

Practical Use of the (Observer)—Reporter—Interpreter—Manager—Expert ((O)RIME) Framework in Veterinary Clinical Teaching with a Clinical Example



Abstract
1. Introduction
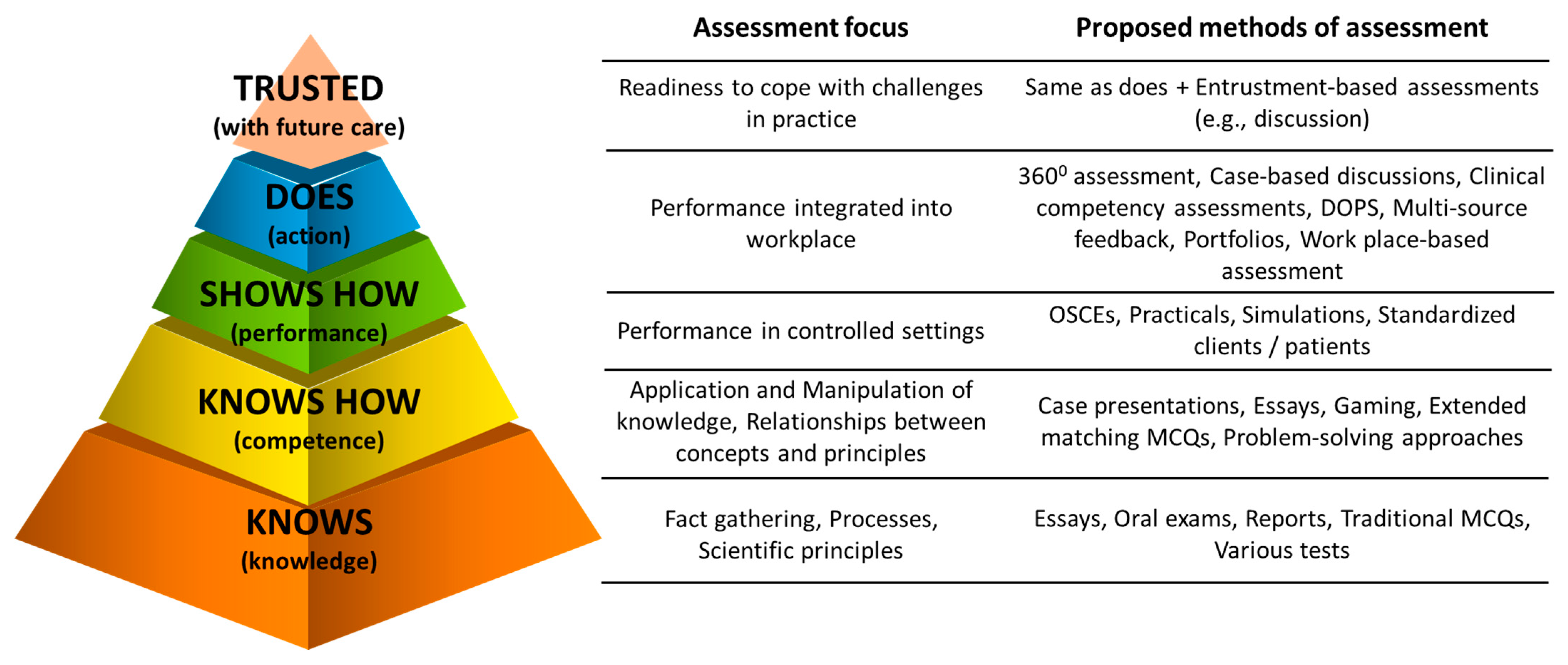
1.1. Basics of Assessment of Clinical Competency of Veterinary Learners
1.2. Common Traps in Assessment of Clinical Competency in Veterinary Learners
2. (O)RIME Framework for Assessment of Clinical Competency of Learners
2.1. Levels of Clinical Competence of Learners Using the (O)RIME Model of Assessment
2.2. Advantages of the (O)RIME Framework
- A systematic structure of expectations that can be coupled with day one competencies to guide students though their education, and allow Faculty to assess and evaluate the introduction, implementation and assessment of these skills in the curriculum [30].
