


Microbial Organisms in the Lower Respiratory Tract Associated with SARS-CoV-2 Infection: A Cross-Sectional Study in Northern Ghana

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Area
2.3. Study Design and Sample Collection
2.4. Laboratory Methods
Bacteria Culture
2.5. Detection of SARS-CoV-2
2.6. Data Collection
2.7. Statistical Analysis
3. Results
3.1. Socio-Demographic and Clinical Characteristics of Study Participants
3.2. Clinical and Socio-Demographic Risk Factors Associated with SARS-CoV-2 Infection
3.3. Co-Infection/Microbial Isolates among Study Participants
3.4. Sputum Culture and Microbial Isolates as Potential Risk Factors of SARS-CoV-2 Infection
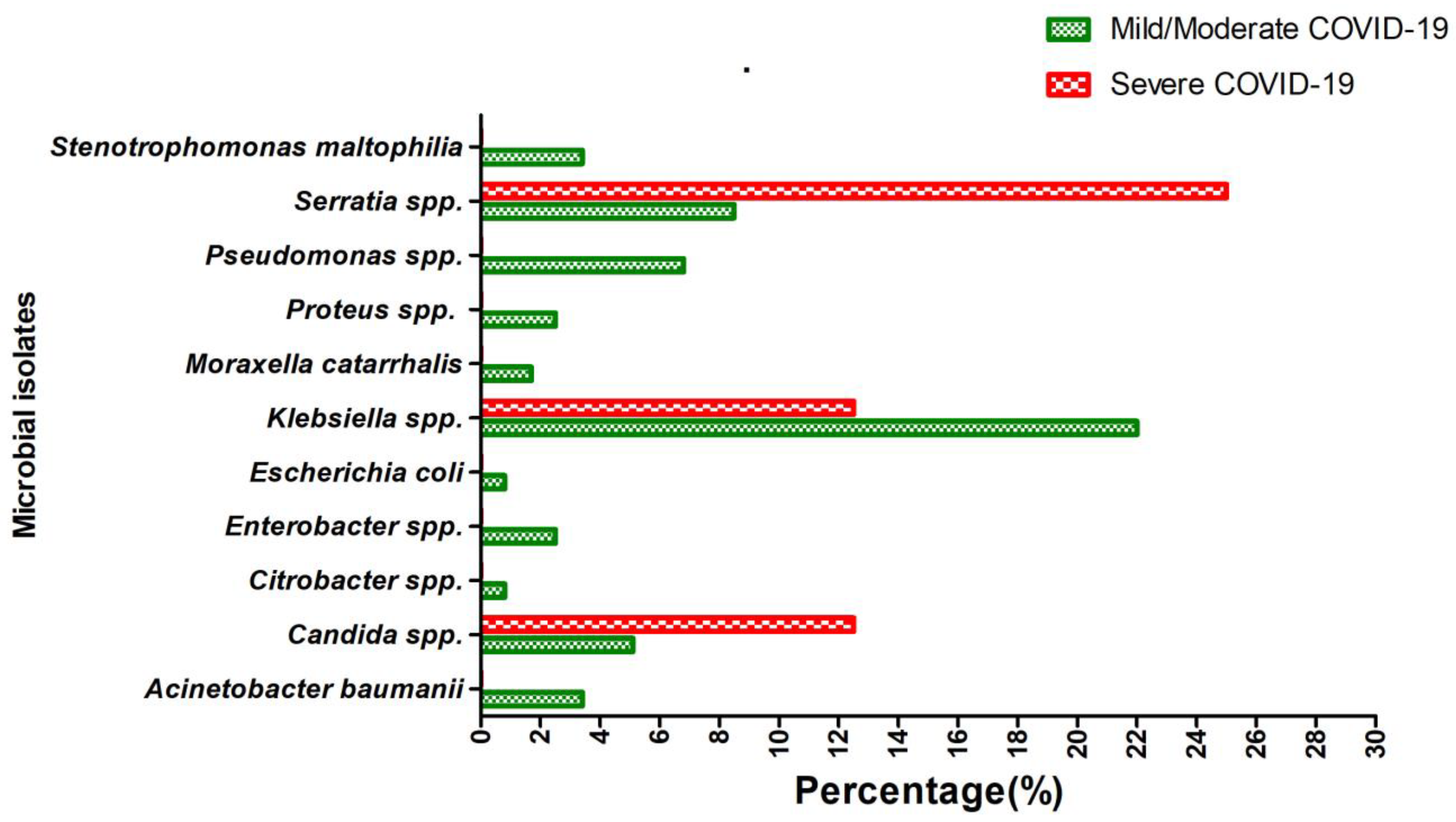
3.5. Distribution of Microbial Isolates According to the Disease Severity among COVID-19 Patients
3.6. Antimicrobial Resistance Pattern amongst Isolated Pathogens in SARS-CoV-2 Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- He, C.; Qin, M.; Sun, X. Highly pathogenic coronaviruses: Thrusting vaccine development in the spotlight. Acta Pharm. Sin. B 2020, 10, 1175–1191. [Google Scholar] [CrossRef] [PubMed]
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation and treatment coronavirus (COVID-19). In Statpearls [Internet]; StatPearls Publishing: Tampa, FL, USA, 2020. [Google Scholar]
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Ghana Health Service. COVID-19 Situation Dashboard, Ghana. Available online: https://ghs.gov.gh/covid19/dashboardm.php (accessed on 17 February 2023).
