
Cardiac Arrhythmias in Pediatric Age: Are They Triggered by SARS-CoV-2 Infection?

 , ,
, ,  and
and
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Case Presentation
2.1. Case 1
2.2. Case 2
3. Discussion
4. Conclusions
5. Learning Objectives
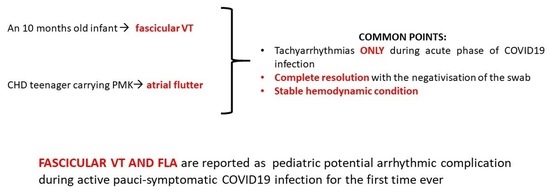
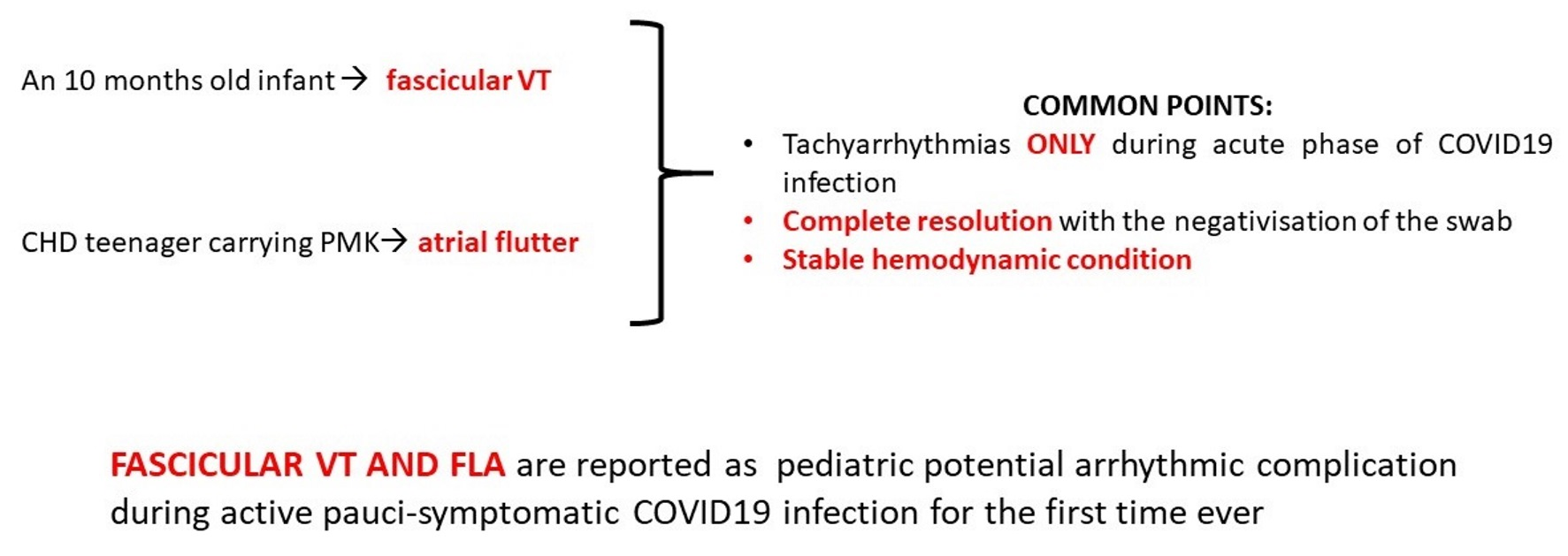
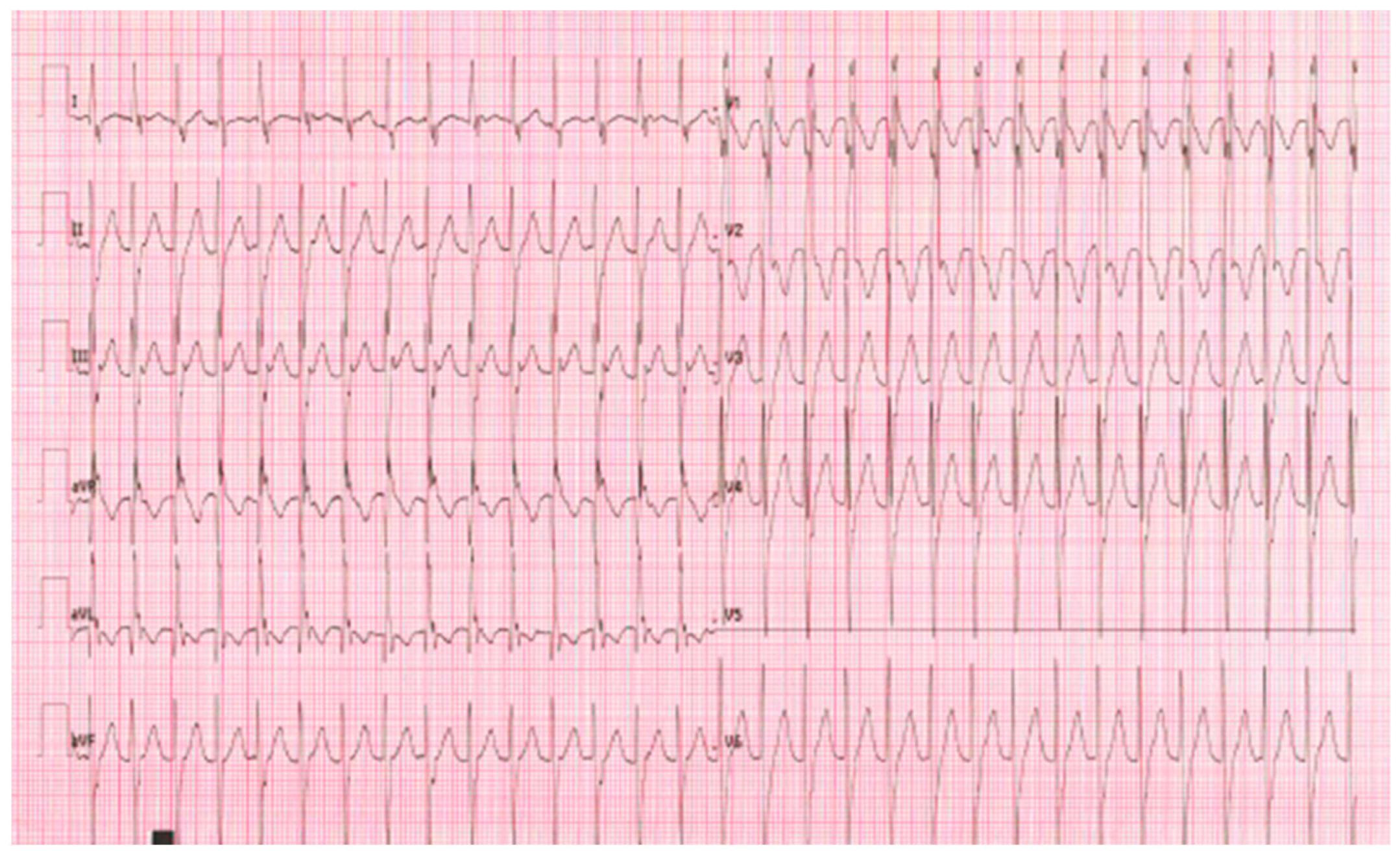
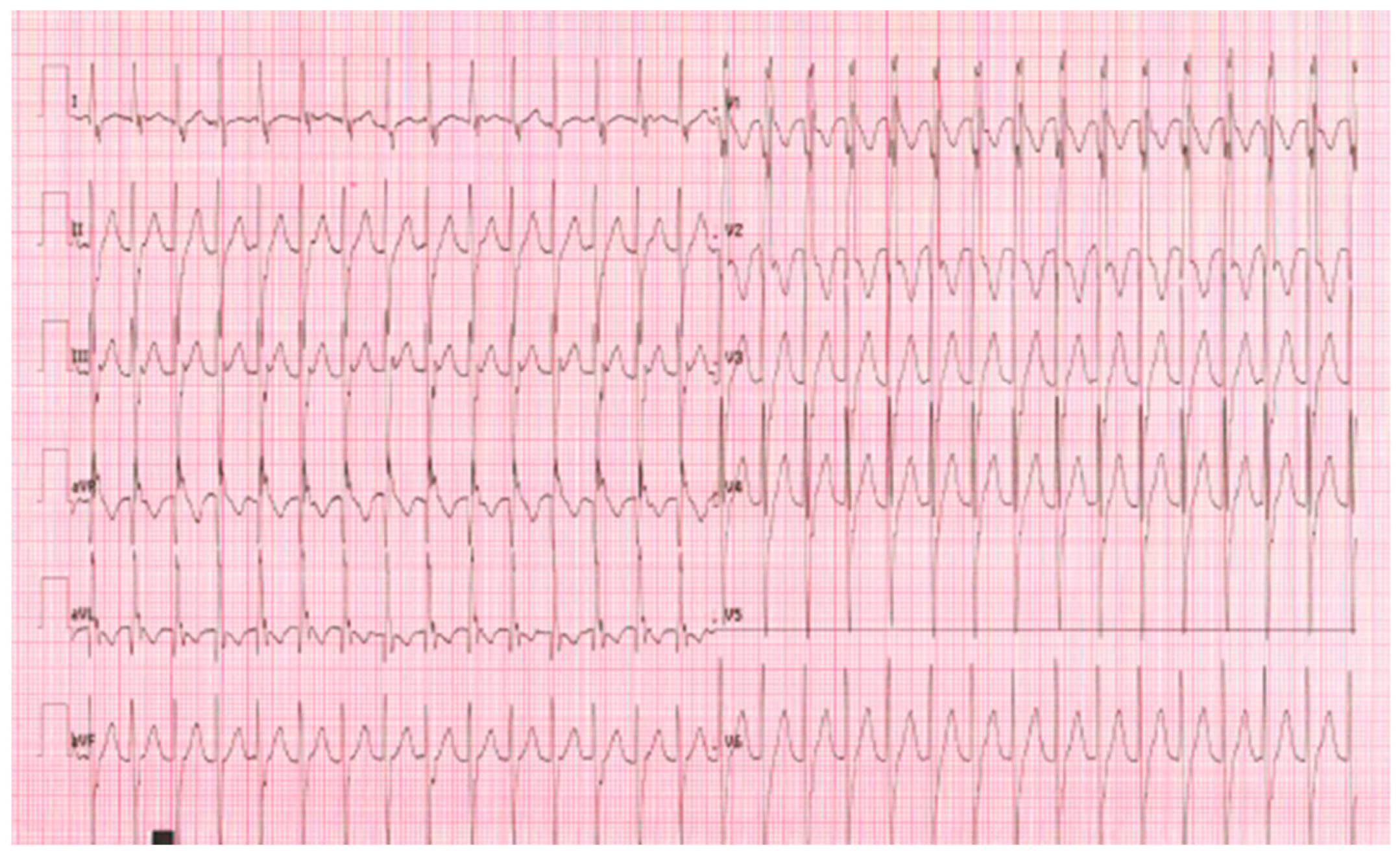
5.1. Case 1: An Infant with Posterior Left Fascicular Tachycardia
- To define the etiology of the fascicular tachycardia
- To understand the role of COVID-19 as a trigger factor of the ventricular tachycardia
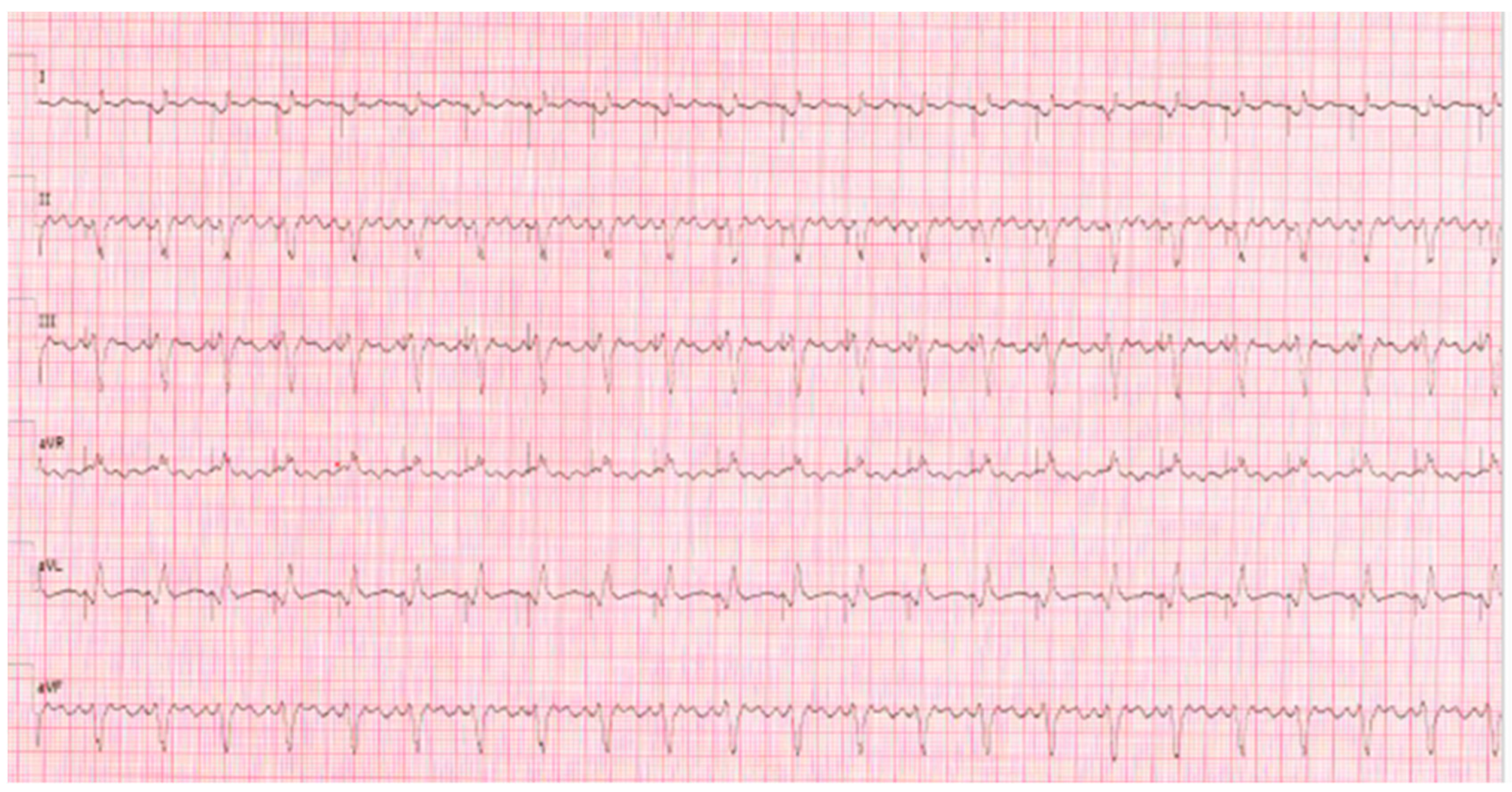
