
Protocol of the Long-COVID Patients Causal Diagnosis and Rehabilitation Randomized Feasibility Controlled Trial in Patients with Dysautonomia: The LoCoDiRe-Dys Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
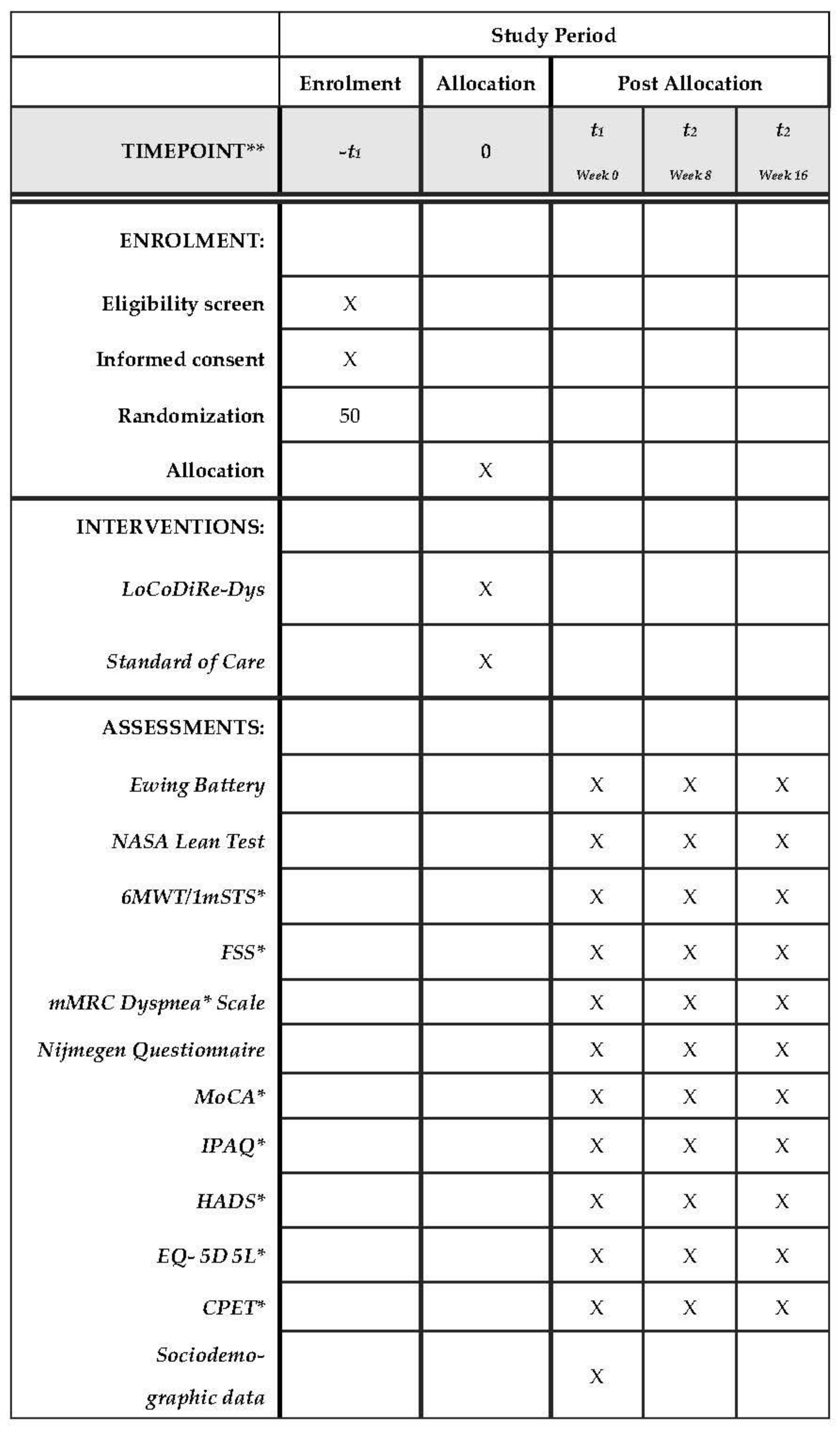
2.1. Study Design
2.2. Eligibility Criteria
2.3. Ethics
2.4. Study Population
2.5. Study Procedures
2.5.1. Clinical Assessment
- (i)
- The Valsalva maneuver, where the patient blows in a mouthpiece at a pressure of 40 mmHg for 15 s and an ECG measurement takes places of the ratio of the longest R-R interval after the maneuver with the shortest during the maneuver (“Valsalva ratio” being the mean of 3 subsequent maneuvers).
