
Estimates of the COVID-19 Infection Fatality Rate for 48 African Countries: A Model-Based Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Data Sources
2.2. Assumptions
2.3. Statistical Model
- Y = dependent variable
- X = the matrix of independent variable
- β = vector of regression model parameters
- σ2 = Standard deviation
- μ = prior mean μ
- Λ = prior precision matrix
- k = number of regression coefficients
- V = prior hyperparameter values
2.4. Spatial Analysis
3. Results
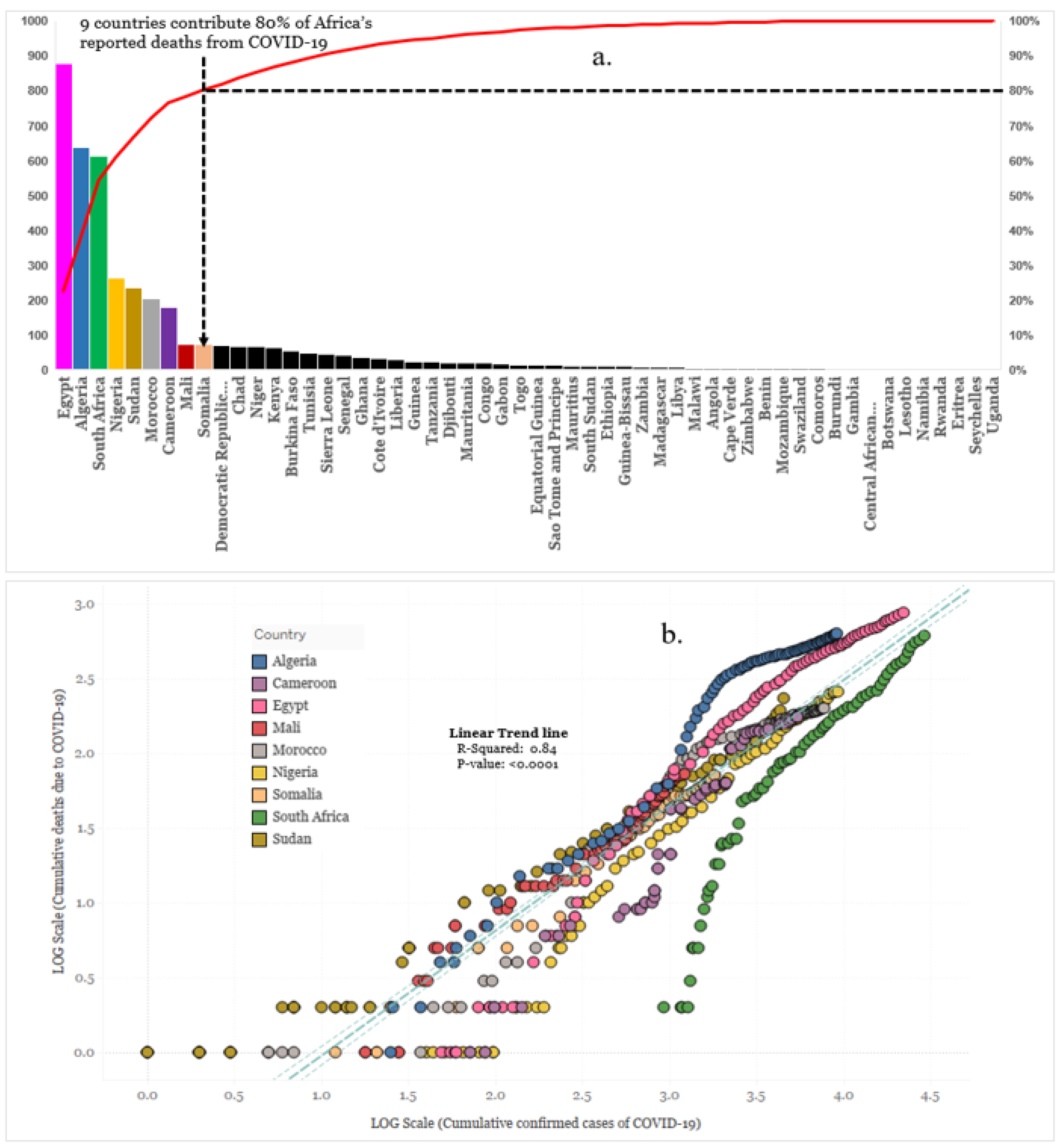
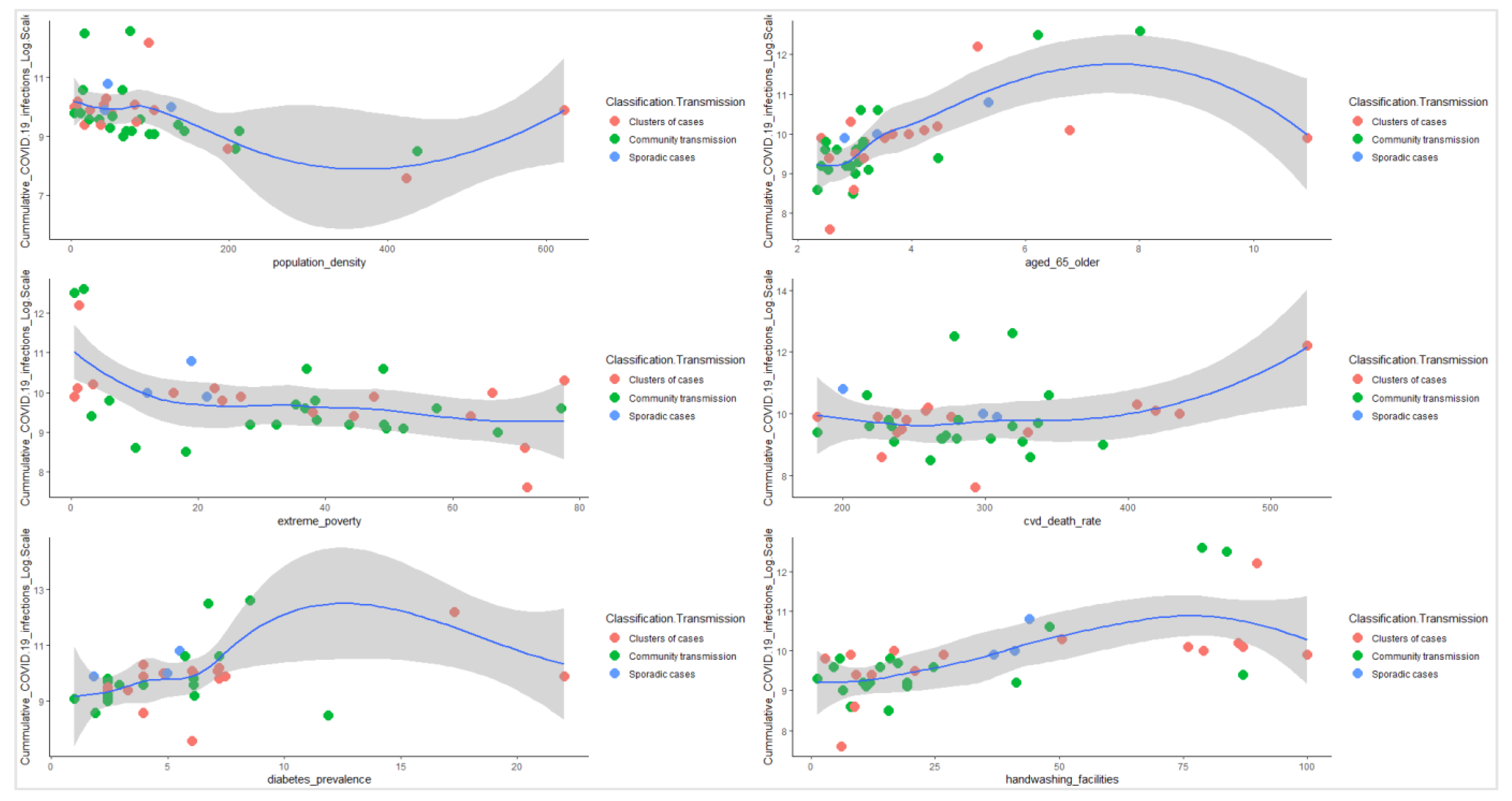
3.1. Descriptive Analysis
3.1.1. Bayesian Regression Model
3.1.2. Bayesian Prediction Model
