




Neuropsychological Outcomes of COVID-19: A Multicenter, Cross-Cultural Study of Patients Referred for Outpatient Assessment
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sampling
2.2. Ethical Considerations
2.3. Outcome Variables and Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid-mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef] [PubMed]
- Ermis, U.; Rust, M.I.; Bungenberg, J.; Costa, A.; Dreher, M.; Balfanz, P.; Marx, G.; Wiesmann, M.; Reetz, K.; Tauber, S.C.; et al. Neurological symptoms in COVID-19: A cross-sectional monocentric study of hospitalized patients. Neurol. Res. Pract. 2021, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Watson, C.J.; Badenoch, J.; Cross, B.; Butler, M.; Song, J.; Hafeez, D.; Morrin, H.; Rengasamy, E.R.; Thomas, L.; et al. Neurology and neuropsychiatry of COVID-19: A systematic review and meta-analysis of the early literature reveals frequent CNS manifestations and key emerging narratives. J. Neurol. Neurosurg. Psychiatry 2021, 92, 932–941. [Google Scholar] [CrossRef]
- Clift, A.K.; Ranger, T.A.; Patone, M.; Coupland, C.A.C.; Hatch, R.; Thomas, K.; Hippisley-Cox, J.; Watkinson, P. Neuropsychiatric Ramifications of Severe COVID-19 and Other Severe Acute Respiratory Infections. JAMA Psychiatry 2022, 79, 690–698. [Google Scholar] [CrossRef]
- Crivelli, L.; Palmer, K.; Calandri, I.; Guekht, A.; Beghi, E.; Carroll, W.; Frontera, J.; Garcia-Azorin, D.; Westenberg, E.; Winkler, A.S.; et al. Changes in cognitive functioning after COVID-19: A systematic review and meta-analysis. Alzheimers Dement. 2022, 18, 1047–1066. [Google Scholar] [CrossRef]
- Garcia-Sanchez, C.; Calabria, M.; Grunden, N.; Pons, C.; Arroyo, J.A.; Gomez-Anson, B.; Lleo, A.; Alcolea, D.; Belvis, R.; Morollon, N.; et al. Neuropsychological deficits in patients with cognitive complaints after COVID-19. Brain Behav. 2022, 12, e2508. [Google Scholar] [CrossRef]
- Bungenberg, J.; Humkamp, K.; Hohenfeld, C.; Rust, M.I.; Ermis, U.; Dreher, M.; Hartmann, N.K.; Marx, G.; Binkofski, F.; Finke, C.; et al. Long COVID-19: Objectifying most self-reported neurological symptoms. Ann. Clin. Transl. Neurol. 2022, 9, 141–154. [Google Scholar] [CrossRef]