- Allows for early detection of at-risk learners [17,21,28,31]. These identified learners need immediate attention. The prompt addressing of poor performance has been stated as a priority for any medical, presumably including veterinary medical, education delivered in an outcome-based training mode [32].
- Allows for standardized assessment of clinical competencies of learners and, when implemented correctly, should prevent assessment of learners relative to each-other [21].
- At each level, it assesses a synthesis of attitudes, knowledge and skills, rather than assessing them individually as done with many other frameworks of assessment.
- Can be used for assessment of a single clinical encounter, day, week or an entire course. Hence, the (O)RIME framework can be used as an assessment method for the creating of a regular record of in-training assessment (RITA) [34]
- The framework takes advantage of a clinician’s ability to draw conclusions from observations and data, and uses that the same diagnostic approach in the assessment of students whilst also addressing the emotional difficulty teachers have in “giving” a grade, e.g., “does what I see before me in this patient fit better with xxx” translates into ”does what I see before me in this student fit better with reporter, interpreter or manager?” [37].
2.3. Limitations of the (O)RIME Framework
- The meaning of words and terminology are not always self-evident, e.g., “reporting” is not simply repeating the facts but is about the process of getting the facts [37].
- The (O)RIME framework is not suitable for assessing individual skills. It rather assesses the overall clinical competency of the learner [21], albeit potentially within a single clinical encounter. This is completely understandable as the framework is a synthetic method of assessment, not analytical.
- During a single clinical encounter a learner may demonstrate capacity from several domains of the (O)RIME framework [33]. This may occur in any of the assessments. Analytical methods of assessment may suffer less from this problem.
- The framework is not designed for assessment of non-technical skills and competencies but rather for only technical skills and competencies [26,33]. Hence, Holmes et al. (2014) recommended the use of the (P)RIME framework, where P is for professionalism [33]. An alternative assessment method for soft skills is the multi-sourced feedback [34]. However, the suggested limitation of the framework related to the assessment of non-technical skills may not be entirely true, as some studies have shown it to be effective in assessing these skills and competencies of learners [38]. Clearly, this ‘limitation’ requires further investigation.
- The framework is often not recommended as a sole method of assessment of the progression of learners [21], particularly at schools relying on a tier mark-associated grading system. Hence, some authors have recommended it to be used only as part of the toolbox of assessment of the progression of learners [21] coupled with methodologies such as direct observations.
- For fulfilling the assessment requirements, the (O)RIME framework requires team involvement (observations by all team members), rather than grading by a single person. Hence, some organizational skills are required to ensure ‘a round table discussion’ occurs before the level is discussed by a nominated person with the learner [39]. However, this limitation of the framework may not be always true as some studies have shown good assessment characteristics using the learners’ progression judged by single assessors [40].
- Educators can get confused that the (O)RIME is a developmental framework in which students go through the phases. It is not. When the student moves from ‘reporter’ to ‘interpreter’, they do not stop being a reporter. When they move to ‘manager’, they must continue to gather information and interpret it.
