
SARS-CoV-2 Contacts’ Symptom Development and Secondary Attack Rate: A Retrospective Analysis of a Contact-Tracing Cohort in Catalonia

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
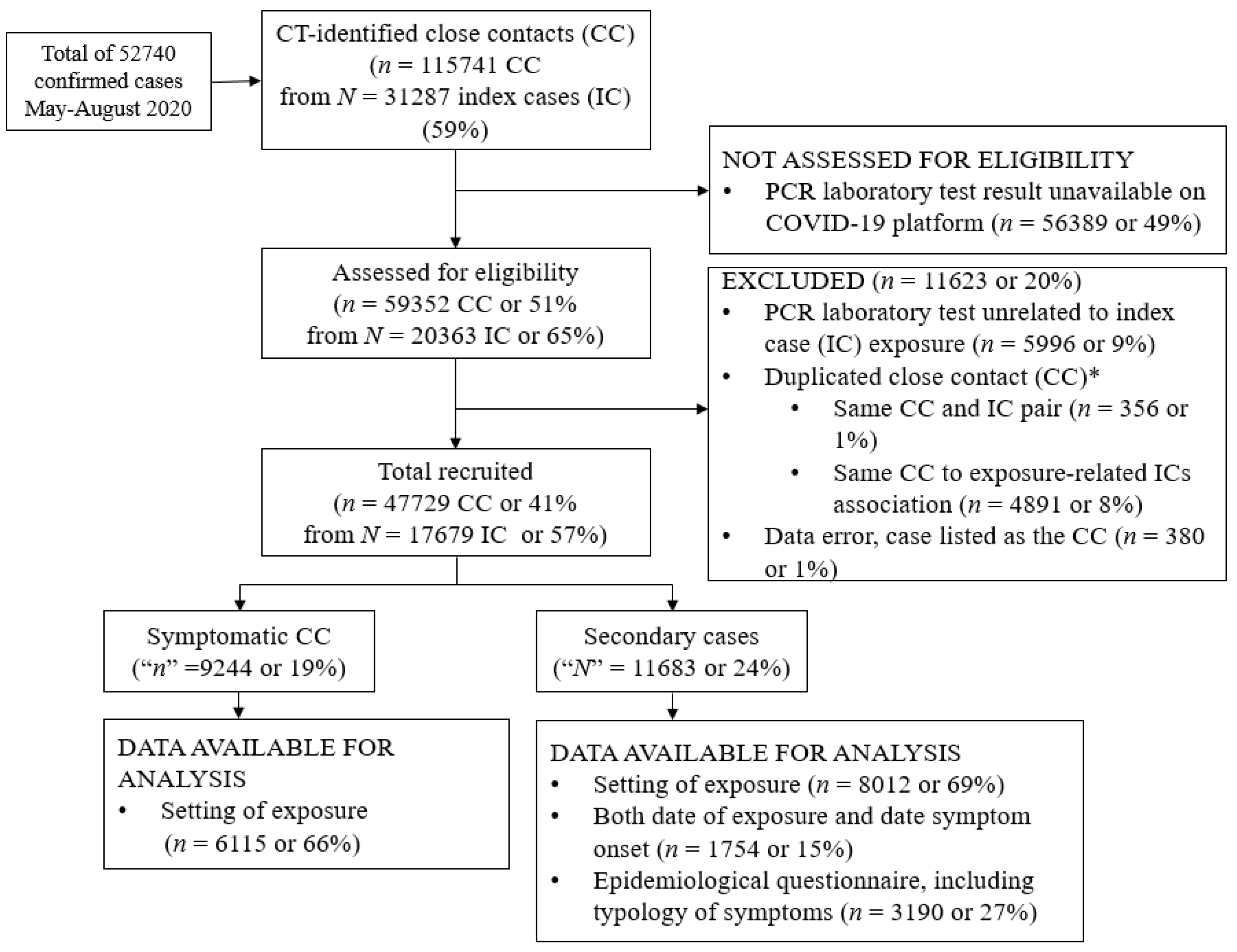
2.1. Study Design and Population
2.2. Case Ascertainment and COVID-19 CT Program
2.3. Close Contacts’ Assessed Outcomes
2.4. Statistical Methods
2.5. Ethical Considerations
3. Results
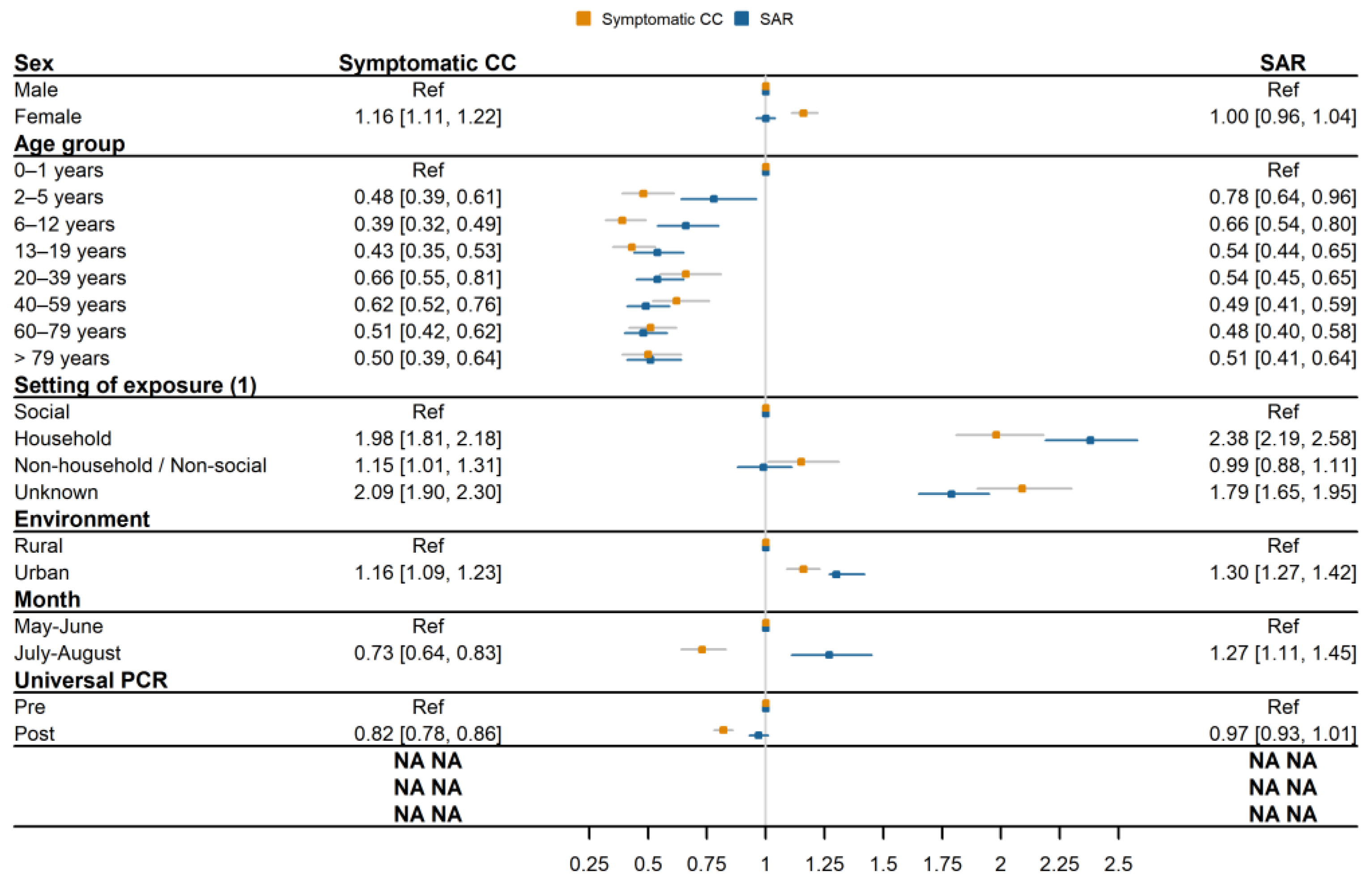