- Becker, J.H.; Lin, J.J.; Doernberg, M.; Stone, K.; Navis, A.; Festa, J.R.; Wisnivesky, J.P. Assessment of Cognitive Function in Patients After COVID-19 Infection. JAMA Netw. Open 2021, 4, e2130645. [Google Scholar] [CrossRef]
- Zhou, H.; Lu, S.; Chen, J.; Wei, N.; Wang, D.; Lyu, H.; Shi, C.; Hu, S. The landscape of cognitive function in recovered COVID-19 patients. J. Psychiatr. Res. 2020, 129, 98–102. [Google Scholar] [CrossRef]
- Vannorsdall, T.D.; Brigham, E.; Fawzy, A.; Raju, S.; Gorgone, A.; Pletnikova, A.; Lyketsos, C.G.; Parker, A.M.; Oh, E.S. Rates of Cognitive Dysfunction, Psychiatric Distress, and Functional Decline After COVID-19. J. Acad. Consult.-Liaison Psychiatry 2021, 63, 133–143. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Jaywant, A.; Vanderlind, W.M.; Alexopoulos, G.S.; Fridman, C.B.; Perlis, R.H.; Gunning, F.M. Frequency and profile of objective cognitive deficits in hospitalized patients recovering from COVID-19. Neuropsychopharmacology 2021, 46, 2235–2240. [Google Scholar] [CrossRef]
- Negrini, F.; Ferrario, I.; Mazziotti, D.; Berchicci, M.; Bonazzi, M.; de Sire, A.; Negrini, S.; Zapparoli, L. Neuropsychological Features of Severe Hospitalized Coronavirus Disease 2019 Patients at Clinical Stability and Clues for Postacute Rehabilitation. Arch. Phys. Med. Rehabil. 2021, 102, 155–158. [Google Scholar] [CrossRef]
- Batty, G.D.; Deary, I.J.; Gale, C.R. Pre-pandemic cognitive function and COVID-19 mortality: Prospective cohort study. Eur. J. Epidemiol. 2021, 36, 559–564. [Google Scholar] [CrossRef]
- Webb Hooper, M.; Napoles, A.M.; Perez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef]
- Ladds, E.; Rushforth, A.; Wieringa, S.; Taylor, S.; Rayner, C.; Husain, L.; Greenhalgh, T. Persistent symptoms after Covid-19: Qualitative study of 114 “long Covid” patients and draft quality principles for services. BMC Health Serv. Res. 2020, 20, 1144. [Google Scholar] [CrossRef]
