
Real-World Safety and Effectiveness of Remdesivir and Corticosteroids in Hospitalized Patients with COVID-19

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
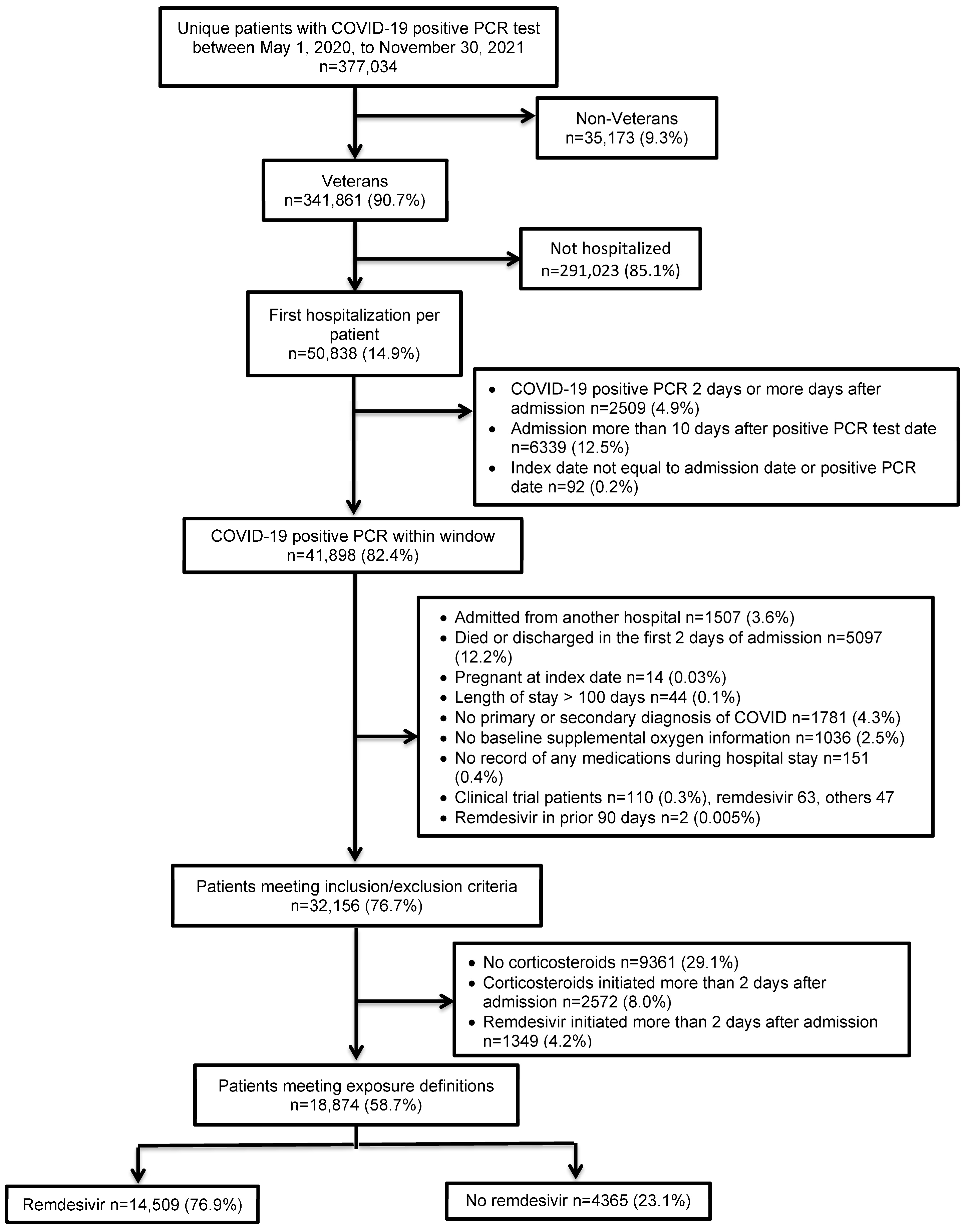
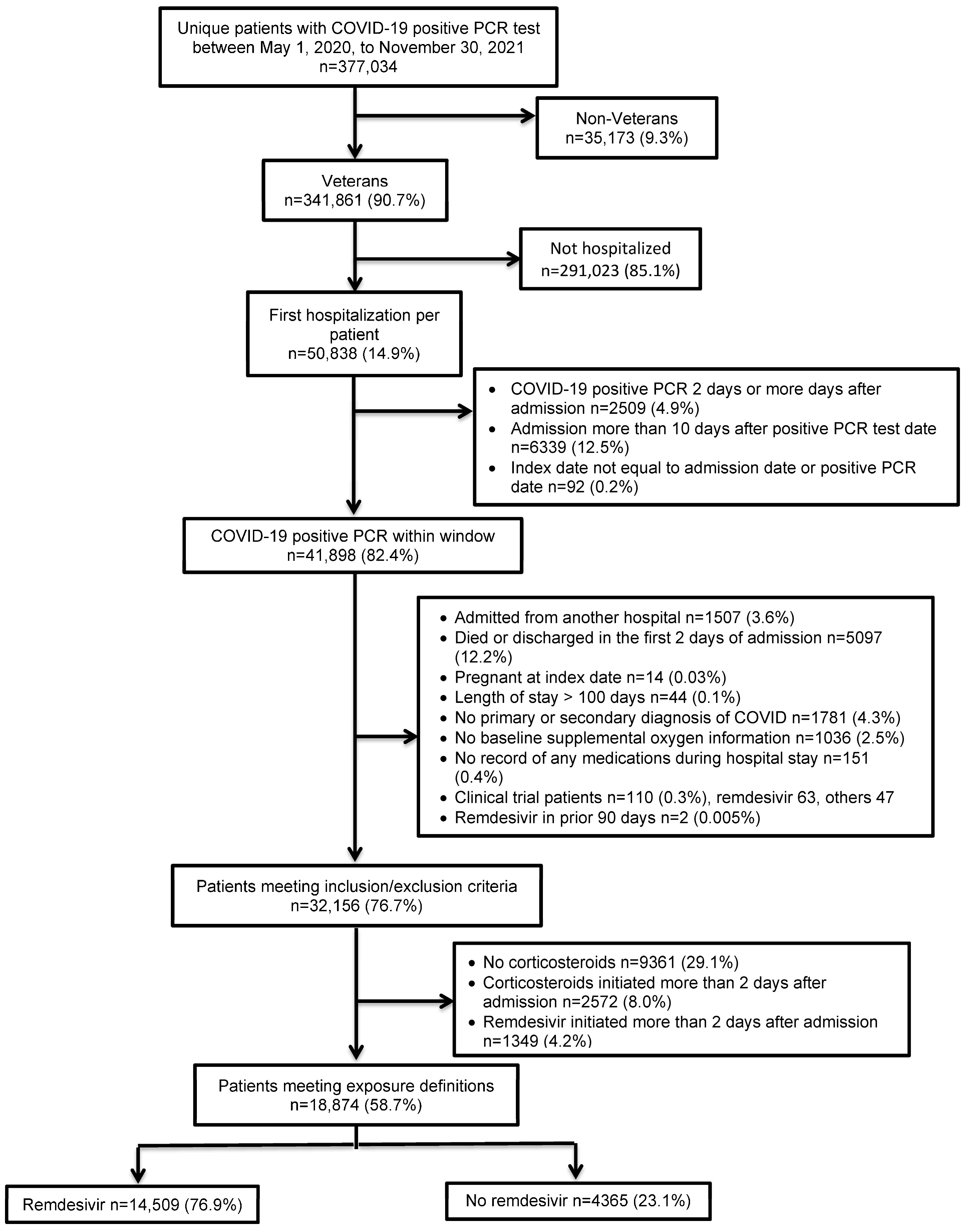
2.2. Study Population
2.3. Outcomes
2.4. Variables
2.5. Statistical Analyses
3. Results
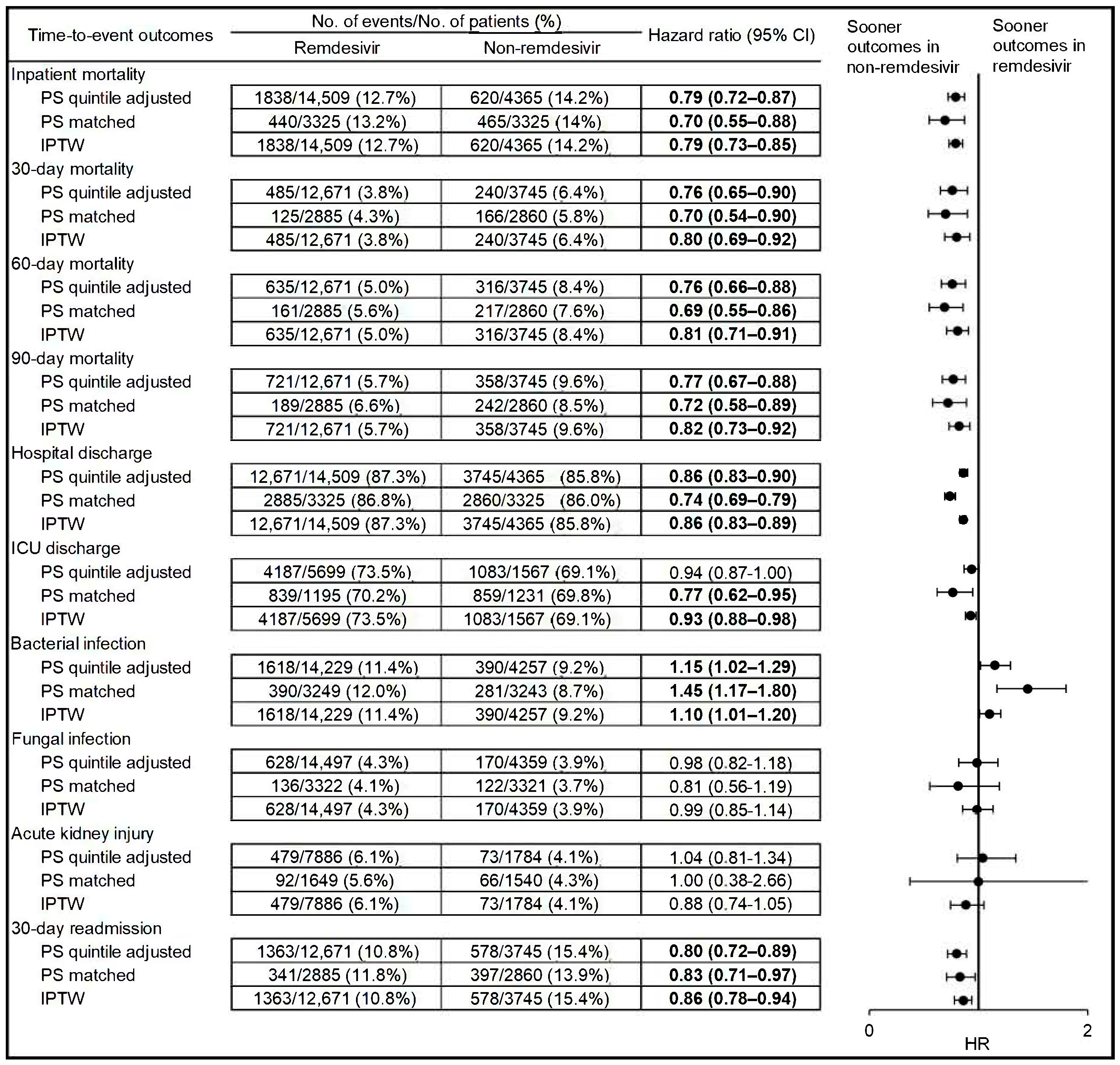
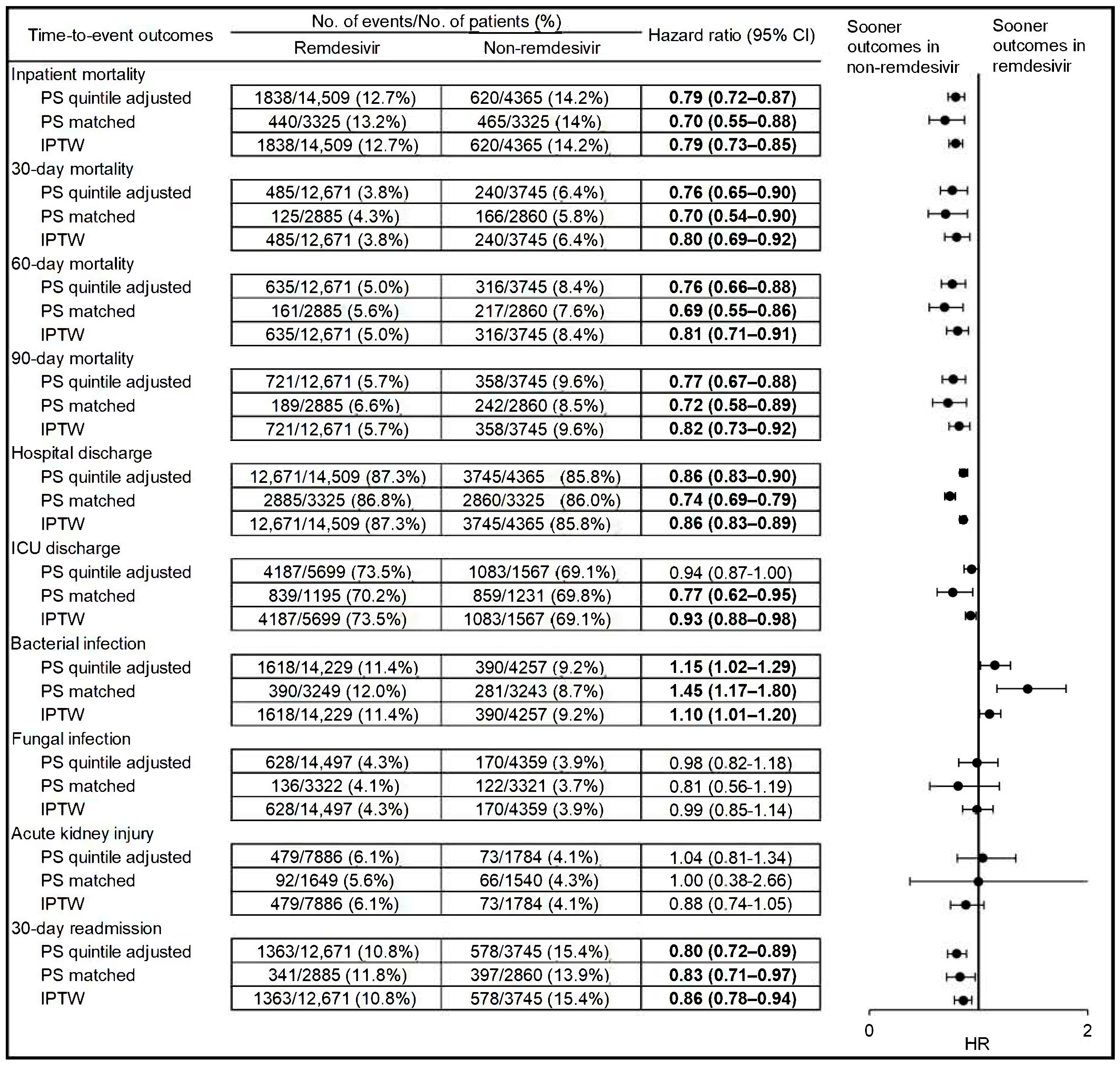
3.1. Time-to-Event Outcomes
3.2. Sensitivity and Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gilead Sciences I. Veklury® (Remdesivir) Prescribing Information. Available online: https://www.gilead.com/-/media/files/pdfs/medicines/covid-19/veklury/veklury_pi.pdf (accessed on 4 August 2022).
- WHO. Therapeutics and COVID-19: Living Guideline, 16 September 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2022.5 (accessed on 11 October 2022).
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://covid19treatmentguidelines.nih.gov/ (accessed on 8 August 2022).
- Infectious Diseases Society of America Guidelines. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Available online: https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/ (accessed on 8 August 2022).
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Preliminary report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Peto, R.; Henao-Restrepo, A.M.; WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.-P.; Peytavin, G.; Staub, T.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2022, 22, 209–221. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Zeger, S.L.; Bandeen-Roche, K.; Wang, M.-C.; Alexander, G.C.; Gupta, A.; Bollinger, R.; Xu, Y. Comparison of Time to Clinical Improvement with vs. without Remdesivir Treatment in Hospitalized Patients with COVID-19. JAMA Netw. Open 2021, 4, e213071. