1. Introduction
COVID-19 is a serious infectious disease caused by SARS-CoV-2 virus and is responsible for almost 6 million deaths worldwide since its emergence in 2019 [
1]. COVID-19 has disrupted normal life and has enforced a substantial change in the policies, priorities and activities of individuals, organisations and governments [
2,
3,
4]. Vaccination has been a key in our fight against this disease (in addition to preventive measures such as masks, lockdowns, isolation etc.). Several different types of effective vaccines were prepared and approved in a remarkably short duration. Although around 60% of the world population is now fully vaccinated [
5], the fight against COVID-19 is far from over mainly because COVID-19 has been evolving into different variants with higher transmissibility and severity. Moreover, vaccines have been found to be less effective against some of these variants [
6]. Some of the most notable variants include Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2) and Omicron (B.1.1.529). Newly evolved COVID-19 variants have led to an increasing call for booster doses [
7].
Some countries have recently experienced high mortality rates despite the ongoing vaccination drive [
8] which is partly due to the inefficacy of vaccines on new COVID-19 variants. The impact of vaccines in mitigating COVID-19 pandemic has been dissimilar in different countries. This is possibly due to the differences in protective measures, demographics, and types of vaccines used by different countries. There may be other factors involved such as the difference in the acceptance of vaccines in different regions and different prosocial behavior of people [
9,
10]. Thus, there is a need to study COVID-19 in different countries considering different vaccines, age groups and variants etc.
To the best of our knowledge, we are the first to present a detailed correlation study of COVID-19 in 30 European countries considering different types of vaccines, age groups and variants. Many of the existing studies on the effectiveness of COVID-19 vaccines are based on clinical trials [
11]. A few existing studies use publicly available datasets to study the impact of COVID-19 vaccinations in different countries [
12]. The effectiveness of some specific vaccines on COVID-19 mortality rates and related symptoms is analysed in [
13]. Impact of a double dose COVID-19 vaccination campaign on reducing hospitalisations and deaths in the United States (US) is evaluated in [
14]. A correlation of Bacille Calmette–Guérin (BCG) vaccination policy and reduced mortality rates is provided in [
15]. The effectiveness of vaccines for people aged 65 years and above is analysed in [
16]. The efficacy of COVID-19 vaccines against Delta variant is analysed in a recent study [
17].
In contrast to the existing studies mentioned above, we present a comprehensive analysis considering a variety of important factors. Specifically, we use publicly available datasets and present a set of detailed correlation analyses considering 6 different COVID-19 vaccines, 20 COVID-19 variants, and different age groups in 30 European countries. Four different sets of correlation analyses are presented in this paper by using data ranged from Week 1 of 2021 to Week 5 of 2022. The main contributions are summarised below.
A correlation analysis between the total number of administered vaccines and weekly COVID-19 cases and deaths is conducted. We present the correlation analyses for the whole Europe as well as each of the 30 countries separately.
We present a correlation study between different types of vaccines and COVID-19 cases and deaths. Country-wise correlation analyses are also presented for these vaccines.
We provide a correlation analysis between the number of age-wise administered vaccine doses and weekly COVID-19 cases and deaths. The age-wise analyses are alsresented separately for different types of vaccines.
We also present detailed correlation analyses between the total number of doses administered and cases of different COVID-19 variants including the prevalent Delta and Omicron variants.
The correlation trends show how the correlation evolves with time i.e., the change in correlation with respect to change in vaccination rate and COVID-19 cases. The correlation graphs plotted with the variant-wise cases exhibit important insights. There are many dissimilarities in the correlation trends for many countries. However, most of the countries show an abrupt increase in the correlation around week 15 and after week 45. The increase in correlation is potentially due to the emergence of different COVID-19 variants around those weeks.
2. Related Work
Most of the existing work to evaluate the effectiveness of vaccine are based on empirical analysis of the data. The effectiveness of Pfizer-BioNTech BNT162b2 and Oxford-AstraZeneca ChAdOx1-S vaccines against confirmed COVID-19 symptoms, admissions to hospitals and deaths is estimated in [
13]. It concludes that the vaccination with either one dose of Pfizer or AstraZeneca is associated with a significant reduction in symptomatic COVID-19 in older adults. A few studies are based on computational models. The work in [
14] evaluates the impact of double dose COVID-19 vaccination campaign on reducing incidence, hospitalizations and deaths in the United States (US). An agent-based model is developed and parameterized with US demographics and age-specific COVID-19 outcomes. Another study evaluates the impact of age-specific vaccination in reducing daily cases, hospitalization and death rates in Tennessee [
12]. The study indicates that vaccination targeting older age groups is the optimal way to avoid higher transmissions. It also reduces hospitalization and death rates in older age groups. A progress report provides an overview of ongoing vaccine efficacy studies [
11]. The report is based on clinical trials of vaccines on different COVID-19 variants. It suggests that a comprehensive research is required to prepare for an unknown future pathogen. Most of these research studies are based on empirical methods and clinical trials. The statistical relationship/association between vaccination rates and confirmed COVID-19 cases and deaths can also be considered to support these empirical analysis.
Some research studies on the effectiveness of COVID-19 vaccines are based on correlation analysis. A recent research study compares Bacillus Calmette–Guérin (BCG) vaccination policies with the morbidity and mortality for COVID-19 in middle-high and high-income countries [
15]. It concludes that the countries without universal policies of BCG vaccination have been more severely affected as compared to the countries with universal and long-standing BCG policies. Authors in [
18] developed an application to evaluate COVID-19 vaccines using a public COVID-19 database. The application is based on the correlation between the number of daily administered vaccine doses and the number of new COVID-19 cases and deaths. Another study examines the correlation between COVID-19 vaccine coverage rates and impact of COVID-19 variants based on real-world data [
19]. A report provides a correlation between the case fatality rates of COVID-19 and the percentage of BCG vaccination coverage in 183 most affected countries [
20]. Effectiveness of vaccines against hospitalization with COVID-19 is estimated in [
21]. Correlation of COVID-19 with different diseases is observed in [
22]. It clusters different countries based on the correlation.
A number of research articles present an analysis on the impact of vaccines in different countries. A striking comparison between the similar-sized and neighboring countries of Bahrain and Qatar is presented in [
23]. It also compares the outcomes of the top 10 vaccinated countries based on their reliance on inactivated virus vaccines. Another article explores the impact of vaccines on COVID-19 in countries with vaccination rate below the herd immunity threshold [
24]. A major impact of vaccines on reducing infection rates is observed in Israel, UAE, Chile, United Kingdom, United States, Hungary and Qatar. The vaccine’s effectiveness against SARS-CoV-2 infection is measured in 8 European countries using a multicentre test-negative design in [
16]. The study concludes that the vaccination provides substantial protection against COVID-19 presentation at primary care among those aged 65 and above. Another article investigates the relationship between the fully vaccinated population and new COVID-19 cases across 68 countries and across 2947 counties in US [
25]. It observes that the increase in COVID-19 cases are unrelated to the levels of vaccination across 68 countries and 2947 counties in the US. Descriptive statistics and bivariate correlations for vaccination rates and cases across counties in New York State (NYS) are presented in [
26]. Results reveal that the two-dose vaccination rate is a significant negative predictor of cases per 100K population.
Some existing studies focus on the effectiveness of certain COVID-19 vaccines on some specific COVID-19 variants. The effectiveness of Pfizer vaccine against Alpha (B.1.1.7) and Beta (B.1.351) variant is estimated with a test-negative case–control study design in [
27]. It observes Pfizer vaccine to be 95% effective on Alpha variant and 75.0% effective on Beta variant. The efficacy of AstraZeneca vaccine against Beta variant is clinically investigated in [
28]. It explores that the two-dose regimen of AstraZeneca vaccine does not show protection against mild-to-moderate COVID-19 caused by Beta variant. The effectiveness of Novavax vaccine against different COVID-19 variants is discussed in [
29]. It shows that Novavax vaccine is more than 85% effective against a COVID-19 variant detected in the United Kingdom. An article presents results on the effectiveness and the duration of protection provided by EU-licensed COVID-19 vaccines against Delta variant [
30]. It considers all those studies that investigate the vaccine effectiveness against SARS-CoV-2 infection. The effectiveness of Pfizer vaccine against Omicron variant in South Africa is investigated in [
31]. It considers PCR test results and observes the reduction in the effectiveness of the vaccine due to the emergence of Omicron variant. A test-negative case-control design is used in [
17] to estimate the effectiveness of vaccination against Delta variant. Modest differences in vaccine effectiveness were noted for Delta variant as compared to Alpha variant after the administration of 2 doses.
The studies mentioned above are limited in at least one of the following ways: (1) the studies consider the overall vaccination rate and do not take into account the type of vaccines administered; (2) the studies do not consider effect of vaccinating different age groups; (3) the effect of vaccines on different COVID-19 variants is not considered; (4) the studies are limited to only one country (or a few countries). In this paper, we present a comprehensive study considering six different vaccines, 10 different age groups, 20 COVID-19 variants and 30 countries in Europe (see
Table 1).
4. Results and Analyses
In this section, we present correlation analyses between the total number of administered vaccine doses and weekly COVID-19 cases/deaths. Specifically, in
Section 4.1, we present and analyse the results for correlation considering overall data regardless of vaccine types, age groups and variants. In
Section 4.2, we discuss the correlation considering different types of vaccines.
Section 4.3 presents the correlation between the total number of doses administered to different age groups and weekly COVID-19 cases/deaths. Finally, in
Section 4.4, we present the results considering different COVID-19 variants.
For each of the sections, we present the overall results for all 30 European countries as well as for each country individually. Given the large number of results, we only present overall results for Europe in the main text. Appendices contain country-wise results of the most prevalent variants (Alpha, Delta and Omicron) and the most widely used vaccines (AstraZeneca, Pfizer and Moderna). Rest of the results are made available in the
supplementary file. Specifically, country-wise results for
Section 4.1 are given in
Appendix A. In
Appendix B, we present country-wise figures for AstraZeneca, Pfizer and Moderna. Age-wise results for AstraZeneca, Pfizer and Moderna are given in
Appendix C. Country-wise results for three of the most prevalent COVID-19 variants (Alpha, Delta and Omicron) are given in
Appendix D. All other figures can be found in the
Supplementary File provided with this submission.
4.1. Correlation Considering All Vaccine Types, Age Groups and Variants
This section provides the correlation between total administered vaccine doses and weekly COVID-19 cases/deaths (regardless of the vaccine type, age groups and COVID-19 variants). We present and analyse the results for weekly COVID-19 cases and COVID-19 deaths in
Section 4.1.1 and
Section 4.1.2, respectively.
4.1.1. Correlation between Total Doses and Weekly Cases
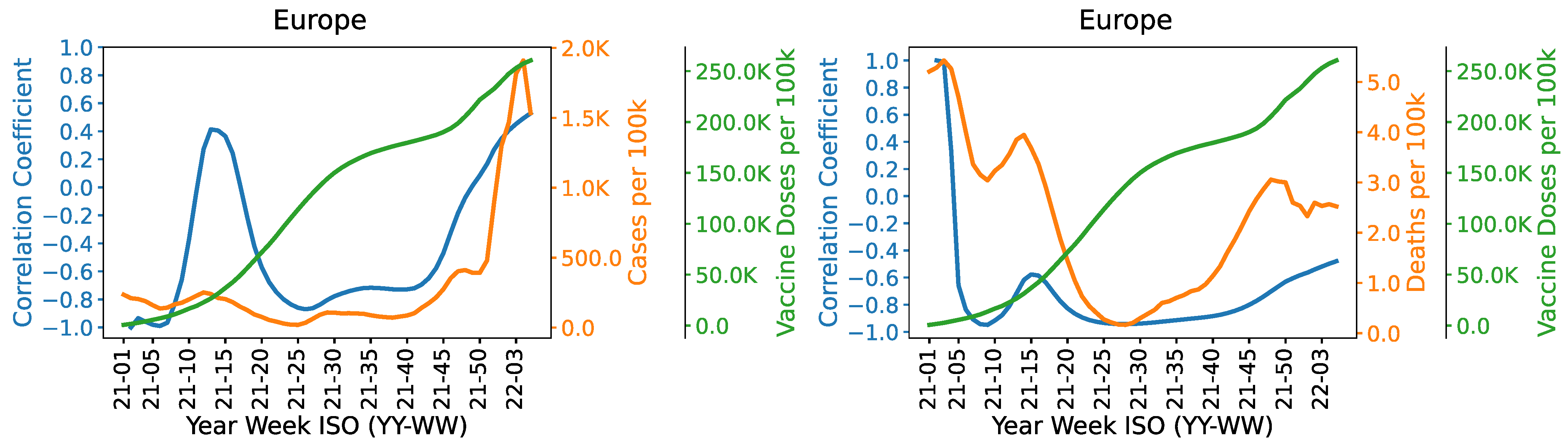
Overall results. First, we discuss the overall results for all of the European countries considered in this study. The correlation between cumulative vaccine doses and weekly COVID-19 cases is shown in
Figure 2. A significant positive surge in correlation can be seen from around 10th to 15th week. This may be partly due to the emergence of Alpha variant in these weeks and low vaccination rate during the initial few weeks.
Figure A14 and
Figure A15 show the emergence of Alpha variant in these weeks. From week 15 onwards, as the vaccination rate increases (and possibly due to the additional protection measures such as lockdowns), the correlation becomes negative and the weekly cases start dropping. The case numbers start increasing again at around week 25 and the correlation starts moving towards positive mainly due to the emergence of Delta variant which was the prevalent variant around that time (as can be seen in
Figure A16 and
Figure A17). The weekly case numbers and the correlation sharply increase at around week 45 and onwards. This is mainly due to the emergence of the highly contiguous Omicron variant which became the prevalent variant at around week 45 onwards (see
Figure A18 and
Figure A19). The correlation remains significantly negative from week 20 to 45 indicating the positive impact of vaccination rate in reducing COVID-19 cases. This changes after week 45 mainly because of the waning effectiveness of vaccines and reduced efficacy of vaccines against Omicron.