3.1. CC Demographic Characteristics by Outcome
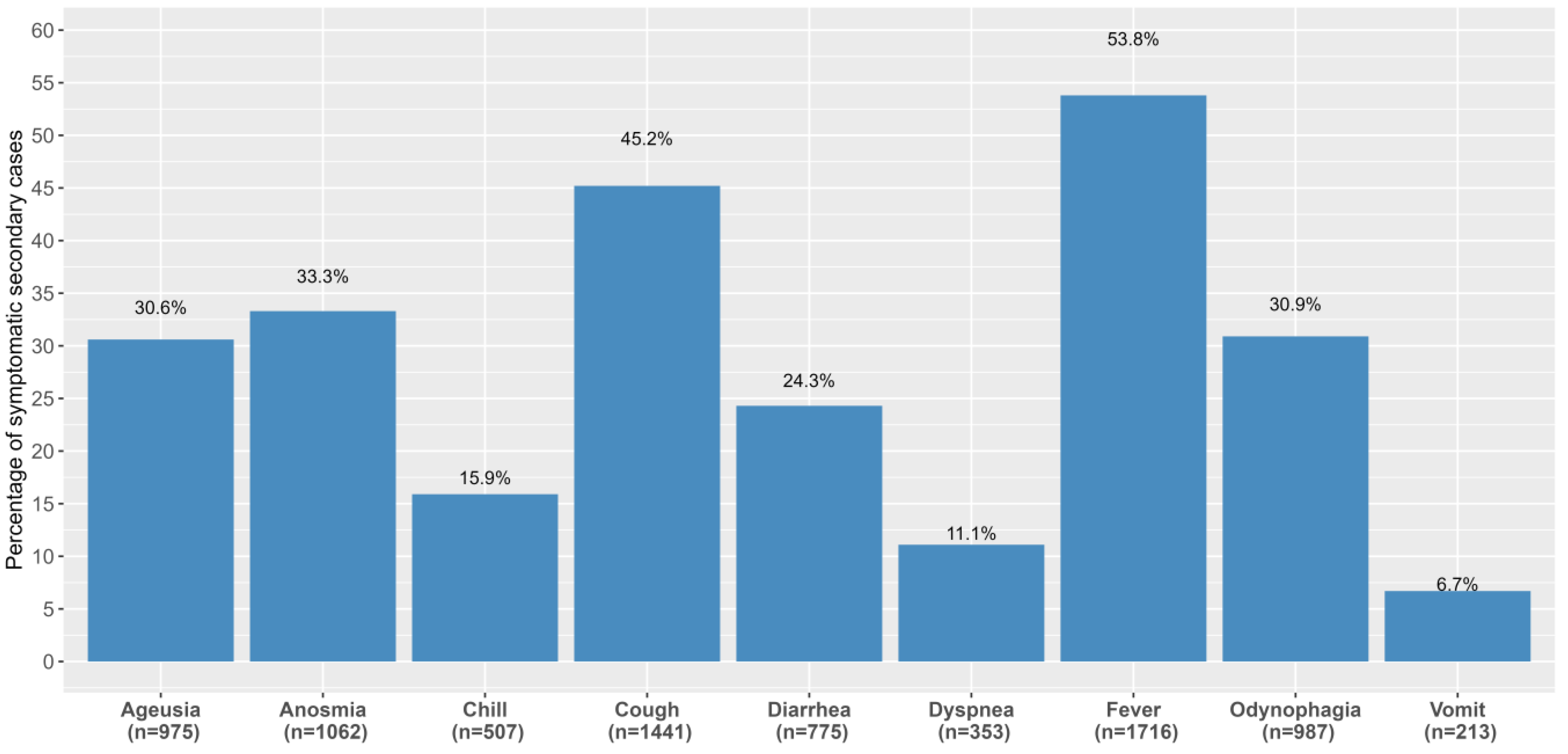
3.2. Symptom Development among Secondary Cases
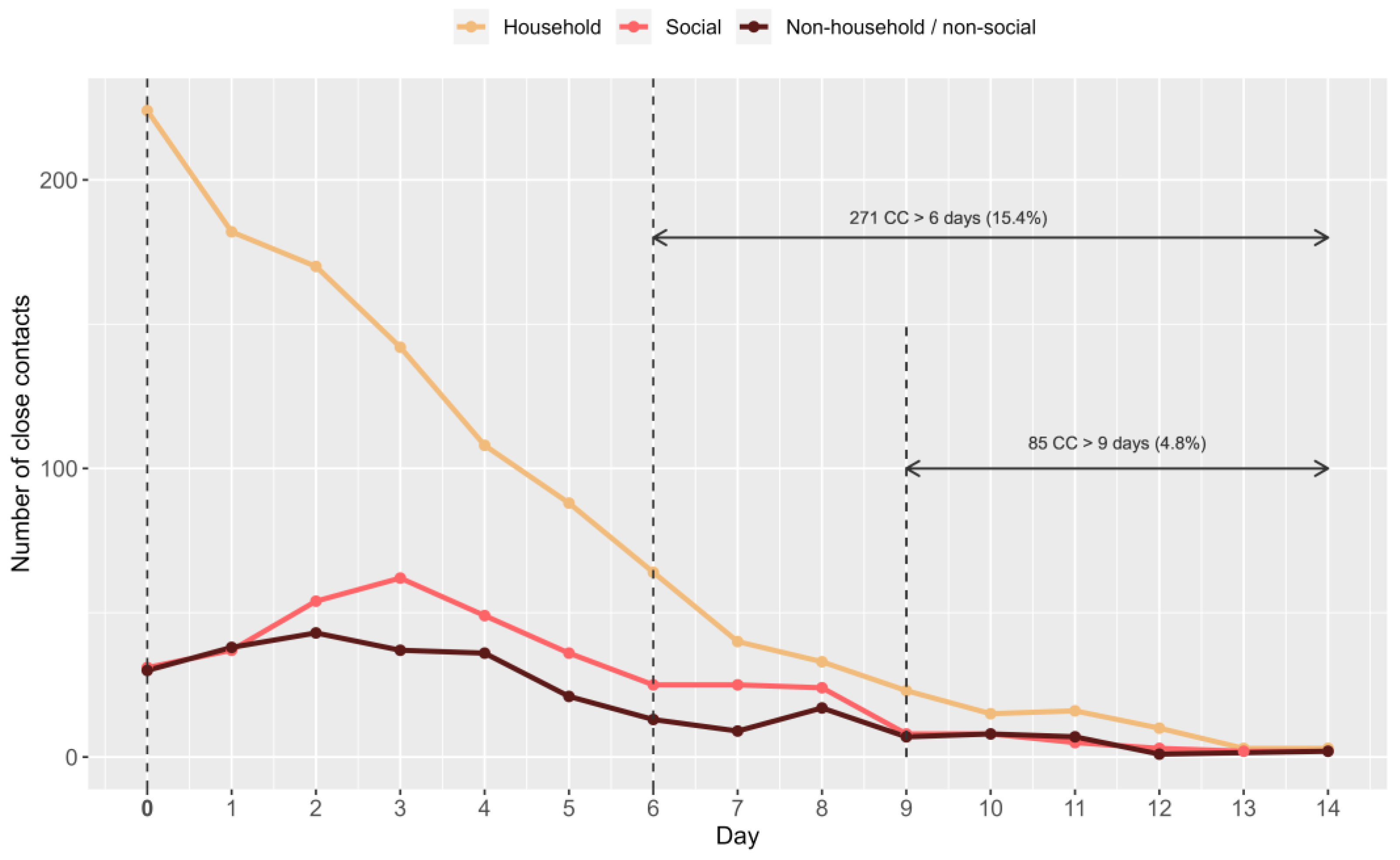
3.3. Incubation Period of Secondary Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grantz, K.H.; Lee, E.C.; McGowan, L.D.; Lee, K.H.; Metcalf, C.J.E.; Gurley, E.S.; Lessler, J. Maximizing and evaluating the impact of test-trace-isolate programs: A modeling study. PLoS Med. 2021, 18, e1003585. [Google Scholar] [CrossRef] [PubMed]
- Edmond, J.S. Pandemic Resilience: Getting it Done. A TTSI Technical Advice Handbook. In Massachusetts Testing, Tracing, and Supported Isolation Collaborative, v 2.0 ed.; Center for Ethics, Harvard Global Health Institute, Harvard University: Cambridge, MA, USA, 2020; p. 3. [Google Scholar]
- Working group for the surveillance and control of COVID-19 in Spain. The first wave of the COVID-19 pandemic in Spain: Characterisation of cases and risk factors for severe outcomes, as at 27 April 2020. Eurosurveillance 2020, 25, 2001431. [Google Scholar] [CrossRef]
- Subdirectorate General for Surveillance and Public Health Emergency Response-Public Health Agency of Catalonia (PHAC). Technical Summary Report of the COVID-19 Cases in Catalonia. 24 August (no. 23) 2020. (In Catalan). Available online: http://hdl.handle.net/11351/6395 (accessed on 3 July 2021).
