
Do Exercise, Physical Activity, Dietetic, or Combined Interventions Improve Body Weight in New Kidney Transplant Recipients? A Narrative Systematic Review and Meta-Analysis

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Protocol and Registration
2.2. Study Identification
2.3. Study Selection, Data Extraction, and Risk-of-Bias
2.4. Statistical Analysis
3. Results
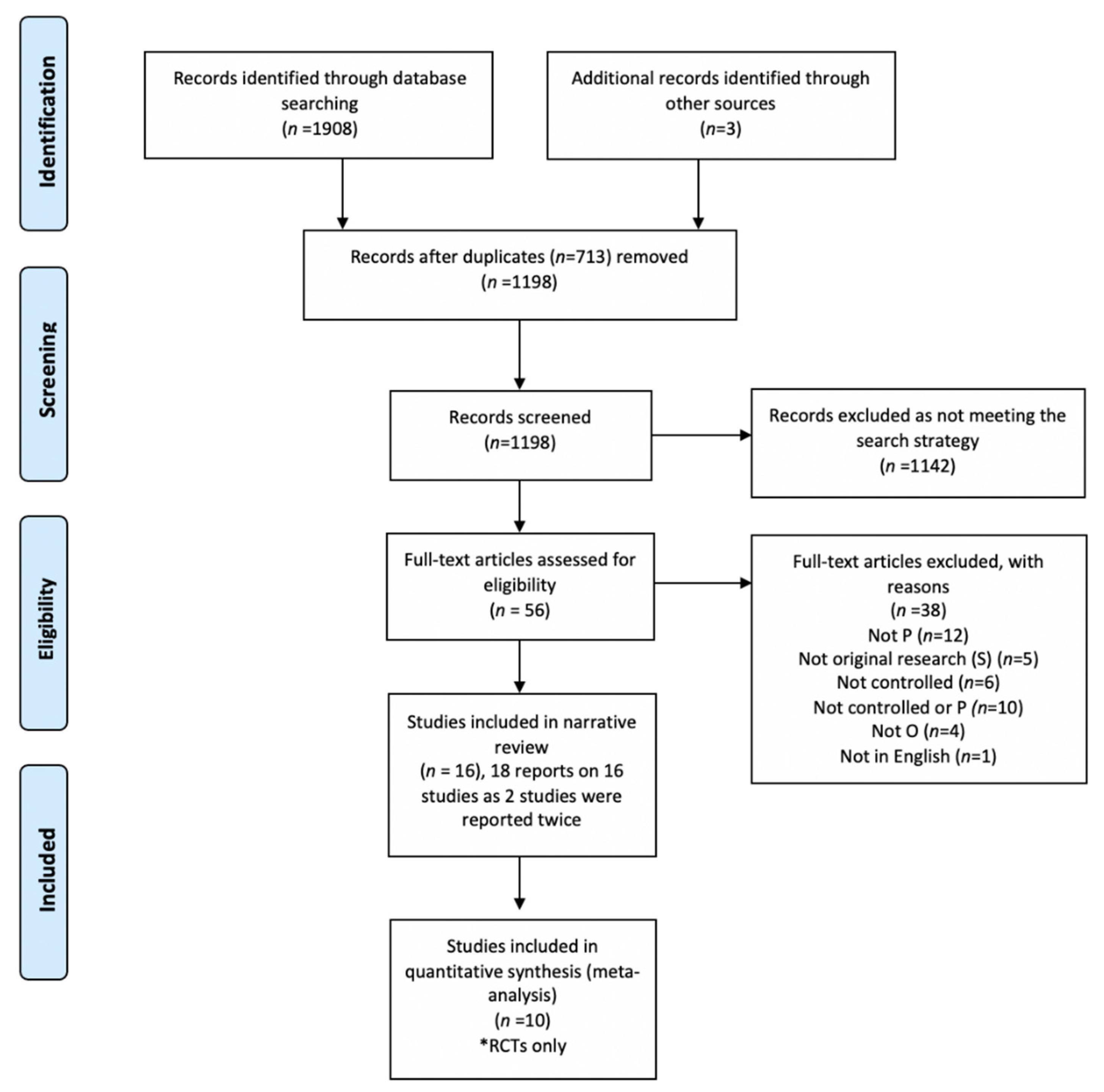
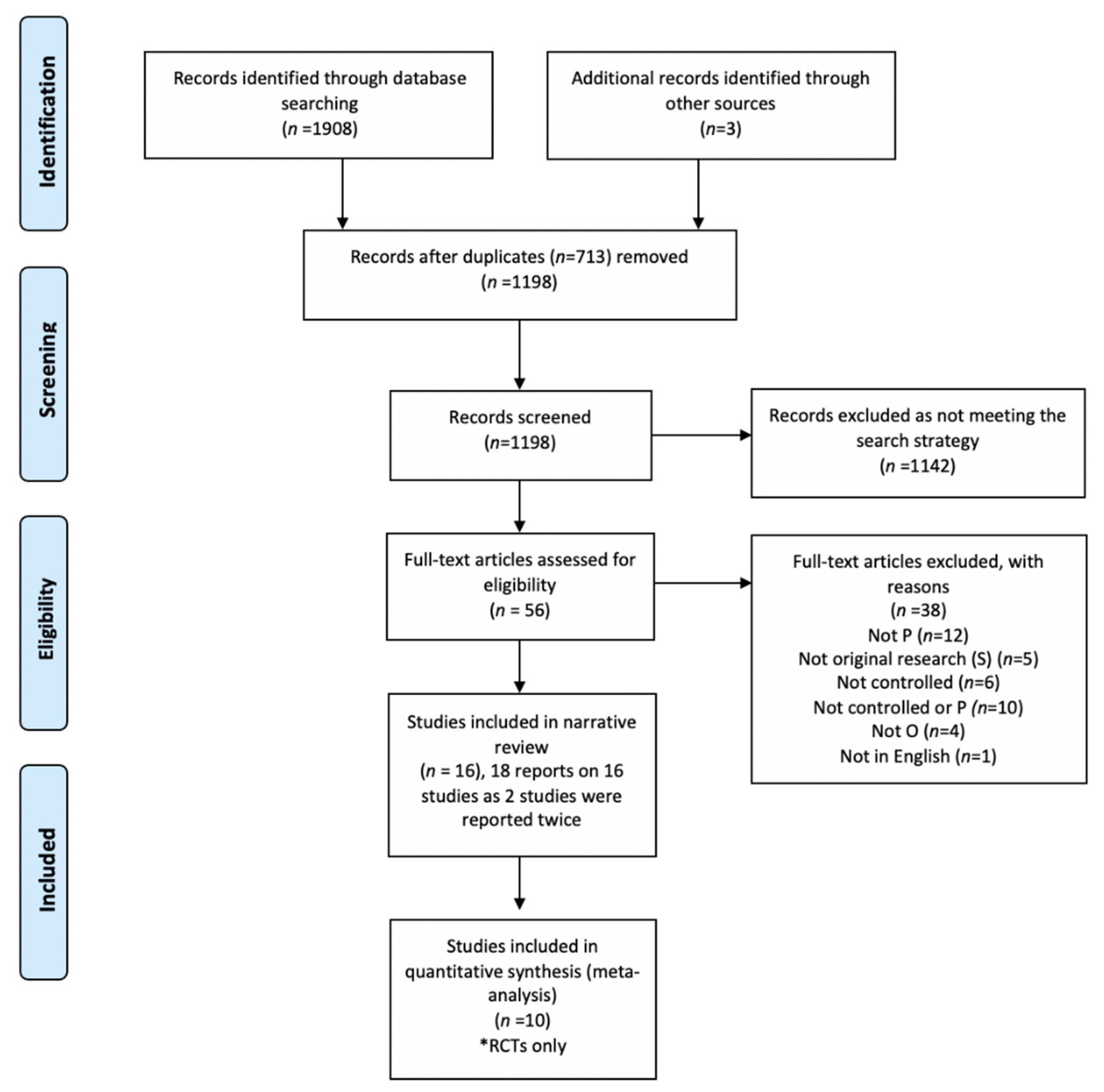
3.1. Search Results and Study Characteristics
3.2. Characteristics of Interventions
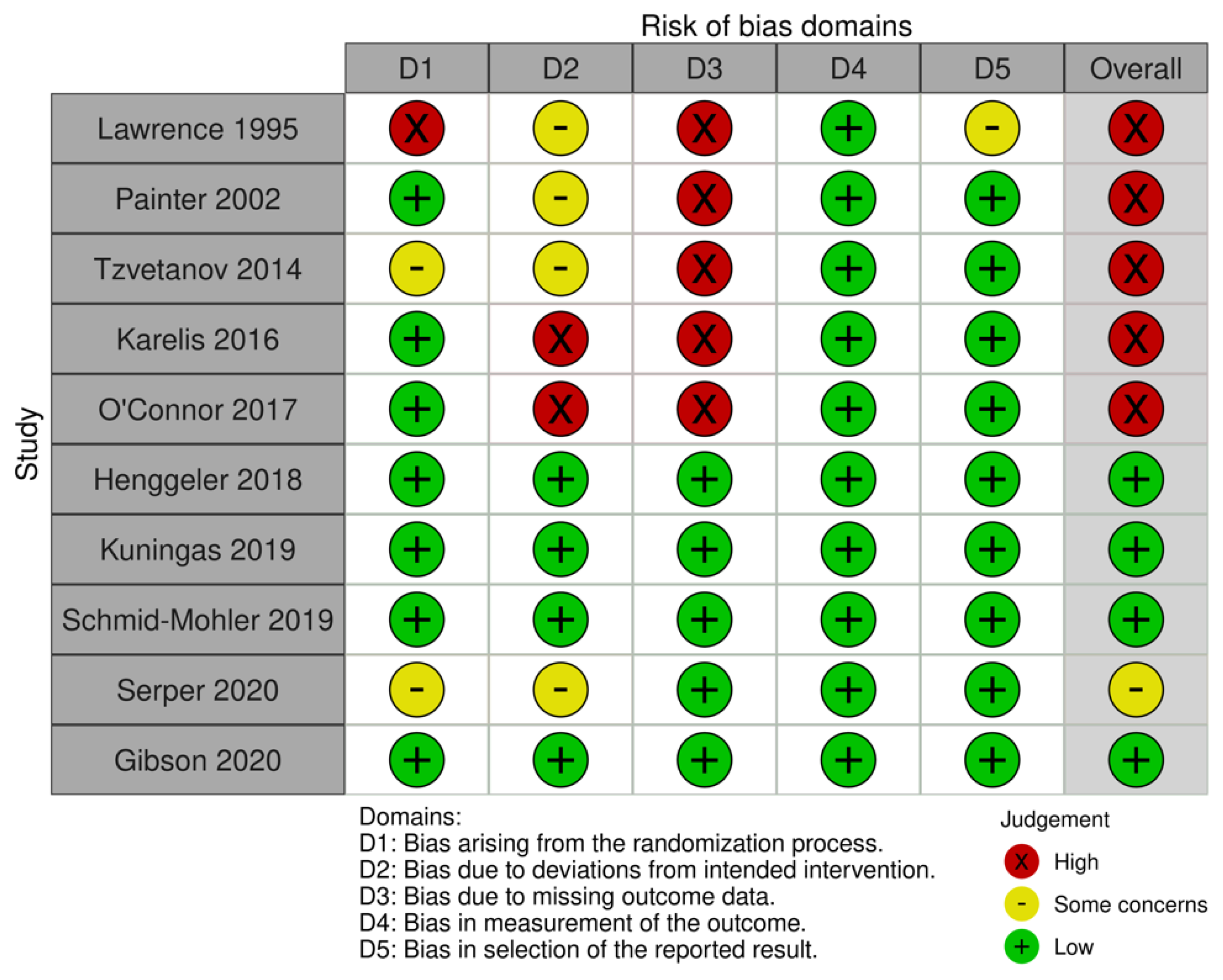
3.3. Risk-of-Bias
3.4. Body Weight and BMI
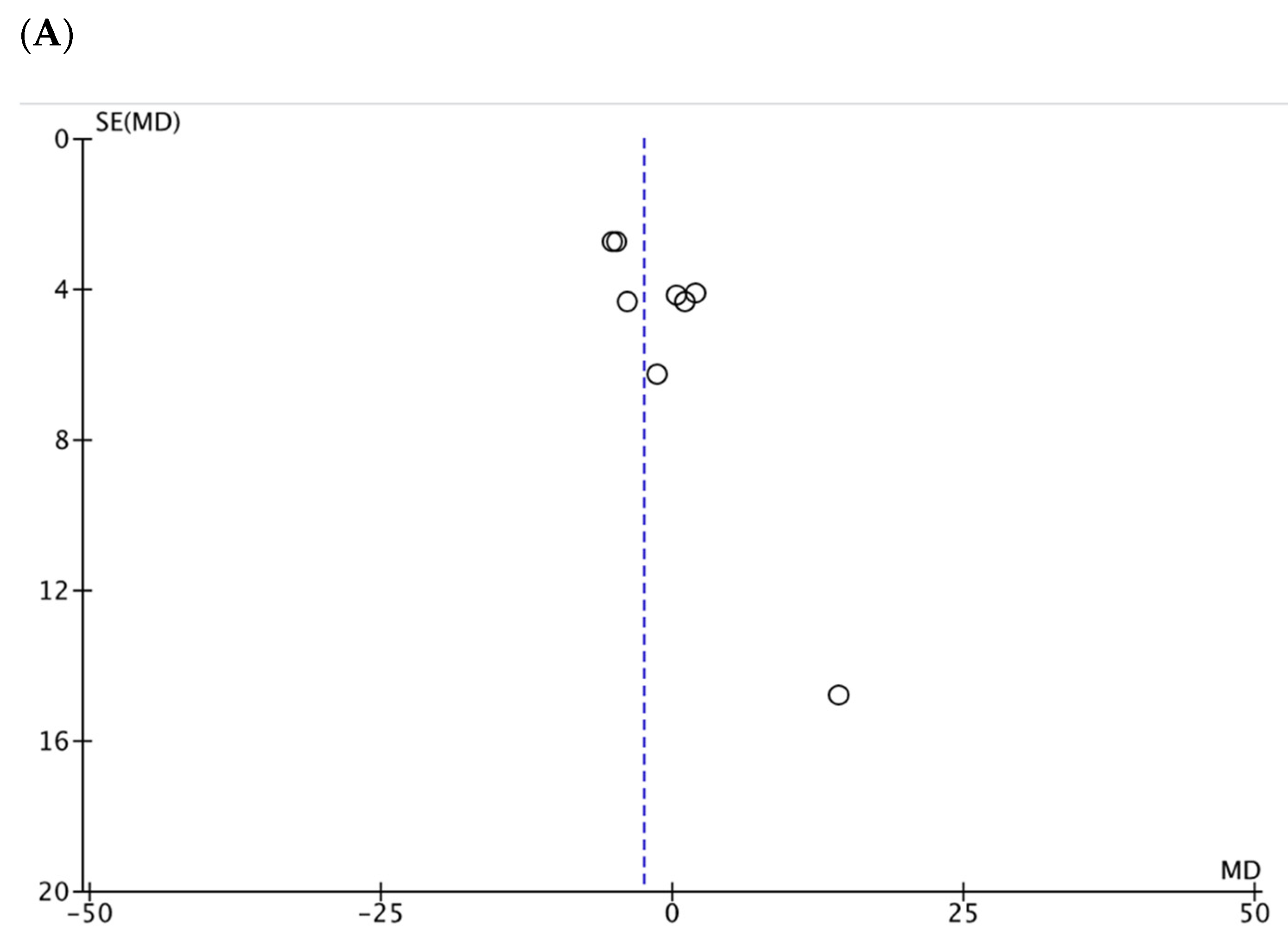
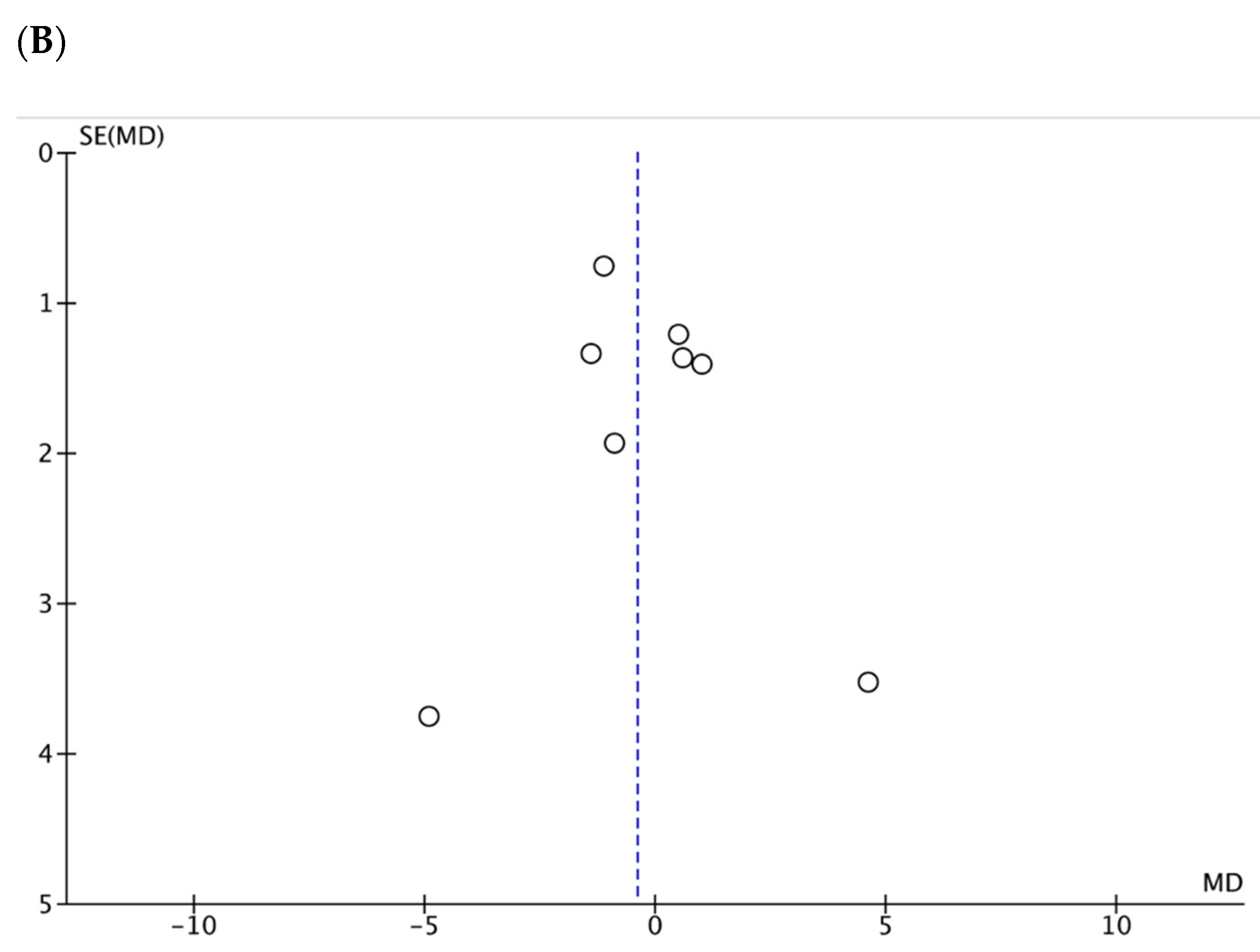
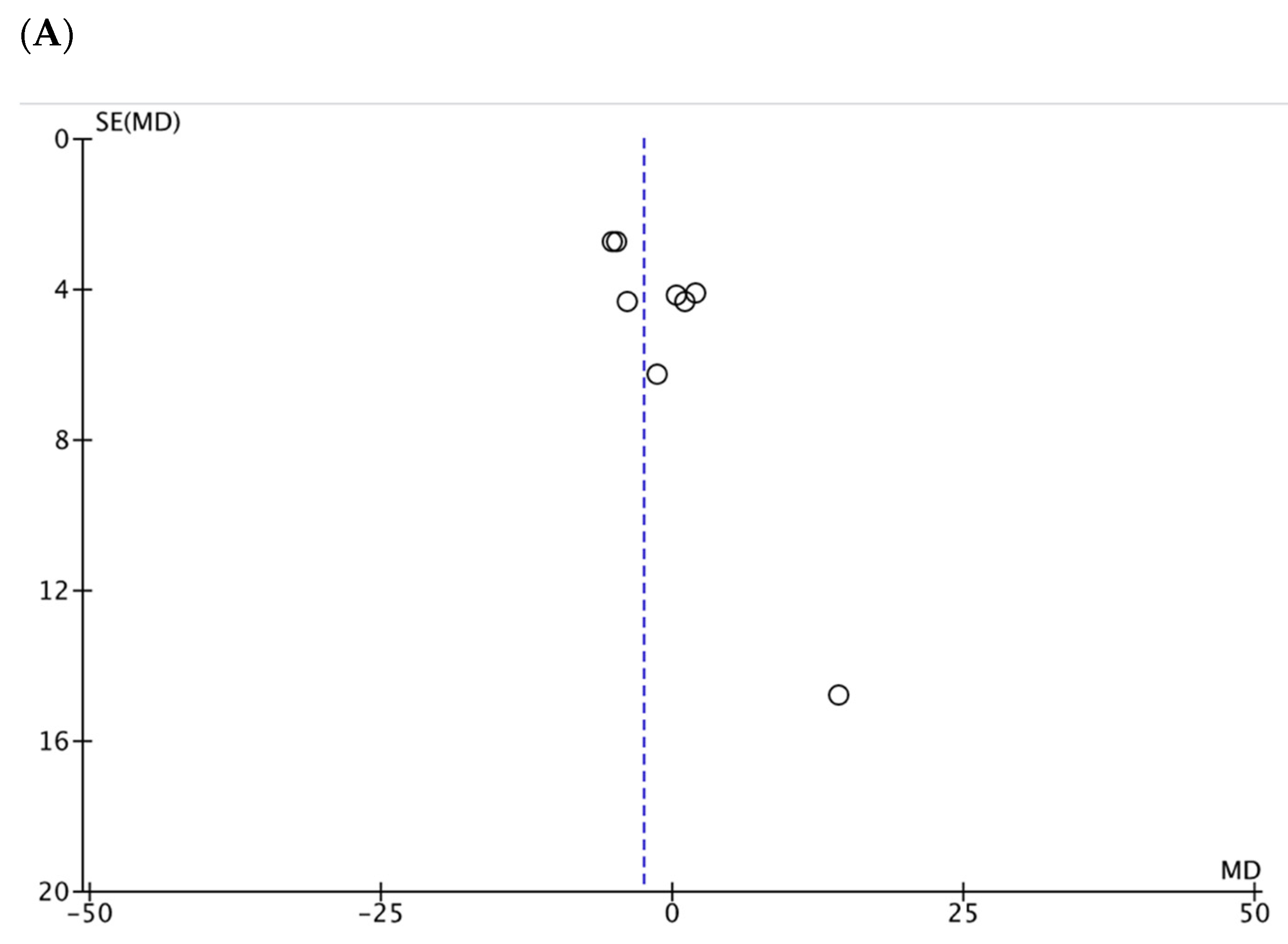
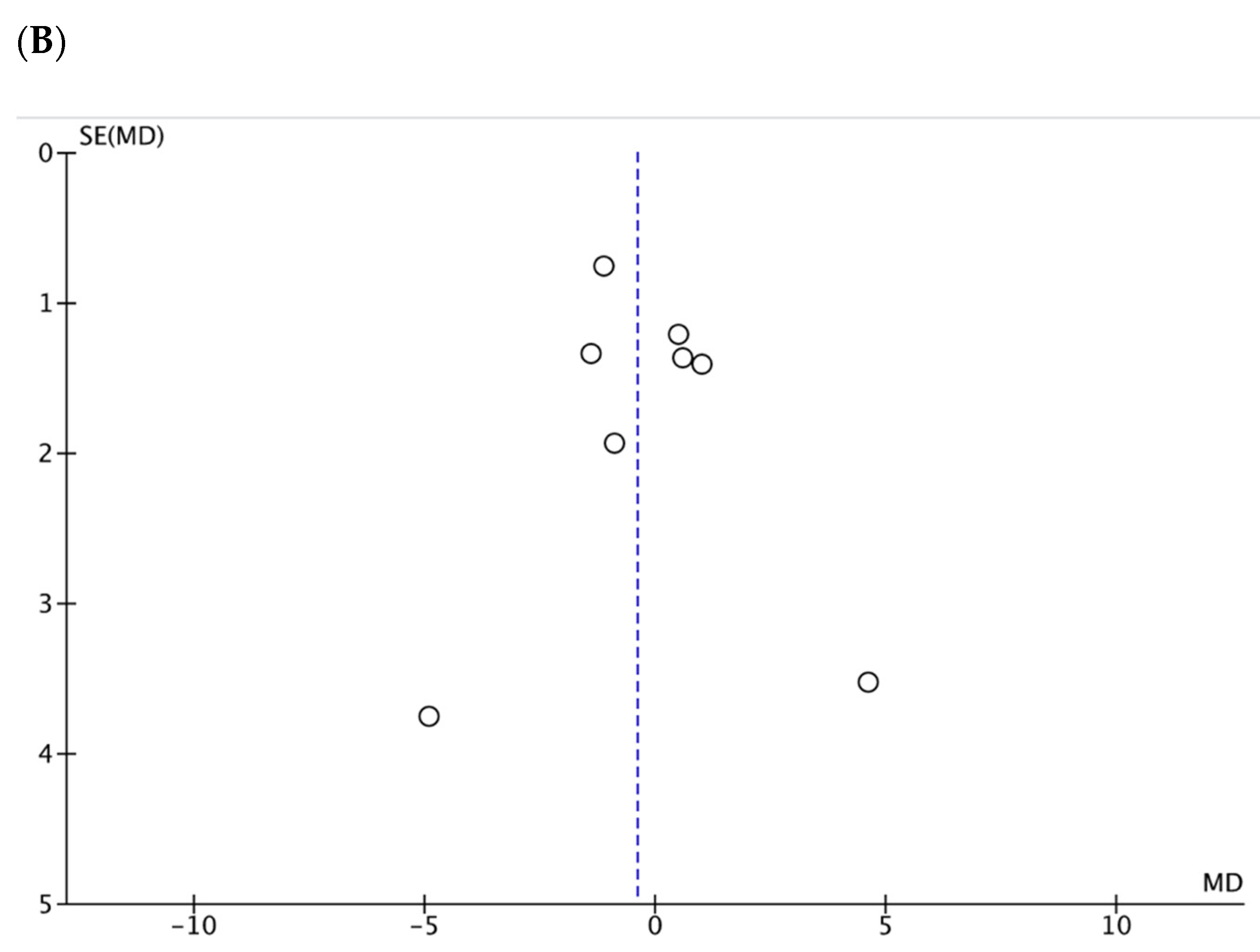
3.5. Meta-Analyses Body Weight and BMI
3.6. Secondary Outcomes
4. Discussion
4.1. Summary of Main Findings
4.2. Implications for Clinical Practice
4.3. Implications for Future Research
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kugler, C.; Einhorn, I.; Gottlieb, J.; Warnecke, G.; Schwarz, A.; Barg-Hock, H.; Bara, C.; Haller, H.; Haverich, A. Postoperative weight gain during the first year after kidney, liver, heart, and lung transplant: A prospective study. Prog. Transplant. 