- Lancet, T. Facing up to long COVID. Lancet 2020, 396, 1861. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, jiac136. [Google Scholar] [CrossRef]
- Goertz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542-2020. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef] [PubMed]
- Munro Cullum, C.; Hynan, L.S.; Grosch, M.; Parikh, M.; Weiner, M.F. Teleneuropsychology: Evidence for video teleconference-based neuropsychological assessment. J. Int. Neuropsychol. Soc. 2014, 20, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Darley, D.R.; Dore, G.J.; Cysique, L.; Wilhelm, K.A.; Andresen, D.; Tonga, K.; Stone, E.; Byrne, A.; Plit, M.; Masters, J.; et al. Persistent symptoms up to four months after community and hospital-managed SARS-CoV-2 infection. Med. J. Aust. 2021, 214, 279–280. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, D.M.; Basso, M.R.; Naini, S.M.; Porter, J.; Holker, E.; Waldron, E.J.; Melnik, T.E.; Niskanen, N.; Taylor, S.E. Outcomes in post-acute sequelae of COVID-19 (PASC) at 6 months post-infection Part 1: Cognitive functioning. Clin. Neuropsychol. 2022, 36, 806–828. [Google Scholar] [CrossRef]
- Vanderlind, W.M.; Rabinovitz, B.B.; Miao, I.Y.; Oberlin, L.E.; Bueno-Castellano, C.; Fridman, C.; Jaywant, A.; Kanellopoulos, D. A systematic review of neuropsychological and psychiatric sequalae of COVID-19: Implications for treatment. Curr. Opin. Psychiatry 2021, 34, 420–433. [Google Scholar] [CrossRef]
- Hellmuth, J.; Barnett, T.A.; Asken, B.M.; Kelly, J.D.; Torres, L.; Stephens, M.L.; Greenhouse, B.; Martin, J.N.; Chow, F.C.; Deeks, S.G.; et al. Persistent COVID-19-associated neurocognitive symptoms in non-hospitalized patients. J. Neurovirol. 2021, 27, 191–195. [Google Scholar] [CrossRef]
- Boesl, F.; Audebert, H.; Endres, M.; Pruss, H.; Franke, C. A Neurological Outpatient Clinic for Patients With Post-COVID-19 Syndrome - A Report on the Clinical Presentations of the First 100 Patients. Front. Neurol. 2021, 12, 738405. [Google Scholar] [CrossRef]