- World Health Organization. Contact tracing in the context of COVID-19. Interim guidance. Pediatr. I Med. Rodz. 2020, 16, 33–39. Available online: http://www.pimr.pl/index.php/issues/2020-vol-16-no-1/contact-tracing-in-the-context-of-covid-19-interim-guidance-1721?aid=1465 (accessed on 7 July 2021). [CrossRef]
- Merkur, S.; Maresso, A.; Cylus, J.; Van Ginneken, E.; Lessof, S. Lessons from the first wave: The covid-19 health system response monitor. Eurohealth 2020, 26, 5. [Google Scholar]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Delfraissy, J.-F.; Duault, L.A.; Benamouzig, A.D.; Bouadma, S.L.; Cauchemez, R.S.; Chauvin, M.F.; de Sante Publique, M.; de Ville Arnaud Fontanet, M.; Grard, E.M.-A.; Hoang, M.A.M.; et al. Membres du Conseil Scientifique Associés à cet Avis: 3 Septembre 2020 Strategie et Modalites d’Isolement Partie I-les Prerequis Necessaires à la Construction des Scenarios avis 7 du Conseil Scientifique COVID-19. 2020. 19–19. Available online: https://solidarites-sante.gouv.fr/IMG/pdf/avis_conseil_scientifique_3_septembre_2020.pdf (accessed on 7 July 2021).
- Koh, W.C.; Naing, L.; Chaw, L.; Rosledzana, M.A.; Alikhan, M.F.; Jamaludin, S.A.; Amin, F.; Omar, A.; Shazli, A.; Griffith, M.; et al. What do we know about SARS-CoV-2 transmission? A systematic review and meta-analysis of the secondary attack rate and associated risk factors. PLoS ONE 2020, 15, e0240205. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 Transmission from People Without COVID-19 Symptoms. JAMA Netw. Open 2021, 4, e2035057. [Google Scholar] [CrossRef] [PubMed]
- Subdirectorate General for Surveillance and Public Health Emergency Response-Public Health Agency of Catalonia (PHAC). Acting Protocol against SARS-CoV-2 Infection Cases. 7 August Update. 2020. (In Catalan). Available online: https://salutpublica.gencat.cat/ca/detalls/Article/Actualitzacio-del-procediment-dactuacio-enfront-de-casos-dinfeccio-pel-nou-coronavirus-SARS-CoV-2 (accessed on 10 October 2021).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Rossetto, M.; Brand, É.M.; Hahn, G.V.; Oliveira, D.L.; Teixeira, L.B. Epidemiological profile of tuberculosis cases with HIV coinfection in Porto Alegre city, Brazil. Rev. Bras. Enferm. 2019, 72, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- WMA Declaration of Helsinki–Ethical Principles for Medical Research Involving Human Subjects–WMA–The World Medical Association. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 22 September 2022).
- Subdirectorate General for Surveillance and Public Health Emergency Response-Public Health Agency of Catalonia (PHAC). Acting Protocol against SARS-CoV-2 Infection Cases, 16 April Update; PHAC: Winnipeg, OT, Canada, 2020.
- Instituto Nacional Estadística (INE). Glosario de Conceptos Básicos. Available online: https://www.ine.es/DEFIne/?L=0 (accessed on 13 May 2021).