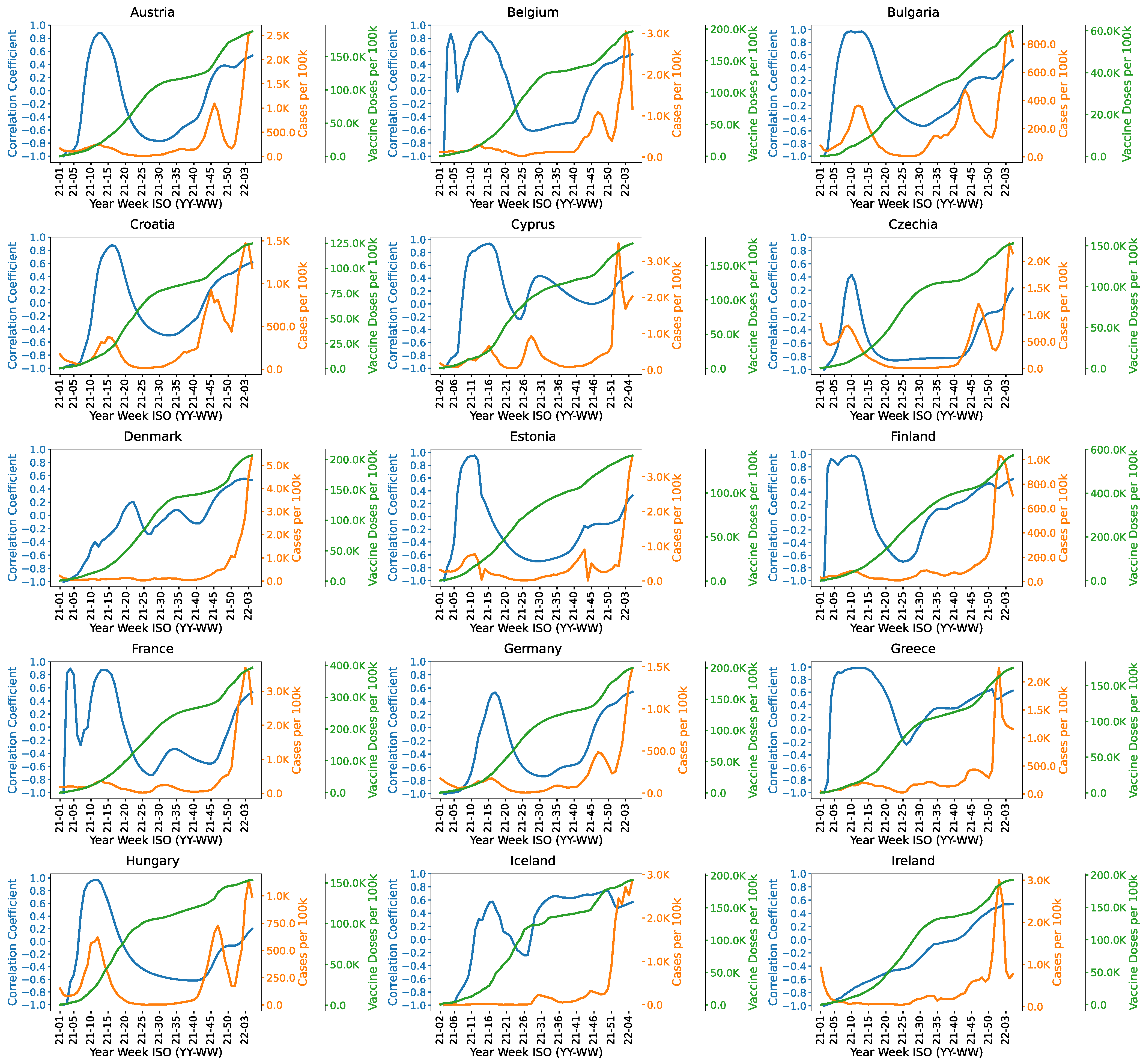
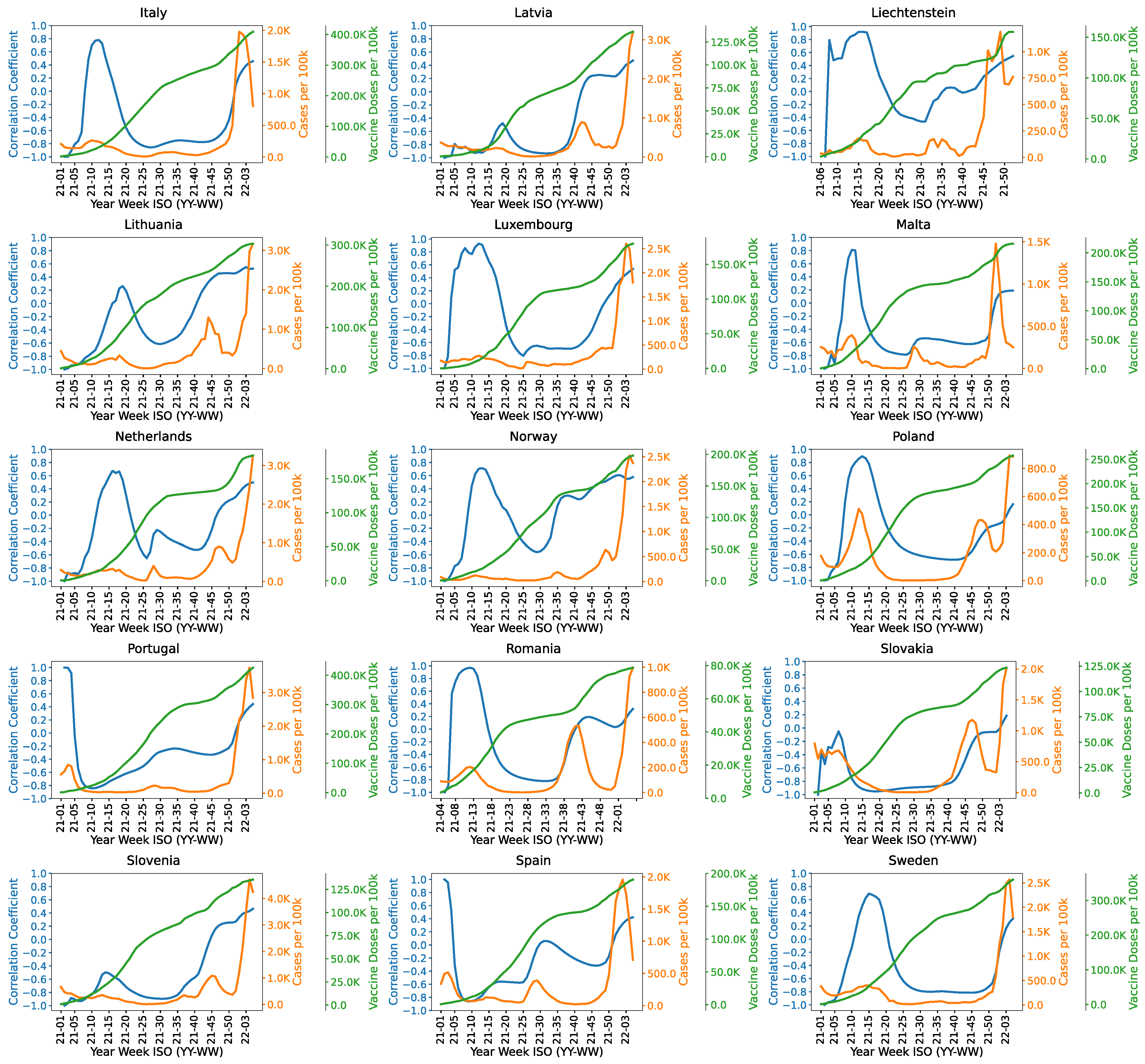
Country-wise results.Figure A1 and
Figure A2 show the country-wise correlation results for the European countries considered in this study. Similar to the overall results, most of the countries have a positive peak in the correlation between 10th and 20th weeks. Moreover, the correlation starts increasing around 45th week in most of the countries mainly due to the emergence of Omicron variant. In Austria, the correlation is highly negative from week 20 to week 40. There is a significant increase in the correlation after the 43rd week. Bulgaria, Croatia, Estonia, France, Hungary, Germany, Luxembourg and Romania show similar correlation trends. However, the negative correlation spans from week 15 to week 45 in Czechia, Italy, Malta and Slovakia. The correlation graphs of Denmark, Iceland, Norway, Netherlands, Liechtenstein and Finland show an increase in the correlation around 30th week. It might be due to the prevalence of Delta variant (B.1.617.2) in these countries as shown in
Figure A16 and
Figure A17. In Greece, Cyprus and Iceland, the correlation trend remains positive in almost all weeks. It might be due to the exposure of highly transmissible variants leading to high number of COVID-19 cases. Prominent variants in Greece are Alpha and Delta as shown in
Figure A14 and
Figure A16. Cyprus has relatively higher number of cases of Alpha and Delta variants. Latvia, Slovenia and Slovakia show a significant negative correlation in most of the weeks as compared to the other countries. These countries show an increasing trend in the correlation after 40th week due to Omicron variant. Portugal and Spain have a similar correlation trend. The correlation is highly negative around week 10 but increases afterwards, which is partly because the case numbers remain relatively stable and do not decrease significantly.
4.1.2. Correlation between Total Doses and Weekly Deaths
Overall results. First, we show the correlation between the total administered doses and weekly COVID-19 deaths for all European countries considered in the study.
Figure 2 shows that the number of weekly deaths generally decreases with the increase in the vaccination rate. There is a strong negative correlation between the total number of doses administered and weekly deaths. The negative correlation becomes somewhat weaker when new variants of concerns emerge, e.g., around week 10 when Alpha variant emerges and around week 45 when Omicron variant spreads. Overall, the results show that the vaccination significantly reduces the number of weekly deaths even when the number of cases sharply increase due to the emergence of new variants.
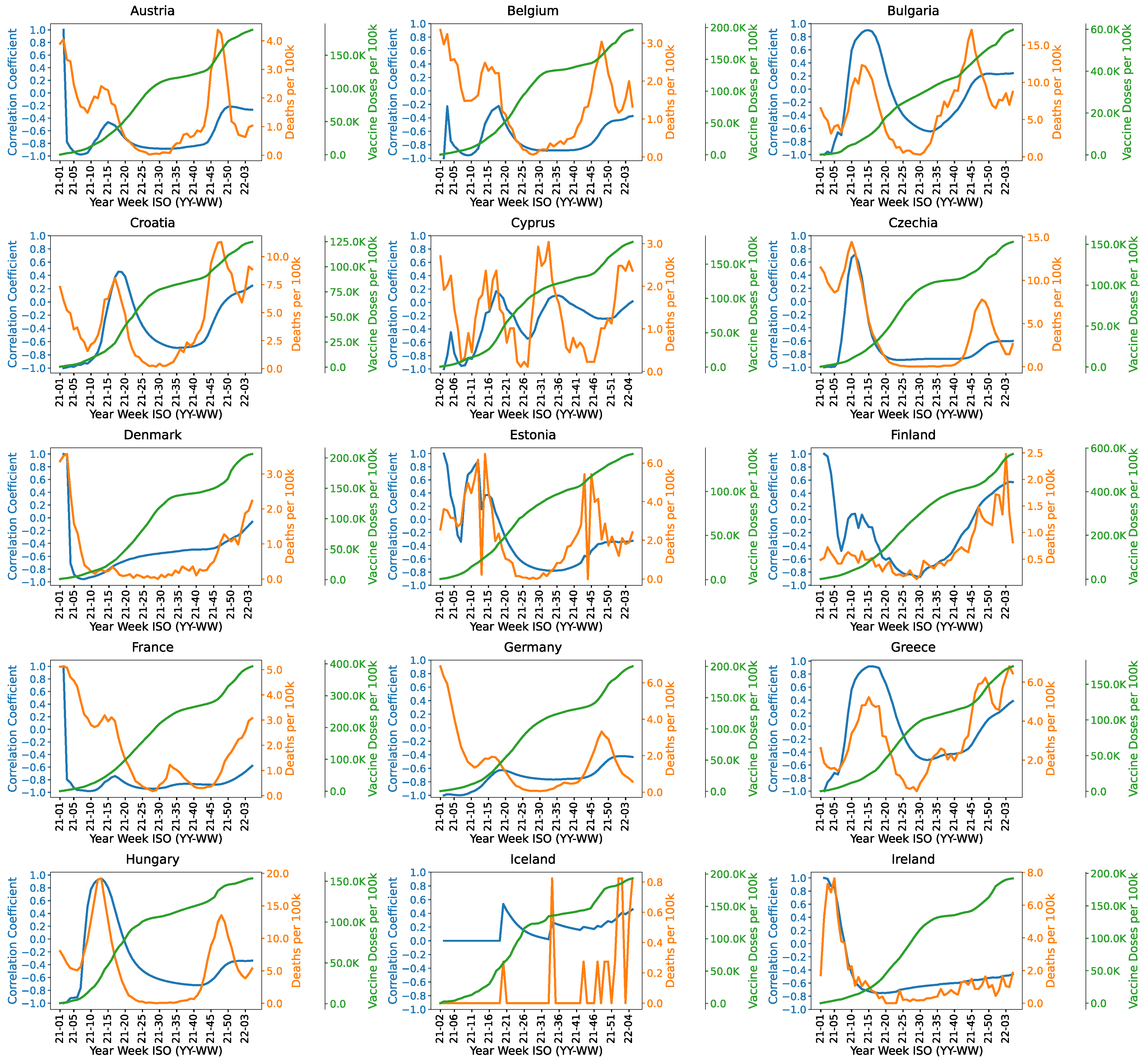
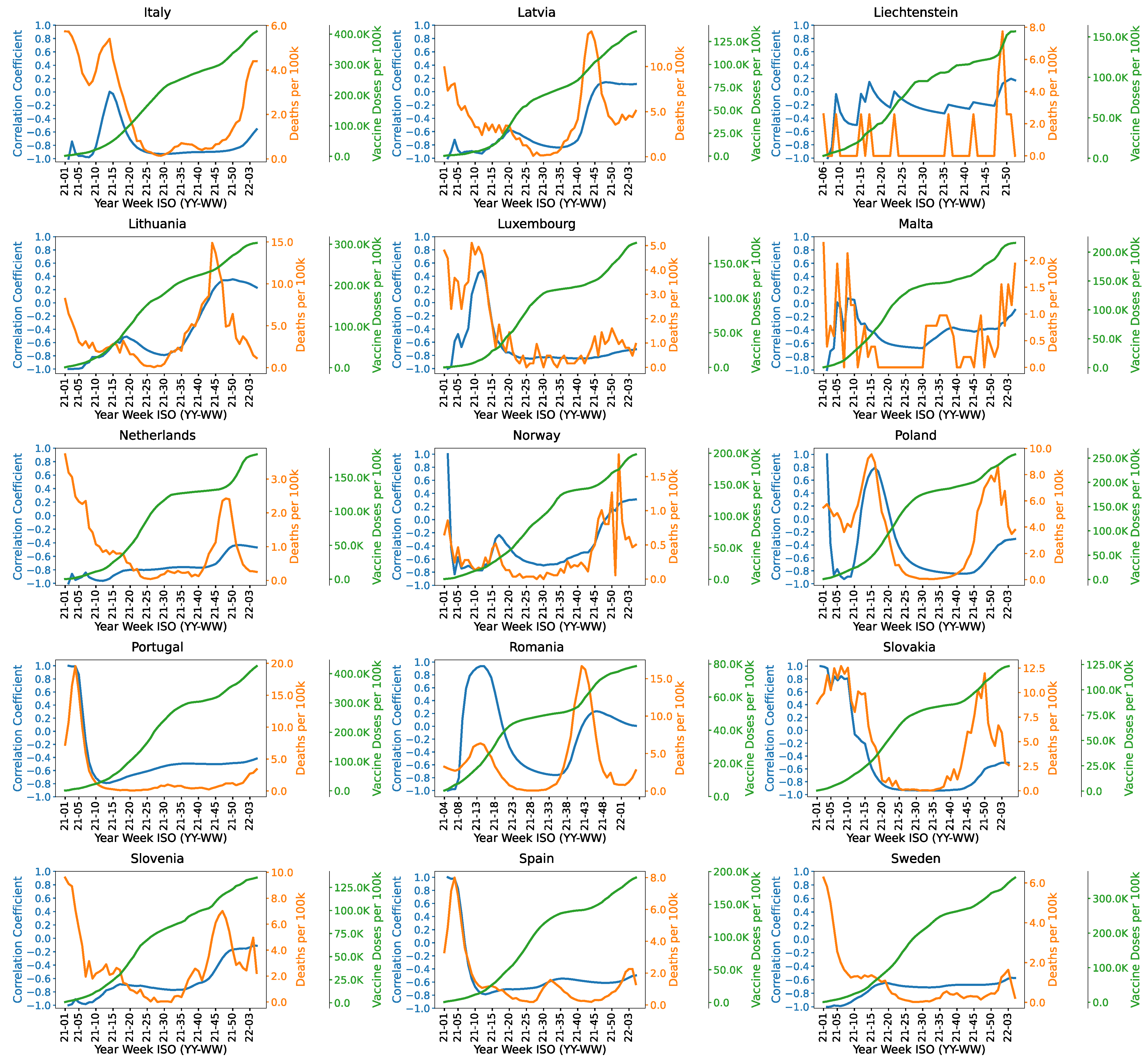
Country-wise results.Figure A3 and
Figure A4 show the country-wise correlation results between the total administered doses and weekly COVID-19 deaths. The correlation starts increasing after week 45 in most countries. Some countries have a positive peak in the correlation from week 10 to 20 which is partly due to the emergence of Alpha variant and low vaccination rates in the initial phase. This peak is more prominent in Bulgaria and Greece. The correlation trend is consistently negative in Denmark, France, Germany, Ireland, Netherlands, Portugal, Slovenia, Spain and Sweden. It reflects the positive efficacy of vaccines in these countries. Luxembourg and Italy show the similar correlation pattern except a positive peak in the correlation from week 10th to 15th. It may be due to the emergence of Alpha variant in Luxembourg and Italy as evident in
Figure A15. Austria and Belgium have a small peak in the correlation between week 10th to 20th. It might be due to the prevalence of Alpha variant in these countries.