- (ii)
- The heart rate response to standing up, where the patient lies and then stands up without help and a ratio of the R-R interval is measured (30th beat to 15th beat after standing up).
- (iii)
- The heart rate response to deep breathing, where the patients slows his breathing rate to 6 breaths/min and the maximum and minimum heart rates during each breath are measured (mean difference of three successive attempts is used).
- (iv)
- * The blood pressure response to standing up, with measures taken between lying and standing position (difference of systolic blood pressure is measured).
- (v)
- * The blood pressure response to handgrip, with the patient maintain 30% of the maximum voluntary contraction with a handgrip at max 5 min (difference of diastolic pressure close to releasing and before the beginning of the test).
2.5.2. Functional Assessment
2.5.3. Outcome Measures
- (i)
- (ii)
- (iii)
- (iv)
- (v)
- (vi)
2.5.4. Cardiopulmonary Exercise Test
2.5.5. Primary and Secondary Outcomes
2.5.6. Sample Size Calculation
2.5.7. Randomization and Design
2.5.8. Study Intervention
2.5.9. Adverse Events and Drop-Out Monitoring
2.5.10. Patient Organization Feedback
2.5.11. Data Collection and Analysis
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 15 April 2023).
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Long-Term Consequences of COVID-19 at 6 Months and Above: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6865. [Google Scholar] [CrossRef] [PubMed]
- O’Mahoney, L.L.; Routen, A.; Gillies, C.; Ekezie, W.; Welford, A.; Zhang, A.; Karamchandani, U.; Simms-Williams, N.; Cassambai, S.; Ardavani, A.; et al. The Prevalence and Long-Term Health Effects of Long Covid among Hospitalised and Non-Hospitalised Populations: A Systematic Review and Meta-Analysis. eClinicalMedicine 2023, 55, 101762. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, T.; Shafran, R.; Ladhani, S.N. Long COVID in Children and Adolescents. Curr. Opin. Infect. Dis. 2022, 35, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Wulf Hanson, S.; Abbafati, C.; Aerts, J.G.; Al-Aly, Z.; Ashbaugh, C.; Ballouz, T.; Blyuss, O.; Bobkova, P.; Bonsel, G.; Borzakova, S.; et al. A Global Systematic Analysis of the Occurrence, Severity, and Recovery Pattern of Long COVID in 2020 and 2021. medRxiv 2022. [Google Scholar] [CrossRef]
- Wise, J. Covid-19: WHO Urges Action as 17 Million Long Covid Cases Are Estimated in Europe. BMJ 2022, 378, o2232. [Google Scholar] [CrossRef]
- National Center for Health Statistics. U.S. Census Bureau, Household Pulse Survey, 2022–2023. Long COVID. Available online: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm (accessed on 19 April 2023).
