




Long COVID as a Possible Contributor to Rising Suicide Mortality in Bharat (India): An Analysis of Suicide Trends Since the Emergence of COVID-19


Abstract
1. Introduction
2. Methods
3. Results
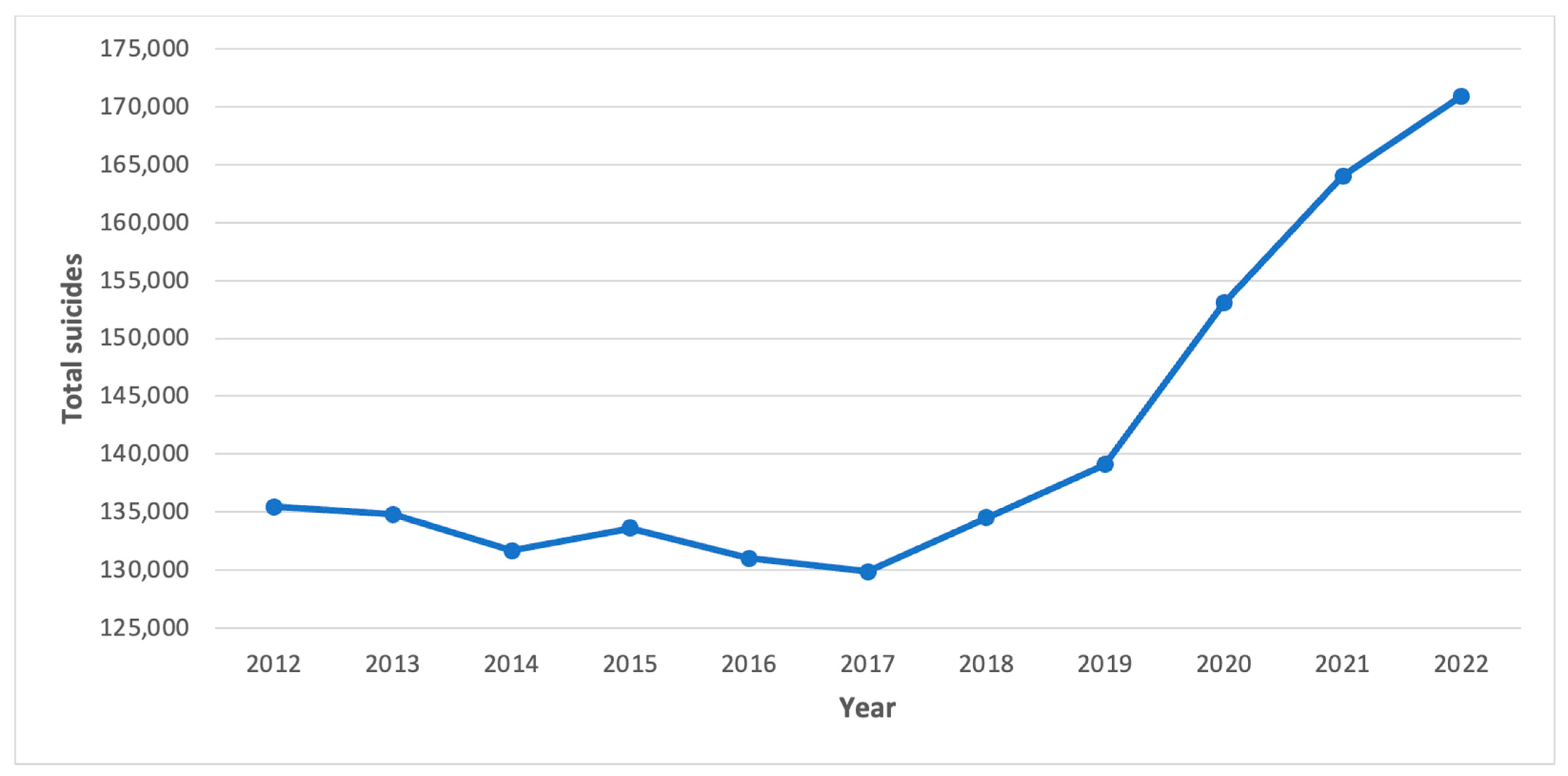
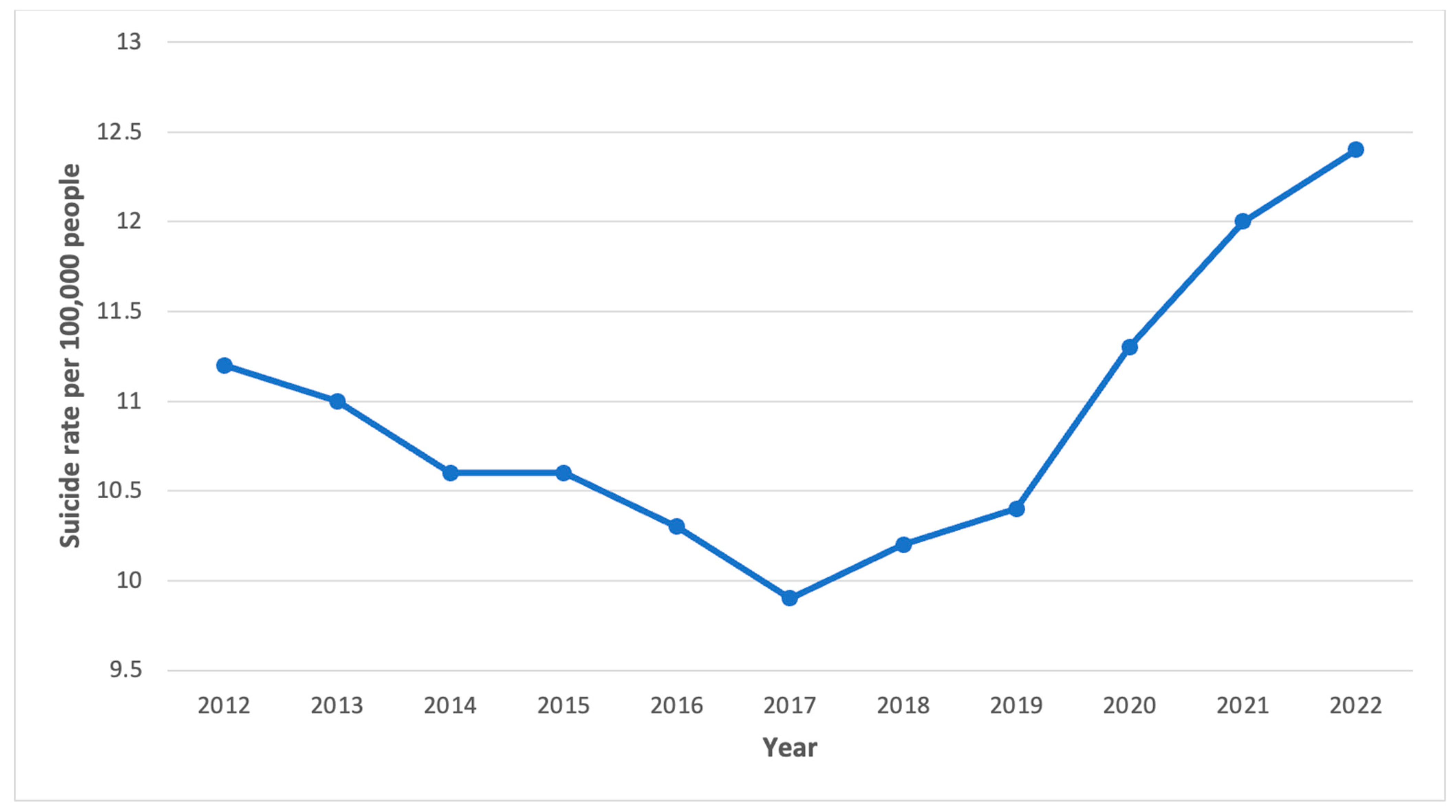
3.1. National Suicide Trends
3.2. State Level Trends—Total Suicides
3.3. State Level Trends—Suicide Rates
3.4. Associations with COVID-19 Caseload and Deaths
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide [Internet]. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 7 June 2024).