- Idescat. Short-Term Economic Indicators. Weekly Incidence of COVID-19. Available online: https://www.idescat.cat/indicadors/?lang=en&id=conj&n=14356 (accessed on 12 January 2022).
- Dong, X.C.; Li, J.M.; Bai, J.Y.; Liu, Z.Q.; Zhou, P.H.; Gao, L.; Li, X.Y.; Zhang, Y. Epidemiological characteristics of confirmed COVID-19 cases in Tianjin. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 638–641. [Google Scholar] [PubMed]
- Dawson, P.; Rabold, E.M.; Laws, R.L.; Conners, E.E.; Gharpure, R.; Yin, S.; Buono, S.A.; Dasu, T.; Bhattacharyya, S.; Westergaard, R.P.; et al. Loss of Taste and Smell as Distinguishing Symptoms of Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 72, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Li, Y.Y.; Liu, M.J.; Fang, L.Q.; Dean, N.E.; Wong, G.W.; Yang, X.B.; Longini, I.; Halloran, M.E.; Wang, H.J.; et al. Household transmission of SARS-CoV-2 and risk factors for susceptibility and infectivity in Wuhan: A retrospective observational study. Lancet Infect. Dis. 2021, 21, 617. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Szefler, S.J. COVID-19 and the impact of social determinants of health. Lancet Respir. Med. 2020, 8, 659–661. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, M.; Lantz, P.M.; Tipirneni, R. Association of Social and Demographic Factors with COVID-19 Incidence and Death Rates in the US. JAMA Netw. Open 2021, 4, e2036462. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. COVID vaccines and kids: Five questions as trials begin. Nature 2021, 592, 670–671. [Google Scholar] [CrossRef] [PubMed]
- Torjesen, I. Covid-19: Delta variant is now UK’s most dominant strain and spreading through schools. BMJ 2021, 373, n1445. [Google Scholar] [CrossRef] [PubMed]
- UN News. COVID-19: Wealthy Nations Urged to Delay Youth Vaccines, Donate to Solidarity Scheme. Available online: https://news.un.org/en/story/2021/05/1091952 (accessed on 5 May 2021).
- King, J.A.; Whitten, T.A.; Bakal, J.A.; McAlister, F.A. Symptoms associated with a positive result for a swab for SARS-CoV-2 infection among children in Alberta. Can. Med. Assoc. J. 2021, 193, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Wells, C.R.; Townsend, J.P.; Pandey, A.; Moghadas, S.M.; Krieger, G.; Singer, B.; McDonald, R.H.; Fitzpatrick, M.C.; Galvani, A.P. Optimal COVID-19 quarantine and testing strategies. Nat. Commun. 2021, 12, 356. [Google Scholar] [CrossRef] [PubMed]
- Subdirectorate General for Surveillance and Public Health Emergency Response-Public Health Agency of Catalonia (PHAC). Acting Protocol against SARS-CoV-2 Infection Cases in the Re-Opening Phase. Follow-Up Indicators. 2020. Available online: http://hdl.handle.net/11351/4919 (accessed on 19 February 2023).
- Kissler, S.; Fauver, J.R.; Mack, C.; Tai, C.G.; Mallery, I.B.; Watkins, A.E.; Radhika, S.M.; Anderson, D.J.; Ho, D.D.; Grubaugh, N.D.; et al. Viral Dynamics of SARS-CoV-2 variants in vaccinated and unvaccinated persons. N. Engl. J. Med. 2021, 385, 2489–2491. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Operational Considerations for Adapting a Contact Tracing Program to Respond to the COVID-19 Pandemic [Internet]. Centers for Disease Control and Preventive. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/global-covid-19/operational-considerations-contact-tracing.html (accessed on 27 January 2021).
