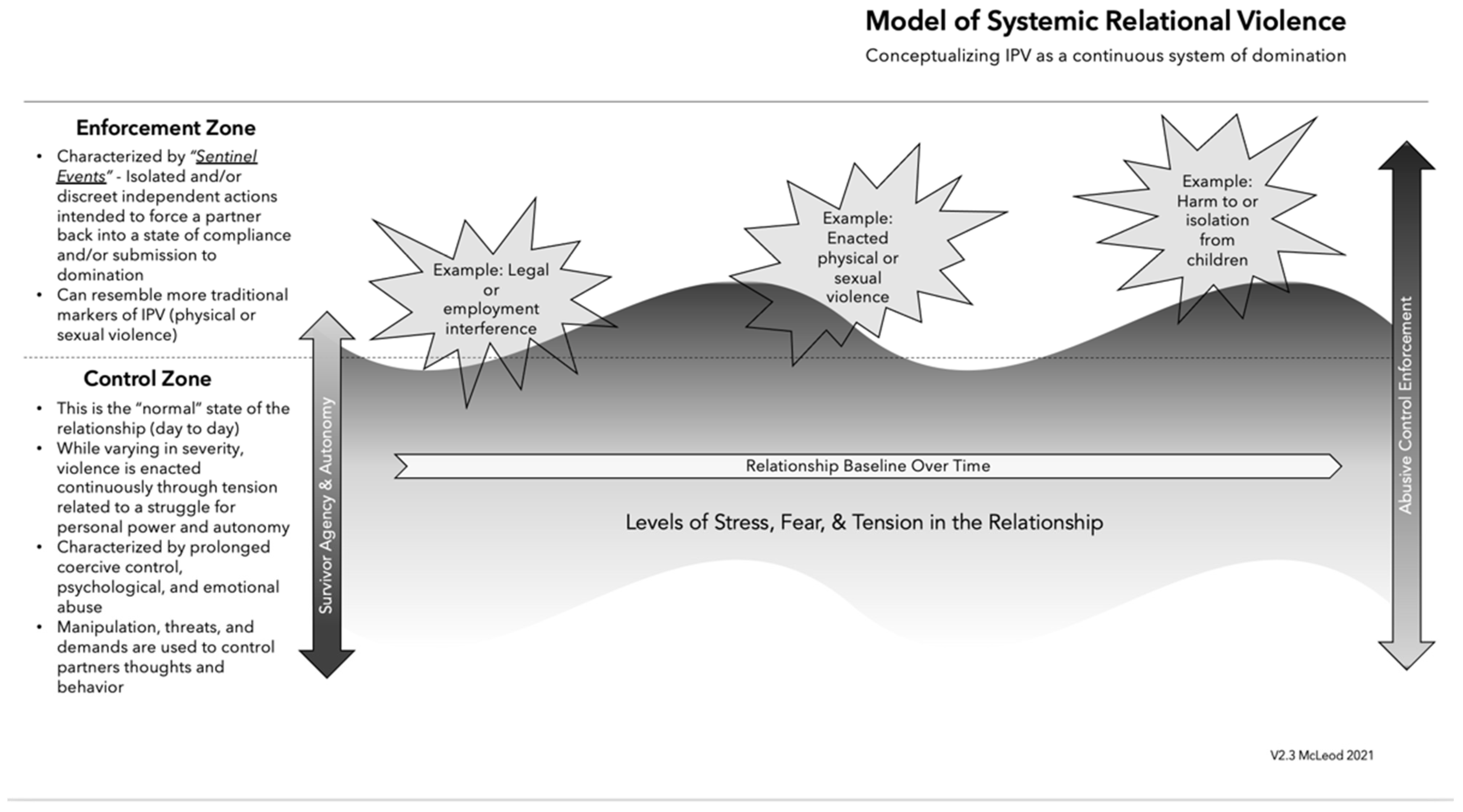
When the focus groups’ notes were analyzed and coded, multiple themes emerged from the data: (1) The focus group participants predominantly found the model accurate and applicable to their practice experiences. (2) There was a strong consensus that the honeymoon phase is an outsider’s perspective and is not relevant to the lived experience of survivors. Instead, survivors experience a continuous threat of violence (coercive control), and the momentary absence of violent acts does not represent a healthy period in the relationship. (3) Constant behavioral control is enforced through discreet sentinel events, such as acts of physical violence or threats of harm to children, and (4) every relationship may have a different baseline regarding tension, autonomy, and control. It is essential to note that across all the themes was the feedback that social responses to relational violence tend to work from the outside in, meaning that the focus is traditionally on responding to the correction of abusive enforcement strategies (such as hitting) rather than the presence of constant behavioral domination and coercive control.