3. Examples of Bovine Clinical Encounters
3.1. Example Clinical Encounter: Left Displaced Abomasum in a Dairy Cow
3.2. Example Clinical Encounter: Left Displaced Abomasum in a Dairy Cow
4. Discussion
Usefullness of (O)RIME for Veterinary Medical Education
5. Conclusions
6. Glossary of Terms
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carr, A.N.M.; Kirkwood, R.N.; Petrovski, K.R. Effective Veterinary Clinical Teaching in a Variety of Teaching Settings. Vet. Sci. 2022, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Modi, J.N.; Anshu; Gupta, P.; Singh, T. Teaching and assessing clinical reasoning skills. Indian Pediatrics 2015, 52, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Lateef, F. Clinical reasoning: The core of medical education and practice. Int. J. Intern. Emerg. Med. 2018, 1, 1015. [Google Scholar]
- Linn, A.; Khaw, C.; Kildea, H.; Tonkin, A. Clinical reasoning: A guide to improving teaching and practice. Aust. Fam. Physician 2012, 41, 18–20. [Google Scholar] [PubMed]
- Dreifuerst, K.T. Using debriefing for meaningful learning to foster development of clinical reasoning in simulation. J. Nurs. Educ. 2012, 51, 326–333. [Google Scholar] [CrossRef]
- Carr, A.N.; Kirkwood, R.N.; Petrovski, K.R. Using the five-microskills method in veterinary medicine clinical teaching. Vet. Sci. 2021, 8, 89. [Google Scholar] [CrossRef]
- McKimm, J. Giving effective feedback. Br. J. Hosp. Med. 2009, 70, 158–161. [Google Scholar] [CrossRef]
- Steinert, Y.; Mann, K.V. Faculty Development: Principles and Practices. J. Vet. Med. Educ. 2006, 33, 317–324. [Google Scholar] [CrossRef]
- Houston, T.K.; Ferenchick, G.S.; Clark, J.M.; Bowen, J.L.; Branch, W.T.; Alguire, P.; Esham, R.H.; Clayton, C.P.; Kern, D.E. Faculty development needs. J. Gen. Intern. Med. 2004, 19, 375–379. [Google Scholar] [CrossRef][Green Version]
- Hashizume, C.T.; Hecker, K.G.; Myhre, D.L.; Bailey, J.V.; Lockyer, J.M. Supporting veterinary preceptors in a distributed model of education: A faculty development needs assessment. J. Vet. Med. Educ. 2016, 43, 104–110. [Google Scholar] [CrossRef]
- Lane, I.F.; Strand, E. Clinical veterinary education: Insights from faculty and strategies for professional development in clinical teaching. J. Vet. Med. Educ. 2008, 35, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, S.T.; Couldry, R.; Phillips, H.; Buck, B. Preceptor development: Providing effective feedback. Hosp Pharm 2013, 48, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.E. The assessment of clinical skills/competence/performance. Acad. Med. 1990, 65, S63–S67. [Google Scholar] [CrossRef]
- ten Cate, O.; Carraccio, C.; Damodaran, A.; Gofton, W.; Hamstra, S.J.; Hart, D.; Richardson, D.; Ross, S.; Schultz, K.; Warm, E.; et al. Entrustment Decision Making: Extending Miller’s Pyramid. Acad. Med. 2020, 96, 199–204. [Google Scholar] [CrossRef]
- Al-Eraky, M.; Marei, H. A fresh look at Miller’s pyramid: Assessment at the ‘Is’ and ‘Do’ levels. Med. Educ. 2016, 50, 1253–1257. [Google Scholar] [CrossRef] [PubMed]
- Pangaro, L.; Ten Cate, O. Frameworks for learner assessment in medicine: AMEE Guide No. 78. Med. Teach. 2013, 35, e1197–e1210. [Google Scholar] [CrossRef]
- Hemmer, P.A.; Papp, K.K.; Mechaber, A.J.; Durning, S.J. Evaluation, grading, and use of the RIME vocabulary on internal medicine clerkships: Results of a national survey and comparison to other clinical clerkships. Teach. Learn. Med. 2008, 20, 118–126. [Google Scholar] [CrossRef]
- Smith, C.S. A developmental approach to evaluating competence in clinical reasoning. J. Vet. Med. Educ. 2008, 35, 375–381. [Google Scholar] [CrossRef]
- Pangaro, L.N. A shared professional framework for anatomy and clinical clerkships. Clin. Anat. 2006, 19, 419–428. [Google Scholar] [CrossRef]