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Betz, J.; Alexander, G.C.; Andersen, K.M.; Joseph, C.S.; Mehta, H.B.; Korwek, K.; E Sands, K.; et al. Real-World Effectiveness of Remdesivir in Adults Hospitalized with Coronavirus Disease 2019 (COVID-19): A Retrospective, Multicenter Comparative Effectiveness Study. Clin. Infect. Dis. 2021, 75, e516–e524. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Betz, J.; Alexander, G.C.; Andersen, K.M.; Joseph, C.S.; Mehta, H.B.; Korwek, K.; E Sands, K.; et al. Effectiveness of remdesivir with and without dexamethasone in hospitalized patients with COVID-19. medRxiv 2020. medRxiv:2020.11.19.20234153. [Google Scholar]
- Olender, S.A.; Perez, K.K.; Go, A.S.; Balani, B.; Price-Haywood, E.G.; Shah, N.S.; Wang, S.; Walunas, T.L.; Swaminathan, S.; Slim, J.; et al. Remdesivir for Severe Coronavirus Disease 2019 (COVID-19) Versus a Cohort Receiving Standard of Care. Clin. Infect. Dis. 2020, 73, e4166–e4174. [Google Scholar] [CrossRef]
- Lapadula, G.; Bernasconi, D.P.; Bellani, G.; Soria, A.; Rona, R.; Bombino, M.; Avalli, L.; Rondelli, E.; Cortinovis, B.; Colombo, E.; et al. Remdesivir Use in Patients Requiring Mechanical Ventilation due to COVID-19. Open Forum Infect. Dis. 2020, 7, ofaa481. [Google Scholar] [CrossRef]
- Larson, D.T.; Ewers, E.C.; Gallagher, K.M.; Mahoney, A.M.; Paul, M.L.; Weina, P.J. Real World Impact of Remdesivir and Dexamethasone on Clinical Outcomes of Severe Coronavirus Disease 2019 in a Community Hospital. Mil. Med. 2022, usac052. [Google Scholar] [CrossRef]
- Ohl, M.E.; Miller, D.R.; Lund, B.C.; Kobayashi, T.; Miell, K.R.; Beck, B.F.; Alexander, B.; Crothers, K.; Sarrazin, M.S.V. Association of Remdesivir Treatment with Survival and Length of Hospital Stay Among US Veterans Hospitalized with COVID-19. JAMA Netw. Open 2021, 4, e2114741. [Google Scholar] [CrossRef]