3.1.3. Estimated Infection Fatality Rate by Country
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Sensitivity Analysis of the Infection Fatality Rates of the Posterior Summary Statistics, 30 May 2020

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Posterior Summary Statistics | Mean | Maximum | ||||
|---|---|---|---|---|---|---|
| 75% Cred. Interval | 90% Cred. Interval | 95% Cred. Interval | 75% Cred. Interval | 90% Cred. Interval | 95% Cred. Interval | |
| Cumulative COVID-19 Infections Estimated (as of 30 May 2020) | 47,366 [44,565, 50,167] | 56,839 [54,038, 59,640] | 63,154 [60,353, 65,955] | 1,265,159 [1,262,358, 1,267,960] | 1,518,191 [1,515,390, 1,520,992] | 1,686,879 [1,684,078, 1,689,680] |
| Calculated IFR (as of 30 May 2020) | 8.28% | 6.90% | 6.21% | 0.31% | 0.26% | 0.23% |
| Total Number of Infections Per confirmed Case (as of 30 May 2020) | 0.35 | 0.42 | 0.47 | 9.36 | 11.24 | 12.48 |
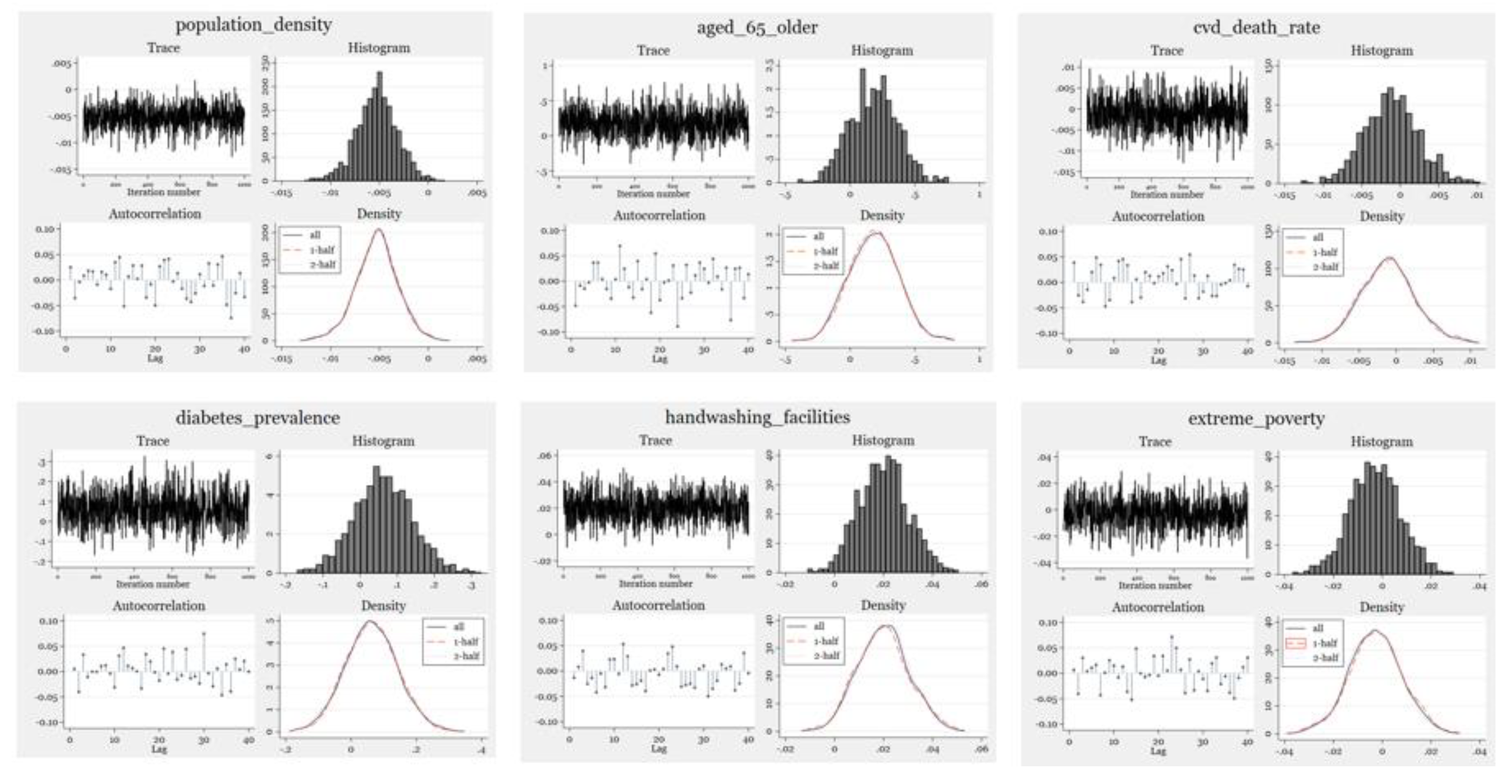
Appendix A.2. Posterior Predictive Checks for Convergence Across All Model Parameters

Appendix A.3. Posterior Predictive Summary for Test Statistics
| Posterior Predictive Summary | MCMC Sample Size = 1000 | |||||
|---|---|---|---|---|---|---|
| T | Mean | Std. Dev. | E(T_Obs) | P(T ≥ T_Obs) | ||
| Mean | 6.749488 | 0.3085233 | 6.775585 | 0.462 | ||