- Papp, K.K.; Huang, G.C.; Clabo, L.M.L.; Delva, D.; Fischer, M.; Konopasek, L.; Schwartzstein, R.M.; Gusic, M. Milestones of critical thinking: A developmental model for medicine and nursing. Acad. Med. 2014, 89, 715–720. [Google Scholar] [CrossRef]
- Sepdham, D.; Julka, M.; Hofmann, L.; Dobbie, A. Using the RIME model for learner assessment and feedback. Fam. Med.-Kans. City 2007, 39, 161. [Google Scholar]
- Fazio, S.B.; Torre, D.M.; DeFer, T.M. Grading Practices and Distributions Across Internal Medicine Clerkships. Teach. Learn. Med. 2016, 28, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.; Robillard, D.; Gehlbach, L.; Moore Simas, T.A. Impact of pass/fail grading on medical students’ well-being and academic outcomes. Med. Educ. 2011, 45, 867–877. [Google Scholar] [CrossRef] [PubMed]
- Pangaro, L. A new vocabulary and other innovations for improving descriptive in-training evaluations. Acad. Med. 1999, 74, 1203–1207. [Google Scholar] [CrossRef] [PubMed]
- Battistone, M.J.; Pendelton, B.; Milne, C.; Battistone, M.L.; Sande, M.A.; Hemmer, P.A.; Shomaker, T.S. Global descriptive evaluations are more responsive than global numeric ratings in detecting students’ progress during the inpatient portion of an internal medicine clerkship. Acad. Med. 2001, 76, S105–S107. [Google Scholar] [CrossRef]
- Ander, D.S.; Wallenstein, J.; Abramson, J.L.; Click, L.; Shayne, P. Reporter-Interpreter-Manager-Educator (RIME) Descriptive Ratings as and Evaluation tool in an Emergency Medicine Clerkship. J. Emerg. Med. 2012, 43, 720–727. [Google Scholar] [CrossRef]
- Tham, K.Y. Observer-Reporter-Interpreter-Manager-Educator (ORIME) Framework to Guide Formative Assessment of Medical Students. Ann. Acad. Med. Singap. 2013, 42, 603–607. [Google Scholar]
- Tolsgaard, M.G.; Arendrup, H.; Lindhardt, B.O.; Hillingso, J.G.; Stoltenberg, M.; Ringsted, C. Construct Validity of the Reporter-Interpreter-Manager-Educator Structure for Assessing Students’ Patient Encounter Skills. Acad. Med. 2012, 87, 799–806. [Google Scholar] [CrossRef]
- Hauer, K.E.; Mazotti, L.; O’Brien, B.; Hemmer, P.A.; Tong, L. Faculty verbal evaluations reveal strategies used to promote medical student performance. Med. Educ. Online 2011, 16, 6354. [Google Scholar] [CrossRef]
- Battistone, M.J.; Milne, C.; Sande, M.A.; Pangaro, L.N.; Hemmer, P.A.; Shomaker, T.S. The feasibility and acceptability of implementing formal evaluation sessions and using descriptive vocabulary to assess student performance on a clinical clerkship. Teach. Learn. Med. 2002, 14, 5–10. [Google Scholar] [CrossRef]
- Hemmer, P.A.; Pangaro, L. The effectiveness of formal evaluation sessions during clinical clerkships in better identifying students with marginal funds of knowledge. Acad. Med. J. Assoc. Am. Med. Coll. 1997, 72, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Irvine, D. The performance of doctors. II: Maintaining good practice, protecting patients from poor performance. BMJ 1997, 314, 1613. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.V.; Peltier, C.B.; Hanson, J.L.; Lopreiato, J.O. Writing medical student and resident performance evaluations: Beyond “performed as expected”. Pediatrics 2014, 133, 766–768. [Google Scholar] [CrossRef]
- Cook, R.; Pedley, D.; Thakore, S. A structured competency based training programme for junior trainees in emergency medicine: The “Dundee Model”. Emerg. Med. J. 2006, 23, 18–22. [Google Scholar] [CrossRef][Green Version]
- Krathwohl, D.R. A revision of Bloom’s taxonomy: An overview. Theory Into Pract. 2002, 41, 212–218. [Google Scholar] [CrossRef]
- Bloom, B.S. Taxonomy of Educational Objectives: The Classification of Educational Goals: Cognitive Domain; David McKay Company: New York, NY, USA, 1956. [Google Scholar]
- Pangaro, L. Behind the Curtain with Louis Pangaro: How the RIME Framework Was Born. Available online: https://harvardmacy.org/index.php/hmi/behind-the-curtain-with-louis-pangaro-how-the-rime-framework-was-born (accessed on 18 October 2021).