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact. eClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Ormiston, C.K.; Świątkiewicz, I.; Taub, P.R. Postural Orthostatic Tachycardia Syndrome as a Sequela of COVID-19. Heart Rhythm 2022, 19, 1880–1889. [Google Scholar] [CrossRef]
- Rich, E.M.; Vas, A.; Parsons, T.D.; Krone, R.; Goodman, B.P. Functional Status in Postural Tachycardia Syndrome. Br. J. Occup. Ther. 2022, 85, 418–426. [Google Scholar] [CrossRef]
- Benarroch, E.E. “Dysautonomia”: A Plea for Precision. Clin. Auton. Res. 2021, 31, 27–29. [Google Scholar] [CrossRef]
- Blitshteyn, S.; Whiteson, J.H.; Abramoff, B.; Azola, A.; Bartels, M.N.; Bhavaraju-Sanka, R.; Chung, T.; Fleming, T.K.; Henning, E.; Miglis, M.G.; et al. Multi-Disciplinary Collaborative Consensus Guidance Statement on the Assessment and Treatment of Autonomic Dysfunction in Patients with Post-Acute Sequelae of SARS-CoV-2 Infection (PASC). PM&R 2022, 14, 1270–1291. [Google Scholar] [CrossRef]
- Mayuga, K.A.; Fedorowski, A.; Ricci, F.; Gopinathannair, R.; Dukes, J.W.; Gibbons, C.; Hanna, P.; Sorajja, D.; Chung, M.; Benditt, D.; et al. Sinus Tachycardia: A Multidisciplinary Expert Focused Review. Circ. Arrhythm. Electrophysiol. 2022, 15, E007960. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A.; Ricci, F.; Hamrefors, V.; Sandau, K.E.; Hwan Chung, T.; Muldowney, J.A.S.; Gopinathannair, R.; Olshansky, B. Orthostatic Hypotension: Management of a Complex, But Common, Medical Problem. Circ. Arrhythm. Electrophysiol. 2022, 15, 212–229. [Google Scholar] [CrossRef]
- Nwazue, V.C.; Paranjape, S.Y.; Black, B.K.; Biaggioni, I.; Diedrich, A.; Dupont, W.D.; Robertson, D.; Raj, S.R. Postural Tachycardia Syndrome and Inappropriate Sinus Tachycardia: Role of Autonomic Modulation and Sinus Node Automaticity. J. Am. Heart Assoc. 2014, 3, e000700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raj, S.R.; Guzman, J.C.; Harvey, P.; Richer, L.; Schondorf, R.; Seifer, C.; Thibodeau-Jarry, N.; Sheldon, R.S. Canadian Cardiovascular Society Position Statement on Postural Orthostatic Tachycardia Syndrome (POTS) and Related Disorders of Chronic Orthostatic Intolerance. Can. J. Cardiol. 2020, 36, 357–372. [Google Scholar] [CrossRef] [Green Version]
- Cutsforth-Gregory, J.K.; Sandroni, P. Clinical Neurophysiology of Postural Tachycardia Syndrome. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; Volume 161, pp. 429–445. [Google Scholar] [CrossRef]
- Stewart, J.M.; Pianosi, P.; Shaban, M.A.; Terilli, C.; Svistunova, M.; Visintainer, P.; Medow, M.S. Postural Hyperventilation as a Cause of Postural Tachycardia Syndrome: Increased Systemic Vascular Resistance and Decreased Cardiac Output When Upright in All Postural Tachycardia Syndrome Variants. J. Am. Heart Assoc. 2018, 7, e008854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Whiteson, J.H.; Azola, A.; Barry, J.T.; Bartels, M.N.; Blitshteyn, S.; Fleming, T.K.; McCauley, M.D.; Neal, J.D.; Pillarisetti, J.; Sampsel, S.; et al. Multi-Disciplinary Collaborative Consensus Guidance Statement on the Assessment and Treatment of Cardiovascular Complications in Patients with Post-Acute Sequelae of SARS-CoV-2 Infection (PASC). PM&R 2022, 14, 855–878. [Google Scholar] [CrossRef]
- Bateman, L.; Bested, A.C.; Bonilla, H.F.; Chheda, B.V.; Chu, L.; Curtin, J.M.; Dempsey, T.T.; Dimmock, M.E.; Dowell, T.G.; Felsenstein, D.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clin. Proc. 2021, 96, 2861–2878. [Google Scholar] [CrossRef]
- Jason, L.A.; Dorri, J.A. ME/CFS and Post-Exertional Malaise among Patients with Long COVID. Neurol. Int. 2022, 15, 1–11. [Google Scholar] [CrossRef]
- Moore, G.E.; Keller, B.A.; Stevens, J.; Mao, X.; Stevens, S.R.; Chia, J.K.; Levine, S.M.; Franconi, C.J.; Hanson, M.R. Recovery from Exercise in Persons with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medicina 2023, 59, 571. [Google Scholar] [CrossRef]
- Singh, I.; Joseph, P.; Heerdt, P.M.; Cullinan, M.; Lutchmansingh, D.D.; Gulati, M.; Possick, J.D.; Systrom, D.M.; Waxman, A.B. Persistent Exertional Intolerance after COVID-19. Chest 2022, 161, 54–63. [Google Scholar] [CrossRef]
- de Boer, E.; Petrache, I.; Goldstein, N.M.; Olin, J.T.; Keith, R.C.; Modena, B.; Mohning, M.P.; Yunt, Z.X.; San-Millán, I.; Swigris, J.J. Decreased Fatty Acid Oxidation and Altered Lactate Production during Exercise in Patients with Post-Acute COVID-19 Syndrome. Am. J. Respir. Crit. Care Med. 2022, 205, 126–129. [Google Scholar] [CrossRef]
- Vermeulen, R.C.; Vermeulen van Eck, I.W. Decreased Oxygen Extraction during Cardiopulmonary Exercise Test in Patients with Chronic Fatigue Syndrome. J. Transl. Med. 2014, 12, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Clinical Management of COVID-19: Living Guideline/15.9.2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Clinical-2022.2?fbclid=IwAR3z0Lri3JSVnBgk7DFh8vTCOHNvwisMPN9Q4ciOPVNFwzESed-PDjK5D5Q (accessed on 15 April 2023).