Figure A14 and
Figure A15 show weekly reported cases of Alpha variant. This peak is more prominent in Bulgaria, Croatia, Czechia, Estonia, Greece, Malta, Poland and Romania. It shows positive correlation between week 10th to 25th. Prevalence of Alpha variant in these countries is evident from
Figure A14. The correlation in these countries starts increasing around 45th week. It might be due to the high number of cases of Delta and Omicron as evident in
Figure A16 and
Figure A18. The correlation is not very meaningful for Iceland as there are very few COVID-19 deaths in Iceland and, for most of the weeks, there were zero COVID-19 deaths.
4.2. Correlation Considering Different Vaccine Types
This section provides a correlation analysis between the total administered doses of different COVID-19 vaccines and weekly COVID-19 cases/deaths. For each vaccine type, the number of COVID-19 cases/deaths represents the sum of weekly cases/deaths considering only the countries where the vaccine was administered. For instance, if a vaccine is only administered in countries named x and y, then the number of cases/deaths is the sum of weekly cases/deaths in countries x and y per 100k of the total population of the two countries. We also provide country-wise results for each vaccine. Some vaccines are not administered in all 30 countries. For instance, Beijing’s CNBG (Sinopharm) is only administered in Hungary, and Sputnik is administered in Hungary and Slovakia.
4.2.1. Correlation between the Total Doses of Different Vaccines and Weekly Cases
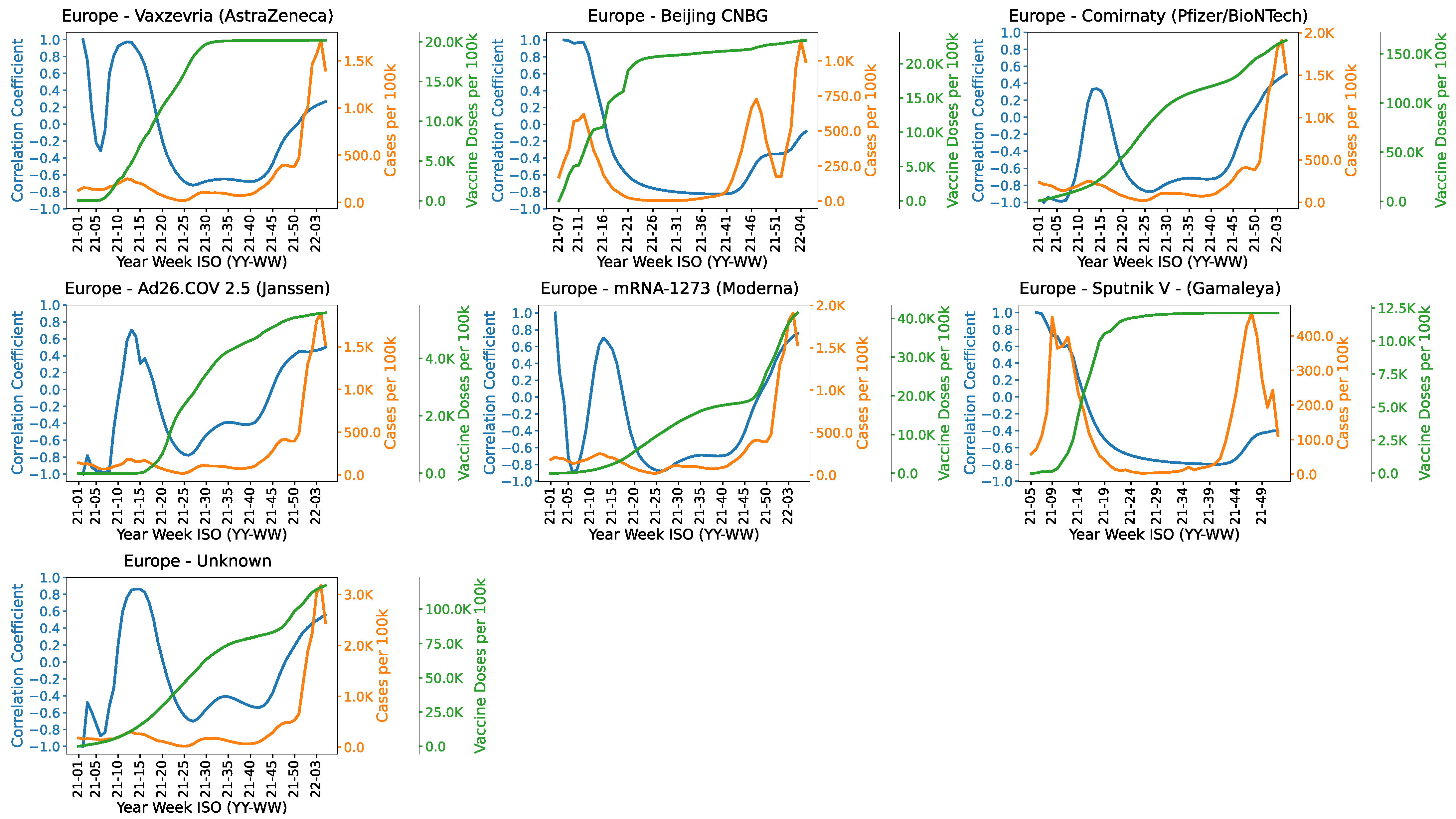
Overall results.Figure 3 shows the correlation between administered doses of different COVID-19 vaccines and COVID-19 cases. The correlation for AstraZeneca starts decreasing as more doses are administered which demonstrate its notable impact in controlling COVID-19. In Europe, Beijing’s CNBG (Sinopharm) vaccine was only administered in Hungary. The correlation trend reflects a significant impact of the vaccine against COVID-19 cases as evident from the graph. The correlation increases after 45th week which might be due to the prevalence of Omicron variant. The correlation for Pfizer Vaccine has a positive spike from week 10 to 20. It is evident from
Figure A14 and
Figure A15 that Alpha variant was prevalent from week 10 to 20 in all countries. The correlation then remains consistently negative until week 45. The correlation starts rising gain after week 45 which might be due to the emergence of Omicron variant. The correlation of Janssen does not clearly show a strong impact of the vaccine in reducing COVID-19 cases and deaths. There is a spike in cases and deaths from week 10 to 15 potentially due to Alpha variant which was prevalent during that time. The correlation starts increasing again after the 30th week. It might be due to Delta variant which emerged after week 30 in most countries. Please also note that the number of Janssen doses administered per 100K is significantly smaller than those of some other vaccines such as AstraZeneca and Pfizer. The correlation trend for Moderna vaccine is similar to Janssen vaccine. There is a spike in the 10th week. Cases start rising again from the 40th week. The impact of Sputnik in reducing COVID-19 cases and deaths have been very prominent as shown by the steady negative correlation from week 20 to 40. The correlation starts increasing after 42th week. It may be due to the Omicron variant. The effect of unknown vaccines have been quite similar to other vaccines where we see a spike in cases in the 10–11th week.
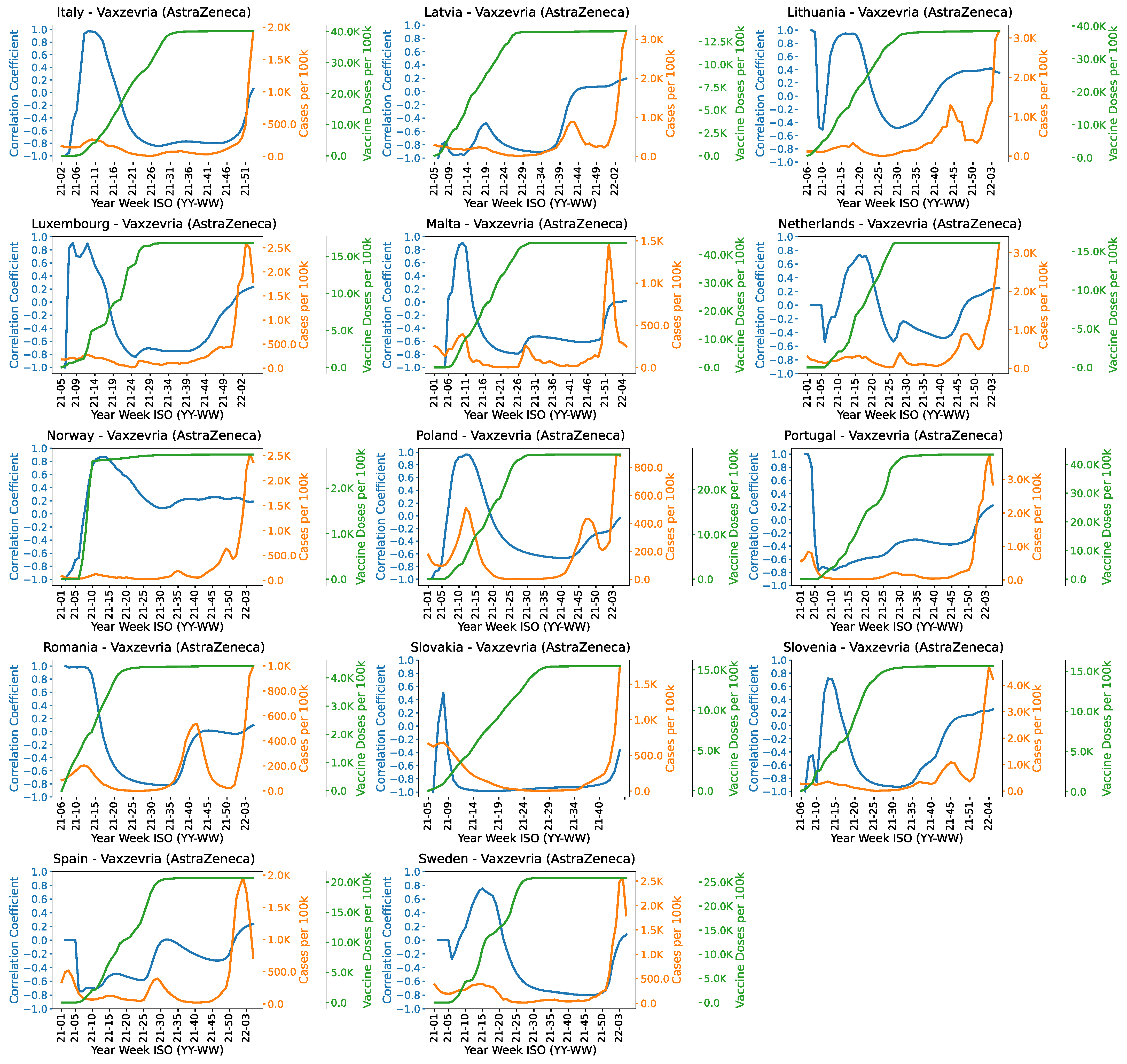
Country-wise results. The figures showing country-wise results for three of the most popular and widely-used vaccines (AstraZeneca, Pfizer and Moderna) are given in
Appendix B. Figures for other vaccines can be found in the
Supplementary File.
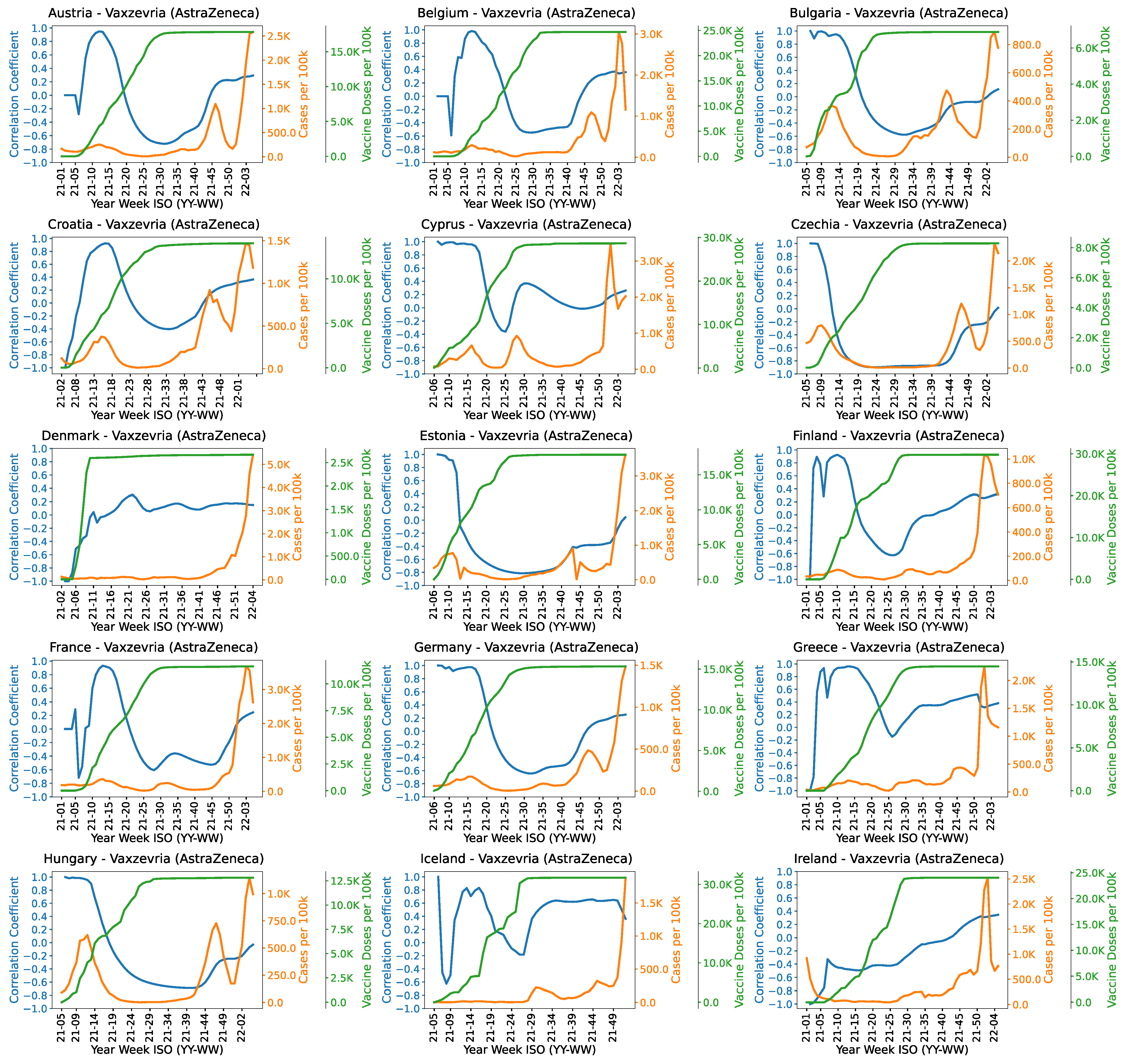
Figure A5 and
Figure A6 show the country-wise correlation for AstraZeneca. There are some unexpected trends in the correlation for some countries. In Cyprus and Spain, cases start increasing after 25th week. It might be due to the prevalence of Delta variant in those days.