- Lim, H.; Palaiodimos, L.; Berto, C.G.; Tedunjaiye, O.; Malik, P.; Nagraj, S.; Choi, H.; Seng, N.S.H.L.; Kladas, M.; Kharawala, A.; et al. Remdesivir in the Treatment of COVID-19: A Propensity Score-Matched Analysis from a Public Hospital in New York City Assessing Renal and Hepatic Safety. J. Clin. Med. 2022, 11, 3132. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.X.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Mozaffari, E.; Chandak, A.; Zhang, Z.; Liang, S.; Thrun, M.; Gottlieb, R.L.; Kuritzkes, D.R.; E Sax, P.; A Wohl, D.; Casciano, R.; et al. Remdesivir Treatment in Hospitalized Patients with Coronavirus Disease 2019 (COVID-19): A Comparative Analysis of In-hospital All-cause Mortality in a Large Multicenter Observational Cohort. Clin. Infect. Dis. 2021, 75, e450–e458. [Google Scholar] [CrossRef]
- Gressens, S.B.; Esnault, V.; De Castro, N.; Sellier, P.; Sene, D.; Chantelot, L.; Hervier, B.; Delaugerre, C.; Chevret, S.; Molina, J.-M.; et al. Remdesivir in combination with dexamethasone for patients hospitalized with COVID-19: A retrospective multicenter study. PLoS ONE 2022, 17, e0262564. [Google Scholar] [CrossRef]
- Lee, T.C.; Murthy, S.; Del Corpo, O.; Senécal, J.; Butler-Laporte, G.; Sohani, Z.N.; Brophy, J.M.; McDonald, E.G. Remdesivir for the treatment of COVID-19: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 1203–1210. [Google Scholar] [CrossRef]
- China National Health Commission. Chinese Clinical Guidance for COVID-19 Pneumonia Diagnosis and Treatment. Available online: http://kjfy.meetingchina.org/msite/news/show/cn/3337.html (accessed on 8 August 2022).