- Hemmer, P.A.; Hawkins, R.; Jackson, J.L.; Pangaro, L.N. Assessing how well three evaluation methods detect deficiencies in medical students’ professionalism in two settings of an internal medicine clerkship. Acad. Med. 2000, 75, 167–173. [Google Scholar] [CrossRef]
- Bloomfield, L.; Magney, A.; Segelov, E. Reasons to try ‘RIME’. Med. Educ. 2007, 41, 1104. [Google Scholar] [CrossRef]
- Griffith, C.H.; Wilson, J.F. The association of student examination performance with faculty and resident ratings using a modified RIME process. J. Gen. Intern. Med. 2008, 23, 1020–1023. [Google Scholar] [CrossRef]
- Bordage, G.; Daniels, V.; Wolpaw, T.M.; Yudkowsky, R. O–RI–M: Reporting to include data interpretation. Acad. Med. 2021, 96, 1079–1080. [Google Scholar] [CrossRef]
- Ryan, M.S.; Lee, B.; Richards, A.; Perera, R.A.; Haley, K.; Rigby, F.B.; Park, Y.S.; Santen, S.A. Evaluating the Reliability and Validity Evidence of the RIME (Reporter-Interpreter-Manager-Educator) Framework for Summative Assessments Across Clerkships. Acad. Med. 2021, 96, 256–262. [Google Scholar] [CrossRef]
- Neher, J.O.; Gordon, K.C.; Meyer, B.; Stevens, N. A five-step “microskills” model of clinical teaching. J. Am. Board Fam. Pract./Am. Board Fam. Pract. 1992, 5, 419–424. [Google Scholar]
- Neher, J.O.; Stevens, N.G. The one-minute preceptor: Shaping the teaching conversation. Fam. Med. 2003, 35, 391–393. [Google Scholar]
- Swartz, M.K. Revisiting “The One-Minute Preceptor”. J. Pediatric Health Care 2016, 30, 95–96. [Google Scholar] [CrossRef]
- Kelly, W.; Durning, S.; Denton, G. Comparing a script concordance examination to a multiple-choice examination on a core internal medicine clerkship. Teach. Learn. Med. 2012, 24, 187–193. [Google Scholar] [CrossRef]
- Stephens, M.B.; Gimbel, R.W.; Pangaro, L. Commentary: The RIME/EMR scheme: An educational approach to clinical documentation in electronic medical records. Acad. Med. 2011, 86, 11–14. [Google Scholar] [CrossRef]
- Klocko, D.J. Enhancing physician assistant student clinical rotation evaluations with the RIME scoring format: A retrospective 3-year analysis. J. Physician Assist. Educ. 2016, 27, 176–179. [Google Scholar] [CrossRef]
- DeWitt, D.; Carline, J.; Paauw, D.; Pangaro, L. Pilot study of a ‘RIME’-based tool for giving feedback in a multi-specialty longitudinal clerkship. Med. Educ. 2008, 42, 1205–1209. [Google Scholar] [CrossRef]
- Tolsgaard, M.G.; Jepsen, R.; Rasmussen, M.B.; Kayser, L.; Fors, U.; Laursen, L.C.; Svendsen, J.H.; Ringsted, C. The effect of constructing versus solving virtual patient cases on transfer of learning: A randomized trial. Perspect. Med. Educ. 2016, 5, 33–38. [Google Scholar] [CrossRef]
- Van Der Vleuten, C.P.; Schuwirth, L.W. Assessing professional competence: From methods to programmes. Med. Educ. 2005, 39, 309–317. [Google Scholar] [CrossRef]
- Norcini, J.J.; McKinley, D.W. Assessment methods in medical education. Teach. Teach. Educ. 2007, 23, 239–250. [Google Scholar] [CrossRef]
- Baker, E.A.; Ledford, C.H.; Fogg, L.; Way, D.P.; Park, Y.S. The IDEA assessment tool: Assessing the reporting, diagnostic reasoning, and decision-making skills demonstrated in medical students’ hospital admission notes. Teach. Learn. Med. 2015, 27, 163–173. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Learner Level | Descriptor | Learner Report | Effective Instructor’s Feedback 1 |
|---|---|---|---|
| Observer | Bystander. Merely describing data | ’We were presented with a Holstein Friesian cow that calved 3 weeks ago. The client reported sudden loss of appetite and a drop in milk production was detected yesterday afternoon and is still present.’ | ’This is a really good start. Do you know the age of the cow? This would be very helpful. Based on the information you have gathered, how you would examine this patient if I was not around?’ |