Figure A16 shows the cases of Delta variant which emerged after week no 25. Ireland and Portugal show an increasing correlation from week 10 and onwards. The negative correlation is not very prominent in Denmark, Iceland, Norway and Greece after week 15 as compared to other countries.
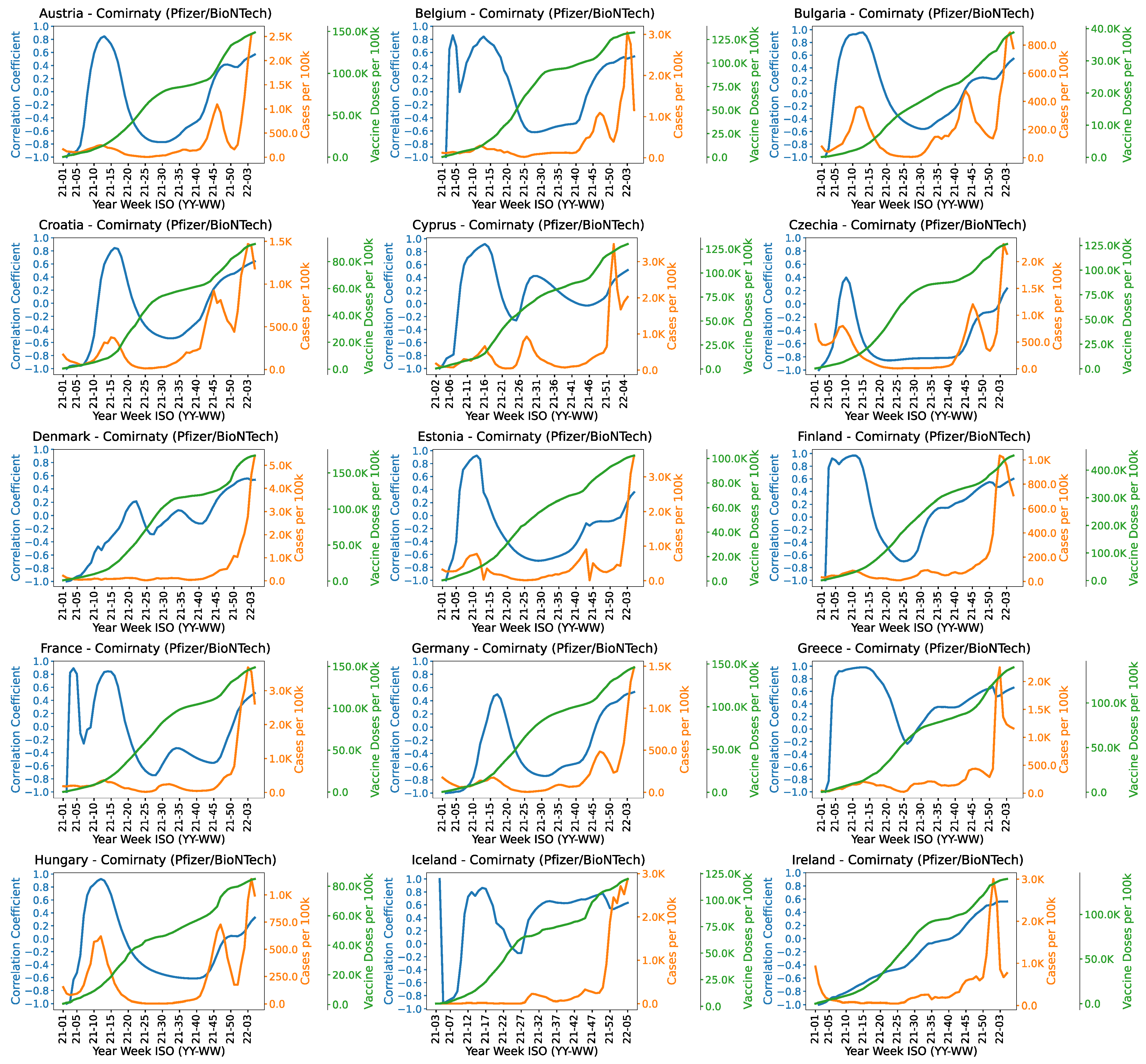
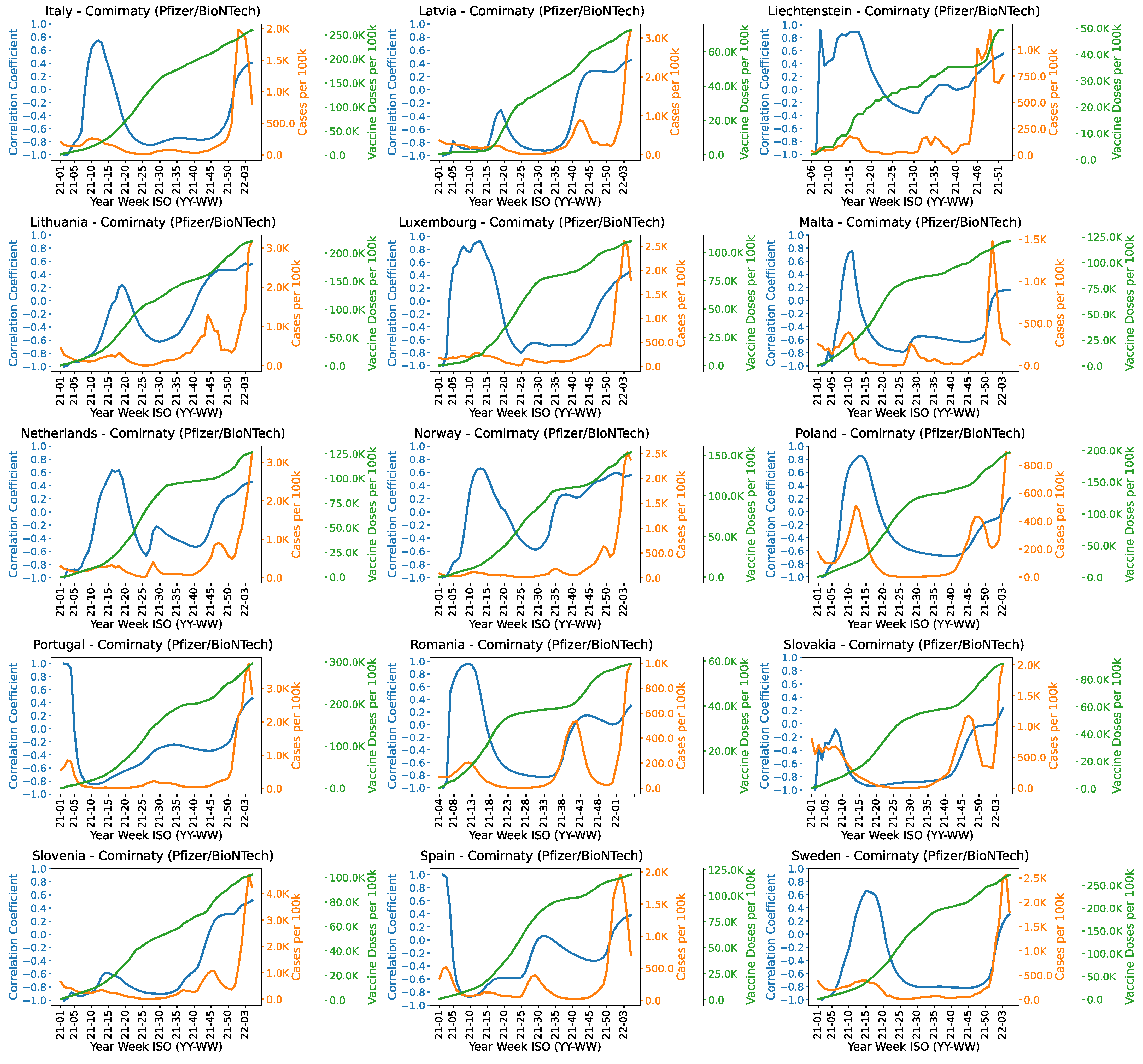
Figure A7 and
Figure A8 show the country-wise correlation between administered doses of Pfizer and COVID-19 cases. There are some uncommon trends in the correlation for some countries. For instance, Cyprus, Netherlands and Spain have a positive spike in the correlation around 26th week.
Figure A16 and
Figure A17 show the cases of Delta variant which emerged around 26th week. In Finland, Greece, Iceland, Norway and Liechtenstein, the correlation starts increasing around 25th week and it never shows a decreasing trend afterwards. It might be due to the emergence of Delta variant. Denmark, Ireland and Portugal show an increasing correlation throughout. Alpha and Delta variants were prevalent during those weeks in Denmark, Ireland and Portugal.
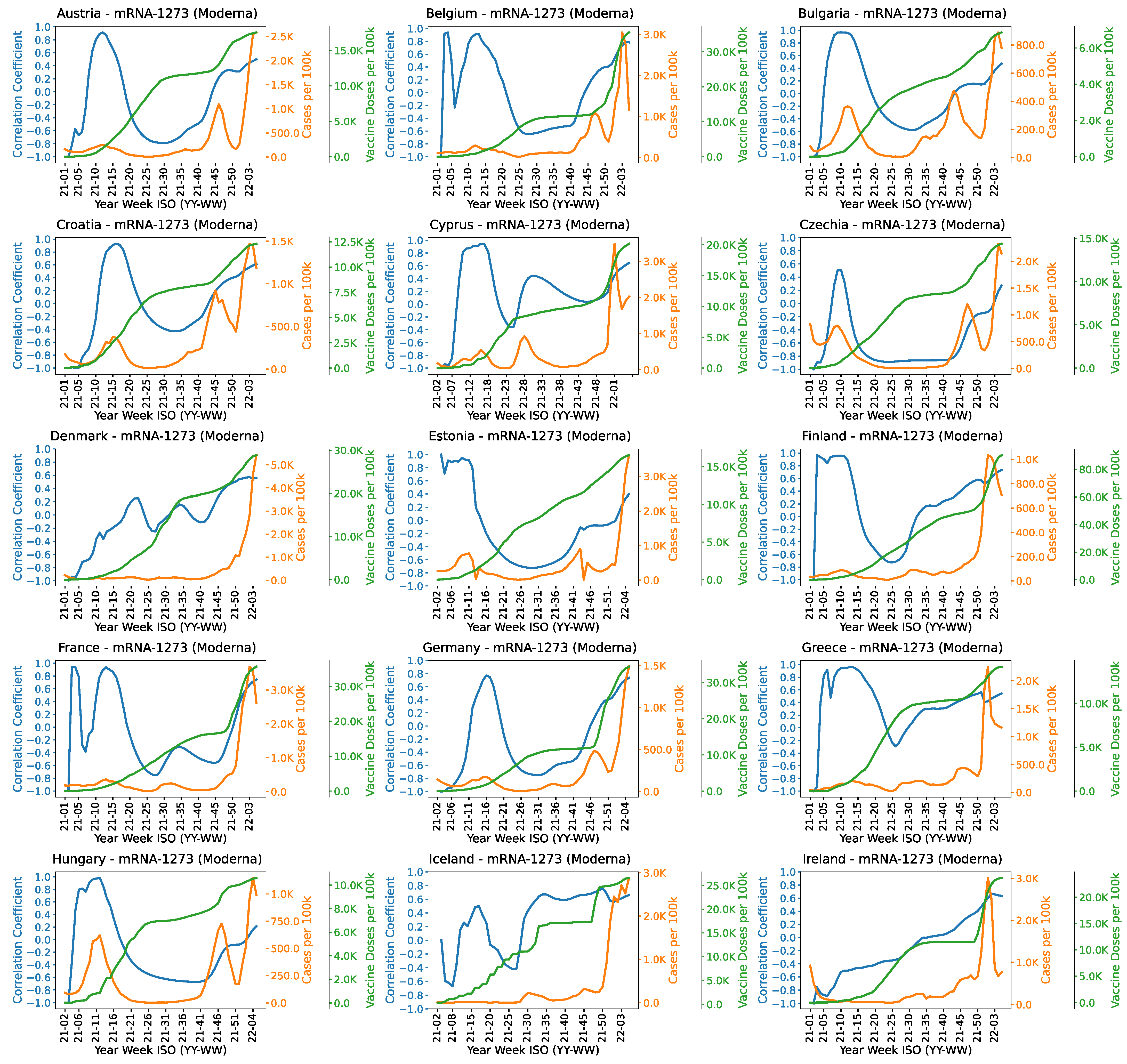
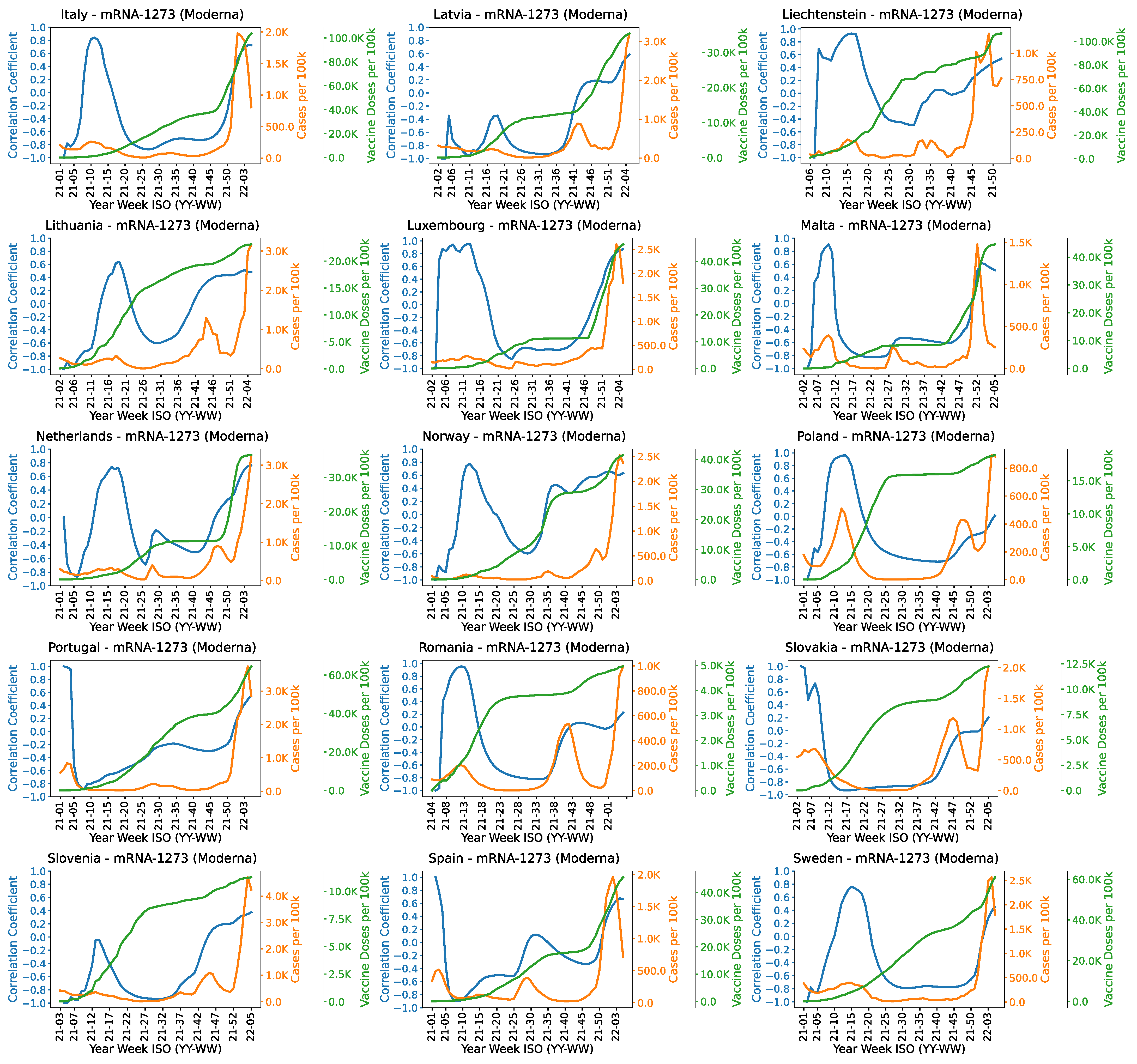
Figure A9 and
Figure A10 show the country-wise correlation between the administered doses of Moderna vaccine and COVID-19 cases. Ireland has a constantly increasing correlation. This trend for Ireland is similar for almost all types of vaccines. Ireland shows Alpha and other type of variant cases in initial weeks, Delta variant is prominent around mid-year and in the proceeding weeks it reflects the emergence of Omicron variant. Country-wise results of Janssen, Sputnik and unknown vaccines are available in the
Supplementary Files.