- DeMars, J.; Brown, D.A.; Angelidis, I.; Jones, F.; McGuire, F.; O’Brien, K.K.; Oller, D.; Pemberton, S.; Tarrant, R.; Verduzco-Gutierrez, M.; et al. What Is Safe Long COVID Rehabilitation? J. Occup. Rehabil. 2022, 33, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Winker, R.; Barth, A.; Bidmon, D.; Ponocny, I.; Weber, M.; Mayr, O.; Robertson, D.; Diedrich, A.; Maier, R.; Pilger, A.; et al. Endurance Exercise Training in Orthostatic Intolerance. Hypertension 2005, 45, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Reilly, C.C.; Floyd, S.V.; Lee, K.; Warwick, G.; James, S.; Gall, N.; Rafferty, G.F. Breathlessness and Dysfunctional Breathing in Patients with Postural Orthostatic Tachycardia Syndrome (POTS): The Impact of a Physiotherapy Intervention. Auton. Neurosci. Basic Clin. 2020, 223, 102601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, S.A.; Bivens, T.B.; Howden, E.J.; Saleem, Y.; Galbreath, M.M.; Hendrickson, D.; Fu, Q.; Levine, B.D. The International POTS Registry: Evaluating the Efficacy of an Exercise Training Intervention in a Community Setting. Heart Rhythm 2016, 13, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; VanGundy, T.B.; Shibata, S.; Auchus, R.J.; Williams, G.H.; Levine, B.D. Exercise Training Versus Propranolol in the Treatment of the Postural Orthostatic Tachycardia Syndrome. Hypertension 2011, 58, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Shibata, S.; Fu, Q.; Bivens, T.B.; Hastings, J.L.; Wang, W.; Levine, B.D. Short-Term Exercise Training Improves the Cardiovascular Response to Exercise in the Postural Orthostatic Tachycardia Syndrome. J. Physiol. 2012, 590, 3495–3505. [Google Scholar] [CrossRef]
- WMA. Deklaration von Helsinki. Available online: http://www.bundesaerztekammer.de/fileadmin/user_upload/Deklaration_%0Avon_Helsinki_2013_DE.pdf (accessed on 22 April 2023).