2015, 25, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Saigi-Morgui, N.; Quteineh, L.; Bochud, P.Y.; Crettol, S.; Kutalik, Z.; Wojtowicz, A.; Bibert, S.; Beckmann, S.; Mueller, N.J.; Binet, I.; et al. Weighted Genetic Risk Scores and Prediction of Weight Gain in Solid Organ Transplant Populations. PLoS ONE 2016, 11, e0164443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckmann, S.; Nikolic, N.; Denhaerynck, K.; Binet, I.; Koller, M.; Boely, E.; De Geest, S. Evolution of body weight parameters up to 3 years after solid organ transplantation: The prospective Swiss Transplant Cohort Study. Clin. Transplant. 2017, 31, e12896. [Google Scholar] [CrossRef] [PubMed]
- Kostakis, I.D.; Kassimatis, T.; Bianchi, V.; Paraskeva, P.; Flach, C.; Callaghan, C.; Phillips, B.L.; Karydis, N.; Kessaris, N.; Calder, F.; et al. UK renal transplant outcomes in low and high BMI recipients: The need for a national policy. J. Nephrol. 2020, 33, 371–381. [Google Scholar] [CrossRef]
- Glicklich, D.; Mustafa, M.R. Obesity in Kidney Transplantation: Impact on Transplant Candidates, Recipients, and Donors. Cardiol. Rev. 2019, 27, 63–72. [Google Scholar] [CrossRef]
- Vega, J.; Huidobro, E.J.; De La Barra, S.; Haro, D. Influence of weight gain during the first year after kidney transplantation in the survival of grafts and patients. Rev. Med. Chil. 2015, 143, 961–970. [Google Scholar] [CrossRef]