| Min | 2.818528 | 1.005077 | 3.218876 | 0.389 | ||
| Max | 10.89979 | 1.062004 | 10.28329 | 0.694 | ||
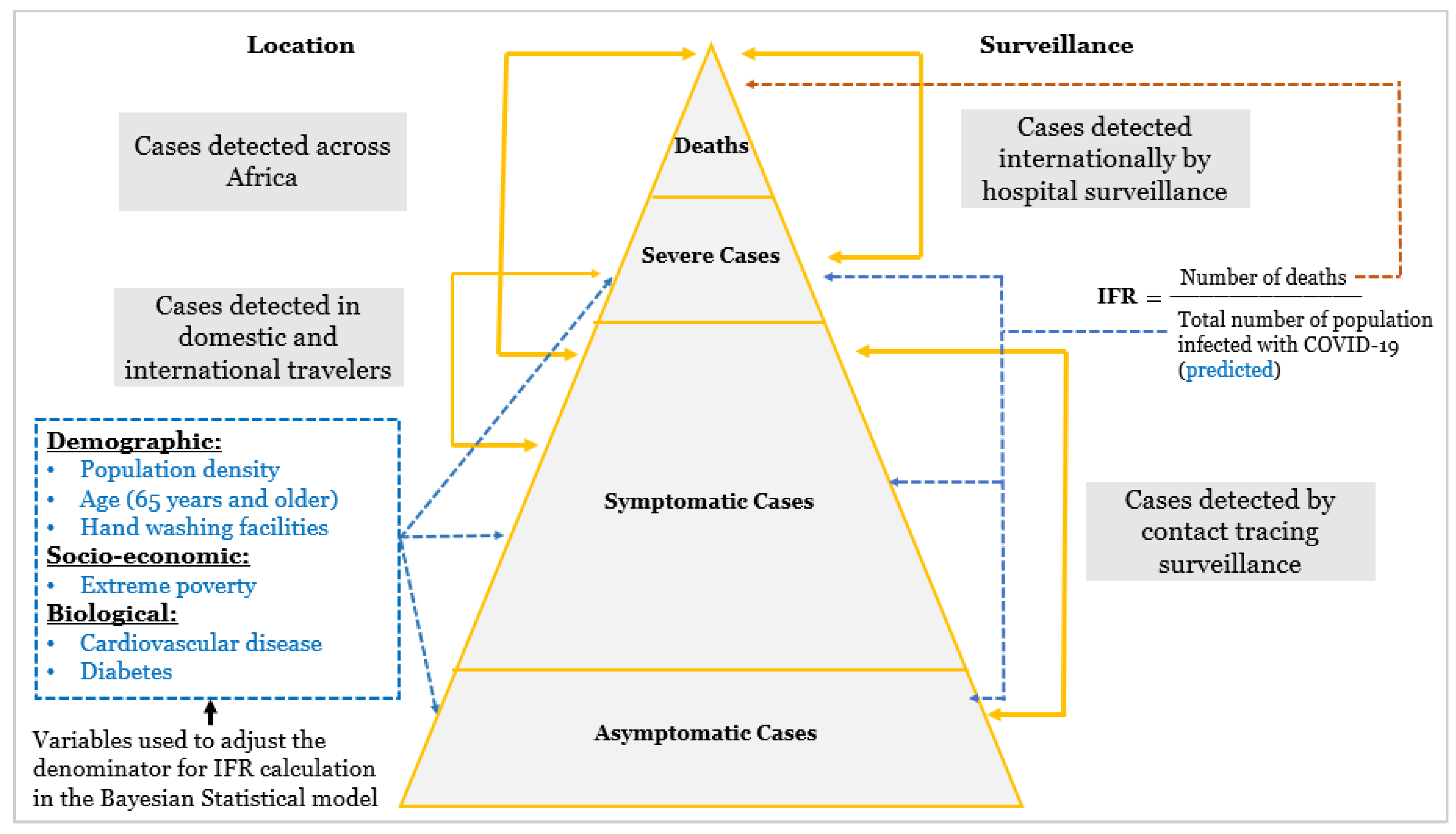
Appendix A.4. WHO COVID-19 Transmission Classification Type
References
- World Health Organization. Available online: https://www.covid19.who.int/ (accessed on 30 May 2021).
- World Health Organization. (n.d.) Coronavirus. World Health Organization. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 30 May 2021).
- World Health Organization. (n.d.) Severe Acute Respiratory Syndrome (Sars). World Health Organization. Available online: https://www.who.int/health-topics/severe-acute-respiratory-syndrome#tab=tab_1 (accessed on 31 August 2021).