- Heesakkers, H.; van der Hoeven, J.G.; Corsten, S.; Janssen, I.; Ewalds, E.; Simons, K.S.; Westerhof, B.; Rettig, T.C.D.; Jacobs, C.; van Santen, S.; et al. Clinical Outcomes Among Patients With 1-Year Survival Following Intensive Care Unit Treatment for COVID-19. JAMA 2022, 327, 559–565. [Google Scholar] [CrossRef]
- Almeria, M.; Cejudo, J.C.; Sotoca, J.; Deus, J.; Krupinski, J. Cognitive profile following COVID-19 infection: Clinical predictors leading to neuropsychological impairment. Brain Behav. Immun. Health 2020, 9, 100163. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Martin-Guerrero, J.D.; Cancela-Cilleruelo, I.; Rodriguez-Jimenez, J.; Moro-Lopez-Menchero, P.; Pellicer-Valero, O.J. Exploring trajectory recovery curves of post-COVID cognitive symptoms in previously hospitalized COVID-19 survivors: The LONG-COVID-EXP-CM multicenter study. J. Neurol. 2022, 269, 4613–4617. [Google Scholar] [CrossRef]
- Ferrucci, R.; Dini, M.; Rosci, C.; Capozza, A.; Groppo, E.; Reitano, M.R.; Allocco, E.; Poletti, B.; Brugnera, A.; Bai, F.; et al. One-year cognitive follow-up of COVID-19 hospitalized patients. Eur. J. Neurol. 2022, 29, 2006–2014. [Google Scholar] [CrossRef]
- Serrano-Castro, P.J.; Garzon-Maldonado, F.J.; Casado-Naranjo, I.; Ollero-Ortiz, A.; Minguez-Castellanos, A.; Iglesias-Espinosa, M.; Baena-Palomino, P.; Sanchez-Sanchez, V.; Sanchez-Perez, R.M.; Rubi-Callejon, J.; et al. The cognitive and psychiatric subacute impairment in severe Covid-19. Sci. Rep. 2022, 12, 3563. [Google Scholar] [CrossRef]
- Miskowiak, K.W.; Johnsen, S.; Sattler, S.M.; Nielsen, S.; Kunalan, K.; Rungby, J.; Lapperre, T.; Porsberg, C.M. Cognitive impairments four months after COVID-19 hospital discharge: Pattern, severity and association with illness variables. Eur. Neuropsychopharmacol. 2021, 46, 39–48. [Google Scholar] [CrossRef]
- Honarmand, K.; Lalli, R.S.; Priestap, F.; Chen, J.L.; McIntyre, C.W.; Owen, A.M.; Slessarev, M. Natural History of Cognitive Impairment in Critical Illness Survivors. A Systematic Review. Am. J. Respir. Crit. Care Med. 2020, 202, 193–201. [Google Scholar] [CrossRef]