- Koufaki, P.; Greenwood, S.A.; Macdougall, I.C.; Mercer, T.H. Exercise therapy in individuals with chronic kidney disease: A systematic review and synthesis of the research evidence. Ann. Rev. Nurs. Res. 2013, 31, 235–275. [Google Scholar] [CrossRef]
- Nielens, H.; Lejeune, T.M.; Lalaoui, A.; Squifflet, J.P.; Pirson, Y.; Goffin, E. Increase of physical activity level after successful renal transplantation: A 5 year follow-up study. Nephrol. Dial. Transplant. 2001, 16, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Cashion, A.K.; Hathaway, D.K.; Stanfill, A.; Thomas, F.; Ziebarth, J.D.; Cui, Y.; Cowan, P.A.; Eason, J. Pre-transplant predictors of one yr weight gain after kidney transplantation. Clin. Transplant. 2014, 28, 1271–1278. [Google Scholar] [CrossRef] [Green Version]
- Aksoy, N. Weight Gain After Kidney Transplant. Exp. Clin. Transplant. 2016, 14, 138–140. [Google Scholar]
- Stanfill, A.; Bloodworth, R.; Cashion, A. Lessons learned: Experiences of gaining weight by kidney transplant recipients. Prog. Transplant. 2012, 22, 71–78. [Google Scholar] [CrossRef]
- Stefanović, V.; Milojković, M. Effects of physical exercise in patients with end stage renal failure, on dialysis and renal transplantation: Current status and recommendations. Int. J. Artif. Organs 2005, 28, 8–15. [Google Scholar] [CrossRef]
- Takahashi, A.; Hu, S.L.; Bostom, A. Physical Activity in Kidney Transplant Recipients: A Review. Am. J. Kidney Dis. 2018, 72, 433–443. [Google Scholar] [CrossRef]