- Puthiyedath, R.; Kataria, S.; Payyappallimana, U.; Mangalath, P.; Nampoothiri, V.; Sharma, P.; Singh, M.K.; Kumar, K.; Trehan, N. Ayurvedic clinical profile of COVID-19—A preliminary report. J. Ayurveda Integr. Med. 2020, 13, 100326. [Google Scholar] [CrossRef] [PubMed]
- Kantarcioglu, B.; Iqbal, O.; Lewis, J.; Carter, C.A.; Singh, M.; Lievano, F.; Ligocki, M.; Jeske, W.; Adiguzel, C.; Gerotziafas, G.T.; et al. An Update on the Status of Vaccine Development for SARS-CoV-2 Including Variants. Practical Considerations for COVID-19 Special Populations. Clin. Appl. Thromb. Hemost. 2022, 28, 10760296211056648. [Google Scholar] [CrossRef] [PubMed]
- Paget, J.; Spreeuwenberg, P.; Charu, V.; Taylor, R.J.; Iuliano, A.D.; Bresee, J.; Simonsen, L.; Viboud, C.; Global Seasonal Influenza-Associated Mortality Collaborator Network and GLaMOR Collaborating Teams. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J. Glob. Health 2019, 9, 020421. [Google Scholar] [CrossRef]
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef]
- Cao, Y.; Chen, M.; Dong, D.; Xie, S.; Liu, M. Environmental pollutants damage airway epithelial cell cilia: Implications for the prevention of obstructive lung diseases. Thorac. Cancer 2020, 11, 505–510. [Google Scholar] [CrossRef]
- Ghana Statistical Service, Population of Regions and Districts Report. Available online: https://statsghana.gov.gh/gssmain/fileUpload/pressrelease/2021%20PHC%20General%20Report%20Vol%203A_Population%20of%20Regions%20and%20Districts_181121.pdf (accessed on 23 March 2023).