4.2.2. Correlation between the Total Doses of Different Vaccines and Weekly Deaths
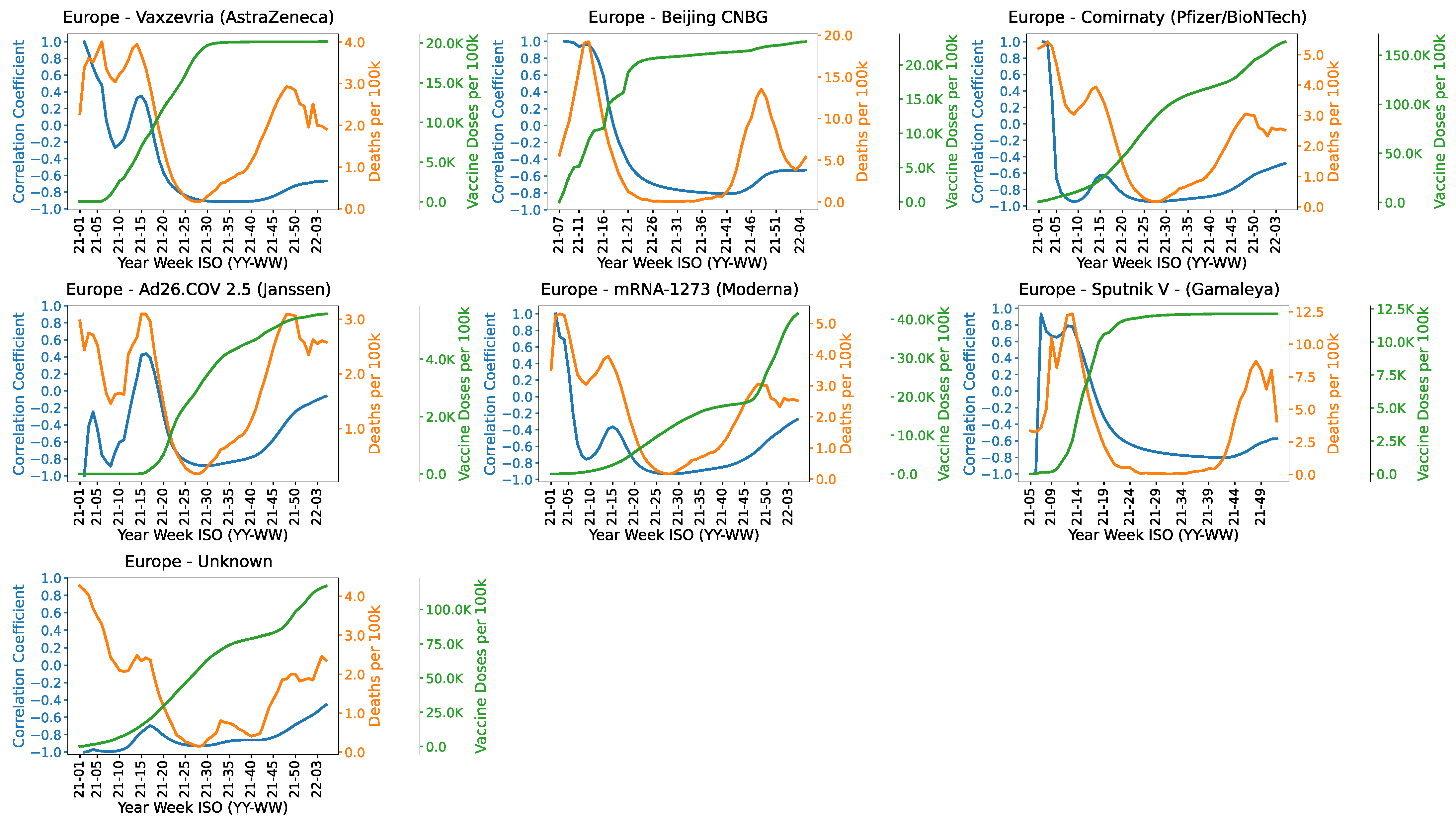
Figure 4 shows the correlation between administered doses of different COVID-19 vaccines and COVID-19 deaths. The correlation for AstraZeneca is highly negative from week 20 and onwards. Beijing’s CNBG (Sinopharm) vaccine was only administered in Hungary. The correlation trends reflect a significant impact of the vaccine against COVID-19 cases. The correlation of Pfizer vaccine is highly negative in most weeks. The correlation values of Janssen do not reflect a strong impact of the vaccine in reducing COVID-19 deaths. There is a spike in deaths from week 10 to 15. It might be due to Alpha variant which was prevalent during that time. The correlation starts increasing again after 40th week. It might be due to Delta variant which emerged after week 30 in most countries. The correlation trend for Moderna vaccine is similar to Janssen vaccine except the magnitude of the spike after the 10th week. The cases start rising again from the 40th week. The spike in the correlation might be due to the emergence of Alpha variant and some unknown variants in those weeks. The correlation values for Sputnik are steadily negative from week 25 to 40. The correlation starts increasing after 45th week which might be due to the Omicron variant.
4.3. Correlation Considering Different Age Groups
This Section provides a correlation analysis between the total number of administered doses in different age groups and weekly COVID-19 cases/deaths. We did not have access to the cases/deaths grouped into same age brackets as the number of administered doses. Therefore, we show the effect of vaccinating different age groups on overall weekly cases/deaths. In other words, cases/deaths represent the total number of weekly COVID-19 cases/deaths irrespective of the age groups.
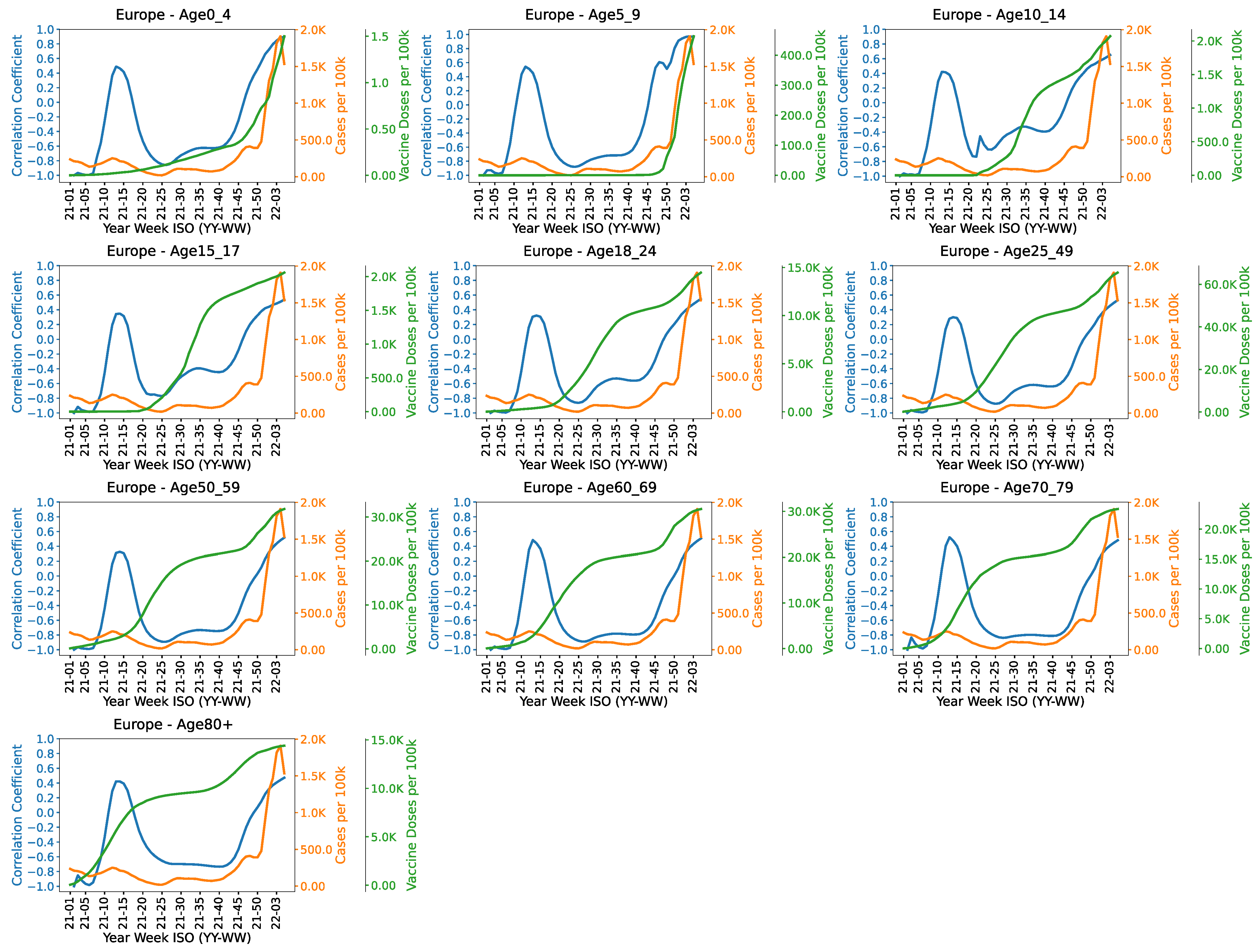
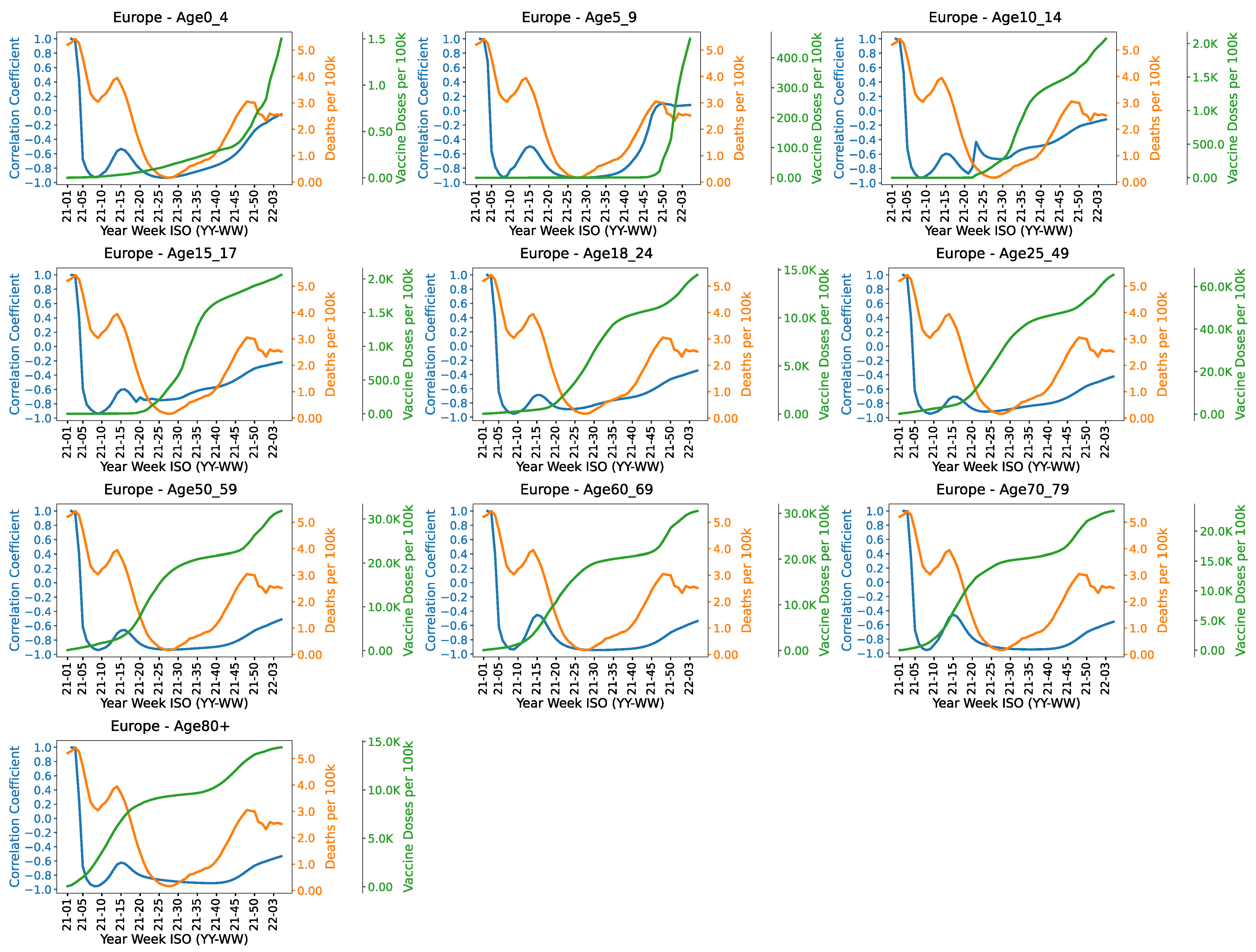
Overall results.Figure 5 shows the correlation between administered vaccine doses in different age groups and overall weekly cases. It can be observed that the vaccination rate for age groups <10 years has been quite slow up to week 45 as compared to the other age groups. Total weekly reported COVID-19 cases remain under control up to week 45. Afterwards, there is a sharp increase in cases which may be partly due to the prevalence of Omicron variant in those weeks. The correlation is highly negative from around week 20 to 40 in almost all age groups. It might be partly due to the relatively higher vaccination rate in age groups >10 years in these weeks.