- Garske, T.; Legrand, J.; Donnelly, C.A.; Ward, H.; Cauchemez, S.; Fraser, C.; Ferguson, N.M.; Ghani, A.C. Assessing the severity of the novel influenza A/H1N1 pandemic. BMJ 2009, 339, b2840. [Google Scholar] [CrossRef] [PubMed]
- Lipsitch, M.; Donnelly, C.A.; Fraser, C.; Blake, I.M.; Cori, A.; Dorigatti, I.; Ferguson, N.M.; Garske, T.; Mills, H.L.; Riley, H.; et al. Potential biases in estimating absolute and relative case-fatality risks during outbreaks. PLoS Negl. Trop. Dis. 2015, 9, e0003846. [Google Scholar] [CrossRef] [Green Version]
- Eubank, S.; Eckstrand, I.; Lewis, B.; Venkatramanan, S.; Marathe, M.; Barrett, C.L. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand 2020: Comparison of effects of strategies for mitigation and for suppression. Bull. Math. Biol. 2020, 82, 1–7. [Google Scholar]
- Forecasting COVID-19 Impact on Hospital Bed-Days, ICU-Days. (n.d.) Available online: http://www.healthdata.org/sites/default/files/files/research_articles/2020/covid_paper_MEDRXIV-2020-043752v1-Murray.pdf (accessed on 26 July 2020).
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.W.; Yip, C.C.Y.; To, K.K.W.; Tang, T.H.C.; Wong, S.C.Y.; Leung, K.H.; Fung, A.Y.F.; Ng, A.C.K.; ZoU, Z.; Tsoi, H.; et al. Improved molecular diagnosis of COVID-19 by the novel, highly sensitive and specific COVID-19-RdRp/Hel real-time reverse transcription-PCR assay validated In Vitro and with clinical specimens. J. Clin. Microbiol. 2020, 58, e00310-20. [Google Scholar] [CrossRef] [Green Version]
- Ng, Y.; Li, Z.; Chua, Y.X.; Chaw, W.L.; Zhao, Z.; Er, B.; Pung, R.; Chiew, C.J.; Lye, D.C.; Heng, D.; et al. Evaluation of the effectiveness of surveillance and containment measures for the first 100 patients with COVID-19 in Singapore—January 2–February 29, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 307. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (n.d.) Estimating mortality from COVID-19: SCIENTIFIC Brief. World Health Organization. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Sci-Brief-Mortality-2020.1 (accessed on 4 August 2020).
- Ghani, A.C.; Donnelly, C.A.; Cox, D.R.; Griffin, J.T.; Fraser, C.; Lam, T.H.; Ho, L.M.; Chan, W.S.; Anderson, R.M.; Hedley, A.J.; et al. Methods for estimating the case fatality ratio for a novel, emerging infectious disease. Am. J. Epidemiol. 2005, 162, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Perez-Saez, J.; Lauer, S.A.; Kaiser, L.; Regard, S.; Delaporte, E.; Guessous, I.; Stringhini, S.; Azman, A.S. Serology-Informed Estimates of SARS-CoV-2 Infection Fatality Risk in Geneva, Switzerland. Lancet Infect. Dis. 2021, 21, e69–e70. [Google Scholar] [CrossRef]
- Gao, X.; Dong, Q. A primer on Bayesian estimation of prevalence of COVID-19 patient outcomes. JAMIA Open 2020, 3, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, C. COVID-19 Infection Fatality Rate Associated with Incidence-A Population-Level Analysis of 19 Spanish Autonomous Communities. Biology 2020, 9, 128. [Google Scholar] [CrossRef]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; Bogan, A.; et al. COVID-19 Antibody Seroprevalence in Santa Clara County, California. Int. J. Epidemiol. 2021, 50, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Cook, R.C. World population prospects—Population division. Ohio St. LJ 1966, 27, 634. [Google Scholar]
- Ioannidis, J.P. Infection fatality rate of COVID-19 inferred from seroprevalence data. Bull. World Health Organ. 2021, 99, 19. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.; Tran, A.B.; Reinhard, B.; Ulmanu, M. US deaths soared in early weeks of pandemic, far exceeding number attributed to COVID-19. Anchorage Daily News. Available online: www.adn.com/nation-world/2020/04/27/us-deaths-soared-in-early-weeks-of-pandemic-far-exceeding-number-attributed-to-covid-19/ (accessed on 27 April 2020).