- Chan, Y.Y.; Lim, K.H.; Teh, C.H.; Kee, C.C.; Ghazali, S.M.; Lim, K.K.; Khoo, Y.Y.; Tee, E.O.; Ahmad, N.A.; Ibrahim, N. Prevalence and risk factors associated with suicidal ideation among adolescents in Malaysia. Int. J. Adolesc. Med. Health 2018, 30, 20160053. [Google Scholar] [CrossRef]
- Nandini, N.; Chaube, N.; Dahiya, M.S. Psychological review of suicide stories of celebrities: The distress behind contentment. IJHW 2018, 9, 280–285. [Google Scholar]
- Suokas, J.; Suominen, K.; Isometsä, E.; Ostamo, A.; Lönnqvist, J. Long-term risk factors for suicide mortality after attempted suicide-Findings of a 14-year follow-up study. Acta Psychiatr. Scand. 2001, 104, 117–121. [Google Scholar] [CrossRef]
- Beautrais, A.L. Risk factors for suicide and attempted suicide among young people. Aust. N. Z. J. Psychiatry 2000, 34, 420–436. [Google Scholar] [CrossRef]
- Conwell, Y.; Duberstein, P.R.; Caine, E.D. Risk factors for suicide in later life. Biol. Psychiatry 2002, 52, 193–204. [Google Scholar] [CrossRef]
- Vijayakumar, L.; Chandra, P.S.; Kumar, M.S.; Pathare, S.; Banerjee, D.; Goswami, T.; Dandona, R. The national suicide prevention strategy in India: Context and considerations for urgent action. Lancet Psychiatry 2022, 9, 160–168. [Google Scholar] [CrossRef]
- Radhakrishnan, R.; Andrade, C. Suicide: An Indian perspective. Indian J. Psychiatry 2012, 54, 304–319. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Senapati, R.E.; Jena, S.; Parida, J.; Panda, A.; Patra, P.K.; Pati, S.; Kaur, H.; Acharya, S.K. The patterns, trends and major risk factors of suicide among Indian adolescents—A scoping review. BMC Psychiatry 2024, 24, 35. [Google Scholar] [CrossRef]
- World Health Organization. Number of COVID-19 Deaths Reported to WHO (Cumulative Total). WHO. [Internet]. Available online: https://data.who.int/dashboards/covid19/deaths?n=o (accessed on 5 June 2024).
- Salvatore, M.; Basu, D.; Ray, D.; Kleinsasser, M.; Purkayastha, S.; Bhattacharyya, R.; Mukherjee, B. Comprehensive public health evaluation of lockdown as a non-pharmaceutical intervention on COVID-19 spread in India: National trends masking state-level variations. BMJ Open 2020, 10, e041778. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Mamun, M.A.; Griffiths, M.D. PTSD-related suicide six years after the Rana Plaza collapse in Bangladesh. Psychiatry Res. 2019, 287, 112645. [Google Scholar] [CrossRef]
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Mani, V.E.; Kumar, R.; Srivastava, A.K.; Sarkar, Z.; Babu, G.N.; Tandon, R.; Paliwal, V.K.; Jha, S. The Psychosocial Impact of COVID-19 on an Adult Indian Population. Cureus 2023, 15, e38504. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ministry of Health and Family Welfare. National Comprehensive Guidelines for Management of Post Covid Sequelae [Internet]. Government of India. Available online: https://www.mohfw.gov.in/pdf/NationalComprehensiveGuidelinesforManagementofPostCovidSequelae.pdf (accessed on 7 June 2024).