Figure 6 shows the correlation between age-wise administered doses and weekly deaths. An increase in deaths after week 25 can be observed. This might be partly due to the prevalence of Delta variant in those weeks. The number of deaths increases further around week 45 which might be due to the emergence of Omicron variant. The correlation for older age groups is relatively more negative. It might be a reflection of the higher efficacy of vaccines in older age groups.
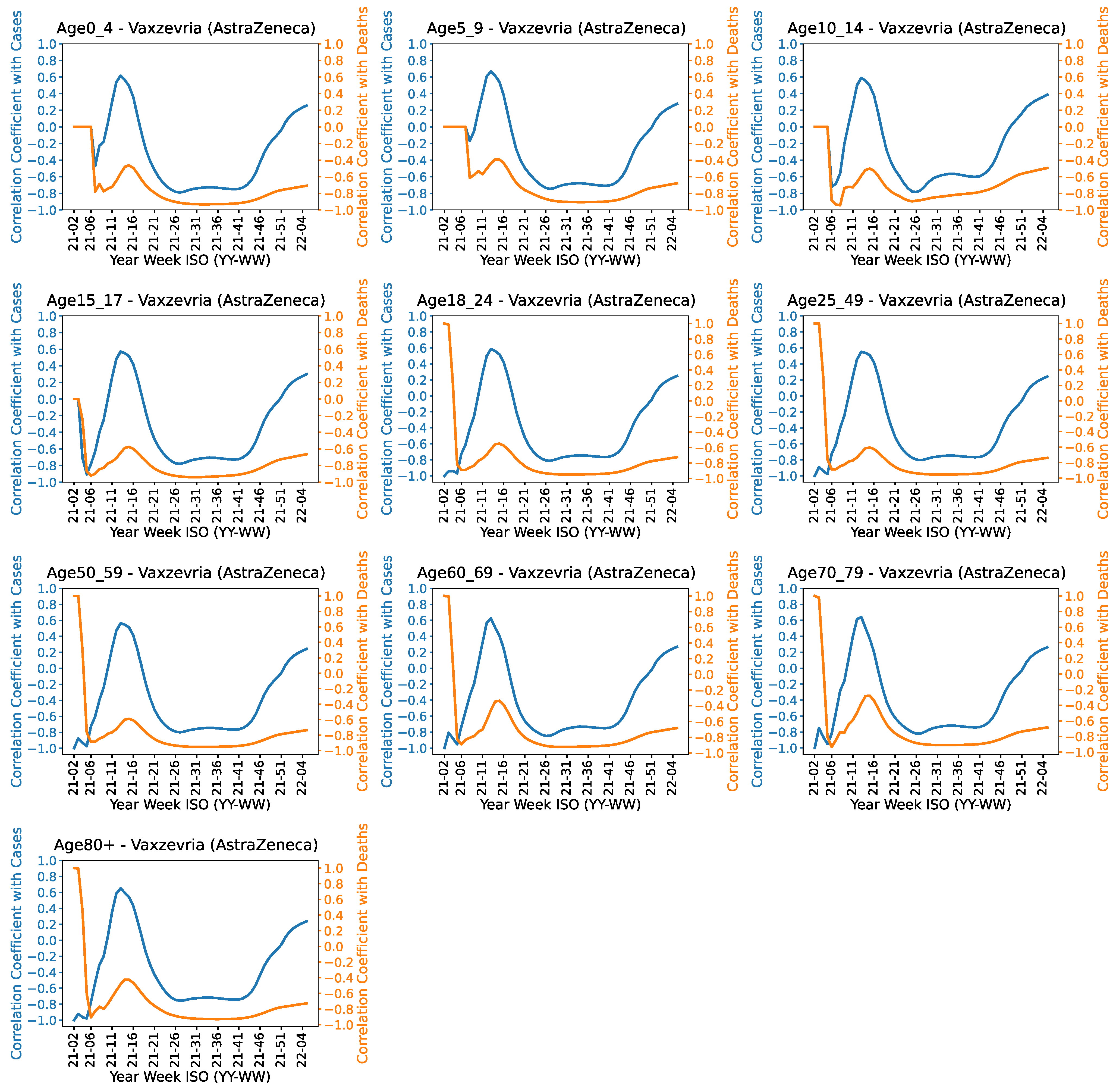
Results for different vaccines. We provide details of the correlation analysis between age-wise administered doses of different vaccines and COVID-19 cases/deaths. Figures showing the results for different age groups for some of the most widely used vaccines (AstraZenca, Pfizer and Moderna) are provided in
Appendix C. Figures for the other vaccines are given in the
Supplementary File.
Figure A11 shows the correlation trends for AstraZeneca for different age groups. It can be observed from the graphs that the correlation has a positive spike from week 10 to 15. The negative correlation starts decreasing after the 40th week which is potentially due to the Omicron variant. It can be observed from
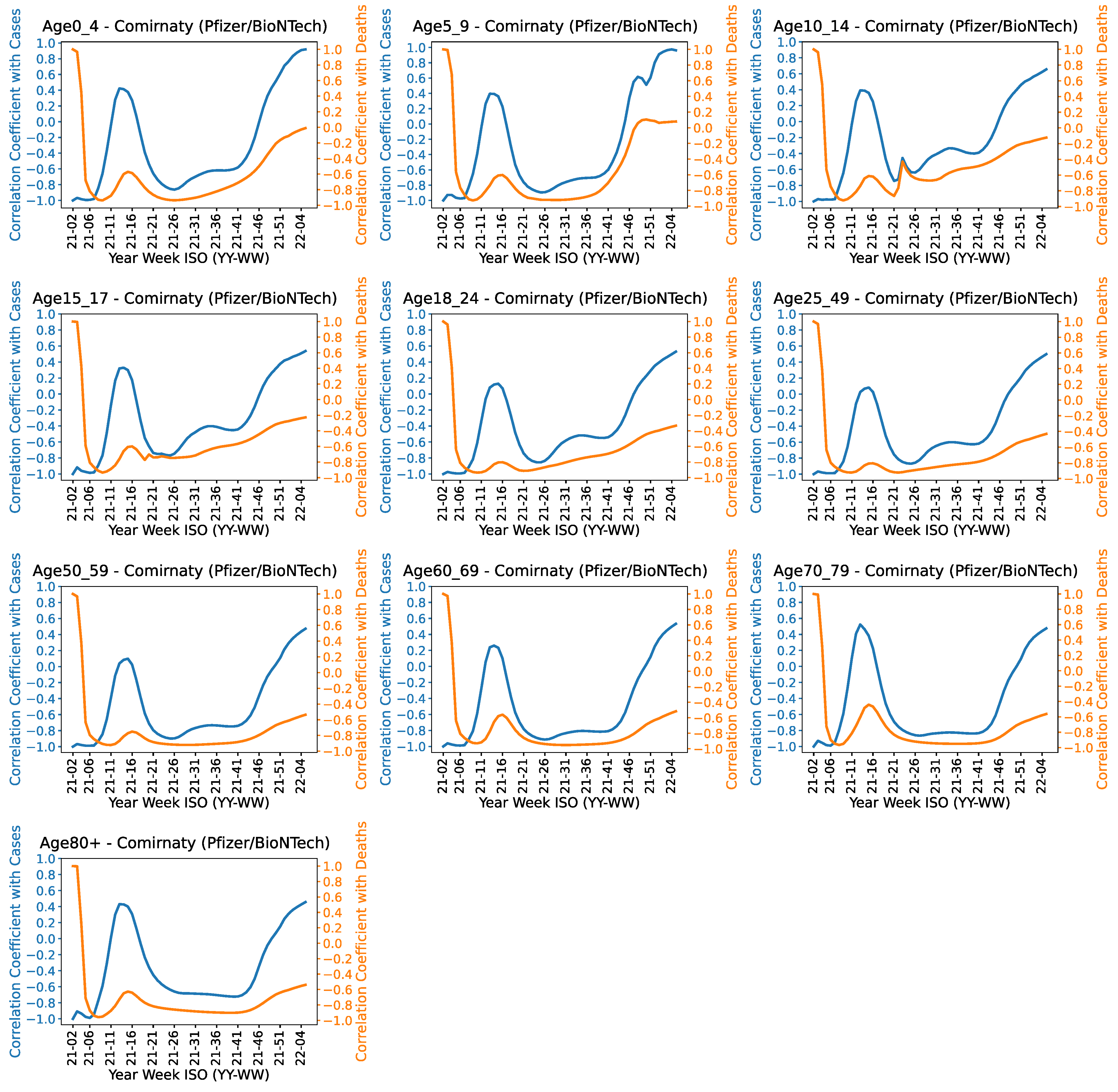
Figure A12 that Pfizer vaccine shows a positive spike in the correlation with COVID-19 cases and deaths from week 5 to 20. This behavior is less prominent in age groups <60 years. The correlation remains highly negative from week 20 to 40. This trend is relatively more eminent in age groups >60 years. The negative correlation starts decreasing after 40th week for all age groups. The impact of vaccine against COVID-19 mortality reduces significantly after the 40th week for age groups <10 years.
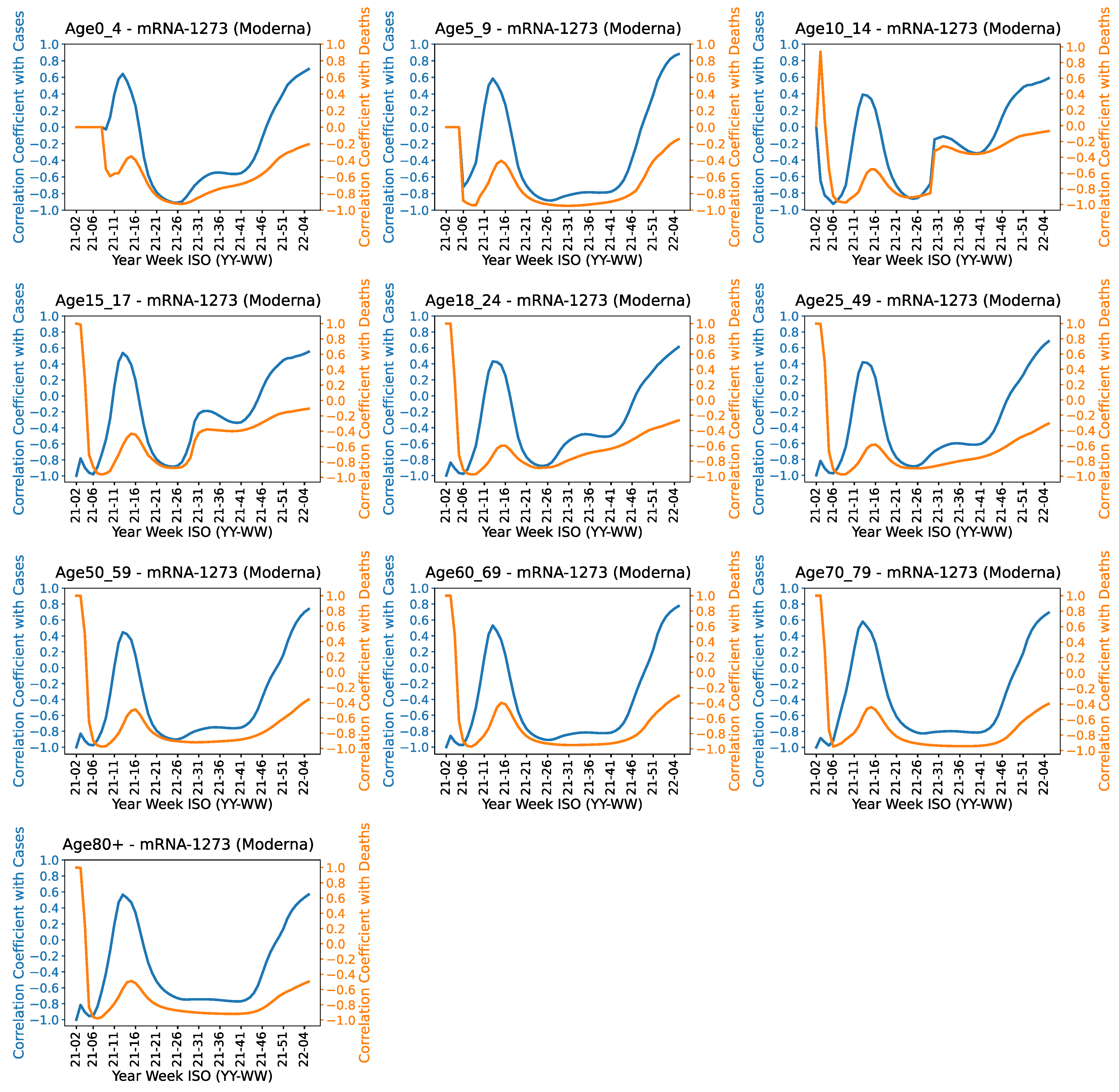
Figure A13 shows the correlation results for Moderna. It shows a relatively more steady correlation in older age groups between the 20th and 40th weeks.
The age-wise correlation curves of Janssen, Sputnik, Sinopharm and unknown vaccines are provided in the
Supplementary File. The correlation of Janssen vaccine is almost similar in all age groups. Sputnik shows a relatively more steady correlation in older age groups between the 20th and 40th weeks. The correlation of Sinopharm vaccine is almost similar in all age groups. The correlation is relatively less negative in age groups >60 years. It might be an indication of the low impact of Sinopharm vaccine in age groups >60 years.