- O’Brien, T.; Hathaway, D. An Integrative Literature Review of Physical Activity Recommendations for Adult Renal Transplant Recipients. Prog. Transplant. 2016, 26, 381–385. [Google Scholar] [CrossRef]
- Calella, P.; Hernandez-Sanchez, S.; Garofalo, C.; Ruiz, J.R.; Carrero, J.J.; Bellizzi, V. Exercise training in kidney transplant recipients: A systematic review. J. Nephrol. 2019, 16, 16. [Google Scholar] [CrossRef]
- Oguchi, H.; Tsujita, M.; Yazawa, M.; Kawaguchi, T.; Hoshino, J.; Kohzuki, M.; Ito, O.; Yamagata, K.; Shibagaki, Y.; Sofue, T. The efficacy of exercise training in kidney transplant recipients: A meta-analysis and systematic review. Clin. Exp. Nephrol. 2019, 23, 275–284. [Google Scholar] [CrossRef]
- Chen, G.; Gao, L.; Li, X. Effects of exercise training on cardiovascular risk factors in kidney transplant recipients: A systematic review and meta-analysis. Ren. Fail. 2019, 41, 408–418. [Google Scholar] [CrossRef]
- Palmer, S.C.; Maggo, J.K.; Campbell, K.L.; Craig, J.C.; Johnson, D.W.; Sutanto, B.; Ruospo, M.; Tong, A.; Strippoli, G.F. Dietary interventions for adults with chronic kidney disease. Cochrane Database Syst. Rev. 2017, 4, Cd011998. [Google Scholar] [CrossRef] [Green Version]
- PRISMA. PRISMA Transparent Reporting of Systematic Reviews and Meta-Analyses. Available online: www.prisma-statement.org (accessed on 10 December 2019).