| Reporter | Understanding ‘what is wrong’ and some of the ‘why it is wrong’ | ’We were presented with a 5-yr old, Holstein Friesian cow that calved 3 weeks ago. The client reported a sudden inappetence and a drop in milk production from last night. Major abnormalities detected on clinical examination included 4+ ketone bodies in urine, ketone odor of the breath, rumen fill of score 1, rumen atony, left side ‘ping’ in the area of the last 2 ribs on the left side, and sloshing sounds on succussion.’ | ’This is a really good summary. Now, can you think of some reasons for these detected signs?’ ’This is a really good summary. Now, based on the detected signs, it will be great to come up with a list of 3–4 differential diagnoses that should be considered.’ |
| Interpreter | Understanding ‘why it is wrong’ | ‘… based on the presenting signs, I believe she suffers from left displaced abomasum with a secondary ketosis due to the loss of appetite. Another possibility that should be considered is a LDA secondary to metritis. However, the basic clinical examination gave no indications of metritis.’ | ‘Excellent differential diagnosis. You mentioned metritis. I would be very interested to hear your reasoning that resulted in the elimination of metritis as a primary diagnosis in this case.’ ‘Excellent differential diagnosis. You mentioned secondary ketosis. I would be interested to hear your reasoning as why it has occurred in this case’ |
| Manager | Understanding ‘how to address the problem’ demonstrating prioritization and skills of analysis of major problems. Considers client’s particular circumstances. | ‘… I would like to ensure that she really has LDA before opting for surgery. As the cow is in the clinic, options that I consider in the workup include ultrasonography and/or Liptak test. If the diagnosis is confirmed, LDA surgery by right side approach will be recommended. Post-operatively, I would consider giving the cow some propylene glycol and electrolytes by oral administration. Surgical correction should result in full recovery. As the transit of ingesta return, ketosis should self-cure.’ | ‘This sounds like an excellent approach to reach the final diagnosis and very well-planned management of the case. Please elaborate the reason you considered this surgical approach for this particular case (NOTE: e.g., Client has experience and/or preference), and the post-operative care instructions to the client.’ I like your approach. I would be interested to hear what you would be looking for on ultrasound to confirm your diagnosis and surgical approach’ |
| Educator | Commit to self-learning, demonstration of reflection, and education of the team | ‘… This clinical encounter meets the criteria for a primary LDA with a secondary ketosis. Research indicates that surgical correction of LDA results in self-cure of ketosis but return to full production and good fertility indicators benefit from 3–7 days propylene glycol treatment. I discussed with the client the importance of the transition cow diet and its role in prevention of LDA in the future.’ | ‘Well done. Specifically, you managed this clinical encounter well and educated the client on the reasons for LDA occurring. I think you are ready for more complicated clinical encounters’ |
| Learner Level | Descriptor | Learner Report | Effective Instructor’s Feedback 1 |
|---|---|---|---|
| Observer | Bystander. Merely describing data | ’We were presented with a Jersey cow that calved 3 months ago. The client reported sudden loss of appetite and a drop in milk production was detected yesterday afternoon and is still present.’ | ’This is a really good start. Do you know the age of the cow? This would be very helpful. Based on the information you have gathered, how you would examine this patient if I was not around?’ |
| Reporter | Understanding ‘what is wrong’ and some of the ‘why it is wrong’ | ’We were presented with a 5-yr old, Holstein Friesian cow that calved 3 weeks ago. The client reported a sudden inappetence and a drop in milk production from last night. Major abnormalities detected on clinical examination included 4+ ketone bodies in urine, ketone odor of the breath, rumen fill of score 1, rumen atony, left side ‘ping’ in the area of the last 2 ribs on the left side, and sloshing sounds on succussion.’ | ’This is a really good summary. Now, can you think of some reasons for these detected signs?’ ’This is a really good summary. Now, based on the detected signs, it will be great to come up with a list of 3–4 differential diagnoses that should be considered.’ |