- Cano, E.J.; Fuentes, X.F.; Campioli, C.C.; O’Horo, J.C.; Abu Saleh, O.; Odeyemi, Y.; Yadav, H.; Temesgen, Z. Impact of Corticosteroids in Coronavirus Disease 2019 Outcomes: Systematic Review and Meta-analysis. Chest 2020, 159, 1019–1040. [Google Scholar] [CrossRef]
- Wang, J.; Yang, W.; Chen, P.; Guo, J.; Liu, R.; Wen, P.; Li, K.; Lu, Y.; Ma, T.; Li, X.; et al. The proportion and effect of corticosteroid therapy in patients with COVID-19 infection: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0249481. [Google Scholar] [CrossRef]
- Bahl, A.; Johnson, S.; Chen, N.-W. Timing of corticosteroids impacts mortality in hospitalized COVID-19 patients. Intern. Emerg. Med. 2021, 16, 1593–1603. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2000. [Google Scholar]
- Johnson, M.L.; Crown, W.; Martin, B.C.; Dormuth, C.R.; Siebert, U. Good Research Practices for Comparative Effectiveness Research: Analytic Methods to Improve Causal Inference from Nonrandomized Studies of Treatment Effects Using Secondary Data Sources: The ISPOR Good Research Practices for Retrospective Database Analysis Task Force Report—Part III. Value Health 2009, 12, 1062–1073. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Rubin, D.B. Estimating causal effects from large data sets using propensity scores. Ann. Intern. Med. 1997, 127 (8 Pt 2), 757–763. [Google Scholar] [CrossRef]
- Schneeweiss, S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiol. Drug Saf. 2006, 15, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. The design versus the analysis of observational studies for causal effects: Parallels with the design of randomized trials. Stat. Med. 2007, 26, 20–36. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Using propensity scores to help design observational studies: Application to the tobacco litigation. Health Serv. Outcomes Res. Methodol. 2001, 2, 169–188. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Survival Analysis: Regression Modeling of Time to Event Data; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1999. [Google Scholar]
- Hernán, M.A.; Robins, J.M. Causal Inference; Chapman & Hall/CRC, Forthcoming: Boca Raton, FL, USA, 2016. [Google Scholar]
- Austin, P.C. Variance estimation when using inverse probability of treatment weighting (IPTW) with survival analysis. Stat. Med. 2016, 35, 5642–5655. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Gilead. Veklury MOA, December 2022. Available online: https://www.vekluryhcp.com/about/about-moa.php (accessed on 30 January 2023).
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines–Immunomodulators-Orticosteroids. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/immunomodulators/corticosteroids/ (accessed on 30 January 2023).
- Divyansh, B.; Ankit, A.; Manasvi, G.; Gaurav, M.; Kurt, H.; Umesha, B. Dexamethasone versus Methylprednisolone in Hospitalized COVID-19 Patients: A Systematic Review and Meta-Analysis. Int. J. Crit. Care Emerg. Med. 2021, 7, 128. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Wang, X.Q.; Iwashyna, T.J.; Prescott, H.C. Readmission and Death After Initial Hospital Discharge Among Patients with COVID-19 in a Large Multihospital System. JAMA 2021, 325, 304–306. [Google Scholar] [CrossRef]
- Finn, A.; Jindal, A.; Andrea, S.B.; Selvaraj, V.; Dapaah-Afriyie, K. Association of Treatment with Remdesivir and 30-day Hospital Readmissions in Patients Hospitalized with COVID-19. Am. J. Med. Sci. 2022, 363, 403–410. [Google Scholar] [CrossRef]
- Lucijanic, M.; Cikara, T.; Bistrovic, P.; Papic, I.; Hadziabdic, M.O.; Busic, N.; Lackovic, M.; Cesar, N.; Koscak, V.; Mitrovic, J.; et al. Remdesivir use in COVID-19 patients might predispose bacteremia, matched case-control analysis. J. Infect. 2022, 85, 174–211. [Google Scholar] [CrossRef]
- Alam, M.S.; Costales, M.G.; Cavanaugh, C.; Williams, K. Extracellular Adenosine Generation in the Regulation of Pro-Inflammatory Responses and Pathogen Colonization. Biomolecules 2015, 5, 775–792. [Google Scholar] [CrossRef]
- Antonioli, L.; Pacher, P.; Vizi, E.S.; Haskó, G. CD39 and CD73 in immunity and inflammation. Trends Mol. Med. 2013, 19, 355–367. [Google Scholar] [CrossRef]
- Markovskaya, Y.; Gavioli, E.M.; Cusumano, J.A.; Glatt, A.E. Coronavirus disease 2019 (COVID-19): Secondary bacterial infections and the impact on antimicrobial resistance during the COVID-19 pandemic. Antimicrob. Steward. Heal. Epidemiol. 2022, 2, e114. [Google Scholar] [CrossRef]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Lopez, A.A.; Diez-Remesal, Y.; Castro, N.M.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502. [Google Scholar] [CrossRef]