7. Description of the Model of Systemic Relational Violence
The Model of Systemic Relational Violence, with visual depiction in
Figure 1, highlights the non-physical elements of control which exist within intimate partner abuse. The model was developed in response to an abundance of field data and qualitative responses, which described a continual state of control. Those experiencing relational violence describe a constant state of control that is not depicted in the current models of domestic violence—survivors and helping professionals describe these relationships as a
perpetual system of domination. The Model of Systemic Relational Violence illustrates the constant expression of behavioral control that may fluctuate and then later be enforced through physical and non-physical sentinel acts. The model demonstrates how the abuser constantly maintains dominance and behavioral control and acts in unique and/or discreet ways to enforce their dominance and maintain that control. For example, hitting a partner is not the focus of domestic violence, it is merely a symptom of a more extensive disease of systematic daily interpersonal control and domination.
The concept we are proposing contrasts with other models, which reflect a period of relational happiness or tranquility in the absence of abuse. Previous models have characterized periods of reduced physical violence as a “honeymoon phase” for survivors. From the perspective of the model of relational violence, the honeymoon phase is a phenomenon viewed from an outsider’s perspective, and the presence of control and the threat of violence constantly occurs for the abused partner. Statistically, research has shown that the threat of violence will nearly always result in enacted violence at some point in the relationship [
42]. While enforcement techniques may be minimized at certain times within the relationship, the control and threat of enforcement are ever-present. There may be periods in which the victim is compliant and, thus, will experience more control tactics rather than enforcement techniques. The Model of Systemic Relational Violence reflects two separate zones that the victim continuously fluctuates between at any point in the abusive relationship. The enforcement zone and the control zone are characterized by violence and threat of violence.
The enforcement zone represents an interactive space where the abusive partner attempts to force the abused partner back into compliance. This typically happens when the power dynamic shifts to a point where the abuser fears higher levels of autonomy are presenting on the part of the abused partner. It is characterized by the abusive partner incorporating and using
sentinel events as a tool to gain behavioral control of the abused. The Joint Commission (2013) [
43] defines a sentinel event as “an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof”. In this model,
sentinel events could include a wide range of behaviors on the part of the abusive partner, which can persuade, manipulate, or force the abused partner to alter their behavior to comply with what they believe to be the behavioral expectations of the abuser. This is an integral part of the system function. The victim believes that their submission to their abusers’ behavioral expectations may reduce the risk of physical violence, or other collateral damage, as the relationship status re-enters the control zone. Sentinel events can include traditional markers of domestic violence, such as physical or sexual assaults but are also much broader in context. Other examples of sentinel events could include but are most certainly not limited to threats toward the safety of children or pets, actions that cause problems with employment, or a wide range of psychological and emotional abuses. Sentinel events are inclusive of traditional conceptualizations of abusive acts, such as acts of physical violence, but are certainly not limited to those.
The control zone is characterized by prolonged coercive control and psychological and emotional abuse. Regularly, the perpetrator controls the victim through threats of physical violence to maintain conformity. Additionally, manipulation tactics involving finances, children, or other family members are used regularly to ensure the obedience of the victim. The victim is kept in compliance with the perpetrator’s needs and demands through emotional and psychological abuse. The instances of relational violence within the control zone are primarily characterized by events beyond the traditional view of relational violence. Understanding the victim’s day-to-day experience may facilitate the development of comprehensive interventions.
Note: Perpetrator behavior fluctuates between enacted violence and other non-physical forms of abuse. Rather than a cycle, relational violence is a system, which ebbs and flows over time.
8. Discussion and Conclusions
The Systemic Relational Violence presentation model provides a potential extension for the two existing theoretical models, the Cycle of Violence and the Duluth Power and Control Wheel. Critics of the existing models of relational violence have insisted that there is more to this phenomenon than what meets the eye. The Model of Systemic Relational Violence draws from these current models while offering a better understanding of the whole picture. The findings presented in the Model of Systemic Relational Violence suggest that distinct conceptual events occur in abusive or violent relationships that have been absent in prior models and may provide a better tool for training and professional development, and guide future research studies.