- Taquet, M.; Geddes, J.R.; Husain, M.; Luciano, S.; Harrison, P.J. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospective cohort study using electronic health records. Lancet Psychiatry 2021, 8, 416–427. [Google Scholar] [CrossRef]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an acute to chronic disease? Potential long-term health consequences. Crit. Rev. Clin. Lab. Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef]
- Anaya, J.M.; Rojas, M.; Salinas, M.L.; Rodríguez, Y.; Roa, G.; Lozano, M.; Rodríguez-Jiménez, M.; Montoya, N.; Zapata, E.; Monsalve, D.M.; et al. Post-COVID syndrome. A case series and comprehensive review. Autoimmun. Rev. 2021, 20, 102947. [Google Scholar] [CrossRef]
- Chaudhry, D.; Khandelwal, S.; Bahadur, C.; Daniels, B.; Bhattacharyya, M.; Gangakhedkar, R.; Desai, S.; Das, J.; Gupta, U.; Singh, V.; et al. Prevalence of long COVID symptoms in Haryana, India: A cross-sectional follow-up study. Lancet Reg. Health-Southeast Asia 2024, 25. [Google Scholar] [CrossRef]
- Arjun, M.C.; Singh, A.K.; Roy, P.; Ravichandran, M.; Mandal, S.; Pal, D.; Das, K.; Gajjala, A.; Venkateshan, M.; Mishra, B.; et al. Long COVID following Omicron wave in Eastern India—A retrospective cohort study. J. Med. Virol. 2023, 95, e28214. [Google Scholar] [CrossRef]
- National Crime Records Bureau (NCRB). Accidental Deaths & Suicides in India (ADSI)—2018. Government of India. Available online: https://www.data.gov.in/catalog/accidental-deaths-suicides-india-adsi-2018?page=3 (accessed on 11 September 2024).
- National Crime Records Bureau (NCRB). Accidental Deaths & Suicides in India (ADSI)—2019. Government of India. Available online: https://www.data.gov.in/catalog/accidental-deaths-suicides-india-adsi-2019 (accessed on 11 September 2024).
- National Crime Records Bureau (NCRB). Accidental Deaths & Suicides in India (ADSI)—2020. Government of India. Available online: https://www.data.gov.in/catalog/accidental-deaths-suicides-india-adsi-2020 (accessed on 11 September 2024).
- National Crime Records Bureau (NCRB). Accidental Deaths & Suicides in India (ADSI)—2021. Government of India. Available online: https://www.data.gov.in/catalog/accidental-deaths-suicides-india-adsi-2021 (accessed on 11 September 2024).
- National Crime Records Bureau (NCRB). Accidental Deaths & Suicides in India (ADSI)—2022. Government of India. Available online: https://www.data.gov.in/catalog/accidental-deaths-suicides-india-adsi-2022 (accessed on 11 September 2024).
- MOHFW. COVID-19 Dashboard. Government of India. COVID-19. Available online: https://covid19dashboard.mohfw.gov.in/ (accessed on 11 September 2024).
- IBM Corp. IBM SPSS Statistics for Windows; Version 28 IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Varshney, K.; Patel, H.; Kamal, S. Trends in Tuberculosis Mortality Across India: Improvements Despite the COVID-19 Pandemic. Cureus 2023, 15, e38313. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Varshney, K.; Mustafa, A.D. Trends in HIV incidence and mortality across Bharat (India) after the emergence of COVID-19. Int. J. STD AIDS 2024, 35, 865–872. [Google Scholar] [CrossRef]
- Garg, K.; Kumar, C.N.; Chandra, P.S. Number of psychiatrists in India: Baby steps forward, but a long way to go. Indian J. Psychiatry 2019, 61, 104–105. [Google Scholar]
- Longkumer, N. Traditional Healing Practices and Perspectives of Mental Health in Nagaland. 2020. Available online: https://repository.tribal.gov.in/handle/123456789/74195 (accessed on 4 June 2024).