4.4. Correlation Considering Different COVID-19 Variants
This Section provides the correlation between the total administered COVID-19 vaccine doses and weekly cases of different COVID-19 variants. The number of weekly cases for each variant is estimated using the results from the sequenced COVID-19 cases. Specifically, we use the results of sequenced COVID-19 cases and scale the results to the total population to compute cases per 100k for each variant based on their ratio in the sequenced cases. The data for deaths caused by different variants was not available; therefore, we only show the correlation study for weekly cases for different variants.
4.4.1. Overall Results
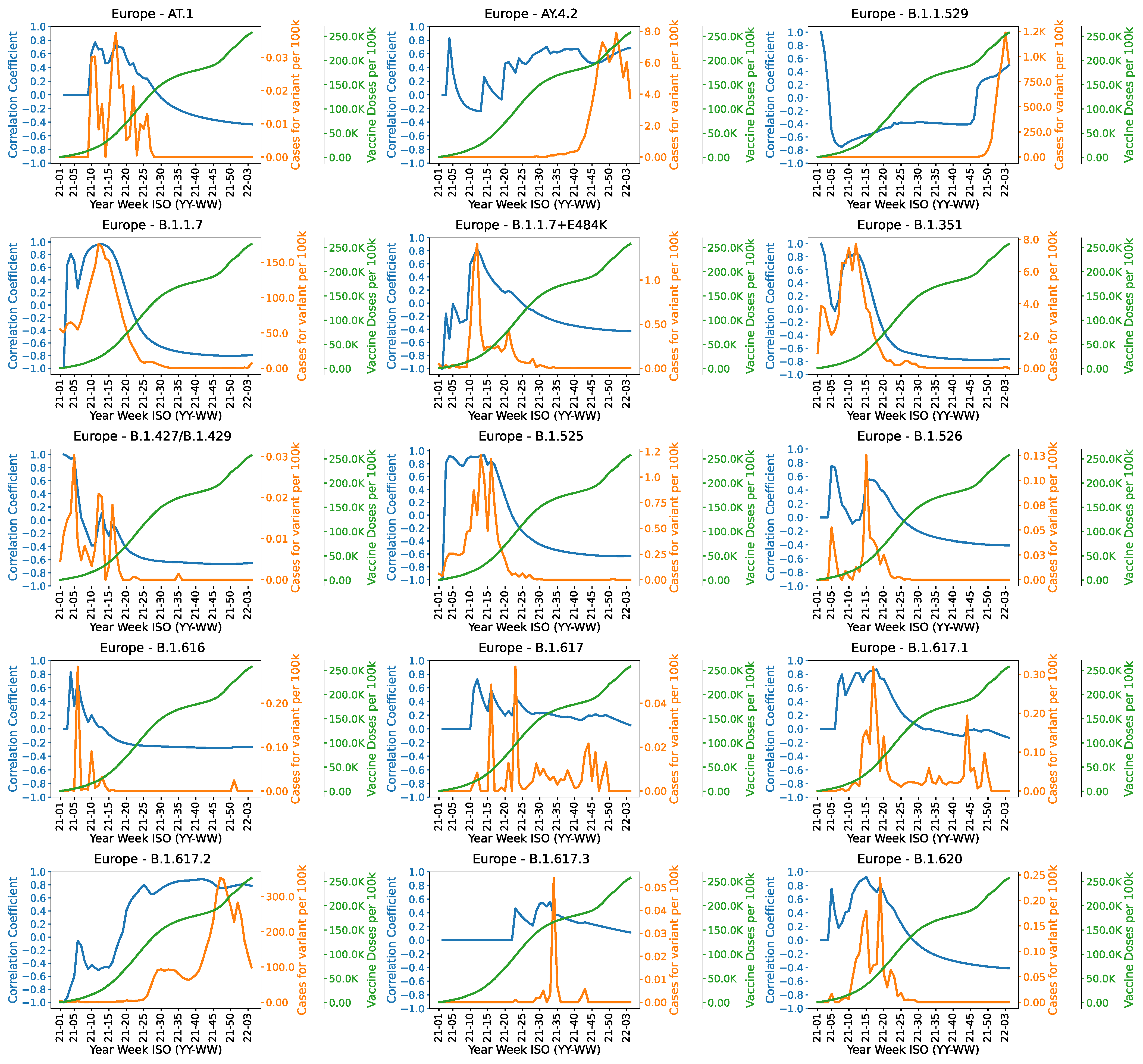
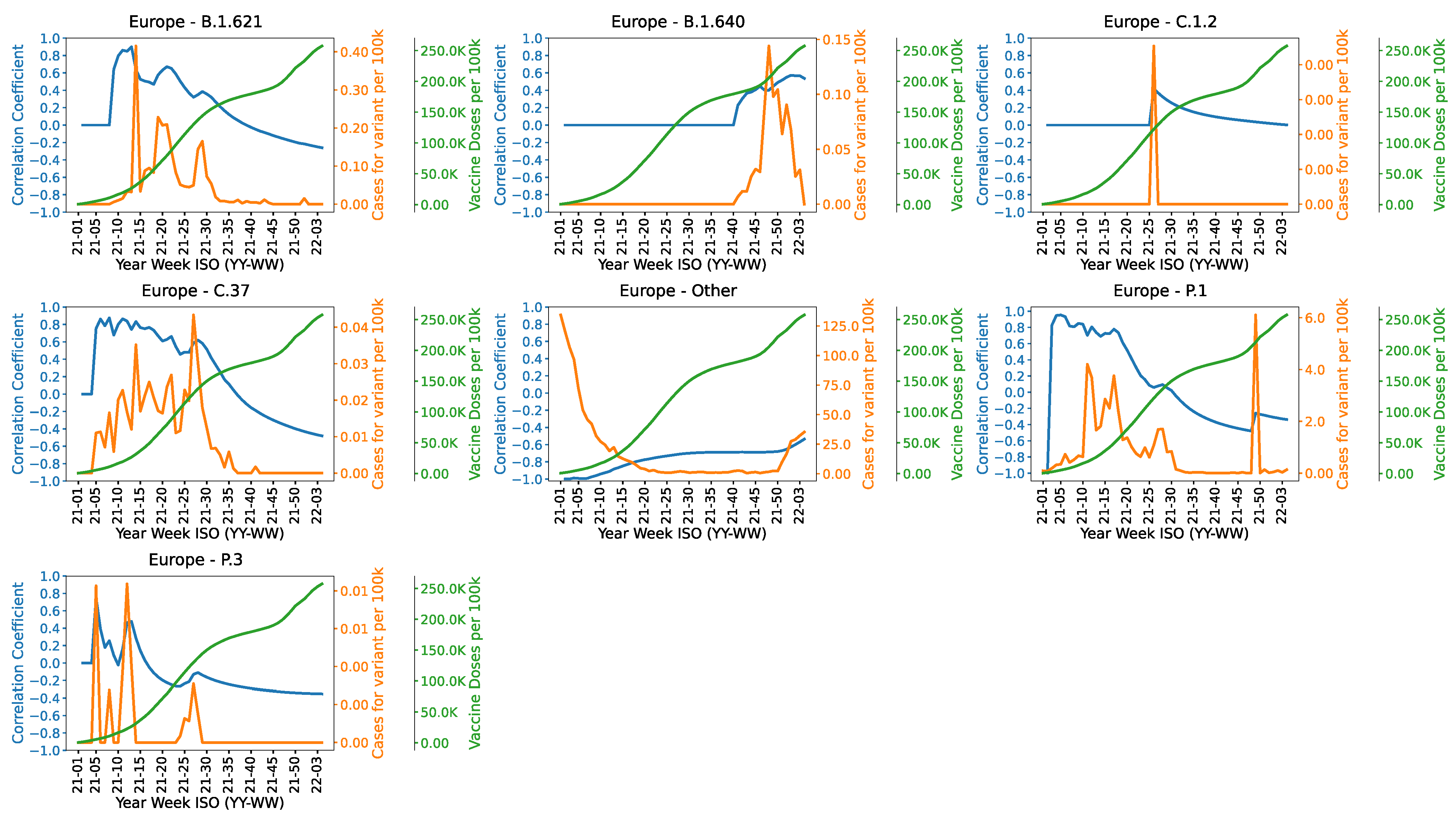
Figure 7 and
Figure 8 show the correlation trends of different COVID-19 variants in Europe considering all countries mentioned in
Table 1. The graphs also show the emergence of different variants. For instance, Omicron variant (B.1.1.529) is prevalent after week 45 and Delta variant (B.1.617.2) is prevalent from week 20 to week 50. The graphs also show how the correlation changes with time with the increasing number of vaccine doses. For instance, the correlation of Alpha variant (B.1.1.7) changes from high positive to high negative with the increasing number of administered vaccines. The correlation of Gamma variant (P.1) remains positive until week 30. The correlation for Delta variant is negative until week 20 and afterwards it moves to high positive values. The correlation of Omicron shows a peak in the 45th week.
4.4.2. Country-Wise Results
European Centre for Disease Prevention and Control (ECDC) regularly assesses evidence on variants detected through epidemic intelligence or other scientific sources. The variant that are relatively more harmful are categorized as Variants of Concern (VoC). For VoC, clear evidence is available indicating a significant impact on their high transmission rate and severity that is likely to have an impact on the epidemiological situation in the European Economic Area (EU/EEA). The latest list of Variants of Concern as of 3 February 2022 includes Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2) and Omicron (B.1.1.529) variants [