- Dupper, A.C.M.; Malik, Y.; Cusumano, J.A.P.; Nadkarni, D.B.; Banga, J.; Caban, A.B.; Twyman, K.; Obla, A.; Patel, D.M.; Mazo, D.M.; et al. Longer Steroid Treatment Increases Secondary Bloodstream Infection Risk among Patients with COVID-19 Requiring Intensive Care. Infect. Dis. Clin. Pr. 2022, 30, 1188. [Google Scholar] [CrossRef]
- Ackley, T.W.; McManus, D.; Topal, J.E.; Cicali, B.; Shah, S. A Valid Warning or Clinical Lore: An Evaluation of Safety Outcomes of Remdesivir in Patients with Impaired Renal Function from a Multicenter Matched Cohort. Antimicrob. Agents Chemother. 2021, 65, e02290-20. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Overall | Matched | |||||
|---|---|---|---|---|---|---|
| Demographics | Remdesivir | Non-Remdesivir | Std Diff | Remdesivir | Non-Remdesivir | Std Diff |
| N = 14,509 | N = 4365 | N = 3325 | N = 3325 | |||
| Age (years), mean (SD) | 66.7 (13.8) | 68.9 (13.5) | −0.16 | 68.2 (13.5) | 68.4 (13.6) | −0.02 |
| BMI, mean (SD) | 31.3 (7.2) | 29.7 (7.2) | 0.22 | 30.6 (7.1) | 30.1 (7.3) | 0.06 |
| Severe obesity (BMI ≥40) | 1540 (10.7%) | 357 (8.2%) | 0.08 | 307 (9.3%) | 304 (9.2%) | 0 |
| Obesity (BMI ≥30) | 6136 (42.4%) | 1579 (36.3%) | 0.13 | 1253 (37.9%) | 1256 (37.9%) | 0 |
| Male | 13,705 (94.5%) | 4144 (94.9%) | −0.02 | 3168 (95.3%) | 3150 (94.7%) | 0.02 |
| Race | ||||||
| White | 9960 (68.6%) | 2802 (64.2%) | 0.09 | 2208 (66.4%) | 2247 (67.6%) | −0.02 |
| Black/African American | 3053 (21.0%) | 1172 (26.9%) | −0.14 | 799 (24.0%) | 773 (23.3%) | 0.02 |
| Asian | 155 (1.1%) | 30 (0.7%) | 0.04 | 26 (0.8%) | 25 (0.8%) | 0 |
| All other | 1341 (9.2%) | 361 (8.3%) | 0.03 | 292 (8.8%) | 280 (8.4%) | 0.01 |
| Hispanic or Latino | 1442 (9.9%) | 389 (8.9%) | 0.04 | 293 (8.8%) | 279 (8.4%) | 0.02 |
| Married | 7664 (52.8%) | 2168 (49.7%) | 0.06 | 1704 (51.3%) | 1673 (50.3%) | 0.02 |
| Admit source | ||||||
| Direct/outpatient | 14,296 (98.5%) | 4258 (97.5%) | 0.07 | 3255 (97.9%) | 3262 (98.1%) | −0.02 |
| Nursing home | 213 (1.5%) | 107 (2.4%) | −0.07 | 70 (2.1%) | 63 (1.9%) | 0.02 |
| Admit specialty | ||||||
| ICU | 2914 (20.1%) | 851 (19.5%) | 0.01 | 644 (19.4%) | 654 (19.7%) | −0.01 |
| Medicine | 10,953 (75.5%) | 3263 (74.5%) | 0.02 | 2527 (76.0%) | 2506 (75.4%) | 0.01 |
| Surgery | 642 (4.4%) | 251 (5.7%) | −0.06 | 154 (4.6%) | 165 (5.0%) | −0.02 |
| Rurality | ||||||
| Urban | 10,919 (75.3%) | 3279 (75.1%) | 0 | 2480 (74.6%) | 2496 (75.1%) | −0.01 |
| Rural | 951 (6.6%) | 272 (6.2%) | 0.01 | 206 (6.2%) | 220 (6.6%) | −0.02 |
| Other/missing | 2639 (18.2%) | 814 (18.7%) | −0.01 | 639 (19.2%) | 609 (18.3%) | 0.02 |
| Patient active in past 24 months | 14,164 (97.6%) | 4261 (97.6%) | 0 | 3243 (97.5%) | 3240 (97.4%) | 0.01 |
| Primary care visit in past 18 months | 13,584 (93.6%) | 4088 (93.7%) | 0 | 3100 (93.2%) | 3105 (93.4%) | −0.01 |
| ICU during current admission | 5699 (39.3%) | 1567 (35.9%) | 0.07 | 1195 (35.9%) | 1231 (37.0%) | −0.02 |
| Healthcare exposures, 30 days prior to admission | ||||||
| Hospitalization | 187 (1.3%) | 95 (2.2%) | −0.07 | 46 (1.4%) | 55 (1.6%) | −0.02 |
| Nursing home | 7 (0.05%) | 6 (0.1%) | −0.03 | <5 (<0.1%) | <5 (<0.1%) | 0 |
| Intensive care | 29 (0.2%) | 18 (0.4%) | −0.04 | 6 (0.2%) | 10 (0.3%) | −0.02 |
| Infection, 90 days prior to index date a | ||||||
| Bacterial infection | 471 (3.3%) | 214 (4.9%) | −0.08 | 132 (4.0%) | 124 (3.7%) | 0.01 |
| Fungal infection | 19 (0.1%) | 13 (0.3%) | −0.04 | <5 (<0.1%) | 6 (0.2%) | −0.02 |
| Baseline supplemental oxygen | ||||||
| Mechanical | ||||||
| ventilator/ECMO | 586 (4.0%) | 188 (4.3%) | −0.01 | 153 (4.6%) | 148 (4.4%) | 0.01 |
| Non-invasive ventilator | 1363 (9.4%) | 315 (7.2%) | 0.08 | 233 (7.0%) | 268 (8.1%) | −0.04 |
| Supplemental oxygen | 11,029 (76.0%) | 2893 (66.3%) | 0.22 | 2357 (70.9%) | 2381 (71.6%) | −0.02 |
| No supplemental oxygen | 1531 (10.6%) | 969 (22.2%) | −0.32 | 582 (17.5%) | 528 (15.9%) | 0.04 |
| Vaccine status prior to index date | ||||||
| Fully vaccinated | 1690 (11.7%) | 665 (15.2%) | −0.11 | 411 (12.4%) | 441 (13.3%) | −0.03 |
| Booster | 78 (4.6%) | 37 (5.6%) | −0.04 | 19 (4.6%) | 23 (5.2%) | −0.02 |
| Partially vaccinated | 417 (2.9%) | 113 (2.6%) | 0.02 | 90 (2.7%) | 86 (2.6%) | 0.01 |