- European Center for Disease Prevention and Control (ECDC). Monitoring and evaluation framework for COVID-19 response activities in the EU/EEA and the UK. Stockholm:. ECDC Tech. Rep. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-monitoring-and-evaluation-framework-response-activities (accessed on 20 October 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SYMPTOMATIC CCs | SECONDARY CASES | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TOTAL | Before | After | p-Value | TOTAL | Before | After | p-Value | ||||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||||||||||
| TOTAL | 9244 | 19.4% | 4267 | 21.2% | 4977 | 18.0% | <0.05 | 11,683 | 24.5% | 4998 | 24.8% | 6685 | 24.2% | 0.151 | |||||||
| Sex | |||||||||||||||||||||
| Males | 4060 | 18.1% | 1850 | 19.8% | 2210 | 16.9% | <0.05 | 5479 | 24.5% | 2297 | 24.6% | 3182 | 24.3% | 0.151 | |||||||
| Females | 5184 | 20.5% | 2417 | 22.3% | 2767 | 19.1% | 6204 | 24.5% | 2701 | 25.0% | 3503 | 24.1% | |||||||||
| Age group (years) | |||||||||||||||||||||
| 0–1 | 150 | 29.4% | 74 | 33.3% | 76 | 26.4% | <0.05 | 192 | 37.6% | 87 | 39.2% | 105 | 36.5% | <0.05 | |||||||
| 2–5 | 305 | 16.8% | 156 | 19.5% | 149 | 14.7% | 583 | 32.1% | 256 | 32.0% | 327 | 32.2% | |||||||||
| 6–12 | 534 | 14.0% | 260 | 16.1% | 274 | 12.5% | 1079 | 28.4% | 440 | 27.2% | 639 | 29.2% | |||||||||
| 13–19 | 702 | 15.1% | 315 | 17.4% | 387 | 13.6% | 1139 | 24.5% | 460 | 25.5% | 679 | 23.9% | |||||||||
| 20–39 | 3416 | 21.6% | 1593 | 23.2% | 1823 | 20.4% | 3879 | 24.5% | 1703 | 24.8% | 2176 | 24.3% | |||||||||
| 40–59 | 2952 | 20.6% | 1356 | 22.3% | 1596 | 19.3% | 3267 | 22.8% | 1396 | 22.9% | 1871 | 22.7% | |||||||||
| 60–79 | 995 | 17.5% | 431 | 18.9% | 564 | 16.5% | 1283 | 22.5% | 544 | 23.8% | 739 | 21.7% | |||||||||
| >79 | 190 | 17.2% | 82 | 17.9% | 108 | 16.7% | 261 | 23.6% | 112 | 24.4% | 149 | 23.1% | |||||||||
| Setting of exposure * | |||||||||||||||||||||
| Social | 613 | 11.6% | 6 | 31.6% | 607 | 11.5% | <0.05 | 823 | 15.5% | 4 | 21.1% | 819 | 15.5% | <0.05 | |||||||
| Household | 2572 | 20.6% | 25 | 20.5% | 2547 | 20.6% | 3795 | 30.4% | 36 | 29.5% | 3759 | 30.4% | |||||||||
| Non-household/Non-social | 469 | 13.1% | 23 | 26.1% | 446 | 12.7% | 553 | 15.4% | 28 | 31.8% | 525 | 15.0% | |||||||||
| Unknown | 2461 | 21.5% | 1084 | 21.7% | 1377 | 21.4% | 2841 | 24.8% | 1259 | 25.1% | 1582 | 24.5% | |||||||||
| Environment ^ | |||||||||||||||||||||
| Urban | 8095 | 19.6% | 3655 | 20.8% | 4440 | 18.7% | <0.05 | 10.323 | 25.0% | 4386 | 25.0% | 5937 | 25.0% | <0.05 | |||||||
| Rural | 1552 | 17.4% | 762 | 21.1% | 790 | 14.8% | 1775 | 19.9% | 750 | 20.8% | 1025 | 19.3% | |||||||||
| Asymptomatic | Symptomatic | TOTAL | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| TOTAL | 5357 | 45.9% | 6326 | 54.1% | 11,683 | - | |
| Sex | |||||||
| Males | 2626 | 47.9% | 2853 | 52.1% | 5479 | <0.05 | |
| Females | 2731 | 44.0% | 3473 | 56.0% | 6204 | ||
| Age group (years) | |||||||
| 0–1 | 85 | 44.3% | 107 | 55.7% | 192 | ||