- Richardson, W.; Wilson, M.; Nishikawa, J.; Hayward, R. The well-built clinical question: A key to evidence-based decisions. ACP J Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Thomas, J.; Kneale, D.; McKenzie, J.E.; Brennan, S.E.; Bhaumik, S. Chapter 2: Determining the scope of the review and the questions it will address. In Cochrane Handbook for Systematic Reviews of Interventions Version 6 (Updated July 2019); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane, 2019; Available online: www.training.cochrane.org/handbook (accessed on 1 September 2020).
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2013. [Google Scholar]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- McKenzie, J.; Brennan, S.; Ryan, R.; Thomson, H.; Johnston, R. Chapter 9: Summarizing study characteristics and preparing for synthesis. In Cochrane Handbook for Systematic Reviews of Interventions Version 6 (Updated July 2019); Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; Cochrane, 2019; Available online: www.training.cochrane.org/handbook (accessed on 1 September 2021).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Li, T.; Deeks, J. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions Version 6 (Updated July 2019); Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; Cochrane: London, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 1 September 2020).
- Fu, R.; Holmer, H.K. Change score or follow-up score? Choice of mean difference estimates could impact meta-analysis conclusions. J. Clin. Epidemiol. 2016, 76, 108–117. [Google Scholar] [CrossRef]
- Cochrane UK. The RevMan Calculator: Combining Arms with Continous Outcomes. Available online: https://www.youtube.com/watch?v=jtWVkcKMSBo (accessed on 1 September 2020).
- Rücker, G.; Cates, C.J.; Schwarzer, G. Methods for including information from multi-arm trials in pairwise meta-analysis. Res. Synth. Methods 2017, 8, 392–403. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. RevMan 5.4.1. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download (accessed on 1 September 2020).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.; Higgins, J.; Altman, D. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.1; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Painter, P.L.; Hector, L.; Ray, K.; Lynes, L.; Dibble, S.; Paul, S.M.; Tomlanovich, S.L.; Ascher, N.L. A randomized trial of exercise training after renal transplantation. Transplantation 2002, 74, 42–48. [Google Scholar] [CrossRef]
- Painter, P.L.; Hector, L.; Ray, K.; Lynes, L.; Paul, S.M.; Dodd, M.; Tomlanovich, S.L.; Ascher, N.L. Effects of exercise training on coronary heart disease risk factors in renal transplant recipients. Am. J. Kidney Dis. 2003, 42, 362–369. [Google Scholar] [CrossRef]
- Greenwood, S.A.; Koufaki, P.; Mercer, T.H.; Rush, R.; O’Connor, E.; Tuffnell, R.; Lindup, H.; Haggis, L.; Dew, T.; Abdulnassir, L.; et al. Aerobic or Resistance Training and Pulse Wave Velocity in Kidney Transplant Recipients: A 12-Week Pilot Randomized Controlled Trial (the Exercise in Renal Transplant [ExeRT] Trial). Am. J. Kidney Dis. 2015, 66, 689–698. [Google Scholar] [CrossRef]
- O’Connor, E.M.; Koufaki, P.; Mercer, T.H.; Lindup, H.; Nugent, E.; Goldsmith, D.; Macdougall, I.C.; Greenwood, S.A. Long-term pulse wave velocity outcomes with aerobic and resistance training in kidney transplant recipients—A pilot randomised controlled trial. PLoS ONE 2017, 12, e0171063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leasure, R.; Belknap, D.; Burks, C.; Schlegel, J. The effects of structured exercise on muscle mass, strength, and endurance of immunosuppressed adult renal transplant patients: A pilot study. Rehabil. Nurs. 1995, 4, 47–57. [Google Scholar]
- Jezior, D.; Krajewska, M.; Madziarska, K.; Regulska-Ilow, B.; Ilow, R.; Janczak, D.; Patrzalek, D.; Klinger, M. Weight Reduction in Renal Transplant Recipients Program: The First Successes. Transplant. Proc. 2007, 39, 2769–2771. [Google Scholar] [CrossRef]
- Schmid-Mohler, G.; Zala, P.; Graf, N.; Witschi, P.; Mueller, T.F.; Peter Wuthrich, R.; Huber, L.; Fehr, T.; Spirig, R. Comparison of a Behavioral Versus an Educational Weight Management Intervention After Renal Transplantation: A Randomized Controlled Trial. Transplant. Direct 2019, 5, e507. [Google Scholar] [CrossRef] [Green Version]
- Serper, M.; Barankay, I.; Chadha, S.; Shults, J.; Jones, L.S.; Olthoff, K.M.; Reese, P.P. A randomized, controlled, behavioral intervention to promote walking after abdominal organ transplantation: Results from the LIFT study. Transpl. Int. 2020, 33, 632–643. [Google Scholar] [CrossRef]
- Lawrence, I.R.; Thomson, A.; Hartley, G.H.; Wilkinson, R.; Day, J.; Goodship, T.H.J. The effect of dietary intervention on the management of hyperlipidemia in British renal transplant patients. J. Ren. Nutr. 1995, 5, 73–77. [Google Scholar] [CrossRef]
- Karelis, A.D.; Hébert, M.-J.; Rabasa-Lhoret, R.; Räkel, A. Impact of Resistance Training on Factors Involved in the Development of New-Onset Diabetes After Transplantation in Renal Transplant Recipients: An Open Randomized Pilot Study. Can. J. Diabetes 2016, 40, 382–388. [Google Scholar] [CrossRef]
- Sharif, A.; Moore, R.; Baboolal, K. Influence of lifestyle modification in renal transplant recipients with postprandial hyperglycemia. Transplantation 2008, 85, 353–358. [Google Scholar] [CrossRef]
- Kuningas, K.; Driscoll, J.; Mair, R.; Smith, H.; Dutton, M.; Day, E.; Sharif, A. Comparing glycaemic benefits of active versus passive lifestyle intervention in kidney allograft recipients (CAVIAR): A randomised controlled trial. Transplantation 2019, 104, 1491–1499. [Google Scholar] [CrossRef]
- Tzvetanov, I.; West-Thielke, P.; D’Amico, G.; Johnsen, M.; Ladik, A.; Hachaj, G.; Grazman, M.; Heller, R.U.; Fernhall, B.; Daviglus, M.L.; et al. A novel and personalized rehabilitation program for obese kidney transplant recipients. Transplant. Proc. 2014, 46, 3431–3437. [Google Scholar] [CrossRef]
- Lorenz, E.C.; Amer, H.; Dean, P.G.; Stegall, M.D.; Cosio, F.G.; Cheville, A.L. Adherence to a pedometer-based physical activity intervention following kidney transplant and impact on metabolic parameters. Clin. Transplant. 2015, 29, 560–568. [Google Scholar] [CrossRef]
- Teplan, V.; Mahrova, A.; Pitha, J.; Racek, J.; Gurlich, R.; Teplan, V., Jr.; Valkovsky, I.; Stollova, M. Early exercise training after renal transplantation and asymmetric dimethylarginine: The effect of obesity. Kidney Blood Press. Res. 2014, 39, 289–298. [Google Scholar] [CrossRef]
- Patel, M.G. The effect of dietary intervention on weight gains after renal transplantation. J. Ren. Nutr. 1998, 8, 137–141. [Google Scholar] [CrossRef]
- Gibson, C.A.; Gupta, A.; Greene, J.L.; Lee, J.; Mount, R.R.; Sullivan, D.K. Feasibility and acceptability of a televideo physical activity and nutrition program for recent kidney transplant recipients. Pilot Feasibility Stud. 2020, 6, 126. [Google Scholar] [CrossRef]