| No vaccination | 12,402 (85.5%) | 3587 (82.2%) | 0.09 | 2824 (84.9%) | 2798 (84.2%) | 0.02 |
| Duration of remdesivir | ||||||
| mean (SD) | 4.9 (1.9) | -- | 4.8 (1.9) | -- | ||
| Overall | Matched | |||||
|---|---|---|---|---|---|---|
| Medical History in the 2 Years Prior to Index Date | Remdesivir | Non-Remdesivir | Std Diff | Remdesivir | Non-Remdesivir | Std Diff |
| N = 14,509 | N = 4365 | N = 3325 | N = 3325 | |||
| Charlson comorbidity index, median (IQR) | ||||||
| 2 (0–4) | 3 (1–5) | −0.33 | 2 (1–4) | 2 (1–4) | 0.02 | |
| Elixhauser score, median (IQR) | 4 (0–14) | 9 (0–21) | −0.35 | 6 (0–17) | 6 (0–17) | −0.02 |
| Acute cardiac injury | 521 (3.6%) | 263 (6.0%) | −0.11 | 164 (4.9%) | 153 (4.6%) | 0.02 |
| Acute liver injury | 35 (0.2%) | 11 (0.3%) | 0 | 13 (0.4%) | 8 (0.2%) | 0.03 |
| Acute myocardial infarction | 521 (3.6%) | 262 (6.0%) | −0.11 | 164 (4.9%) | 152 (4.6%) | 0.02 |
| Acute respiratory failure | 1552 (10.7%) | 659 (15.1%) | −0.13 | 440 (13.2%) | 415 (12.5%) | 0.02 |
| Acute kidney failure | 1675 (11.5%) | 908 (20.8%) | −0.25 | 484 (14.6%) | 540 (16.2%) | −0.05 |
| Acute kidney injury | 3238 (22.3%) | 1663 (38.1%) | −0.35 | 955 (28.7%) | 989 (29.7%) | −0.02 |
| Alcohol dependence | 2180 (15.0%) | 695 (15.9%) | −0.02 | 534 (16.1%) | 540 (16.2%) | 0 |
| Anxiety | 2452 (16.9%) | 758 (17.4%) | −0.01 | 539 (16.2%) | 566 (17.0%) | −0.02 |
| Acute respiratory distress syndrome | ||||||
| 17 (0.1%) | 9 (0.2%) | −0.02 | <5 (<0.1%) | 5 (0.1%) | −0.01 | |
| Arrhythmia | 743 (5.1%) | 235 (5.4%) | −0.01 | 161 (4.8%) | 163 (4.9%) | 0 |
| Asthma | 1144 (7.9%) | 338 (7.7%) | 0.01 | 253 (7.6%) | 267 (8.0%) | −0.02 |
| Bronchitis | 1338 (9.2%) | 486 (11.1%) | −0.06 | 328 (9.9%) | 336 (10.1%) | −0.01 |
| Coronary atherosclerosis and other heart disease | ||||||
| 3905 (26.9%) | 1481 (33.9%) | −0.15 | 986 (29.7%) | 1032 (31.0%) | −0.03 | |
| Cancer | 3466 (23.9%) | 1155 (26.5%) | −0.06 | 855 (25.7%) | 825 (24.8%) | 0.02 |
| Cardiomyopathy | 722 (5.0%) | 313 (7.2%) | −0.09 | 209 (6.3%) | 194 (5.8%) | 0.02 |
| Cerebrovascular disease | 411 (2.8%) | 175 (4.0%) | −0.06 | 129 (3.9%) | 115 (3.5%) | 0.02 |
| Congestive heart failure | 1945 (13.4%) | 942 (21.6%) | −0.22 | 546 (16.4%) | 578 (17.4%) | −0.03 |
| Chronic lung disease | 5715 (39.4%) | 1897 (43.5%) | −0.08 | 1369 (41.2%) | 1385 (41.7%) | −0.01 |
| Cirrhosis | 398 (2.7%) | 203 (4.7%) | −0.10 | 124 (3.7%) | 118 (3.6%) | 0.01 |
| Chronic obstructive pulmonary disease | ||||||
| 3714 (25.6%) | 1283 (29.4%) | −0.09 | 953 (28.7%) | 936 (28.2%) | 0.01 | |
| Cardiovascular disease including hypertension | ||||||
| 6385 (44.0%) | 2342 (53.7%) | −0.19 | 1581 (47.5%) | 1632 (48.1%) | −0.03 | |
| Dementia | 882 (6.1%) | 412 (9.4%) | −0.13 | 264 (7.9%) | 263 (7.9%) | 0 |
| Diabetes | 6630 (45.7%) | 2118 (48.5%) | −0.06 | 1518 (45.7%) | 1517 (45.6%) | 0 |
| Diabetes type I | 271 (4.1%) | 138 (6.5%) | −0.08 | 76 (5.0%) | 75 (4.9%) | 0 |
| Diabetes type II | 6597 (99.5%) | 2107 (99.5%) | −0.06 | 1513 (99.7%) | 1509 (99.5%) | 0 |
| Non-alcohol drug dependency | 504 (3.5%) | 230 (5.3%) | −0.09 | 152 (4.6%) | 143 (4.3%) | 0.01 |
| Emphysema | 477 (3.3%) | 129 (3.0%) | 0.02 | 116 (3.5%) | 107 (3.2%) | 0.02 |
| Epilepsy | 212 (1.5%) | 82 (1.9%) | −0.03 | 56 (1.7%) | 53 (1.6%) | 0.01 |
| Heart disease | 4933 (34.0%) | 1909 (43.7%) | −0.20 | 1254 (37.7%) | 1306 (39.3%) | −0.03 |
| Heart failure | 2329 (16.1%) | 1101 (25.2%) | −0.23 | 651 (19.6%) | 677 (20.4%) | −0.02 |
| Human immunodeficiency virus | ||||||
| 123 (0.9%) | 44 (1.0%) | −0.02 | 35 (1.1%) | 29 (0.9%) | 0.02 | |
| Hypertension | 10,533 (72.6%) | 3407 (78.1%) | −0.13 | 2469 (74.3%) | 2501 (75.2%) | −0.02 |
| Hyperlipidemia | 9662 (66.6%) | 2891 (66.2%) | 0.01 | 2168 (65.2%) | 2185 (65.7%) | −0.01 |
| Inflammatory bowel disease | 510 (3.5%) | 198 (4.5%) | −0.05 | 131 (3.9%) | 124 (3.7%) | 0.01 |
| Influenza | 342 (2.4%) | 117 (2.7%) | −0.02 | 83 (2.5%) | 82 (2.5%) | 0 |
| Ischemic stroke | 908 (6.3%) | 381 (8.7%) | −0.09 | 248 (7.5%) | 240 (7.2%) | 0.01 |
| Chronic kidney disease | 4381 (30.2%) | 1999 (45.8%) | −0.33 | 1247 (37.5%) | 1249 (37.6%) | 0 |
| Liver disease | 1194 (8.2%) | 402 (9.2%) | −0.03 | 295 (8.9%) | 267 (8.0%) | 0.03 |
| Lower respiratory infection | 1340 (9.2%) | 446 (10.2%) | −0.03 | 308 (9.3%) | 320 (9.6%) | −0.01 |
| Major depressive disorder | 4396 (30.3%) | 1310 (30.0%) | 0.01 | 1018 (30.6%) | 971 (29.2%) | 0.03 |
| Metastatic tumor | 297 (2.1%) | 149 (3.4%) | −0.08 | 93 (2.8%) | 85 (2.6%) | 0.01 |