- Sisó-Almirall, A.; Brito-Zerón, P.; Ferrín, L.C.; Kostov, B.; Moreno, A.M.; Mestres, J.; Sellarès, J.; Galindo, G.; Morera, R.; Basora, J.; et al. Long COVID-19: Proposed primary care clinical guidelines for diagnosis and disease management. Int. J. Environ. Res. Public Health 2021, 18, 4350. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI Supplement M100: Wayne, PA, USA, 2021. [Google Scholar]
- Owusu, M.; Sylverken, A.A.; Ankrah, S.T.; El-Duah, P.; Ayisi-Boateng, N.K.; Yeboah, R.; Gorman, R.; Asamoah, J.; Binger, T.; Acheampong, G.; et al. Epidemiological profile of SARS-CoV-2 among selected regions in Ghana: A cross-sectional retrospective study. PLoS ONE 2020, 15, e0243711. [Google Scholar] [CrossRef]
- Bao, L.; Zhang, C.; Dong, J.; Zhao, L.; Li, Y.; Sun, J. Oral microbiome and SARS-CoV-2: Beware of lung co-infection. Front. Microbiol. 2020, 11, 1840. [Google Scholar] [CrossRef]
- Ruxton, S.; Burrell, S. Masculinities and COVID-19: Making the Connections; Promundo: Washington, DC, USA, 2020. [Google Scholar]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Faidah, H.; Al-Maiahy, T.J.; Cruz-Martins, N.; Batiha, G.E.S. The looming effects of estrogen in COVID-19: A Rocky Rollout. Front. Nutr. 2021, 8, 649128. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, M.; Elliott, J.; Bodinier, B.; Barclay, W.; Ward, H.; Cooke, G.; Donnelly, C.A.; Chadeau-Hyam, M.; Elliott, P. Variant-specific symptoms of COVID-19 in a study of 1,542,510 adults in England. Nat. Commun. 2022, 13, 6856. [Google Scholar] [CrossRef]
- Lapostolle, F.; Schneider, E.; Vianu, I.; Dollet, G.; Roche, B.; Berdah, J.; Michel, J.; Goix, L.; Chanzy, E.; Petrovic, T.; et al. Clinical features of 1487 COVID-19 patients with outpatient management in the Greater Paris: The COVID-call study. Intern. Emerg. Med. 2020, 15, 813–817. [Google Scholar] [CrossRef]
- Abayomi, A.; Odukoya, O.; Osibogun, A.; Wright, O.; Adebayo, B.; Balogun, M.; Abdur-Razzaq, H. Presenting symptoms and predictors of poor outcomes among 2,184 patients with COVID-19 in Lagos State, Nigeria. Int. J. Infect. Dis. 2021, 102, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Uygun, Ö.; Ertaş, M.; Ekizoğlu, E.; Bolay, H.; Özge, A.; Kocasoy Orhan, E.; Çağatay, A.A.; Baykan, B. Headache characteristics in COVID-19 pandemic-a survey study. J. Headache Pain 2020, 21, 121. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Cuadrado, M.L.; Gómez-Mayordomo, V.; García-Azorín, D.; Arendt-Nielsen, L. Headache as a COVID-19 onset symptom or post-COVID symptom according to the SARS-CoV-2 variant. Expert Rev. Neurother. 2023, 23, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Antinori, S.; Galimberti, L.; Milazzo, L.; Ridolfo, A.L. Bacterial and fungal infections among patients with SARS-CoV-2 pneumonia. Infez Med. 2020, 28 (Suppl. S1), 29–36. [Google Scholar]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Golzari, S.E. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect. Dis. 2020, 20, 646. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res. 2020, 285, 198005. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, H.K.-A.; Mahmoud, M.A.; Aburahma, M.Z.; Elkhawaga, A.A.; El-Mokhtar, M.A.; Sayed, I.M.; Hosni, A.; Hassany, S.M.; Medhat, M.A. Predictors of severity and co-infection resistance profile in COVID-19 patients: First report from upper Egypt. Infect. Drug Resist. 2020, 13, 3409. [Google Scholar] [CrossRef]