- Bayesian Data Analysis. Routledge & CRC Press. Available online: www.routledge.com/Bayesian-Data-Analysis/Gelman-Carlin-Stern-Dunson-Vehtari-Rubin/p/book/9781439840955 (accessed on 26 July 2020).
- Estimated Influenza Illnesses, Medical Visits, Hospitalizations, and Deaths in the United States—2018–2019 Influenza Season. Centers for Disease Control and Prevention. Available online: www.cdc.gov/flu/about/burden/2018-2019.html (accessed on 8 January 2020).
- Sorci, G.; Faivre, B.; Morand, S. Explaining Among-Country Variation IN COVID-19 Case Fatality Rate. Nature News. Available online: https://www.nature.com/articles/s41598-020-75848-2 (accessed on 3 November 2020).
- Vogel, L. World Must Prepare for Inevitable next Flu Pandemic, WHO Says. Reuters 2019, 191, E405. [Google Scholar]
- Baldo, V.; Bertoncello, C.; Cocchio, S.; Fonzo, M.; Pillon, P.; Buja, A.; Baldovin, T. The new pandemic influenza A/(H1N1)pdm09 virus: Is it really “new”? J. Prev. Med. Hyg. 2016, 57, E19. [Google Scholar]
- CEBM. Global COVID-19 Case Fatality Rates-CEBM. Available online: www.cebm.net/covid-19/global-covid-19-case-fatality-rates/ (accessed on 26 July 2021).
- The Infection Fatality Rate of COVID-19 In Stockholm—Technical Report. Available online: www.reddit.com/r/COVID19/comments/hakso9/the_infection_fatality_rate_of_covid19_in/ (accessed on 26 July 2021).
- GardaWorld. Egypt: First Case of Coronavirus Confirmed in Egypt February 14/Update 1. Available online: www.garda.com/crisis24/news-alerts/314286/egypt-first-case-of-coronavirus-confirmed-in-egypt-february-14-update-1 (accessed on 26 April 2021).
- Gardner, W.; States, D.; Bagley, N. The coronavirus and the risks to the elderly in long-term care. J. Aging Soc. Policy 2020, 32, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Lima, C.K.T.; de Medeiros Carvalho, P.M.; Lima, I.D.A.A.S.; de Oliveira Nunes, J.V.A.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.I.; Neto, M.L.R. The emotional impact of coronavirus 2019-NCoV (new coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Tanne, J.H.; Hayasaki, E.; Zastrow, M.; Pulla, P.; Smith, P.; Rada, A.G. COVID-19: How Doctors and Healthcare Systems Are Tackling Coronavirus Worldwide. BMJ 2020, 368, m1090. [Google Scholar] [CrossRef] [Green Version]
- Mikhael, E.M.; Al-Jumaili, A.A. Can developing countries face novel coronavirus outbreak alone? The Iraqi situation. Public Health Pract. 2020, 1, 100004. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- World Health Organization. What are the Health Risks Related TO Overcrowding? Available online: www.who.int/water_sanitation_health/emergencies/qa/emergencies_qa9/en/ (accessed on 26 April 2021).
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical course and outcomes of critically Ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet. Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- UNICEF DATA. Handwashing Data to Inform the COVID-19 Response. Available online: Data.unicef.org/resources/handwashing-data-covid-19-response/#12047-4 (accessed on 26 April 2021).
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.H.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmissions: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Rui, J.; Wang, Q.; Zhao, Z.; Cui, J.; Yin, L. A mathematical model for simulating the phase-based transmissibility of a novel coronavirus. Infect. Dis. Poverty 2020, 9, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsan, M.; Westerhaus, M.; Herce, M.; Nakashima, K.; Farmer, P. Poverty, global health, and infectious disease: Lessons from Haiti and Rwanda. Infect. Dis. Clin. N. Am. 2011, 25, 611–622. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. TDR | Global Report for Research on Infectious Diseases of Poverty. World Health Organization. Available online: https://www.who.int/tdr/publications/global_report/en/ (accessed on 20 August 2015).
- Bonds, M.; Dobson, A.; Keenan, D. Disease ecology, biodiversity, and the latitudinal gradient in income. PLoS Biol. 2012, 10, e1001456. [Google Scholar] [CrossRef] [PubMed]
- Sahasranaman, A.; Jensen, H.J. Poverty in the time of epidemic: A modelling perspective. PLoS ONE 2020, 15, e0242042. [Google Scholar] [CrossRef] [PubMed]
- Bukari, C.; Essilfie, G.; Aning-Agyei, M.A.; Otoo, I.C.; Kyeremeh, C.; Owusu, A.A.; Amuquandoh, K.F.; Bukari, K.I. Impact of COVID-19 on poverty and living standards in Ghana: A micro-perspective. Cogent Econ. Finance 2021, 9, 1. [Google Scholar] [CrossRef]
- World Health Statistics. 2012. Available online: http://apps.who.int/iris/bitstream/10665/44844/1/9789241564441_eng.pdf (accessed on 26 April 2021).