- Henggeler, C.K.; Plank, L.D.; Ryan, K.J.; Gilchrist, E.L.; Casas, J.M.; Lloyd, L.E.; Mash, L.E.; McLellan, S.L.; Robb, J.M.; Collins, M.G. A Randomized Controlled Trial of an Intensive Nutrition Intervention Versus Standard Nutrition Care to Avoid Excess Weight Gain After Kidney Transplantation: The INTENT Trial. J. Ren. Nutr. 2018, 28, 340–351. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Schut, H.A.; Stam, H.J. Goals in rehabilitation teamwork. Disabil. Rehabil. 1994, 16, 223–226. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cogntive Theory; Prentice-Hall Inc: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef]
- Chiarotto, A.; Ostelo, R.W.; Turk, D.C.; Buchbinder, R.; Boers, M. Core outcome sets for research and clinical practice. Braz. J. Phys. Ther. 2017, 21, 77–84. [Google Scholar] [CrossRef]
- Conley, M.M.; McFarlane, C.M.; Johnson, D.W.; Kelly, J.T.; Campbell, K.L.; MacLaughlin, H.L. Interventions for weight loss in people with chronic kidney disease who are overweight or obese. Cochrane Database Syst. Rev. 2021, 3, Cd013119. [Google Scholar] [CrossRef] [Green Version]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.; Siminoff, L.A. Self-care strategies and barriers among kidney transplant recipients: A qualitative study. Chronic Illn. 2009, 5, 75–91. [Google Scholar] [CrossRef] [Green Version]
- Zelle, D.M.; Corpeleijn, E.; Klaassen, G.; Schutte, E.; Navis, G.; Bakker, S.J. Fear of Movement and Low Self-Efficacy Are Important Barriers in Physical Activity after Renal Transplantation. PLoS ONE 2016, 11, e0147609. [Google Scholar] [CrossRef]
- Möhler, R.; Köpke, S.; Meyer, G. Criteria for Reporting the Development and Evaluation of Complex Interventions in healthcare: Revised guideline (CReDECI 2). Trials 2015, 16, 204. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Ju, A.; Josephson, M.A.; Butt, Z.; Jowsey-Gregoire, S.; Tan, J.; Taylor, Q.; Fowler, K.; Dobbels, F.; Caskey, F.; Jha, V.; et al. Establishing a Core Outcome Measure for Life Participation: A Standardized Outcomes in Nephrology-kidney Transplantation Consensus Workshop Report. Transplantation 2019, 103, 1199–1205. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, J.K.; Campbell, Z.C.; Webster, A.C.; Chow, C.K.; Tong, A.; Craig, J.C.; Campbell, K.L.; Lee, V.W.S. eHealth interventions for people with chronic kidney disease. Cochrane Database Syst. Rev. 2019, 8. [Google Scholar] [CrossRef] [Green Version]
- British Transplant Society. BTS Information for Transplant Professionals, 13th ed. Available online: https://renal.org/covid-19/ (accessed on 1 June 2021).
- Fry, K.; Patwardhan, A.; Ryan, C.; Trevillian, P.; Chadban, S.; Westgarth, F.; Chan, M. Development of evidence-based guidelines for the nutritional management of adult kidney transplant recipients. J. Ren. Nutr. 2009, 19, 101–104. [Google Scholar] [CrossRef]
- Nolte Fong, J.V.; Moore, L.W. Nutrition Trends in Kidney Transplant Recipients: The Importance of Dietary Monitoring and Need for Evidence-Based Recommendations. Front. Med. 2018, 5, 302. [Google Scholar] [CrossRef] [Green Version]
- Castle, E.M.; Greenwood, J.; Chilcot, J.; Greenwood, S.A. Usability and experience testing to refine an online intervention to prevent weight gain in new kidney transplant recipients. Br. J. Health Psychol. 2020, 26, 232–255. [Google Scholar] [CrossRef] [PubMed]
- Ducloux, D.; Kazory, A.; Simula-Faivre, D.; Chalopin, J.M. One-year post-transplant weight gain is a risk factor for graft loss. Am. J. Transplant. 2005, 5, 2922–2928. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICO(s) | Inclusion | Exclusion | Reasons for Exclusion |
|---|---|---|---|
| Population | KTRs within the first 12 months of transplantation | >12 months post-transplant <18 years of age Mixed samples (e.g., dialysis and transplant patients) | WG occurs within first year Different populations (adults vs. paediatric) Difficult to isolate effects to just KTR in mixed sample unless information provided by authors |
| Intervention | Complex interventions involving either exercise, activity, nutrition, diet, behaviour-change, or combined interventions designed to prevent WG occurring | Treatments including pharmacological intervention | Difficult to isolate effects of the other components of the treatment |
| Comparator | Usual care or standard care or no intervention | No comparator available | Difficult to determine the treatment effect(s) |
| Outcomes-Primary outcome | WG from baseline to short term (3 months) baseline to long term (6–12 months) | No reported BW or BMI at baseline or follow-up (3–12 months) | Unable to determine change in BW or BMI |
| Study Types | RCTs, non-RCTs (quasi-experimental) | Exclude literature reviews Exclude trials with no control group | Outside scope of this review |
| Language | English | Limited resources for this project | |
| Year | Published after 1985 | Changes to standards of care |
| First Author, Year (Country of Origin) | Study Duration (Months) | Sample | Groups | Outcomes (Primary and Secondary) | Results (for Primary and Secondary Outcomes) | Comments |
|---|---|---|---|---|---|---|
| Lawrence et al. [45] (UK) | 12 | n = 38, KTRs with hyperlipidaemia | IG: Dietitian only for 12 months CG: Usual care, no dietary intervention | Primary: Dietary intake (24-h recall assessed for total energy intake, fibre intake, protein, carbohydrate, fat and distribution of fat intake) and fasting lipids Secondary: BW, BMI, medications, Renal function | Primary: No significant difference between groups in total cholesterol, HDL cholesterol, or plasma triglyceride levels LDL cholesterol was significantly lower in the IG at 1 month after Tx Significant improvement in polyunsaturated-to-unsaturated fat ratio in the IG Change in dietary intake not associated with changes in serum lipid levels Fibre intake significantly higher at 3 months in the IG Secondary: No difference in BMI, medication, or kidney function between groups at any time Both groups reduced average consumption of cigarettes and alcohol | AEs not reported Limited reporting of blinding, allocation, analysis plan, treatment, protocol deviations, and statistical plan |
| Painter et al. [36] (USA) | 12 | n = 167 | IG: 12-months ET, home based AT CG: no ET | Primary: Not stated Secondary: VO2 peak, Muscle strength, BC (DEXA), QoL (SF-36), PA reporting (active or inactive) | Primary/Secondary: No difference in BW, BMI, or BC, all participants increased BW, BMI, FM, LTM, % FM IG had greater gains in VO2 peak and muscle strength IG had higher % classified as active at follow-up No difference in QoL | AEs not reported High dropout rate 42% did not complete assessment at all three timepoints Painter 2003 duplicate paper from this study |