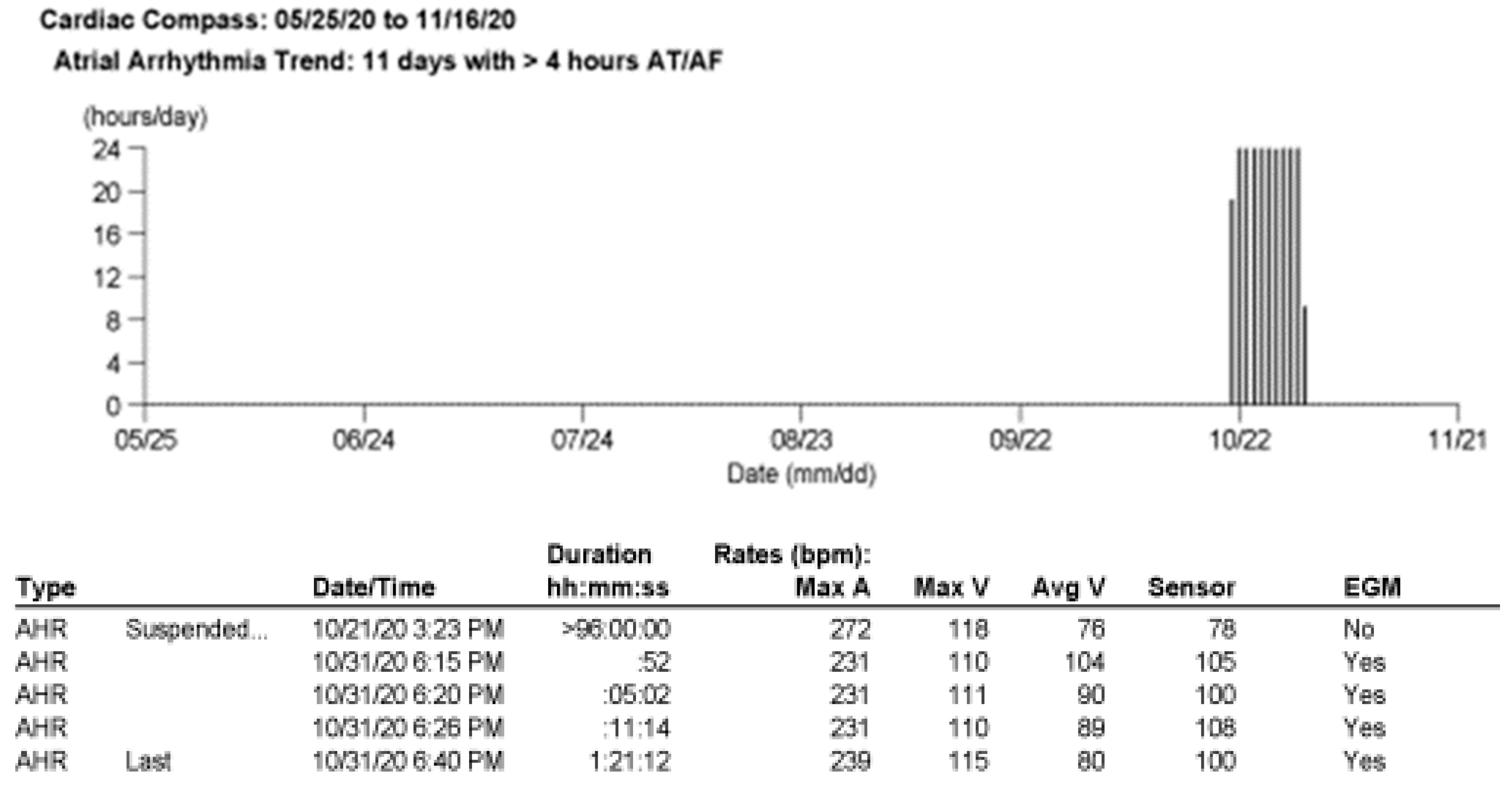
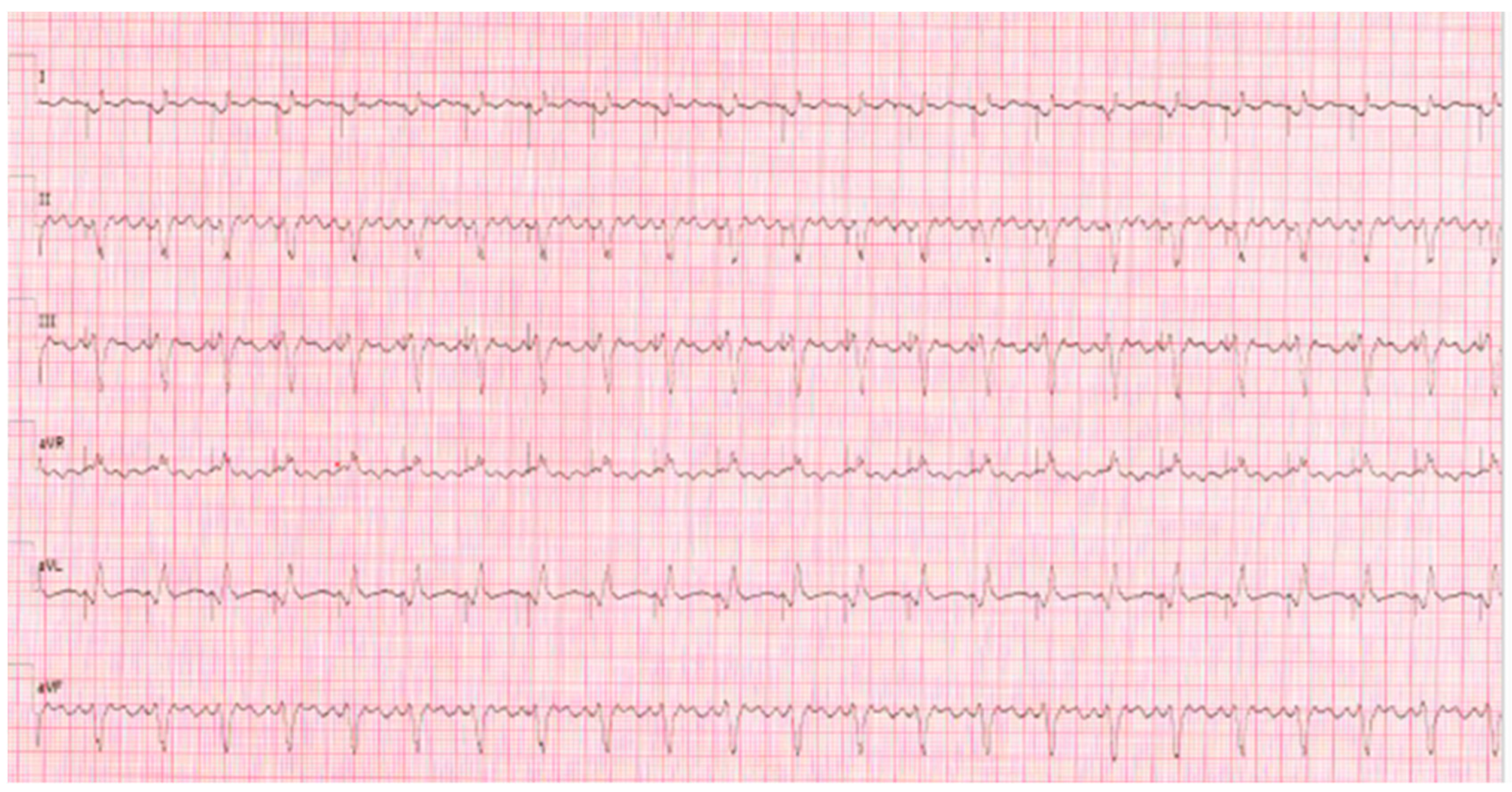
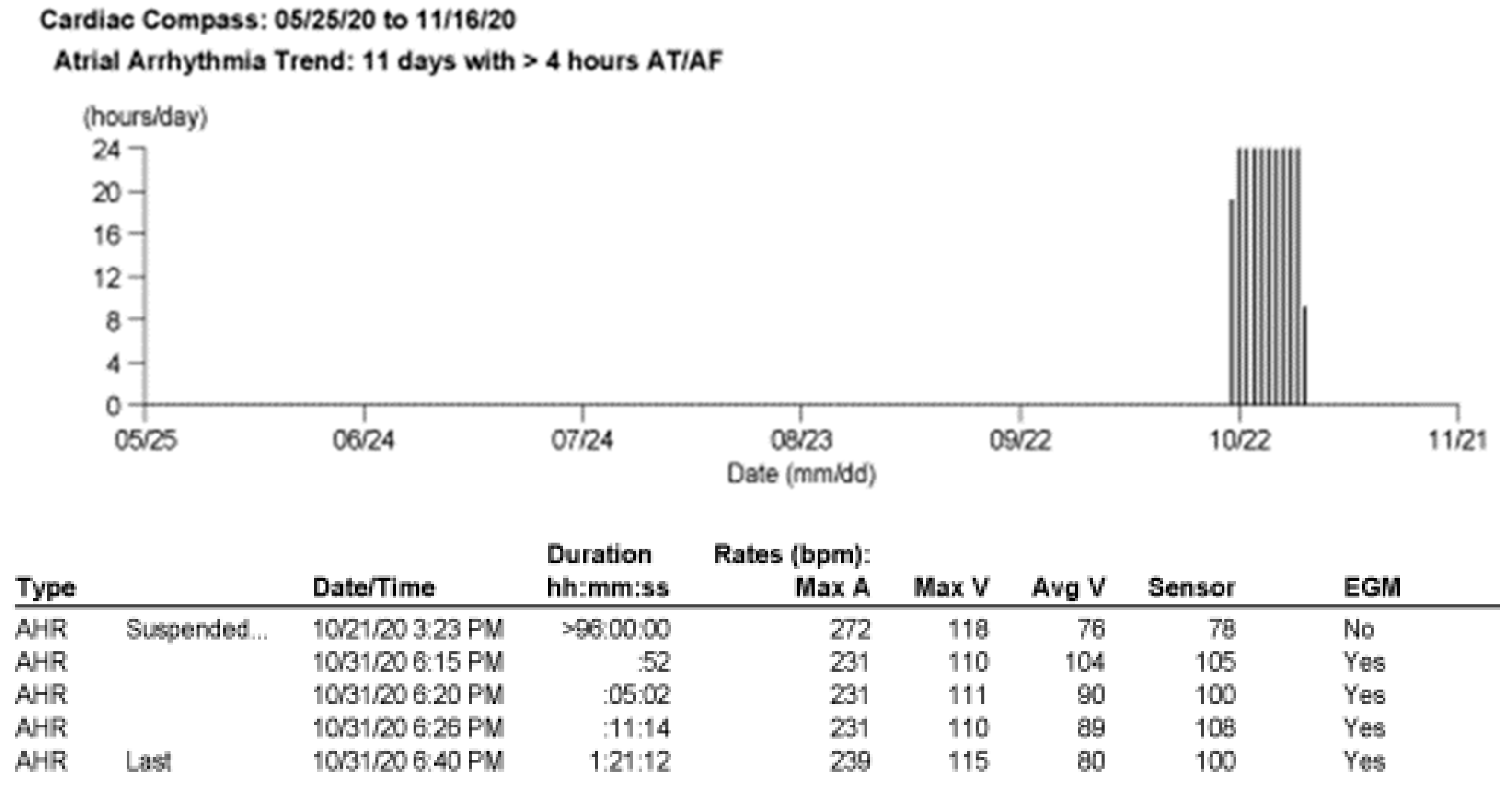
5.2. Case 2: A CHD Patient with PMK and Atrial Flutter
- To define the trigger mechanism of the supraventricular tachycardia
- To understand the time correlation between the arrhythmias and COVID-19 infection
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dherange, P.; Lang, J.; Qian, P.; Oberfeld, B.; Sauer, W.H.; Koplan, B.; Tedrow, U. Arrhythmias and COVID-19: A Review. JACC Clin. Electrophysiol. 2020, 6, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, A.; Mayer, M.M.; Adusumalli, S.; Hyman, M.C.; Oh, E.; Tierney, A.; Moss, J.; Chahal, A.A.; Anesi, G.; Denduluri, S.; et