- Blavatnik School of Government. Coronavirus Government Response Tracker. Available online: www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker (accessed on 28 July 2020).
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Pandemic (COVID-19)—Statistics and Research. Available online: https://ourworldindata.org/coronavirus (accessed on 28 July 2020).
- Harding, A. Coronavirus in South Africa: The lull before the surge? BBC News. 10 April 2020. Available online: www.bbc.com/news/world-africa-52228932 (accessed on 28 July 2021).
- Coronavirus (COVID-19) Testing—Our World in Data. (n.d.) Available online: https://ourworldindata.org/coronavirus-testing (accessed on 30 July 2020).
- World Health Organization COVID-19 Briefing Transcript March 30. Available online: www.rev.com/blog/transcripts/world-health-organization-covid-19-briefing-transcript-march-30 (accessed on 1 April 2020).
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Sasson, I. Age and COVID-19 mortality: A comparison of Gompertz doubling time across countries and causes of death. Demogr. Res. 2021, 44, 379–396. [Google Scholar] [CrossRef]


| Mean | Std.Dev | MCSE | Median | Equal-Tailed 95% Cred. Interval | ||
|---|---|---|---|---|---|---|
| Confirmed_Cases | ||||||
| Population Density | −0.0052613 | 0.0021246 | 0.000067 | −0.0051941 | −0.009677 | −0.0011185 |
| Aged 65 Older | 0.1831922 | 0.1896953 | 0.005703 | 0.1855481 | −0.174675 | 0.550733 |
| Cvd Death Rate | −0.0011224 | 0.0036282 | 0.000113 | −0.0011888 | −0.008117 | 0.0061924 |
| Diabetes Prevalence | 0.062837 | 0.0799469 | 0.002528 | 0.0618234 | −0.093096 | 0.2195652 |
| Handwashing Facilities | 0.0200225 | 0.0102218 | 0.000319 | 0.0200439 | 0.0006078 | 0.0405081 |
| Extreme Poverty | −0.0028848 | 0.010585 | 0.000335 | −0.0029234 | −0.024479 | 0.017851 |
| _Cons | 6.22023 | 1.139261 | 0.036027 | 6.19992 | 3.77586 | 8.390462 |
| Var | 2.209552 | 0.5010807 | 0.018107 | 2.147209 | 1.413217 | 3.442549 |
| Country | Total Cases Reported | Total Deaths Reported | Cumulative Infections Estimated | Estimated IFR | Crude CFR | COVID-19 Transmission Classification Type |
|---|---|---|---|---|---|---|
| Algeria | 9134 | 638 | 272,017 | 0.24% | 7.00% | Community transmission |
| Angola | 77 | 4 | 19,187 | 0.02% | 5.20% | Clusters of cases |
| Benin | 224 | 3 | 8884 | 0.03% | 1.30% | Community transmission |
| Botswana | 35 | 1 | 22,819 | 0.00% | 2.90% | Clusters of cases |
| Burkina Faso | 847 | 53 | 10,257 | 0.52% | 6.30% | Community transmission |
| Burundi | 42 | 1 | 1959 | 0.05% | 2.40% | Clusters of cases |
| Cameroon | 5436 | 177 | 17,603 | 1.01% | 3.30% | Clusters of cases |
| Cape Verde | 405 | 4 | 12,464 | 0.03% | 1.00% | Community transmission |
| Central African Republic | 874 | 1 | 23,043 | 0.00% | 0.10% | Clusters of cases |
| Chad | 759 | 65 | 17,517 | 0.37% | 8.60% | Community transmission |
| Comoros | 87 | 2 | 4894 | 0.04% | 2.30% | Community transmission |
| Congo | 587 | 19 | 40,170 | 0.05% | 3.20% | Community transmission |
| Cote d’Ivoire | 2750 | 32 | 10,386 | 0.31% | 1.20% | Community transmission |
| Democratic Republic of Congo | 2833 | 69 | 14,499 | 0.48% | 2.40% | Community transmission |
| Djibouti | 2914 | 20 | 23,332 | 0.09% | 0.70% | Clusters of cases |
| Egypt | 22,082 | 879 | 205,083 | 0.43% | 4.00% | Clusters of cases |