{kind=link}
{kind=link}
| State/Union Territory | Number of Suicides | Absolute Increase/Decrease | Percent Increase/Decrease | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2021 | 2022 | 2018–2019 | 2019–2022 (Average Annual Change) | 2018–2019 | 2019–2022 (Average Annual Change) | |
| Andhra Pradesh | 5319 | 6465 | 7043 | 8067 | 8908 | 1146 | 814.33 | 21.55 | 12.60 |
| Arunachal Pradesh | 132 | 112 | 160 | 160 | 149 | −20 | 12.33 | −15.15 | 11.01 |
| Assam | 2379 | 2370 | 3243 | 3262 | 3320 | −9 | 316.67 | −0.38 | 13.36 |
| Bihar | 443 | 641 | 809 | 827 | 702 | 198 | 20.33 | 44.70 | 3.17 |
| Chhattisgarh | 7046 | 7629 | 7710 | 7828 | 8446 | 583 | 272.33 | 8.27 | 3.57 |
| Goa | 256 | 259 | 308 | 321 | 302 | 3 | 14.33 | 1.17 | 5.53 |
| Gujarat | 7793 | 7655 | 8050 | 8789 | 9002 | −138 | 449.00 | −1.77 | 5.87 |
| Haryana | 3547 | 4191 | 4001 | 3692 | 3783 | 644 | −136.00 | 18.16 | −3.25 |
| Himachal Pradesh | 740 | 584 | 857 | 889 | 644 | −156 | 20.00 | −21.08 | 3.42 |
| Jharkhand | 1317 | 1646 | 2145 | 1825 | 2181 | 329 | 178.33 | 24.98 | 10.83 |
| Karnataka | 11,561 | 11,288 | 12,259 | 13,056 | 13,606 | −273 | 772.67 | −2.36 | 6.85 |
| Kerala | 8237 | 8556 | 8500 | 9549 | 10,162 | 319 | 535.33 | 3.87 | 6.26 |
| Madhya Pradesh | 11,775 | 12,457 | 14,578 | 14,965 | 15,386 | 682 | 976.33 | 5.79 | 7.84 |
| Maharashtra | 17,972 | 18,916 | 19,909 | 22,207 | 22,746 | 944 | 1276.67 | 5.25 | 6.75 |
| Manipur | 52 | 58 | 44 | 49 | 26 | 6 | −10.67 | 11.54 | −18.39 |
| Meghalaya | 189 | 198 | 224 | 226 | 213 | 9 | 5.00 | 4.76 | 2.53 |
| Mizoram | 79 | 70 | 108 | 99 | 153 | −9 | 27.67 | −11.39 | 39.52 |
| Nagaland | 36 | 41 | 48 | 43 | 49 | 5 | 2.67 | 13.89 | 6.50 |
| Odisha | 4592 | 4582 | 5546 | 5651 | 6140 | −10 | 519.33 | −0.22 | 11.33 |
| Punjab | 1714 | 2357 | 2616 | 2600 | 2441 | 643 | 28.00 | 37.51 | 1.19 |
| Rajasthan | 4333 | 4531 | 5658 | 5593 | 5343 | 198 | 270.67 | 4.57 | 5.97 |
| Sikkim | 199 | 220 | 285 | 266 | 293 | 21 | 24.33 | 10.55 | 11.06 |
| Tamil Nadu | 13,896 | 13,493 | 16,883 | 18,925 | 19,834 | −403 | 2113.67 | −2.90 | 15.66 |
| Telangana | 7845 | 7675 | 8058 | 10,711 | 9980 | −170 | 768.33 | −2.17 | 10.01 |
| Tripura | 720 | 728 | 845 | 771 | 713 | 8 | −5.00 | 1.11 | −0.69 |