First, the Model of Systemic Relational Violence addresses what the two models above lack: the interconnectedness of coercive control and physical and sexual violence. The model presented is inclusive and recognizes that batterers can be both men and women and that survivors can be both men and women. The model also acknowledges the experiences of same-sex couples.
The Model of Systemic Relational Violence examines the relationship between the batterer and the survivor for both physical and non-physical forms of control that may be exhibited and enforced. Prior models lack the representation of daily enforcers of control, physical and non-physical, which cultivate an almost constant state of agony and fear within the victim. The Model of Systemic Relational Violence reinforces Finkelhor, Ormrod, and Turner’s [
2] more clinical definition, which explains domestic violence as “a pattern of assaultive and coercive behavior, including physical, sexual, and psychological attacks and economic coercion that adults or adolescents use against their intimate partner”. The mental and physical health impacts on survivors of relational violence are vast. Additionally, this model resolves the concerns of a “honeymoon” stage and better aligns with the experiences of survivors. Unlike the Cycle of Violence and its honeymoon phase, the Model of Systemic Relational Violence describes a constant system of domination where the abuser is viewed as always working to retain dominance and control. Professionals working within and around the criminal justice system benefit from knowing that what may appear as a honeymoon phase may not be one.
Finally, the model depicts a more accurate relationship between power and control by utilizing the concepts of an enforcement zone and a control zone. The enforcement zone represents the episodes where more physical violence occurs in sentinel events. The control zone depicts the time where non-physical violence is enacted in day-to-day events. The Model of Systemic Relational Violence reveals that while there may be an ebb and flow between physical and non-physical acts, control or violence is a constant factor in these relationships.
Implications for the adoption of this model could be far-reaching. The Model of Systemic Relational Violence could be used to add to existing training on the phenomenon and could prove especially useful in interprofessional contexts to explain how the presence of coercion and control play such an integral role in domestic and interpersonal violence. This could assist criminal justice system partners and policymakers in further understanding the nuances of relational violence beyond the discreet incidents of a physical altercation. The model can also be applied in clinical contexts to assist survivors in identifying their routines of behavior in relationships. In doing so, survivors could be empowered to make decisions about their own lives and relationships and further explore how to manage and change patterns of behavior that leave them vulnerable to all types of abuse. Further research is needed to empirically examine the applicability of the model across a variety of contexts, different varieties of partnerships, and relationships. Additional research is also needed to investigate the application of the model across interprofessional training and clinical contexts.
As noted in the literature, and by any name, violence against women at the hands of their romantic partners is an epidemic public health issue. This model can provide an additional tool to help existing service providers explore the topic further in treatment and advocacy. However, even with the origins of its data and development in spaces more connected with traditional cisgender, heterosexual, romantic relationships, the Model of Systemic Relational Violence facilitates the understanding that anyone may be experiencing relational violence. This is regardless of intimacy levels in the relationship, age, sex, gender expression, sexual orientation, ability, or the presence of physical injuries. Rather than focusing on discreet acts or incidents as the primary function of the abuse, the model allows for the interactions in the relationship to be explored from a context that originates with the unhealthiness of behavioral coercion and control and details how discreet events are used to enforce that control. This provides a model that more accurately reflects the experiences of survivors across a broad spectrum and creates opportunities to improve the delivery of services to victims of relational violence. Moreover, an important contribution of this model lies in its survivor-centered perspective. Concepts such as the “honeymoon phase” are identified as outsider observations that do not fully capture the nuance of the relationship system and its fluctuation over time. This more accurate depiction of a system of domination and control can be used for policy development to support survivors and help resolve the long-lasting and costly negative impacts of relational violence on individuals, communities, and systems to create better prevention and intervention systems. The model provides a potential tool that may be utilized in training to expand how interprofessional systems understand relationship violence and support people to live healthier, happier lives.
9. Patents
The Model of Systemic Relational Violence is not yet patented, but copyrighted training materials exist, and the model should not be used without the expressed consent of David McLeod. Go to www.damcleod.com for more information.


{kind=link}