| Tzvetanov et al. [49] (USA) | 12 | n = 17, Obese KTRs | IG: 12-month combined Rx (lifestyle, exercise, behaviour, and nutrition guidance) CG: Nutritional guidance only | Primary: Not stated? feasibility Secondary: Physical (weightlifting capacity) and vascular function (PWV and CiMT), BC, QoL (SF-36), kidney function, blood lipid markers, and adherence | Primary/Secondary: No significant difference in BMI at 12 months Greater adherence to follow-up in IG (100%) vs. CG (25%) Improved weightlifting and PWV (IG only) significant difference in CiMT (IG only) Improvement in QoL (p = 0.008) and employment rate (p = 0.02) in IG vs. CG No significant differences between groups in kidney function or lipids | AEs not reported Small sample t-tests used, not ITT High dropouts in CG vs. IG Missing data (BC, PWV, CiMT) in CG |
| Karelis et al. [46] (Canada) | ≈4 | n = 24, non-diabetic KTRs, excluded smoking history | IG: Exercise only for 16 weeks (RT)CG: Instructed not to perform any structured exercise | Primary: Feasibility outcomes (adherence, injuries, drop-outs) Secondary: BC (DEXA), OGTT, Lipid profile, BP, QoL, Anthropometrics, Muscle strength (leg press), VO2 peak | Primary: 47% consent rate 80% compliance IG 17% dropout IG Secondary: No difference in BW or BMI, BC, VO2 peak, lipids, OGTT or QoL Both groups increased FM (BC) IG associated with increase in muscle strength (p = 0.003) | No AEs or injuries reported Short study duration (16 weeks) Small sample size |
| O’Connor et al. [39] (UK) | 12 | n = 47 of the original 60 ExeRT cohort [38] | IG1: Supervised AT for 12 weeks IG2:Supervised RT for 12 weeks CG: No ET for 12 weeks | Primary: PWV and VO2 peak Secondary: Anthropometrics, BP | Primary: Significant difference in PWV in IG2 (RT) vs. CG (p = 0.03) Favourable difference in VO2 peak IG1 (AT) vs. CG (p = 0.02) Secondary: No difference between-groups in BW or BP BMI not reported No difference in BMI reported in original study manuscript [38] | No AEs Long-term follow-up data from the ExeRT cohort [38] Dropouts ANCOVA used |
| Henggeler et al. [54] (NZ) | 12 | n = 37 KTRs with a BMI of > 18.5 and <40 kg/m2 | IG: 12-month combined Rx including standard care + dietitian appointments (12 sessions in total) and exercise sessions CG: Standard care (4 sessions in 12 months) with renal dietitian | Primary: BW at 6 months adjusted for baseline weight, obesity, and gender Secondary: Change in Anthropometrics and BC (DEXA), resting energy expenditure, physical function (grip, 25-feet gait speed, STS), PA (NZ PA questionnaire), serum biochem, QoL (SF-36) | Primary: No significant difference in BW or BC between groups at 6 months Secondary: No between-group difference in BC or energy expenditure Both groups increased total body fat and % body fat No significant difference in biochemistry Whole sample HbA1c and fasting glucose increased, cholesterol decreased Whole sample improved physical function, body protein, and QoL | No AEs CG greater than clinical practice in the UK May require formal ET/PA to elicit training response ANCOVA used |
| Kuningas et al. 2019 [48] (UK) | 6 | n = 130 nondiabetic KTRs | IG: 6-month exercise and nutrition education +BCTs CG: Passive education (booklet) on healthy eating, exercise, and risks of PTDM | Primary: 6-month change in insulin sensitivity, secretion, and disposition index (OGTT) Secondary: PA (GPPAQ), Physical function (DASI), QoL (EQ-5D), Beck depression inventory, situational motivational score, safety issues, BW, BC (skinfolds and bioimpedance) | Primary: No between-group difference in 6-month glucose metabolism Secondary: Significant between-group difference in BW favouring IG vs. UC (p = 0.02) Significant between-group difference in FM IG vs. CG (p = 0.03) Clinically significant reduction in PTDM, halved in IG vs. CG No between-group difference in any questionnaires | No safety concerns Dropout out rate 20.8% Pre–post study design with no long-term follow up Excluded non-diabetic KTRs Single centre study No reporting of BMI at 6 months |
| Schmid-Mohler et al. [43] (Switzerland) | 12 | n = 123 KTR and Kidney-pancreas Tx (120 KTR) | IG: Control + 8-month nurse-led intervention including dietary and PA counselling with motivational interviewing and action planning CG: A single nurse-led education session with booklet | Primary: Difference in BMI (baseline to 8 months) in patients with a BMI of ≥18.5 kg/m2 Secondary: change in BMI baseline to 12 months, Rx adherence, satisfaction with counselling, BC (bioimpedance), PA (IPAQ), patient assessment of chronic illness care PACIC) | Primary: No significant between-group difference in change in BMI or BC from baseline to 8 months, or Baseline to 12 months Secondary: No significant differences between-group in BC, steps or IPAQ IG more chronic care related activities (PACIC) High acceptability IG 88.5% IG received ≥7 sessions Significant difference in PACIC in all but one score IG vs. CG No difference between groups in satisfaction with counselling | AEs not reported Sample includes kidney-pancreas Tx Means and SD for KTR (n = 120) provided on request. There was no significant between-group in BW or BMI at any timepoint in KTRs |
| Serper et al. [44] (USA) | 4 | n = 127 KTR and Liver Transplants (65 KTR). Participants needed to own a smartphone compatible with wearable accelerometer | IG1: Device only group, access to online portal with education materials and questions + control education IG2: Control education + Intervention 1 + 2 plus bi-weekly texts, step goals and financial incentives CG: standard education on healthy diet, food hygiene and PA | Primary: Change in BW from baseline to 4 months Secondary: Daily steps—proportion of patients achieving > 7000 steps/day, and continuous daily step data | Primary: No significant difference in weight gain between all three groups (IG1, IG2 and CG) Secondary: Significantly higher step count reported in IG2 vs. IG1 (p < 0.001) Retention rate 92.1% Adherence final study weight assessment 88% 74% IG2 adhered to their step targets Study increased motivation to monitor weight and increase PA Some participants disappointed with randomisation Some IG patients requested ability to track different activities, and have non-step related goals | No AEs associated with study Combined sample (KTR and Liver Transplant) Unique approach with financial incentives Diet education not designed for weight management No longer-term follow-up BMI not reported |