- Katsarou, M.-S.; Iasonidou, E.; Osarogue, A.; Kalafatis, E.; Stefanatou, M.; Pappa, S.; Gatzonis, S.; Verentzioti, A.; Gounopoulos, P.; Demponeras, C.; et al. The Greek Collaborative Long COVID Study: Non-Hospitalized and Hospitalized Patients Share Similar Symptom Patterns. J. Pers. Med. 2022, 12, 987. [Google Scholar] [CrossRef]
- Ewing, D.J.; Martyn, C.N.; Young, R.J.; Clarke, B.F. The Value of Cardiovascular Autonomic Function Tests: 10 Years Experience in Diabetes. Diabetes Care 1985, 8, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Vernon, S.D.; Jeys, P.; Ali, W.; Campos, A.; Unutmaz, D.; Yellman, B.; Bateman, L. Hemodynamics during the 10-Minute NASA Lean Test: Evidence of Circulatory Decompensation in a Subset of ME/CFS Patients. J. Transl. Med. 2020, 18, 314. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Daniel, L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotler, J.; Holtzman, C.; Dudun, C.; Jason, L. A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics 2018, 8, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, D.; Solway, S.; Gibbons, W.J. ATS Statement-Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Crouch, R. 1-Minute Sit-to-Stand Test. J. Cardiopulm. Rehabil. Prev. 2019, 39, 2–8. [Google Scholar] [CrossRef]
- Powell, L.E.; Myers, A.M. The Activities-Specific Balance Confidence (ABC) Scale. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50A, M28–M34. [Google Scholar] [CrossRef]
- Chapman, E.B.; Hansen-Honeycutt, J.; Nasypany, A.; Baker, R.T.; May, J. A Clinical Guide to The Assessment and Treatment Of Breathing Pattern Disorders in the Physically Active: Part 1. Int. J. Sports Phys. Ther. 2016, 11, 803–809. [Google Scholar]
- Mahler, D.A.; Wells, C.K. Evaluation of Clinical Methods for Rating Dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Grammatopoulou, E.P.; Skordilis, E.K.; Georgoudis, G.; Haniotou, A.; Evangelodimou, A.; Fildissis, G.; Katsoulas, T.; Kalagiakos, P. Hyperventilation in Asthma: A Validation Study of the Nijmegen Questionnaire—NQ. J. Asthma 2014, 51, 839–846. [Google Scholar] [CrossRef]
- van Dixhoorn, J.; Duivenvoorden, H.J. Efficacy of Nijmegen Questionnaire in Recognition of the Hyperventilation Syndrome. J. Psychosom. Res. 1985, 29, 199–206. [Google Scholar] [CrossRef]
- Ferentinos, P.; Kontaxakis, V.; Havaki-Kontaxaki, B.; Dikeos, D.; Lykouras, L. Psychometric Evaluation of the Fatigue Severity Scale in Patients with Major Depression. Qual. Life Res. 2011, 20, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B. The Fatigue Severity Scale. Arch. Neurol. 1989, 46, 1121. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. Hell. J. Cardiol. 2009, 50, 283–294. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Konstantopoulos, K.; Vogazianos, P.; Doskas, T. Normative Data of the Montreal Cognitive Assessment in the Greek Population and Parkinsonian Dementia. Arch. Clin. Neuropsychol. 2016, 31, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Kontodimopoulos, N.; Pappa, E.; Niakas, D.; Yfantopoulos, J.; Dimitrakaki, C.; Tountas, Y. Validity of the EuroQoL (EQ-5D) Instrument in a Greek General Population. Value Health 2008, 11, 1162–1169. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and Preliminary Testing of the New Five-Level Version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Mystakidou, K.; Tsilika, E.; Parpa, E.; Katsouda, E.; Galanos, A.; Vlahos, L. The Hospital Anxiety and Depression Scale in Greek Cancer Patients: Psychometric Analyses and Applicability. Support. Care Cancer 2004, 12, 821–825. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G.A. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Jones, N. Appendix D. Normal Standards. In Clinical Exercise Testing; WB Saunders Company: Philadephia, PA, USA, 1988; pp. 243–247. [Google Scholar]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A New Method for Detecting Anaerobic Threshold by Gas Exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Kaminski, D.; Sliwinski, P. Reliability of Inspiratory Capacity for Estimating End-Expiratory Lung Volume Changes during Exercise in Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 1997, 156, 55–59. [Google Scholar] [CrossRef]