- Lu, B.; Yan, Y.; Dong, L.; Han, L.; Liu, Y.; Yu, J.; Chen, J.; Yi, D.; Zhang, M.; Deng, X.; et al. Integrated characterization of SARS-CoV-2 genome, microbiome, antibiotic resistance and host response from single throat swabs. Cell Discov. 2021, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Feehan, A.K.; Rose, R.; Nolan, D.J.; Spitz, A.M.; Graubics, K.; Colwell, R.R.; Garcia-Diaz, J.; Lamers, S.L. Nasopharyngeal Microbiome Community Composition and Structure Is Associated with Severity of COVID-19 Disease and Breathing Treatment. Appl. Microbiol. 2021, 1, 177–188. [Google Scholar] [CrossRef]
- Deinhardt-Emmer, S.; Böttcher, S.; Häring, C.; Giebeler, L.; Henke, A.; Zell, R.; Jungwirth, J.; Jordan, P.M.; Werz, O.; Hornung, F.; et al. SARS-CoV-2 causes severe epithelial inflammation and barrier dysfunction. J. Virol. 2021, 95, e00110-21. [Google Scholar] [CrossRef]
- Ou, X.; Zhou, L.; Huang, H.; Lin, Y.; Pan, X.; Chen, D. A severe case with co-infection of SARS-CoV-2 and common respiratory pathogens. Travel Med. Infect. Dis. 2020, 35, 101672. [Google Scholar] [CrossRef]
- Peddu, V.; Shean, R.C.; Xie, H.; Shrestha, L.; Perchetti, G.A.; Minot, S.S.; Roychoudhury, P.; Huang, M.L.; Nalla, A.; Reddy, S.B.; et al. Metagenomic analysis reveals clinical SARS-CoV-2 infection and bacterial or viral superinfection and colonization. Clin. Chem. 2020, 66, 966–972. [Google Scholar] [CrossRef]
- Goel, N.; Ahmad, R.; Fatima, H.; Khare, S.K. New threatening of SARS-CoV-2 coinfection and strategies to fight the current pandemic. Med. Drug Discov. 2021, 10, 100089. [Google Scholar] [CrossRef]
- Davies-Bolorunduro, O.F.; Fowora, M.A.; Amoo, O.S.; Adeniji, E.; Osuolale, K.A.; Oladele, O.; Onuigbo, T.I.; Obi, J.C.; Oraegbu, J.; Ogundepo, O.; et al. Evaluation of respiratory tract bacterial co-infections in SARS-CoV-2 patients with mild or asymptomatic infection in Lagos, Nigeria. Bull. Natl. Res. Cent. 2022, 46, 115. [Google Scholar] [CrossRef]
- Chu, H.; Chan, J.F.W.; Wang, Y.; Yuen, T.T.T.; Chai, Y.; Hou, Y.; Shuai, H.; Yang, D.; Hu, B.; Huang, X.; et al. Comparative replication and immune activation profiles of SARS-CoV-2 and SARS-CoV in human lungs: An ex vivo study with implications for the pathogenesis of COVID-19. Clin. Infect. Dis. 2020, 71, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.M.; Brill, K.L.; Dhingra, G.; Kannan, S.G. Delayed recurrent spontaneous pneumothorax in a patient recovering from COVID-19 pneumonia. Korean J. Anesthesiol. 2021, 74, 183. [Google Scholar] [CrossRef] [PubMed]