- Pandharipande, P.P.; Girard, T.D.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Pun, B.T.; Brummel, N.E.; Hughes, C.G.; Vasilevskis, E.E.; Shintani, A.K.; et al. Long-term cognitive impairment after critical illness. N. Engl. J. Med. 2013, 369, 1306–1316. [Google Scholar] [CrossRef]
- Hewitt, K.C.; Marra, D.E.; Block, C.; Cysique, L.A.; Drane, D.L.; Haddad, M.M.; Lojek, E.; McDonald, C.R.; Reyes, A.; Eversole, K.; et al. Central Nervous System Manifestations of COVID-19: A Critical Review and Proposed Research Agenda. J. Int. Neuropsychol. Soc. 2021, 28, 311–325. [Google Scholar] [CrossRef]
- Riordan, P.; Stika, M.; Goldberg, J.; Drzewiecki, M. COVID-19 and clinical neuropsychology: A review of neuropsychological literature on acute and chronic pulmonary disease. Clin. Neuropsychol. 2020, 34, 1480–1497. [Google Scholar] [CrossRef]
- Raj, S.R.; Arnold, A.C.; Barboi, A.; Claydon, V.E.; Limberg, J.K.; Lucci, V.M.; Numan, M.; Peltier, A.; Snapper, H.; Vernino, S.; et al. Long-COVID postural tachycardia syndrome: An American Autonomic Society statement. Clin. Auton. Res. 2021, 31, 365–368. [Google Scholar] [CrossRef]

{kind=link}
| Site | ||||
|---|---|---|---|---|
| UKA a (N = 42) | MGH PAC b (N = 27) | JH DMP c (N = 8) | MGH MARC d (N = 7) | |
| Variable | ||||
| Sex (F/M) | 24/18 | 19/8 | 3/5 | 3/4 |
| Race/Ethnicity (% White or European) | 97.6% | 88.9% | 37.5% | 0% |
| Age (years) | 48.39 | 51.93 | 64.3 | 63.57 |
| Range | 22–65 | 25–84 | 44–85 | 51–79 |
| Education (years) | 15 | 16 | 13 | 9 |
| Range | 9–20 | 12–20 | 6–16 | 5–13 |
| Time from COVID Diagnosis to NP Evaluation (months) | 6.58 | 7.55 | 4.30 | 10.57 |
| Range | 1–12 | 2–10 | 2–7 | 9–13 |
| Date of COVID Diagnosis | February 2020–January 2021 | March 2020–January 2021 | April 2020–November 2020 | March–April 2020 |
| Conducted Remotely | 0% | 93% | 63% | 0% |
| Date of NP Evaluation | August 2020–April 2021 | July 2020–May 2021 | July 2020–February 2021 | October 2020–April 2021 |
| Language of Test Administration | German | English | English | Spanish |
| % Yes | ||||
| Comorbidities Prior to COVID | ||||
| Medical | 62% | 96% | 88% | 100% |
| Psychiatric | 14% | 56% | 38% | 43% |