- Parker, M.J.; Manan, A.; Duffett, M. Rapid, Easy, and Cheap Randomization: Prospective Evaluation in a Study Cohort. Trials 2012, 13, 90. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.-W.; Tetzlaff, J.M.; Gotzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hrobjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 Explanation and Elaboration: Guidance for Protocols of Clinical Trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Q.; Levine, B.D. Exercise in the Postural Orthostatic Tachycardia Syndrome. Auton. Neurosci. 2015, 188, 86–89. [Google Scholar] [CrossRef] [Green Version]
- Quade, D. Rank Analysis of Covariance. J. Am. Stat. Assoc. 1967, 62, 1187. [Google Scholar] [CrossRef]
- AL-Mhanna, S.B.; Mohamed, M.; Noor, N.M.; Afolabi, H.A.; Irekeola, A.A.; Bello, K.E.; Aldhahi, M.I.; Wan Ghazali, W.S. Effectiveness of Pulmonary Rehabilitation among COVID-19 Patients: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 2130. [Google Scholar] [CrossRef]
- Huang, J.; Fan, Y.; Zhao, K.; Yang, C.; Zhao, Z.; Chen, Y.; Yang, J.; Wang, T.; Qu, Y. Do Patients with and Survivors of COVID-19 Benefit from Telerehabilitation? A Meta-Analysis of Randomized Controlled Trials. Front. Public Health 2022, 10, 954754. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gotzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Adults 18–65 years of age | Absolute or relative contraindications to exercise due to cardiac pathology |
| * WHO definition of post-COVID-19 condition | Serious mental/cognitive impairment that will not allow systematic participation |
| Confirmed dysautonomia diagnosis through Ewing Battery | Unable to regularly reach the center Pregnancy |
| Able to attend 2 times/week for 8 weeks | * CFS/ME fulfilling the Canadian Consensus Criteria |
| Able to provide informed consent | Secondary health conditions that would explain symptoms, intervene in dysautonomia diagnosis or would impede participation in the exercise protocol (i.e., untreated hypothyroidism and Diabetes Melitus, major psychiatric disorders, * COPD, * PICS, pulmonary fibrosis, chronic respiratory or heart failure, not ambulatory, suffering from dementia, chronically paralyzed, with paraplegia, with multiple injuries or other serious orthopedic problems that caused disability, patients suffering from very serious underlying diseases such as end-stage cancer, and those with neurological diseases causing disability) |
| Conservative Measures | |
|---|---|
| 1 | 3–4 liquid intake per day |
| 2 | 500 mL of water before getting out of bed in the morning and before exercise |
| 3 | 8–12 g of salt daily |
| 4 | Graduated compression garment (ideally class II (20–30 mmHg) covering the lower body and/or an abdominal binder based on tolerance) |
| 5 | Leveling up the head of the bed by 10–18 cm with a bed riser or a full length wedge underneath the mattress. |
| 6 | Maneuvers that increase venous return in case of discomfort/dizziness when standing (leg crossing, isometric contraction of lower limbs, abrupt coughing, squatting) |
| 7 | Avoidance of large meals rich in fat-favoring smaller regular meals |
| 8 | Avoidance of high temperatures, caffeine, and alcohol intake |
| 9 | Exercise in the seated position or swimming |
| 10 | Medication as indicated |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spaggoulakis, D.; Kontaxakis, A.; Asimakos, A.; Spetsioti, S.; Antonoglou, A.; Gounopoulos, P.; Katsarou, M.; Iasonidou, H.; Gatzonis, S.-S.; Katsaounou, P. Protocol of the Long-COVID Patients Causal Diagnosis and Rehabilitation Randomized Feasibility Controlled Trial in Patients with Dysautonomia: The LoCoDiRe-Dys Study. BioMed 2023, 3, 309-319. https://doi.org/10.3390/biomed3030026
Spaggoulakis D, Kontaxakis A, Asimakos A, Spetsioti S, Antonoglou A, Gounopoulos P, Katsarou M, Iasonidou H, Gatzonis S-S, Katsaounou P. Protocol of the Long-COVID Patients Causal Diagnosis and Rehabilitation Randomized Feasibility Controlled Trial in Patients with Dysautonomia: The LoCoDiRe-Dys Study. BioMed. 2023; 3(3):309-319. https://doi.org/10.3390/biomed3030026
Chicago/Turabian StyleSpaggoulakis, Dimitrios, Antonios Kontaxakis, Andreas Asimakos, Stavroula Spetsioti, Archontoula Antonoglou, Pantelis Gounopoulos, Martha Katsarou, Helen Iasonidou, Stergios-Stylianos Gatzonis, and Paraskevi Katsaounou. 2023. "Protocol of the Long-COVID Patients Causal Diagnosis and Rehabilitation Randomized Feasibility Controlled Trial in Patients with Dysautonomia: The LoCoDiRe-Dys Study" BioMed 3, no. 3: 309-319. https://doi.org/10.3390/biomed3030026