| Uttar Pradesh | 4849 | 5464 | 4804 | 5932 | 8176 | 615 | 904.00 | 12.68 | 16.54 |
| Uttarakhand | 421 | 516 | 943 | 717 | 814 | 95 | 99.33 | 22.57 | 19.25 |
| West Bengal | 13,255 | 12,665 | 13,103 | 13,500 | 12,669 | −590 | 1.33 | −4.45 | 0.01 |
| A&N Islands | 164 | 181 | 180 | 159 | 171 | 17 | −3.33 | 10.37 | −1.84 |
| Chandigarh | 160 | 131 | 128 | 120 | 131 | −29 | 0.00 | −18.13 | 0.00 |
| Delhi (UT) | 2526 | 2526 | 3142 | 2840 | 3417 | 0 | 297.00 | 0.00 | 11.76 |
| Lakshadweep | 3 | 0 | 2 | 1 | 2 | −3 | 0.67 | −100.00 | N/A |
| Puducherry | 500 | 493 | 408 | 504 | 481 | −7 | −4.00 | −1.40 | −0.81 |
| Bharat (total) | 134,516 | 139,123 | 153,052 | 164,033 | 170,924 | 4607 | 10,600.33 | 3.42 | 7.62 |
| State/Union Territory | Rate of Suicide (Per 100,000) | Absolute Increase/Decrease | Percent Increase/Decrease | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2021 | 2022 | 2018–2019 | 2019–2022 (Average Annual Change) | 2018–2019 | 2019–2022 (Average Annual Change) | |
| Andhra Pradesh | 10.2 | 12.4 | 13.4 | 15.3 | 16.8 | 2.2 | 1.5 | 21.57 | 11.83 |
| Arunachal Pradesh | 8.9 | 7.4 | 10.5 | 10.4 | 9.6 | −1.5 | 0.7 | −16.85 | 9.91 |
| Assam | 7 | 6.9 | 9.3 | 9.3 | 9.4 | −0.1 | 0.8 | −1.43 | 12.08 |
| Bihar | 0.4 | 0.5 | 0.7 | 0.7 | 0.6 | 0.1 | 0.0 | 25.00 | 6.67 |
| Chhattisgarh | 24.7 | 26.4 | 26.4 | 26.4 | 28.2 | 1.7 | 0.6 | 6.88 | 2.27 |
| Goa | 16.7 | 16.8 | 19.9 | 20.6 | 19.2 | 0.1 | 0.8 | 0.60 | 4.76 |
| Gujarat | 11.6 | 11.2 | 11.6 | 12.5 | 12.7 | −0.4 | 0.5 | −3.45 | 4.46 |
| Haryana | 12.5 | 14.5 | 13.7 | 12.5 | 12.6 | 2 | −0.6 | 16.00 | −4.37 |
| Himachal Pradesh | 10.2 | 8 | 11.6 | 12 | 8.7 | −2.2 | 0.2 | −21.57 | 2.92 |
| Jharkhand | 3.6 | 4.4 | 5.6 | 4.7 | 5.6 | 0.8 | 0.4 | 22.22 | 9.09 |
| Karnataka | 17.7 | 17.1 | 18.4 | 19.5 | 20.2 | −0.6 | 1.0 | −3.39 | 6.04 |
| Kerala | 23.5 | 24.3 | 24 | 26.9 | 28.5 | 0.8 | 1.4 | 3.40 | 5.76 |
| Madhya Pradesh | 14.5 | 15.1 | 17.4 | 17.6 | 17.9 | 0.6 | 0.9 | 4.14 | 6.18 |
| Maharashtra | 14.8 | 15.4 | 16.1 | 17.8 | 18.1 | 0.6 | 0.9 | 4.05 | 5.84 |
| Manipur | 1.7 | 1.9 | 1.4 | 1.5 | 0.8 | 0.2 | −0.4 | 11.76 | −19.30 |
| Meghalaya | 16 | 6.1 | 6.9 | 6.9 | 6.4 | −9.9 | 0.1 | −61.88 | 1.64 |
| Mizoram | 2.5 | 5.9 | 8.9 | 8.1 | 12.4 | 3.4 | 2.2 | 136.00 | 36.72 |
| Nagaland | 1.7 | 1.9 | 2.2 | 2 | 2.2 | 0.2 | 0.1 | 11.76 | 5.26 |