- Asli, R.; Abdullah, M.S.; Chong, P.L.; Metussin, D.; Momin, R.N.; Mani, B.I.; Chong, V.H. Case report: Right bundle brunch block and QTc prolongation in a patient with COVID-19 treated with hydroxychloroquine. Am. J. Trop. Med. Hyg. 2020, 103, 79. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Chen, S.-Y.; Ko, W.-C.; Hsueh, P.-R. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agents 2021, 57, 106324. [Google Scholar] [CrossRef]
- Silva, D.; Lima, C.; Magalhães, V.; Baltazar, L.; Peres, N.; Caligiorne, R.; Moura, A.; Fereguetti, T.; Martins, J.; Rabelo, L.; et al. Fungal and bacterial coinfections increase mortality of severely ill COVID-19 patients. J. Hosp. Infect. 2021, 113, 145–154. [Google Scholar] [CrossRef]
- Egyir, B.; Obeng-Nkrumah, N.; Kyei, G.B. COVID-19 pandemic and antimicrobial resistance: Another call to strengthen laboratory diagnostic capacity in Africa. Afr. J. Lab. Med. 2020, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Kaynar, K.; Gul, S.; Ersoz, S.; Ozdemir, F.; Ulusoy, H.; Ulusoy, S. Amikacin-induced nephropathy: Is there any protective way? Ren. Fail. 2007, 29, 23–27. [Google Scholar] [CrossRef]


{kind=link}
| Variable | All Participants n = 380 (%) | SARS-CoV-2 Negative n = 262 (%) | SARS-CoV-2 Positive n = 118 (%) | p-Value |
|---|---|---|---|---|
| Age group (years) | 0.699 | |||
| <20 | 26 (6.9) | 18 (6.9) | 8 (6.8) | |
| 21–30 | 112 (29.6) | 81 (31.2) | 31 (26.3) | |
| 31–40 | 102 (27.0) | 65 (25.0) | 37 (31.4) | |
| 41–50 | 48 (12.7) | 32 (12.3) | 16 (13.6) | |
| 51–94 | 90 (23.8) | 64 (24.6) | 26 (22.0) | |
| Gender | 0.821 | |||
| Female | 149 (39.2) | 104 (39.7) | 45 (38.1) | |
| Male | 231 (60.8) | 158 (60.3) | 73 (61.9) | |
| Clinical Symptoms | ||||
| Asymptomatic | 120 (31.6) | 60 (22.9) | 60 (50.8) | <0.001 |
| Symptomatic | 260 (68.4) | 202 (77.1) | 58 (49.2) | |
| Cough | <0.001 | |||
| No | 146 (38.6) | 69 (26.5) | 77 (65.3) | |
| Yes | 232 (61.4) | 191 (73.5) | 41 (34.7) | |
| Sore throat | 0.354 | |||
| No | 343 (90.3) | 239 (91.2) | 104 (88.1) | |
| Yes | 37 (9.7) | 23 (8.8) | 14 (11.9) | |
| Runny nose | 0.104 | |||
| No | 364 (95.8) | 254 (96.9) | 100 (93.2) | |
| Yes | 16 (4.2) | 8 (3.1) | 8 (6.8) | |
| Fever | 0.181 | |||
| No | 346 (91.1) | 242 (92.4) | 104 (88.1) | |
| Yes | 34 (8.9) | 20 (7.6) | 14 (11.9) | |
| Shortness of breath | 0.650 | |||
| No | 357 (93.9) | 247 (94.3) | 110 (93.2) | |
| Yes | 23 (6.1) | 15 (5.7) | 8 (6.8) | |
| Diarrhoea | 0.648 | |||
| No | 375 (98.7) | 259 (98.9) | 116 (98.3) | |
| Yes | 5 (1.3) | 3 (1.1) | 2 (1.7) | |
| Nausea/Vomiting | 0.886 | |||
| No | 373 (98.2) | 257 (98.1) | 116 (98.3) | |
| Yes | 7 (1.8) | 5 (1.9) | 2 (1.7) | |
| Headache | <0.001 | |||
| No | 365 (96.1) | 258 (98.5) | 107 (90.7) | |
| Yes | 15 (3.9) | 4 (1.5) | 11 (9.30) | |
| Irritability | ||||
| No | 380 (100.0) | 262 (100.0) | 118 (100.0) | 0.999 |
| Yes | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Pain | 0.127 | |||
| No | 345 (90.8) | 242 (92.4) | 103 (87.3) | |