al. COVID-19 and cardiac arrhythmias. Heart Rhythm 2020, 17, 1439–1444. [Google Scholar] [CrossRef] [PubMed]
- Manolis, A.S.; Manolis, A.A.; Manolis, T.A.; Apostolopoulos, E.J.; Papatheou, D.; Melita, H. COVID-19 infection and cardiac arrhythmias. Trends Cardiovasc. Med. 2020, 30, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Sperotto, F.; Friedman, K.G.; Son, M.B.F.; VanderPluym, C.J.; Newburger, J.W.; Dionne, A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: A comprehensive review and proposed clinical approach. Eur. J. Pediatr. 2021, 180, 307–322. [Google Scholar] [CrossRef] [PubMed]
- de Souza, T.H.; Nadal, J.A.; Nogueira, R.J.N.; Pereira, R.M.; Brandão, M.B. Clinical Manifestations of Children with COVID-19: A Systematic Review. Pediatr. Pulmonol. 2020, 55, 1892–1899. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Shao, J.; Guo, Y.; Peng, X.; Li, Z.; Hu, D. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr. Pulmonol. 2020, 55, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Heching, H.J.; Goyal, A.; Harvey, B.; Malloy-Walton, L.; Follansbee, C.; Mcintosh, A.; Forsha, D. Electrocardiographic changes in non-hospitalised children with COVID-19. Cardiol. Young 2022, 32, 1910–1916. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, F.T.; Gutiérrez-Sacristán, A.; Keller, M.S.; Liu, M.; Hong, C.; Bonzel, C.L.; Tan, A.L.M.; Aronow, B.J.; Boeker, M.; Booth, J.; et al. International Analysis of Electronic Health Records of Children and Youth Hospitalized with COVID-19 Infection in 6 Countries. JAMA Netw. Open 2021, 4, e2112596. [Google Scholar] [CrossRef] [PubMed]
- Sanna, G.; Serrau, G.; Bassareo, P.P.; Neroni, P.; Fanos, V.; Marcialis, M.A. Children’s heart and COVID-19: Up-to-date evidence in the form of a systematic review. Eur. J. Pediatr. 2020, 179, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.; Friedman, R.A.; Sharma, C.; Ganigara, M.; Mitchell, E.; Schleien, C.; Blaufox, A.D. Incidence of arrhythmias and electrocardiographic abnormalities in symptomatic pediatric patients with PCR-positive SARS-CoV-2 infection, including drug-induced changes in the corrected QT interval. Heart Rhythm 2020, 17, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, K.A.; Webster, G. Aberrated supraventricular tachycardia associated with neonatal fever and COVID-19 infection. BMJ Case Rep. 2021, 14, e241846. [Google Scholar] [CrossRef] [PubMed]
- Bertini, M.; Vitali, F.; Malagù, M.; Rapezzi, C. Atrial Flutter in Patient with Critical COVID-19: Beneficial Effects of Rhythm Control on Respiratory Distress. JACC Case Rep. 2021, 3, 162–164. [Google Scholar] [CrossRef]