| 2–5 | 349 | 59.9% | 234 | 40.1% | 583 | ||
| 6–12 | 674 | 62.5% | 405 | 37.5% | 1079 | ||
| 13–19 | 641 | 56.3% | 498 | 43.7% | 1139 | <0.05 | |
| 20–39 | 1643 | 42.4% | 2236 | 57.6% | 3879 | ||
| 40–59 | 1314 | 40.2% | 1953 | 59.8% | 3267 | ||
| 60–79 | 534 | 41.6% | 749 | 58.4% | 1283 | ||
| >79 | 117 | 44.8% | 144 | 55.2% | 261 | ||
| Setting of exposure * | |||||||
| Social | 381 | 46.3% | 442 | 53.7% | 823 | <0.05 | |
| Household | 1903 | 50.1% | 1892 | 49.9% | 3795 | ||
| Non-household/Non-social | 234 | 42.3% | 319 | 57.7% | 553 | ||
| Unknown | 1254 | 44.1% | 1587 | 55.9% | 2841 | ||
| Month | |||||||
| May–June | 80 | 30.1% | 186 | 69.9% | 266 | <0.05 | |
| July–August | 5277 | 46.2% | 6140 | 53.8% | 11,417 | ||
| Days | Household | Social | Non-Household/Non-Social | Total | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||||||
| 0–4 | 826 | 73.9% | 233 | 63.1% | 184 | 68.9% | 1243 | 70.6% | <0.05 | |||
| 5–6 | 152 | 13.6% | 61 | 16.5% | 34 | 12.7% | 247 | 14.0% | ||||
| 7–8 | 73 | 6.5% | 49 | 13.3% | 26 | 9.7% | 148 | 8.4% | ||||
| 9 | 23 | 2.1% | 8 | 2.2% | 7 | 2.6% | 38 | 2.2% | ||||
| >9 | 47 | 3.9% | 20 | 4.9% | 18 | 6.0% | 85 | 4.8% | ||||
| TOTAL | 1121 | 63.7% | 371 | 21.0% | 269 | 15.2% | 1761 | 100% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mallafré-Larrosa, M.; Herrero Garcia, M.; Mendoza-Funes, S.; Martínez-Solanas, È.; Patsi-Bosch, G.; Mendioroz Peña, J.; Ciruela Navas, P., on behalf of the Epidemiological Surveillance Network of Catalonia. SARS-CoV-2 Contacts’ Symptom Development and Secondary Attack Rate: A Retrospective Analysis of a Contact-Tracing Cohort in Catalonia. COVID 2023, 3, 428-439. https://doi.org/10.3390/covid3040032
Mallafré-Larrosa M, Herrero Garcia M, Mendoza-Funes S, Martínez-Solanas È, Patsi-Bosch G, Mendioroz Peña J, Ciruela Navas P on behalf of the Epidemiological Surveillance Network of Catalonia. SARS-CoV-2 Contacts’ Symptom Development and Secondary Attack Rate: A Retrospective Analysis of a Contact-Tracing Cohort in Catalonia. COVID. 2023; 3(4):428-439. https://doi.org/10.3390/covid3040032
Chicago/Turabian StyleMallafré-Larrosa, Meritxell, Mercè Herrero Garcia, Sergi Mendoza-Funes, Èrica Martínez-Solanas, Glòria Patsi-Bosch, Jacobo Mendioroz Peña, and Pilar Ciruela Navas on behalf of the Epidemiological Surveillance Network of Catalonia. 2023. "SARS-CoV-2 Contacts’ Symptom Development and Secondary Attack Rate: A Retrospective Analysis of a Contact-Tracing Cohort in Catalonia" COVID 3, no. 4: 428-439. https://doi.org/10.3390/covid3040032
APA StyleMallafré-Larrosa, M., Herrero Garcia, M., Mendoza-Funes, S., Martínez-Solanas, È., Patsi-Bosch, G., Mendioroz Peña, J., & Ciruela Navas, P., on behalf of the Epidemiological Surveillance Network of Catalonia. (2023). SARS-CoV-2 Contacts’ Symptom Development and Secondary Attack Rate: A Retrospective Analysis of a Contact-Tracing Cohort in Catalonia. COVID, 3(4), 428-439. https://doi.org/10.3390/covid3040032