| Yes | 35 (9.2) | 20 (7.6) | 15 (12.7) | |
| General weakness | 0.030 | |||
| No | 347 (91.3) | 245 (93.5) | 102 (86.4) | |
| Yes | 33 (8.7) | 17 (6.5) | 16 (13.6) |
| Variable | cOR (95% CI) | p-Value |
|---|---|---|
| Categories of age (years) | ||
| <20 | 1 (Ref) | |
| 21–30 | 0.86 (0.34–2.18) | 0.753 |
| 31–40 | 1.28 (0.51–3.23) | 0.6 |
| 41–50 | 1.13 (0.40–3.14) | 0.822 |
| 51–94 | 0.91 (0.35–2.36) | 0.853 |
| Gender | ||
| Female | 1 (Ref) | |
| Male | 1.07 (0.68–1.67) | 0.773 |
| Clinical Symptoms | ||
| Asymptomatic | 1 (Ref) | |
| Symptomatic | 0.29 (0.18–0.46) | <0.001 |
| Cough | ||
| No | 1 (Ref) | |
| Yes | 0.19 (0.12–0.31) | <0.001 |
| Sore throat | ||
| No | 1 (Ref) | |
| Yes | 1.40 (0.69–2.83) | 0.35 |
| Runny nose | ||
| No | 1 (Ref) | |
| Yes | 2.31 (0.85–6.31) | 0.103 |
| Fever | ||
| No | 1 (Ref) | |
| Yes | 1.63 (0.79–3.45) | 0.185 |
| Shortness of breath | ||
| No | 1 (Ref) | |
| Yes | 1.20 (0.49–2.91) | 0.69 |
| Diarrhea | ||
| No | 1 (Ref) | |
| Yes | 1.49 (0.25–9.03) | 0.665 |
| Nausea/Vomiting | ||
| No | 1 (Ref) | |
| Yes | 0.89 (0.17–4.64) | 0.886 |
| Headache | ||
| No | 1 (Ref) | |
| Yes | 6.63 (2.07–21.29) | 0.001 |
| Pain | ||
| No | 1 (Ref) | |
| Yes | 1.76 (0.87–3.58) | 0.117 |
| General weakness | ||
| No | 1 (Ref) | |
| Yes | 2.26 (1.10–4.65) | 0.027 |
| Microbial Isolate | All Participants n = 380 (%) | SARS-CoV-2 Negative n = 262 (%) | SARS-CoV-2 Positive n = 118 (%) | p-Value |
|---|---|---|---|---|
| Acinetobacter baumannii | 0.862 | |||
| No | 368 (96.8) | 254 (96.9) | 114 (96.6) | |
| Yes | 12 (3.2) | 8 (3.1) | 4 (3.4) | |
| Candida spp. | 0.733 | |||
| No | 355 (93.4) | 244 (93.1) | 111 (94.1) | |
| Yes | 25 (6.6) | 18 (6.9) | 7 (5.9) | |
| Citrobacter spp. | 0.932 | |||
| No | 377 (99.2) | 260 (99.2) | 117 (99.2) | |
| Yes | 3 (0.8) | 2 (0.8) | 1 (0.8) | |
| Enterobacter spp. | 0.496 | |||
| No | 373 (98.2) | 258 (98.5) | 115 (97.5) | |
| Yes | 7 (1.8) | 4 (1.5) | 3 (2.5) | |
| Escherichia coli | 0.084 | |||
| No | 368 (96.8) | 251 (95.8) | 117 (99.2) | |
| Yes | 12 (3.2) | 11 (4.2) | 1 (0.8) | |
| Klebsiella spp. | 0.446 | |||
| No | 302 (79.5) | 227 (86.6) | 95 (80.5) | |
| Yes | 78 (20.5) | 35 (13.4) | 23 (19.5) | |
| Moraxella catarrhalis | 0.002 | |||
| No | 350 (92.1) | 234 (89.3) | 116 (98.3) | |
| Yes | 30 (7.9) | 28 (10.7) | 2 (1.7) | |
| Proteus spp. | 0.312 | |||
| No | 374 (98.4) | 259 (98.9) | 115 (97.5) | |
| Yes | 6 (1.6) | 3 (1.1) | 3 (2.5) | |
| Pseudomonas spp. | 0.803 | |||
| No | 356 (93.7) | 246 (93.9) | 110 (93.2) | |
| Yes | 24 (6.3) | 16 (6.1) | 8 (6.8) | |
| Serratia spp. | <0.001 | |||
| No | 368 (96.8) | 262 (100.0) | 106 (89.8) | |
| Yes | 12 (3.2) | 0 (0.0) | 12 (10.2) | |
| Stenotrophomonas maltophilia | 0.017 | |||
| No | 375 (98.7) | 261 (99.6) | 114 (96.6) | |
| Yes | 5 (1.3) | 1 (0.4) | 4 (3.4) | |
| Streptococcus pneumoniae | 0.502 | |||
| No | 379 (99.7) | 261 (99.6) | 118 (100.0) | |
| Yes | 1 (0.3) | 1 (0.4) | 0 (0.0) |