| Obesity hypoventilation | 160 (1.1%) | 42 (1.0%) | 0.01 | 37 (1.1%) | 32 (1.0%) | 0.01 |
| Obstructive sleep apnea | 5229 (36.0%) | 1455 (33.3%) | 0.06 | 1137 (34.2%) | 1116 (33.6%) | 0.01 |
| Peripheral artery disease | 2234 (15.4%) | 945 (21.7%) | −0.16 | 582 (17.5%) | 604 (18.2%) | −0.02 |
| Parkinson’s disease | 247 (1.7%) | 90 (2.1%) | −0.03 | 53 (1.6%) | 65 (2.0%) | −0.03 |
| Pneumonia | 1546 (10.7%) | 675 (15.5%) | −0.14 | 434 (13.1%) | 425 (12.8%) | 0.01 |
| Post-traumatic stress disorder | 2909 (20.1%) | 838 (19.2%) | 0.02 | 649 (19.5%) | 636 (19.1%) | 0.01 |
| Pulmonary heart disease | 595 (4.1%) | 280 (6.4%) | −0.10 | 150 (4.5%) | 174 (5.2%) | −0.03 |
| Pulmonary fibrosis | 257 (1.8%) | 59 (1.4%) | 0.03 | 49 (1.5%) | 44 (1.3%) | 0.01 |
| Septic shock | 641 (4.4%) | 308 (7.1%) | −0.11 | 182 (5.5%) | 194 (5.8%) | −0.02 |
| Smoking status | ||||||
| Current | 1408 (9.7%) | 491 (11.3%) | −0.05 | 362 (10.9%) | 347 (10.4%) | 0.01 |
| Former | 6801 (46.9%) | 1982 (45.4%) | 0.03 | 1555 (46.8%) | 1544 (46.4%) | 0.01 |
| Venous thromboembolism | 545 (3.8%) | 235 (5.4%) | −0.08 | 143 (4.3%) | 150 (4.5%) | −0.01 |
| Overall | Matched | |||||
|---|---|---|---|---|---|---|
| Symptoms 30 Days Prior to Index Date | Remdesivir N = 14,509 | Non-Remdesivir N = 4365 | Std Diff | Remdesivir N = 3325 | Non-Remdesivir N = 3325 | Std Diff |
| Abdominal pain | 684 (4.7%) | 256 (5.9%) | −0.05 | 177 (5.3%) | 172 (5.2%) | 0.01 |
| Chills | 1874 (12.9%) | 385 (8.8%) | 0.13 | 322 (9.7%) | 328 (9.9%) | −0.01 |
| Common cold | 4417 (30.4%) | 1197 (27.4%) | 0.07 | 961 (28.9%) | 952 (28.6%) | 0.01 |
| Cough (new onset) | 8902 (61.4%) | 2308 (52.9%) | 0.17 | 1858 (55.9%) | 1865 (56.1%) | 0.00 |
| Diarrhea | 3356 (23.1%) | 948 (21.7%) | 0.03 | 721 (21.7%) | 725 (21.8%) | 0.00 |
| Dyspnea (shortness of breath) | 9343 (64.4%) | 2545 (58.3%) | 0.13 | 2031 (61.1%) | 2040 (61.4%) | −0.01 |
| Malaise (fatigue) | 3995 (27.5%) | 1204 (27.6%) | 0.00 | 899 (27.0%) | 885 (26.6%) | 0.01 |
| Fever (>100.4 F) | 7980 (55.0%) | 2085 (47.8%) | 0.15 | 1675 (50.4%) | 1666 (50.1%) | 0.01 |
| Headache | 3125 (21.5%) | 676 (15.5%) | 0.16 | 596 (17.9%) | 577 (17.4%) | 0.02 |
| Loss of smell | 702 (4.8%) | 158 (3.6%) | 0.06 | 137 (4.1%) | 132 (4.0%) | 0.01 |
| Loss of taste | 1700 (11.7%) | 368 (8.4%) | 0.11 | 333 (10.0%) | 310 (9.3%) | 0.02 |
| Muscle aches (myalgia) | 1531 (10.6%) | 313 (7.2%) | 0.12 | 268 (8.1%) | 255 (7.7%) | 0.01 |
| Nausea/vomiting | 2922 (20.1%) | 806 (18.5%) | 0.04 | 648 (19.5%) | 622 (18.7%) | 0.02 |
| Runny nose (rhinorrhea) | 711 (4.9%) | 159 (3.6%) | 0.06 | 109 (3.3%) | 132 (4.0%) | −0.04 |
| Sore throat | 1097 (7.6%) | 255 (5.8%) | 0.07 | 216 (6.5%) | 205 (6.2%) | 0.01 |
| No record of symptoms | 1528 (10.5%) | 633 (14.5%) | −0.12 | 398 (12.0%) | 447 (13.4%) | −0.04 |
| Overall | Matched | |||||
|---|---|---|---|---|---|---|
| Medications | Remdesivir | Non-Remdesivir | Std Diff | Remdesivir | Non-Remdesivir | Std Diff |
| N = 14,509 | N = 4365 | N = 3325 | N = 3325 | |||
| Anticoagulant/antiplatelets | ||||||
| Previous | 2773 (19.1%) | 1094 (25.1%) | −0.14 | 682 (20.5%) | 743 (22.4%) | −0.04 |
| Baseline | 13,719 (94.6%) | 3905 (89.5%) | 0.19 | 3061 (92.1%) | 3064 (92.2%) | 0 |
| Concomitant | 14,068 (97.0%) | 3998 (91.6%) | 0.23 | 3140 (94.4%) | 3167 (95.3%) | −0.04 |
| Corticosteroids | ||||||
| Previous | 1344 (9.3%) | 645 (14.8%) | −0.17 | 393 (11.8%) | 384 (11.6%) | 0.01 |
| Baseline | 14,509 (100%) | 4365 (100%) | 0 | 3325 (100%) | 3325 (100%) | 0 |
| Concomitant | 14,443 (99.6%) | 4365 (100%) | −0.10 | 3303 (99.3%) | 3325 (100%) | −0.12 |
| Statins | ||||||
| Previous | 7324 (50.5%) | 2253 (51.6%) | −0.02 | 1636 (49.2%) | 1658 (49.9%) | −0.01 |
| Baseline | 7207 (49.7%) | 2191 (50.2%) | −0.01 | 1640 (49.3%) | 1630 (49.0%) | 0.01 |
| Concomitant | 7469 (51.5%) | 2241 (51.3%) | 0 | 1688 (50.8%) | 1683 (50.6%) | 0 |
| Antibiotics | ||||||
| Previous | 1858 (12.8%) | 694 (15.9%) | −0.09 | 480 (14.4%) | 459 (13.8%) | 0.02 |
| Baseline | 6027 (41.5%) | 1959 (44.9%) | −0.07 | 1468 (44.2%) | 1420 (42.7%) | 0.03 |
| Concomitant | 6667 (46.0%) | 2261 (51.8%) | −0.12 | 1638 (49.3%) | 1637 (49.2%) | 0 |
| NSAIDs | ||||||
| Previous | 4449 (30.7%) | 1396 (32.0%) | −0.03 | 1045 (31.4%) | 1036 (31.2%) | 0.01 |
| Baseline | 4957 (34.2%) | 1578 (36.2%) | −0.04 | 1195 (35.9%) | 1186 (35.7%) | 0.01 |
| Concomitant | 5344 (36.8%) | 1704 (39.0%) | −0.05 | 1314 (39.5%) | 1283 (38.6%) | 0.02 |