| Equatorial Guinea | 1043 | 12 | 39,917 | 0.03% | 1.20% | Community transmission |
| Ethiopia | 968 | 8 | 19,147 | 0.04% | 0.80% | Clusters of cases |
| Gabon | 2613 | 15 | 27,858 | 0.05% | 0.60% | Clusters of cases |
| Gambia | 25 | 1 | 5357 | 0.02% | 4.00% | Community transmission |
| Ghana | 7616 | 34 | 21,248 | 0.16% | 0.40% | Sporadic cases |
| Guinea | 3656 | 22 | 16,782 | 0.13% | 0.60% | Community transmission |
| Guinea-Bissau | 1256 | 8 | 8235 | 0.10% | 0.60% | Community transmission |
| Kenya | 1745 | 62 | 15,440 | 0.40% | 3.60% | Community transmission |
| Liberia | 273 | 27 | 11,455 | 0.24% | 9.90% | Community transmission |
| Libya | 118 | 5 | 25,774 | 0.02% | 4.20% | Community transmission |
| Madagascar | 698 | 5 | 30,097 | 0.02% | 0.70% | Clusters of cases |
| Malawi | 273 | 4 | 5695 | 0.07% | 1.50% | Clusters of cases |
| Mali | 1226 | 73 | 42,636 | 0.17% | 6.00% | Clusters of cases |
| Mauritania | 423 | 20 | 18,496 | 0.11% | 4.70% | Community transmission |
| Mauritius | 335 | 10 | 19,972 | 0.05% | 3.00% | Clusters of cases |
| Morocco | 7714 | 202 | 25,380 | 0.80% | 2.60% | Clusters of cases |
| Mozambique | 234 | 2 | 11,812 | 0.02% | 0.90% | Clusters of cases |
| Niger | 955 | 64 | 12,248 | 0.52% | 6.70% | Clusters of cases |
| Nigeria | 9302 | 261 | 17,052 | 1.53% | 2.80% | Community transmission |
| Sao Tome and Principe | 463 | 12 | 10,292 | 0.12% | 2.60% | Community transmission |
| Senegal | 3429 | 41 | 13,239 | 0.31% | 1.20% | Clusters of cases |
| Sierra Leone | 829 | 45 | 8729 | 0.52% | 5.40% | Community transmission |
| Somalia | 1828 | 72 | 19,366 | 0.37% | 3.90% | Community transmission |
| South Africa | 29,240 | 611 | 47,859 | 1.28% | 2.10% | Sporadic cases |
| South Sudan | 994 | 10 | 26,287 | 0.04% | 1.00% | Community transmission |
| Sudan | 4521 | 233 | 71,606 | 0.33% | 5.20% | Clusters of cases |
| Swaziland | 279 | 2 | 22,122 | 0.01% | 0.70% | Community transmission |
| Tanzania | 509 | 21 | 41,536 | 0.05% | 4.10% | Community transmission |
| Togo | 428 | 13 | 9720 | 0.13% | 3.00% | Community transmission |
| Tunisia | 1071 | 48 | 302,601 | 0.02% | 4.50% | Community transmission |
| Zambia | 1057 | 7 | 14,677 | 0.05% | 0.70% | Community transmission |
| Zimbabwe | 160 | 4 | 20,130 | 0.02% | 2.50% | Sporadic cases |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onovo, A.A.; Kalaiwo, A.; Obanubi, C.; Odezugo, G.; Estill, J.; Keiser, O. Estimates of the COVID-19 Infection Fatality Rate for 48 African Countries: A Model-Based Analysis. BioMed 2021, 1, 63-79. https://doi.org/10.3390/biomed1010005
Onovo AA, Kalaiwo A, Obanubi C, Odezugo G, Estill J, Keiser O. Estimates of the COVID-19 Infection Fatality Rate for 48 African Countries: A Model-Based Analysis. BioMed. 2021; 1(1):63-79. https://doi.org/10.3390/biomed1010005
Chicago/Turabian StyleOnovo, Amobi Andrew, Abiye Kalaiwo, Christopher Obanubi, Gertrude Odezugo, Janne Estill, and Olivia Keiser. 2021. "Estimates of the COVID-19 Infection Fatality Rate for 48 African Countries: A Model-Based Analysis" BioMed 1, no. 1: 63-79. https://doi.org/10.3390/biomed1010005
APA StyleOnovo, A. A., Kalaiwo, A., Obanubi, C., Odezugo, G., Estill, J., & Keiser, O. (2021). Estimates of the COVID-19 Infection Fatality Rate for 48 African Countries: A Model-Based Analysis. BioMed, 1(1), 63-79. https://doi.org/10.3390/biomed1010005