| Neurologic | 36% | 44% | 75% | 0% |
| Primary Referral due to COVID | 99% | 93% | 100% | 100% |
| Self-Reported Post-COVID Symptoms | ||||
| Brain Fog/Cognitive Changes | 71% | 100% | 100% | 100% |
| Fatigue | 55% | 81% | 50% | 71% |
| Mood Disturbance | 19% | 67% | 63% | 100% |
| Sleep Difficulties | 48% | 44% | 50% | 100% |
| Dysautonomia | 24% | 15% | 0% | 43% |
| Psychosocial Distress | - | 26% | 38% | 100% |
| New Pain | 10% | 37% | 63% | 43% |
| Hospitalized | 38% | 30% | 100% | 71% |
| Days Hospitalized (mean) | 26.93 | 24.50 | 24.80 | 14.00 |
| Received Inpatient Treatment | 40% | 30% | 75% | 71% |
| On Ventilator | 46% | 15% | 40% | 71% |
| Delirium | 2% | 11% | 38% | 29% |
| Loss of Employment | 0% | 4% | 67% | 71% |
| Unable to Return to Work at Baseline Capacity | 48% | 85% | 50% | 71% |
| Financial/Housing Strain | - | 18% | 25% | 57% |
| Grief/Health Impact on Family Members | 2% | 4% | 0% | 57% |
| Post-COVID Treatment | ||||
| Physical Rehabilitation | 36% | 26% | 50% | 29% |
| Cognitive Intervention | 14% | 4% | 0% | 29% |
| UKA a (N = 42) | MGH PAC b (N = 27) | JH DMP c (N = 8) | MGH MARC d (N = 7) | UKA a (N = 42) | MGH PAC b (N = 27) | JH DMP c (N = 8) | MGH MARC d (N = 7) | |
|---|---|---|---|---|---|---|---|---|
| Cognitive Domain | Z-Score: M (SD) | Patients with Z-Score ≤ −1.0/≤ −1.5 | ||||||
| Language/Semantic Access | −0.27 (0.66) | −0.28 (0.98) | −0.33 (0.81) | −0.81 (0.65) | 12%/4% | 18%/11% | 0%/0% | 43%/29% |
| Processing Speed | −0.42 (0.67) | −0.98 (1.09) | −1.08 (0.71) | −1.45 (0.89) | 14%/9% | 37%/26% | 63%/38% | 86%/57% |
| Executive Functioning | −0.12 (0.76) | −0.25 (1.02) | −1.15 (0.96) | −1.29 (0.86) | 12%/4% | 18%/15% | 63%/38% | 57%/43% |
| Attention/Working Memory | −0.09 (0.76) | −0.37 (0.90) | −1.08 (0.88) | −0.58 (0.74) | 12%/0% | 29%/7% | 50%/38% | 29%/43% |
| Encoding | −0.24 (0.63) | −0.13 (1.10) | −0.86 (0.76) | −1.14 (0.98) | 15%/0% | 22%/7% | 38%/13% | 57%/14% |
| Delayed Memory | −0.27 (0.66) | 0.00 (1.01) | −0.74 (0.80) | −1.37 (0.95) | 9%/2% | 11%/11% | 38%/13% | 71%/43% |
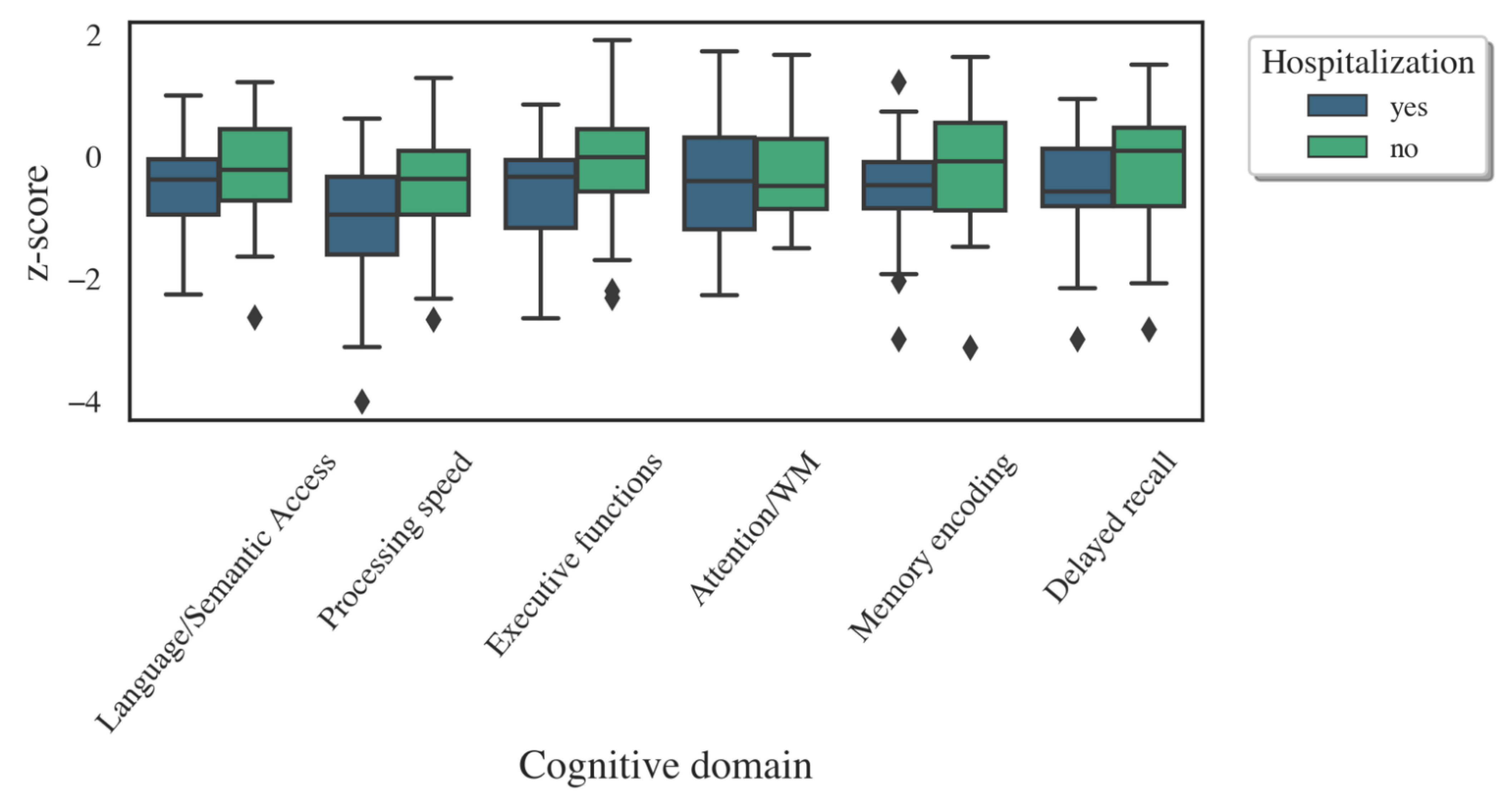