34]. However, according to World Health Organization (WHO), Alpha variant is also included in the VoC [
35]. In this section, we discuss correlation results for the variant of concerns. Figures showing country-wise results for the most prevalent variants (Alpha, Delta and Omicron) are presented in
Appendix D. Figures for the other variants can be found in the
Supplementary File.
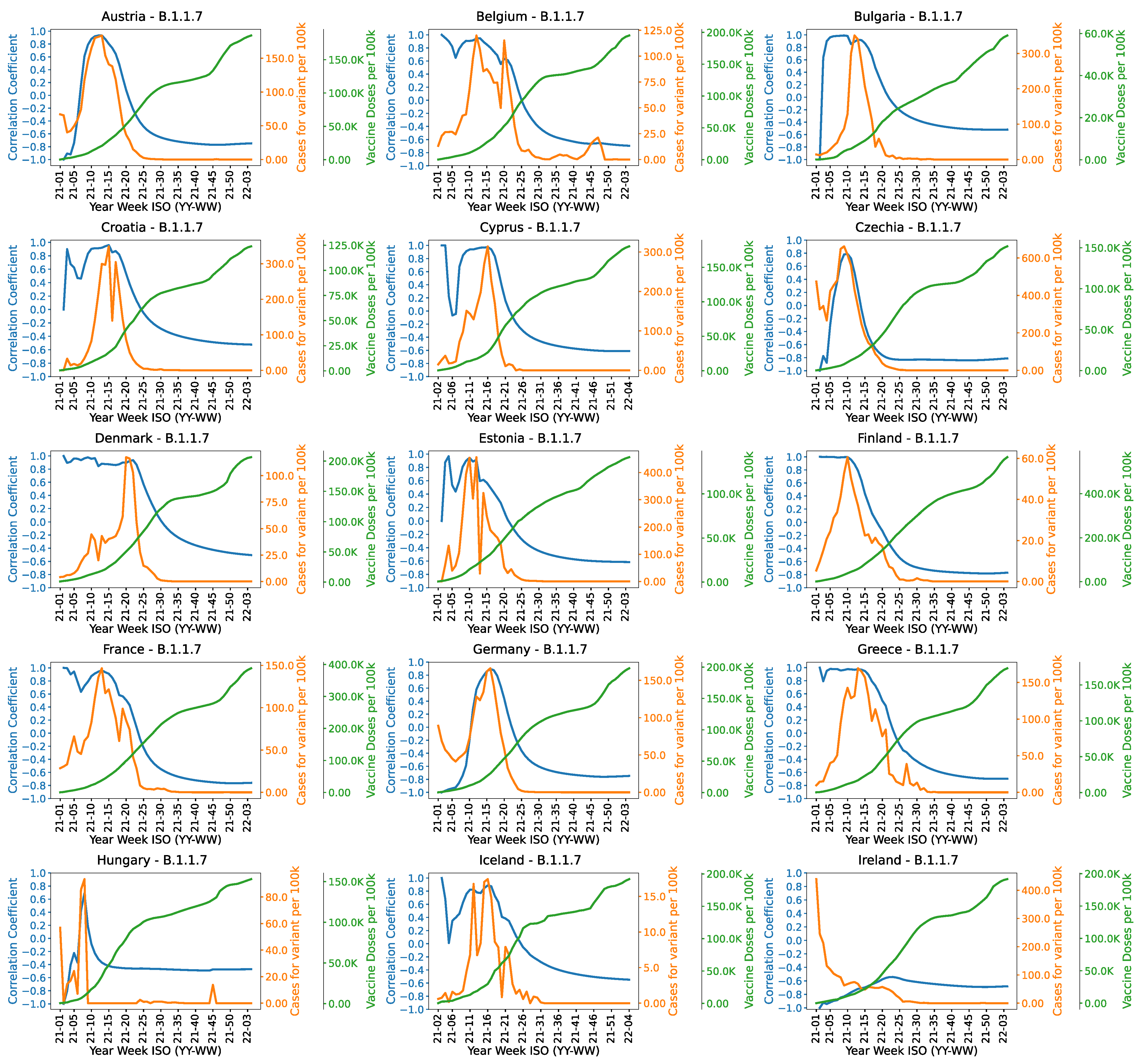
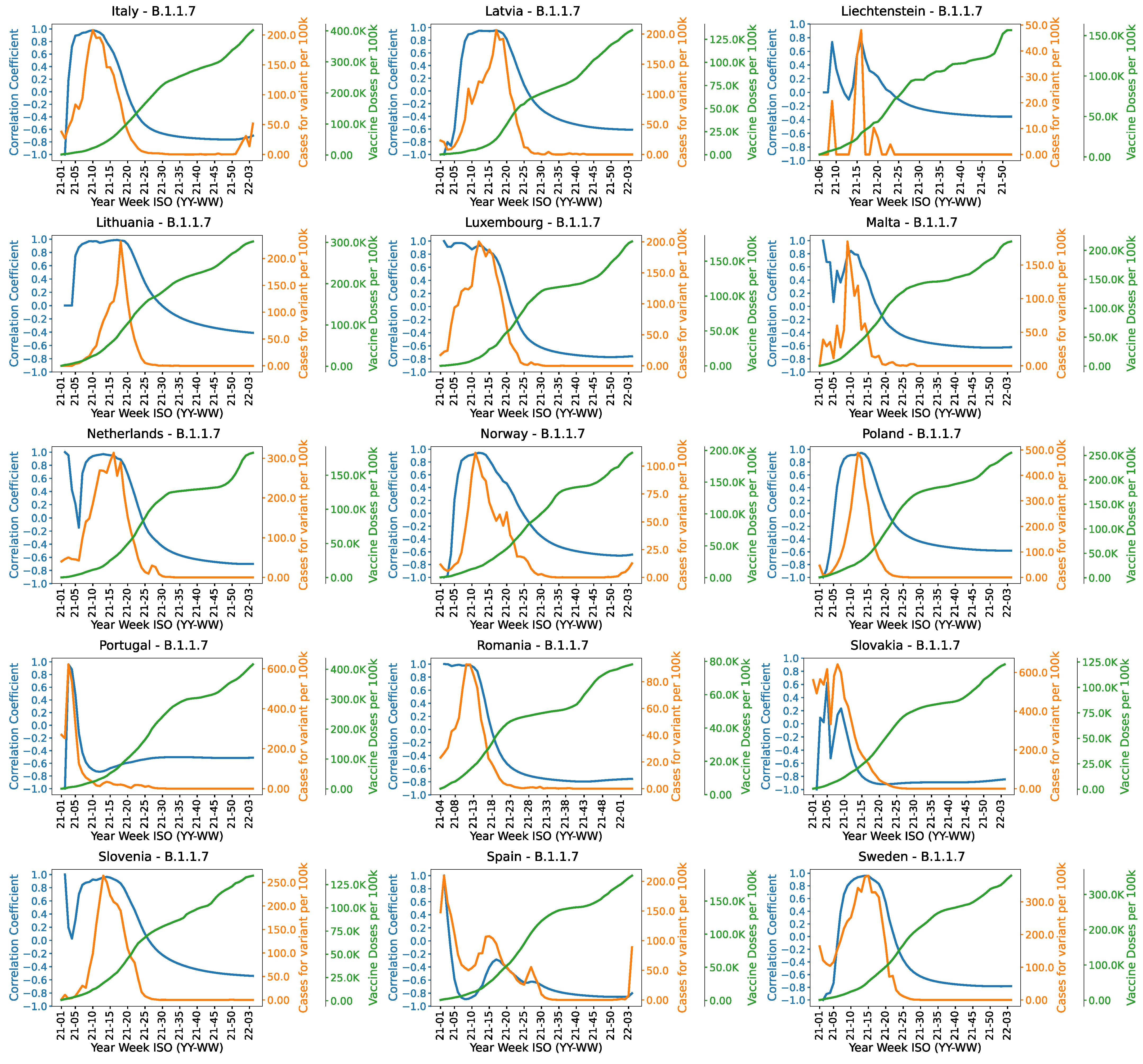
Country-wise correlation between the vaccination rate and cases of Alpha variant are shown in
Figure A14 and
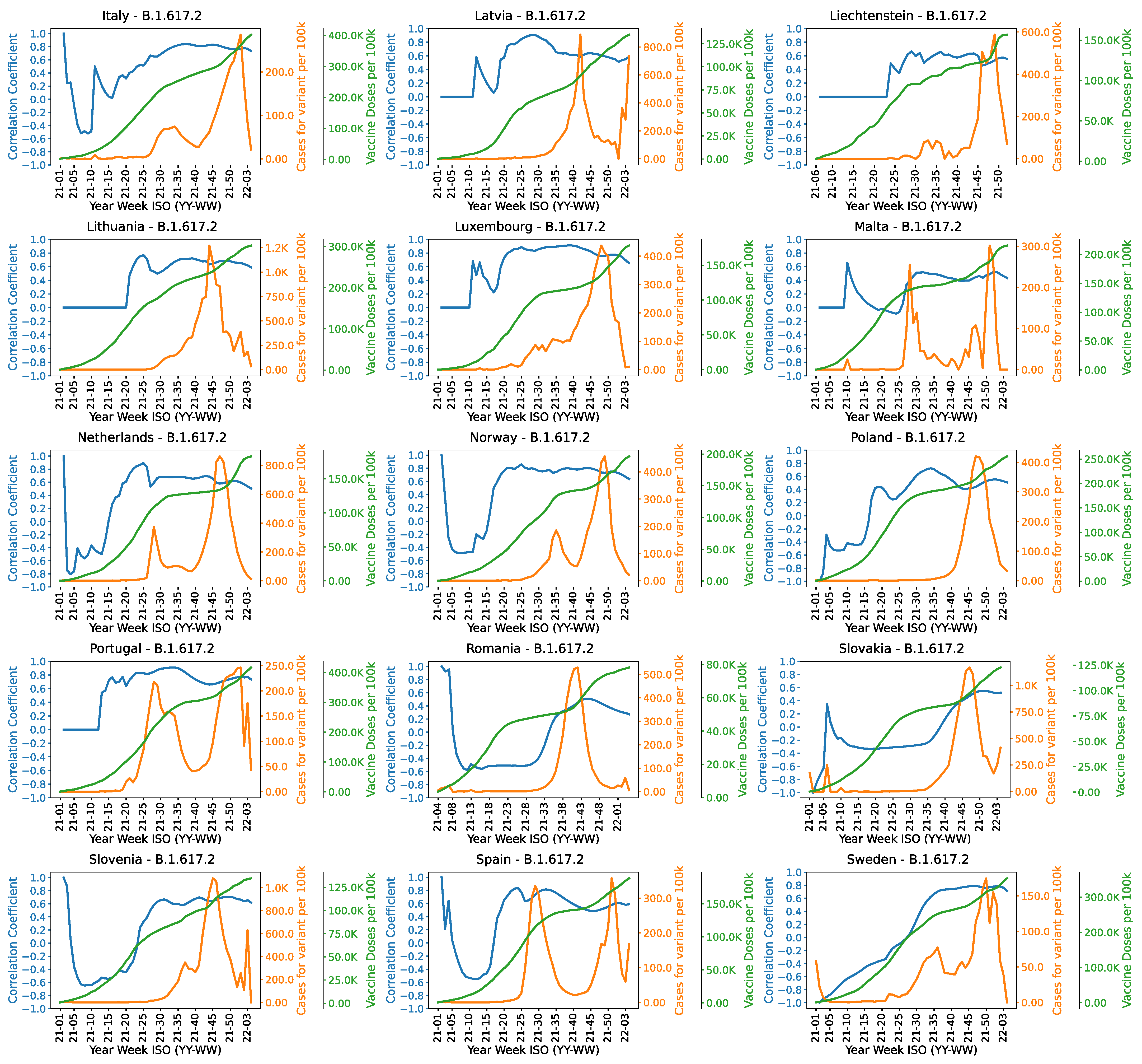
Figure A15. Almost all countries are exposed to this variant. The correlation remains highly positive from week 1 to 25. Cases of the variant starts decreasing after week 25 in all countries except Hungary and Liechtenstein. The correlation trends of Delta variant for different countries are shown in
Figure A16 and
Figure A17. It can be observed from the Figure that almost all countries have higher number of COVID-19 cases from week 20 to 50. The cases start decreasing after 50th week indicating the suppression of the variant.
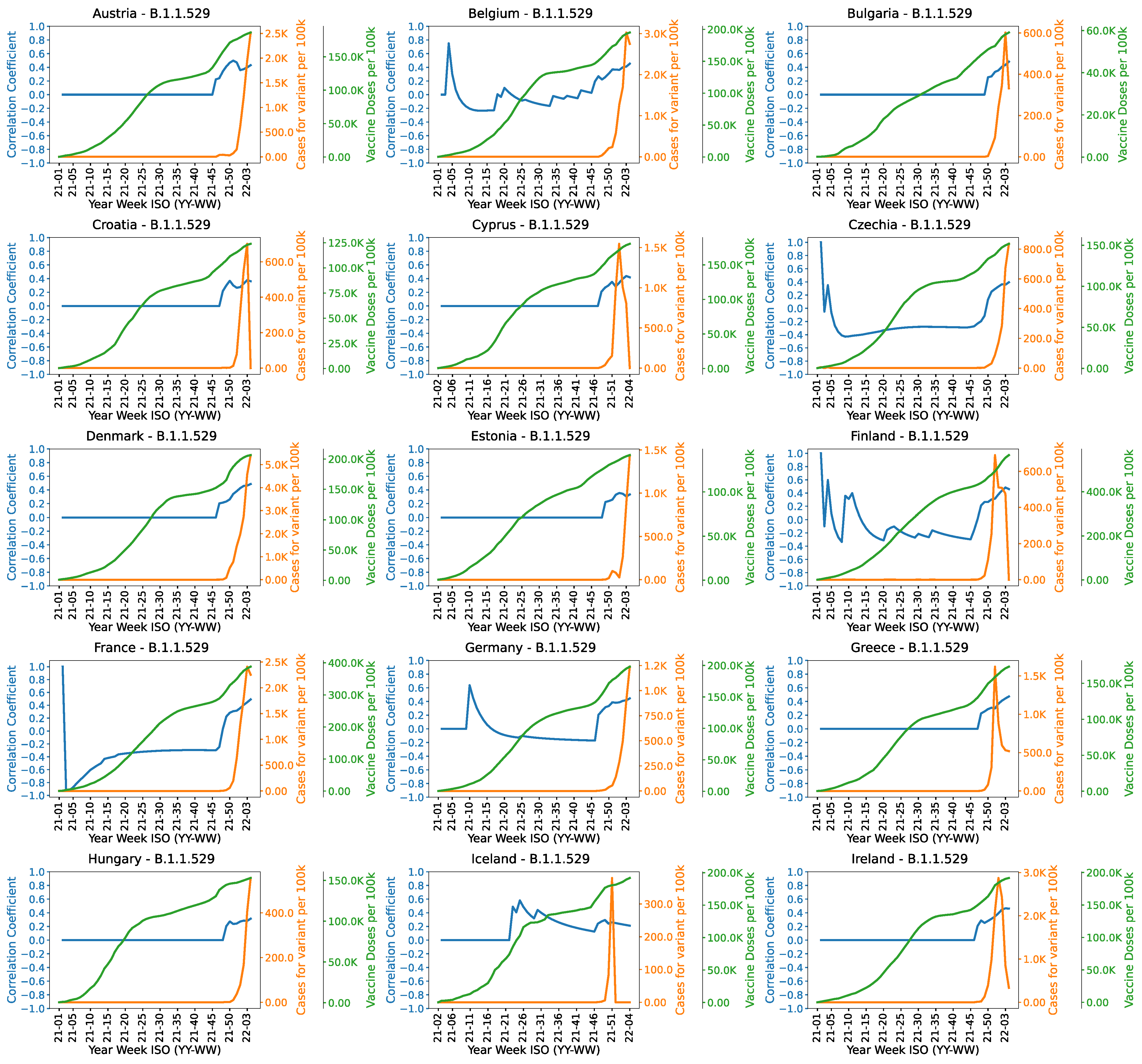
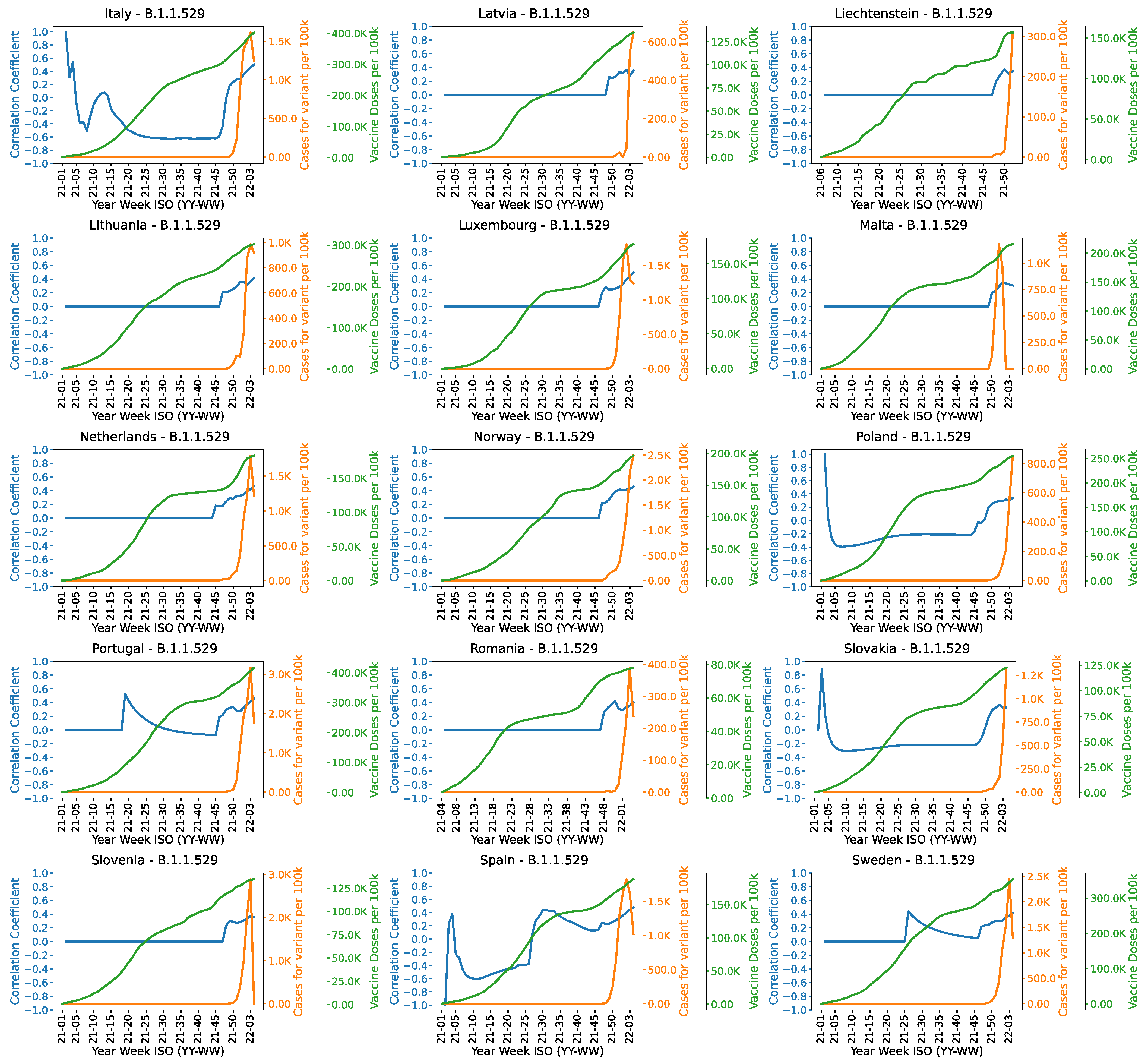
Figure A18 and
Figure A19 show the correlation trends of Omicron variant (B.1.1.529). It can observed from the Figure that the variant emerged after 45th week. The increasing correlation after week 45 shows that with the increase in vaccination rate, the cases are still increasing. It might be an indication of the inefficacy of vaccines on Omicron.
The correlation trends of Beta variant (B.1.351) are provided in the
Supplementary File. It shows that the correlation remains consistently negative. It might be the reflection of the high effectiveness of vaccine. The negative correlation is less significant in Cyprus, Bulgaria and Iceland. Correlation graphs of Gamma variant are also available in the
Supplementary File. It shows a decreasing correlation which is an indication of the suppression of the variant which may be due to the high effectiveness of vaccines. This trend is more prominent in Netherlands, Spain, Sweden, Portugal, Ireland and Italy.

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}