| Melatonin | ||||||
| Previous | 1006 (6.9%) | 371 (8.5%) | −0.06 | 247 (7.4%) | 233 (7.0%) | 0.02 |
| Baseline | 3144 (21.7%) | 905 (20.7%) | 0.02 | 704 (21.2%) | 664 (20.0%) | 0.03 |
| Concomitant | 4363 (30.1%) | 1259 (28.8%) | 0.03 | 972 (29.2%) | 933 (28.1%) | 0.03 |
| ACE inhibitors | ||||||
| Previous | 3756 (25.9%) | 1052 (24.1%) | 0.04 | 828 (24.9%) | 831 (25.0%) | 0 |
| Baseline | 2448 (16.9%) | 577 (13.2%) | 0.1 | 511 (15.4%) | 470 (14.1%) | 0.03 |
| Concomitant | 2901 (20.0%) | 703 (16.1%) | 0.1 | 607 (18.3%) | 586 (17.6%) | 0.02 |
| Histamine H2 antagonists | ||||||
| Previous | 758 (5.2%) | 265 (6.1%) | −0.04 | 200 (6.0%) | 184 (5.5%) | 0.02 |
| Baseline | 1903 (13.1%) | 541 (12.4%) | 0.02 | 450 (13.5%) | 409 (12.3%) | 0.04 |
| Concomitant | 2427 (16.7%) | 706 (16.2%) | 0.01 | 566 (17.0%) | 536 (16.1%) | 0.02 |
| ARBs | ||||||
| Previous | 2138 (14.7%) | 675 (15.5%) | −0.02 | 499 (15.0%) | 500 (15.0%) | 0 |
| Baseline | 1497 (10.3%) | 424 (9.7%) | 0.02 | 355 (10.7%) | 331 (10.0%) | 0.02 |
| Concomitant | 1760 (12.1%) | 489 (11.2%) | 0.03 | 410 (12.3%) | 389 (11.7%) | 0.02 |
| Metformin | ||||||
| Previous | 3285 (22.6%) | 703 (16.1%) | 0.17 | 668 (20.1%) | 604 (18.2%) | 0.05 |
| Baseline | 413 (2.9%) | 84 (1.9%) | 0.06 | 84 (2.5%) | 74 (2.2%) | 0.02 |
| Concomitant | 667 (4.6%) | 155 (3.6%) | 0.05 | 140 (4.2%) | 135 (4.1%) | 0.01 |
| Hydroxychloroquine | ||||||
| Previous | 98 (0.7%) | 40 (0.9%) | −0.03 | 20 (0.6%) | 26 (0.8%) | −0.02 |
| Baseline | 62 (0.4%) | 44 (1.0%) | −0.07 | 14 (0.4%) | 31 (0.9%) | −0.06 |
| Concomitant | 68 (0.5%) | 48 (1.1%) | −0.07 | 14 (0.4%) | 34 (1.0%) | −0.07 |
| Antivirals | ||||||
| Previous | 449 (3.1%) | 148 (3.4%) | −0.02 | 109 (3.3%) | 104 (3.1%) | 0.01 |
| Baseline | 385 (2.7%) | 114 (2.6%) | 0 | 88 (2.7%) | 81 (2.4%) | 0.01 |
| Concomitant | 410 (2.8%) | 118 (2.7%) | 0.01 | 90 (2.7%) | 83 (2.5%) | 0.01 |
| Interleukin-6 inhibitors | ||||||
| Previous | <5 (<0.03) | <5 (<0.1%) | −0.03 | -- | -- | -- |
| Baseline | 486 (3.4%) | 87 (2.0%) | 0.08 | 78 (2.4%) | 73 (2.2%) | 0.01 |
| Concomitant | 874 (6.0%) | 163 (3.7%) | 0.11 | 141 (4.2%) | 141 (4.2%) | 0 |
| Immunosuppressants | ||||||
| Previous | 335 (2.3%) | 180 (4.1%) | −0.10 | 76 (2.3%) | 93 (2.8%) | −0.03 |
| Baseline | 175 (1.2%) | 141 (3.2%) | −0.14 | 50 (1.5%) | 62 (1.9%) | −0.03 |
| Concomitant | 183 (1.3%) | 145 (3.3%) | −0.14 | 52 (1.6%) | 65 (1.9%) | −0.03 |
| Antiparasitic | ||||||
| Previous | <5 (<0.03) | <5 (<0.1%) | 0.02 | -- | -- | -- |
| Baseline | 149 (1.0%) | 20 (0.5%) | 0.07 | 19 (0.6%) | 15 (0.5%) | 0.02 |
| Concomitant | 176 (1.2%) | 22 (0.5%) | 0.08 | 24 (0.7%) | 18 (0.5%) | 0.02 |
| Janus kinase inhibitors | ||||||
| Previous | 29 (0.2%) | 10 (0.2%) | −0.01 | 7 (0.2%) | 10 (0.3%) | −0.02 |
| Baseline | 233 (1.6%) | 29 (0.7%) | 0.09 | 34 (1.0%) | 29 (0.9%) | 0.02 |
| Concomitant | 414 (2.9%) | 59 (1.4%) | 0.1 | 53 (1.6%) | 58 (1.7%) | −0.01 |
| Casirivimab/imdevimab | ||||||
| Previous | <5 (<0.03) | <5 (<0.1%) | 0.01 | -- | -- | -- |
| Baseline | 30 (0.2%) | 24 (0.6%) | −0.06 | 11 (0.3%) | <5 (<0.2%) | 0.05 |
| Concomitant | 11 (0.1%) | 21 (0.5%) | −0.08 | <5 (<0.2%) | <5 (<0.2%) | 0 |
| Bamlanivimab/etesevimab | ||||||
| Baseline | 7 (0.05%) | 14 (0.3%) | −0.06 | <5 (<0.2%) | 5 (0.2%) | −0.03 |
| Concomitant | <5 (<0.03) | 10 (0.2%) | −0.06 | <5 (<0.2%) | <5 (<0.2%) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caffrey, A.R.; Liao, J.X.; Lopes, V.V.; LaPlante, K.L.; Appaneal, H.J. Real-World Safety and Effectiveness of Remdesivir and Corticosteroids in Hospitalized Patients with COVID-19. COVID 2023, 3, 198-217. https://doi.org/10.3390/covid3020015
Caffrey AR, Liao JX, Lopes VV, LaPlante KL, Appaneal HJ. Real-World Safety and Effectiveness of Remdesivir and Corticosteroids in Hospitalized Patients with COVID-19. COVID. 2023; 3(2):198-217. https://doi.org/10.3390/covid3020015
Chicago/Turabian StyleCaffrey, Aisling R., J. Xin Liao, Vrishali V. Lopes, Kerry L. LaPlante, and Haley J. Appaneal. 2023. "Real-World Safety and Effectiveness of Remdesivir and Corticosteroids in Hospitalized Patients with COVID-19" COVID 3, no. 2: 198-217. https://doi.org/10.3390/covid3020015
APA StyleCaffrey, A. R., Liao, J. X., Lopes, V. V., LaPlante, K. L., & Appaneal, H. J. (2023). Real-World Safety and Effectiveness of Remdesivir and Corticosteroids in Hospitalized Patients with COVID-19. COVID, 3(2), 198-217. https://doi.org/10.3390/covid3020015