| Interpreter | Understanding ‘why it is wrong’ | ‘… based on the presenting signs, I believe she suffers from left displaced abomasum with a secondary ketosis due to the loss of appetite. Another possibility that should be considered is a LDA secondary to metritis. However, the basic clinical examination gave no indications of metritis.’ | ‘Excellent differential diagnosis. You mentioned metritis. I would be very interested to hear your reasoning that resulted in the elimination of metritis as a primary diagnosis in this case.’ ‘Excellent differential diagnosis. You mentioned secondary ketosis. I would be interested to hear your reasoning as why it has occurred in this case’ |
| Manager | Understanding ‘how to address the problem’ demonstrating prioritization and skills of analysis of major problems. Considers client’s particular circumstances. | ‘… I would like to ensure that she really has LDA before opting for surgery. As the cow is in the clinic, options that I consider in the workup include ultrasonography and/or Liptak test. If the diagnosis is confirmed, LDA surgery by right side approach will be recommended. Post-operatively, I would consider giving the cow some propylene glycol and electrolytes by oral administration. Surgical correction should result in full recovery. As the transit of ingesta return, ketosis should self-cure.’ | ‘This sounds like an excellent approach to reach the final diagnosis and very well-planned management of the case. Please elaborate the reason you considered this surgical approach for this particular case (NOTE: e.g., Client has experience and/or preference), and the post-operative care instructions to the client.’ I like your approach. I would be interested to hear what you would be looking for on ultrasound to confirm your diagnosis and surgical approach’ |
| Educator | Commit to self-learning, demonstration of reflection, and education of the team | ‘… This clinical encounter meets the criteria for a primary LDA with a secondary ketosis. Research indicates that surgical correction of LDA results in self-cure of ketosis but return to full production and good fertility indicators benefit from 3–7 days propylene glycol treatment. I discussed with the client the importance of the transition cow diet and its role in prevention of LDA in the future.’ | ‘Well done. Specifically, you managed this clinical encounter well and educated the client on the reasons for LDA occurring. I think you are ready for more complicated clinical encounters’ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carr, A.N.; Kirkwood, R.N.; Petrovski, K.R. Practical Use of the (Observer)—Reporter—Interpreter—Manager—Expert ((O)RIME) Framework in Veterinary Clinical Teaching with a Clinical Example. Encyclopedia 2022, 2, 1666-1677. https://doi.org/10.3390/encyclopedia2040113
Carr AN, Kirkwood RN, Petrovski KR. Practical Use of the (Observer)—Reporter—Interpreter—Manager—Expert ((O)RIME) Framework in Veterinary Clinical Teaching with a Clinical Example. Encyclopedia. 2022; 2(4):1666-1677. https://doi.org/10.3390/encyclopedia2040113
Chicago/Turabian StyleCarr, Amanda Nichole (Mandi), Roy Neville Kirkwood, and Kiro Risto Petrovski. 2022. "Practical Use of the (Observer)—Reporter—Interpreter—Manager—Expert ((O)RIME) Framework in Veterinary Clinical Teaching with a Clinical Example" Encyclopedia 2, no. 4: 1666-1677. https://doi.org/10.3390/encyclopedia2040113
APA StyleCarr, A. N., Kirkwood, R. N., & Petrovski, K. R. (2022). Practical Use of the (Observer)—Reporter—Interpreter—Manager—Expert ((O)RIME) Framework in Veterinary Clinical Teaching with a Clinical Example. Encyclopedia, 2(4), 1666-1677. https://doi.org/10.3390/encyclopedia2040113