| Gibson et al. [53] (USA) | 6 | n = 10 KTR, 6–12 months post-transplant, Mean age 44 years, BMI >22 kg/m2, | IG: 6-month combined Rx via telehealth (dietitian-led, 12 weeks of one-hour weekly calls and PA classes). Followed by 12 weeks of maintenance. Provided with tablet to track food and veg intake, whole grains intake, water intake, steps, and PA weekly CG: Standardised education to follow healthy eating and PA. Provided with tablet and tracking (as above). Did not receive weekly video calls or PA classes | Primary: Primary outcomes relate to feasibility (recruitment, adherence, attendance) Secondary: Provide estimates of Rx effectiveness including changes to PA, food intake (fruit, veg, whole-grain, and water). Secondary outcomes included weight gain (baseline to six months), BW, BMI, BP, PA (accelerometer), QoL, Dietary intake (3-day food diary), qualitative interviews for strengths and weakness of intervention | Primary: 78% attendance telehealth sessions (IG) 86% adherence to weekly behaviour tracking via tablet All patients attended week 12 study assessments Tracking increased awareness but some had problems All would recommend trial to others Tailored education and the ability to complete Rx at home was valued Secondary: Weight gain and BMI greater in IG versus CHG QoL improvements greater in CG versus IG No difference in BP and PA between groups Improved diet quality in both groups | Specific recruitment criteria included the ability to take part in six-month trial, ability to report data weekly (by phone, fax, email), access to the internet, English speaking, willingness to be randomised One participant withdrew due to time commitments |
| Study | Rx type | Rx Description | Rx Behaviour Components | Provider | Duration (Months) | Frequency | Intensity | Type of ET | Time (Minutes) |
|---|---|---|---|---|---|---|---|---|---|
| Lawrence et al. [45] | Diet | Written and verbal edu to reduce hyperlipidaemia Diet: 30% total energy from fat and 50% from carbohydrates Mode: NI, assume F2F | NI | RD | 12 s | NI | NA | NA | NA |
| Painter et al. [36] | Exercise | Home ET (independent) Fortnightly phone calls Mode: Telephone | Self-monitoring behaviour (diaries) Phone calls for encouragement | NI | 12 | 4x week | 60–65% HRM, ⬆ 75–80% HRM | AT | ≥30 |
| Tzvetanov et al. [49] | Combined | Combination of 1:1 ET + CBT + nutrition Topics include reduce sodium, emotional eating, increase protein, reduce cholesterol, and balanced meals Aims of Rx; build muscle tissue, change thoughts, and empowerment Mode: F2F | CBT details not provided | P.Tr | 12 | ET 2x week | Not specified | RT | 60 |
| Karelis et al. [46] | Exercise | ET programme of 7 exercises Upper and lower limb RT Mode: F2F supervised | NI | Kinesiology student | 16 weeks (≈3.68 months) | 3x week (1x week supervised) | 80% 1RM | RT | 45–60 |
| O’Connor et al. [39] | Exercise | 2 intervention groups; AT and RT compared with UC Mode: F2F | Motivational interviewing | PT | 3 | 3x week (2x supervised group, 1x not supervised) | AT: 80% HRR RT: 80% 1RM 1–2 sets 10 reps, ⬆ to 3 sets | AT or RT vs. UC | 60 AT or RT 30 min/week edu (AT and RT) |
| Henggeler et al. [54] | Combined | Multi-professional and components 12 sessions (4x UC sessions, plus 8 additional nutrition sessions) with RD Exercise and PA component Mode: NI, assume F2F | SMART goal setting and revision of goals Motivational interviewing Action planning Self-monitoring | RD Ex.Phys: ET and PA | 12 | 12x RD follow-ups 3x ET with Ex.Phys | ‘Tailored PA advice’, No further detail | NI | NI PA |
| Kuningas et al. [48] | Combined | Combined lifestyle Rx to prevent PTDM, Dietary habits, Personalised healthy eating, edu based on Diabetes UK and Public Health England, Graded ET, Exercise diary, Mode: F2F and phone follow-up | BCTs used: Information on consequences, feedback on personal information prompting intention formation, SMART goals, graded tasks, self-monitoring, revision of goals, social support | RD | 6 | 4x F2F 1:1 with RD RD phone consultant between each F2F session | Specifics not Reported | AT | NI |
| Schmid-Mohler et al. [43] | Combined | Developed brochure edu food types and hygiene, and encouraging PA Initial 1:1 edu session with brochure as per UC group +8 APN-led sessions Mode: F2F or phone | BCTs used: goal setting, problem solving, action planning, review behaviour and outcome goals, feedback on behaviour, self-monitoring of behaviour, instruction on how to perform behaviour, information about health consequences, prompts/cues, habit formation and reversal, focus on past success, self-monitoring of behaviour social support | APN (trained in motivational interviewing) | 8 | Combination of F2F and phone follow-up 9 sessions in total. | Specifics PA not reported | NI | 35 |
| Serper et al. [44] | Combined + online | IG1: Device only: Step-counting device, Website with resources on healthy eating and PA, Health knowledge questionnaires Mode: online IG2. Device and Rx: As above + Financial incentives, + Automated step goals, + Bi-weekly text messages, for health questionnaire Mode: online and text | prompts/cues (text), financial incentives (rewards) | 1. Website 2. website and text messages (automated) by research team | 14 weeks (≈3.22 months) | 1. Online website, step-recording device 2. online website, step-recording device and text support | 1. Device only—no prescription 2. Device and Rx: baseline steps increased 15% every 2 weeks until reached 7000 steps/day | AT- steps | NI |
| Gibson et al. [53] | Combined +tracking +video calls | both groups given tablets for weekly tracking (fruit/veg, wholegrains, water, steps, and PA) IG: 6-months video calls: Tracking, 12 weeks of diet Edu (DASH diet), 12 weeks group PA, 12 weeks maintenance using tracking only Mode: video calls | Rx informed by the Social Cognitive Theory [57] and self-efficacy [58] Self-monitoring Goal setting | Tracking (not supervised) on tablet Diet Edu (RD), group PA (exercise professional) | 6 | Weekly | Moderate intensity (3–6 metabolic equivalent of task) | NI | Diet 1:1 and group PA 30 min/week (total 60 min/week) Encouraged to do 10–15 min PA/day |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castle, E.M.; McBride, E.; Greenwood, J.; Bramham, K.; Chilcot, J.; Greenwood, S.A. Do Exercise, Physical Activity, Dietetic, or Combined Interventions Improve Body Weight in New Kidney Transplant Recipients? A Narrative Systematic Review and Meta-Analysis. Kidney Dial. 2021, 1, 100-120. https://doi.org/10.3390/kidneydial1020014
Castle EM, McBride E, Greenwood J, Bramham K, Chilcot J, Greenwood SA. Do Exercise, Physical Activity, Dietetic, or Combined Interventions Improve Body Weight in New Kidney Transplant Recipients? A Narrative Systematic Review and Meta-Analysis. Kidney and Dialysis. 2021; 1(2):100-120. https://doi.org/10.3390/kidneydial1020014
Chicago/Turabian StyleCastle, Ellen M., Emily McBride, James Greenwood, Kate Bramham, Joseph Chilcot, and Sharlene A. Greenwood. 2021. "Do Exercise, Physical Activity, Dietetic, or Combined Interventions Improve Body Weight in New Kidney Transplant Recipients? A Narrative Systematic Review and Meta-Analysis" Kidney and Dialysis 1, no. 2: 100-120. https://doi.org/10.3390/kidneydial1020014
APA StyleCastle, E. M., McBride, E., Greenwood, J., Bramham, K., Chilcot, J., & Greenwood, S. A. (2021). Do Exercise, Physical Activity, Dietetic, or Combined Interventions Improve Body Weight in New Kidney Transplant Recipients? A Narrative Systematic Review and Meta-Analysis. Kidney and Dialysis, 1(2), 100-120. https://doi.org/10.3390/kidneydial1020014