- Castiello, T.; Georgiopoulos, G.; Finocchiaro, G.; Claudia, M.; Gianatti, A.; Delialis, D.; Aimo, A.; Prasad, S. COVID-19 and myocarditis: A systematic review and overview of current challenges. Heart Fail. Rev. 2022, 27, 251–261. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fumanelli, J.; Sabatino, J.; Biffanti, R.; Reffo, E.; Di Salvo, G.; Leoni, L. Cardiac Arrhythmias in Pediatric Age: Are They Triggered by SARS-CoV-2 Infection? COVID 2023, 3, 192-197. https://doi.org/10.3390/covid3020014
Fumanelli J, Sabatino J, Biffanti R, Reffo E, Di Salvo G, Leoni L. Cardiac Arrhythmias in Pediatric Age: Are They Triggered by SARS-CoV-2 Infection? COVID. 2023; 3(2):192-197. https://doi.org/10.3390/covid3020014
Chicago/Turabian StyleFumanelli, Jennifer, Jolanda Sabatino, Roberta Biffanti, Elena Reffo, Giovanni Di Salvo, and Loira Leoni. 2023. "Cardiac Arrhythmias in Pediatric Age: Are They Triggered by SARS-CoV-2 Infection?" COVID 3, no. 2: 192-197. https://doi.org/10.3390/covid3020014
APA StyleFumanelli, J., Sabatino, J., Biffanti, R., Reffo, E., Di Salvo, G., & Leoni, L. (2023). Cardiac Arrhythmias in Pediatric Age: Are They Triggered by SARS-CoV-2 Infection? COVID, 3(2), 192-197. https://doi.org/10.3390/covid3020014