| Microbial Isolate | cOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|
| Moraxella catarrhalis | 0.14 (0.03–0.62) | 0.009 | 0.15 (0.04–0.64) | 0.010 |
| Stenotrophomonas maltophilia | 9.16 (1.01–82.84) | 0.049 | 8.32 (0.92–75.32) | 0.059 |
| Antibiotic | Acinetobacter baumannii (n = 4) | Enterobacter spp. (n = 3) | Escherichia coli (n = 1) | Klebsiella spp. (n = 23) | Moraxella catarrhalis (n = 2) | Proteus spp. (n = 3) | Pseudomonas spp. (n = 8) | Serratia spp. (n = 12) | Stenotrophomonas maltophilia (n = 4) |
|---|---|---|---|---|---|---|---|---|---|
| CRO | 4 (100.0) | 1 (33.3) | 1 (100.0) | 12 (52.2) | - | 1 (33.3) | - | 3 (25.0) | 4 (100.0) |
| CTX | 4 (100.0) | 1 (33.3) | 1 (100.0) | 9 (39.1) | - | 1 (33.3) | - | 2 (16.7) | 4 (100.0) |
| AZM | 0 (0.0) | 1 (33.3) | 1(100.0) | 7 (30.4) | - | 2 (66.7) | - | 5 (41.7) | 0 (0.0) |
| AMC | 4 (100.0) | 3 (100.0) | 1 (100.0) | 15 (65.2) | - | 3 (100.0) | - | 12 (100.0) | 4 (100.0) |
| CIP | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (13.0) | 1 (50.0) | 1 (33.3) | 0 (0.0) | 2 (16.7) | 1 (25.0) |
| GEN | 1 (25.0) | 0 (0.0) | 1 (100.0) | 2 (8.7) | 0 (0.0) | 1 (33.3) | 3 (37.5) | 0 (0.0) | 1(25.0) |
| CAZ | 2 (50.0) | 0 (0.0) | 1 (100.0) | 9 (39.1) | 0 (0.0) | 0 (0.0) | 3(37.5) | 1 (8.3) | 2 (25.0) |
| AK | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (37.5) | 0 (0.0) | 0 (0.0) |
| MEM | - | - | - | - | 0 (0.0) | - | 4 (50.0) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deberu, O.N.; Acheampong, G.; Nkrumah, B.; Ayisi-Boateng, N.K.; Afriyie, S.O.; Agyapong, F.O.; Owusu, D.O.; Mutocheluh, M.; Abdul-Karim, A.; El-Duah, P.; et al. Microbial Organisms in the Lower Respiratory Tract Associated with SARS-CoV-2 Infection: A Cross-Sectional Study in Northern Ghana. COVID 2023, 3, 440-451. https://doi.org/10.3390/covid3040033
Deberu ON, Acheampong G, Nkrumah B, Ayisi-Boateng NK, Afriyie SO, Agyapong FO, Owusu DO, Mutocheluh M, Abdul-Karim A, El-Duah P, et al. Microbial Organisms in the Lower Respiratory Tract Associated with SARS-CoV-2 Infection: A Cross-Sectional Study in Northern Ghana. COVID. 2023; 3(4):440-451. https://doi.org/10.3390/covid3040033
Chicago/Turabian StyleDeberu, Oliver Nangkuu, Godfred Acheampong, Bernard Nkrumah, Nana Kwame Ayisi-Boateng, Stephen Opoku Afriyie, Francis Opoku Agyapong, Dorcas Ohui Owusu, Mohamed Mutocheluh, Abass Abdul-Karim, Philip El-Duah, and et al. 2023. "Microbial Organisms in the Lower Respiratory Tract Associated with SARS-CoV-2 Infection: A Cross-Sectional Study in Northern Ghana" COVID 3, no. 4: 440-451. https://doi.org/10.3390/covid3040033
APA StyleDeberu, O. N., Acheampong, G., Nkrumah, B., Ayisi-Boateng, N. K., Afriyie, S. O., Agyapong, F. O., Owusu, D. O., Mutocheluh, M., Abdul-Karim, A., El-Duah, P., Sylverken, A. A., & Owusu, M. (2023). Microbial Organisms in the Lower Respiratory Tract Associated with SARS-CoV-2 Infection: A Cross-Sectional Study in Northern Ghana. COVID, 3(4), 440-451. https://doi.org/10.3390/covid3040033