| Odisha | 10.5 | 10.5 | 12.2 | 12.3 | 13.3 | 0 | 0.9 | 0.00 | 8.89 |
| Punjab | 5.8 | 7.9 | 8.7 | 8.6 | 8 | 2.1 | 0.0 | 36.21 | 0.42 |
| Rajasthan | 5.7 | 5.8 | 7.2 | 7 | 6.6 | 0.1 | 0.3 | 1.75 | 4.60 |
| Sikkim | 30.2 | 33.1 | 42.5 | 39.2 | 43.1 | 2.9 | 3.3 | 9.60 | 10.07 |
| Tamil Nadu | 18.4 | 17.8 | 22.2 | 24.7 | 25.9 | −0.6 | 2.7 | −3.26 | 15.17 |
| Telangana | 21.2 | 20.6 | 21.5 | 26.9 | 26.3 | −0.6 | 1.9 | −2.83 | 9.22 |
| Tripura | 18.2 | 18.2 | 20.9 | 18.9 | 17.3 | 0 | −0.3 | 0.00 | −1.65 |
| Uttar Pradesh | 2.2 | 2.4 | 2.1 | 2.6 | 3.5 | 0.2 | 0.4 | 9.09 | 15.28 |
| Uttarakhand | 3.8 | 4.6 | 8.3 | 6.3 | 7 | 0.8 | 0.8 | 21.05 | 17.39 |
| West Bengal | 13.7 | 13 | 13.4 | 13.7 | 12.8 | −0.7 | −0.1 | −5.11 | −0.51 |
| A&N Islands | 41 | 45.5 | 45 | 39.7 | 42.8 | 4.5 | −0.9 | 10.98 | −1.98 |
| Chandigarh | 13.7 | 11.1 | 10.7 | 9.9 | 10.7 | −2.6 | −0.1 | −18.98 | −1.20 |
| Delhi (UT) | 12.9 | 12.7 | 15.5 | 13.7 | 16.2 | −0.2 | 1.2 | −1.55 | 9.19 |
| Lakshadweep | 4.3 | 0 | 2.9 | 1.5 | 2.9 | −4.3 | 1.0 | −100.00 | N/A |
| Puducherry | 33.8 | 32.5 | 26.3 | 31.8 | 29.7 | −1.3 | −0.9 | −3.85 | −2.87 |
| Bharat (total) | 10.2 | 10.4 | 26.3 | 12 | 12.4 | 0.2 | 0.7 | 1.96 | 6.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varshney, K.; Panhwar, M.A. Long COVID as a Possible Contributor to Rising Suicide Mortality in Bharat (India): An Analysis of Suicide Trends Since the Emergence of COVID-19. COVID 2024, 4, 1684-1693. https://doi.org/10.3390/covid4100117
Varshney K, Panhwar MA. Long COVID as a Possible Contributor to Rising Suicide Mortality in Bharat (India): An Analysis of Suicide Trends Since the Emergence of COVID-19. COVID. 2024; 4(10):1684-1693. https://doi.org/10.3390/covid4100117
Chicago/Turabian StyleVarshney, Karan, and Mansoor Ahmed Panhwar. 2024. "Long COVID as a Possible Contributor to Rising Suicide Mortality in Bharat (India): An Analysis of Suicide Trends Since the Emergence of COVID-19" COVID 4, no. 10: 1684-1693. https://doi.org/10.3390/covid4100117
APA StyleVarshney, K., & Panhwar, M. A. (2024). Long COVID as a Possible Contributor to Rising Suicide Mortality in Bharat (India): An Analysis of Suicide Trends Since the Emergence of COVID-19. COVID, 4(10), 1684-1693. https://doi.org/10.3390/covid4100117