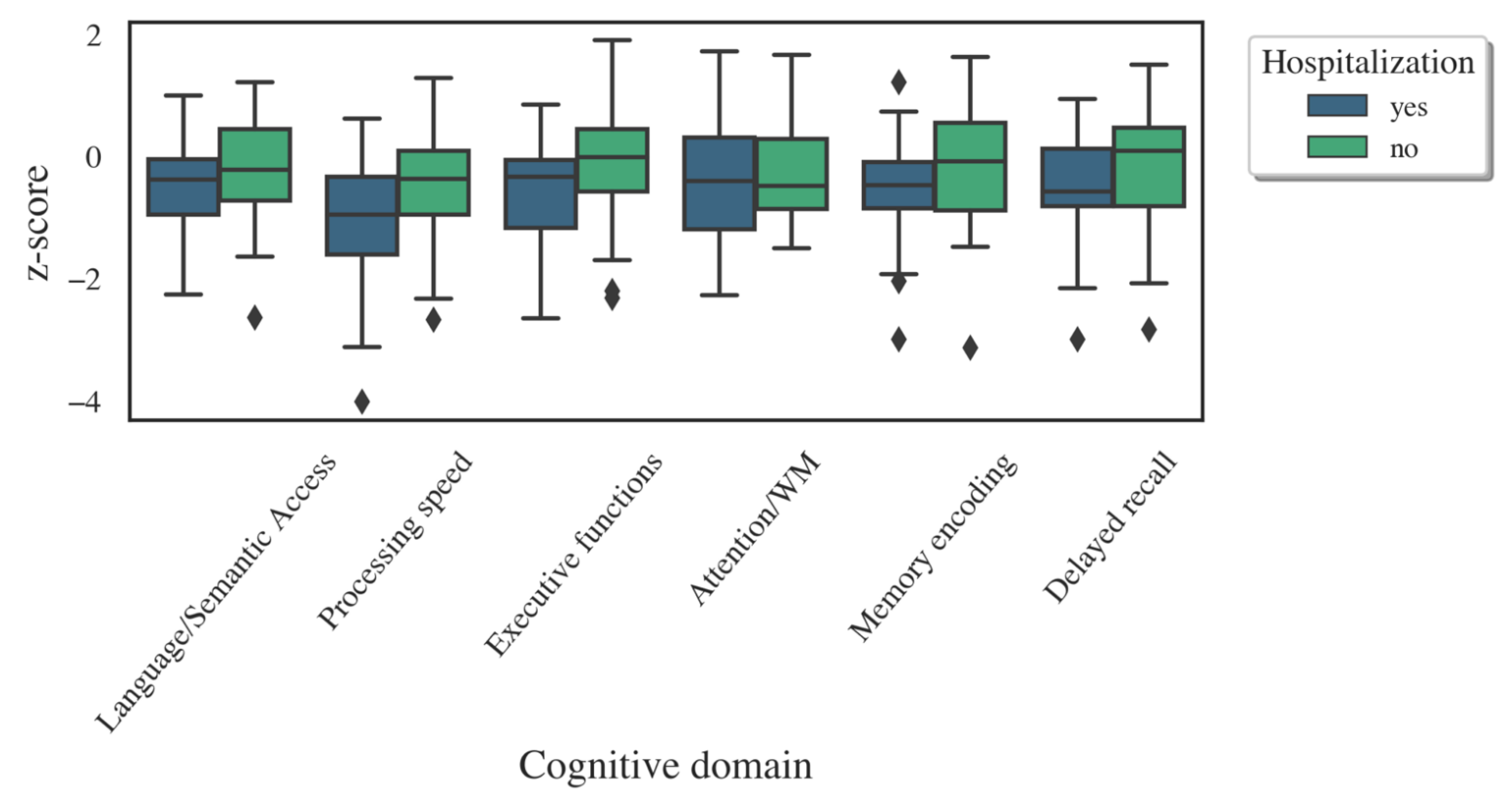
| Hospitalized | Non-Hospitalized | ||||||
|---|---|---|---|---|---|---|---|
| n | M (SD) | n | M (SD) | t (df) | p | Cohen’s d | |
| Language/Semantic Access | 33 | −0.48 (0.76) | 48 | −0.21 (0.79) | 1.53 (79) | 0.130 | 0.35 |
| Processing Speed | 36 | −1.01 (0.97) | 48 | −0.55 (0.80) | 2.35 (82) | 0.021 * | 0.51 |
| Executive Functioning | 36 | −0.64 (0.95) | 48 | −0.15 (0.91) | 2.43 (82) | 0.017 * | 0.53 |
| Attention/Working Memory | 33 | −0.44 (0.98) | 42 | −0.27 (0.77) | 0.83 (73) | 0.408 | 0.19 |
| Memory Encoding | 36 | −0.53 (0.86) | 47 | −0.19 (0.90) | 1.76 (81) | 0.082 | 0.39 |
| Delayed Memory | 36 | −0.49 (0.83) | 47 | −0.18 (0.93) | 1.59 (81) | 0.117 | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kay, C.D.; Costa, A.S.; Vannorsdall, T.D.; Aduen, P.; Vila-Castelar, C.; Burstein, S.M.; Pollak, L.; Leibel, D.K.; Sherman, J.C.; Bungenberg, J.; et al. Neuropsychological Outcomes of COVID-19: A Multicenter, Cross-Cultural Study of Patients Referred for Outpatient Assessment. COVID 2022, 2, 1253-1264. https://doi.org/10.3390/covid2090092
Kay CD, Costa AS, Vannorsdall TD, Aduen P, Vila-Castelar C, Burstein SM, Pollak L, Leibel DK, Sherman JC, Bungenberg J, et al. Neuropsychological Outcomes of COVID-19: A Multicenter, Cross-Cultural Study of Patients Referred for Outpatient Assessment. COVID. 2022; 2(9):1253-1264. https://doi.org/10.3390/covid2090092
Chicago/Turabian StyleKay, Christina D., Ana Sofia Costa, Tracy D. Vannorsdall, Paula Aduen, Clara Vila-Castelar, Sarah M. Burstein, Lauren Pollak, Daniel K. Leibel, Janet C. Sherman, Julia Bungenberg, and et al. 2022. "Neuropsychological Outcomes of COVID-19: A Multicenter, Cross-Cultural Study of Patients Referred for Outpatient Assessment" COVID 2, no. 9: 1253-1264. https://doi.org/10.3390/covid2090092
APA StyleKay, C. D., Costa, A. S., Vannorsdall, T. D., Aduen, P., Vila-Castelar, C., Burstein, S. M., Pollak, L., Leibel, D. K., Sherman, J. C., Bungenberg, J., Reetz, K., & Quiroz, Y. T. (2022). Neuropsychological Outcomes of COVID-19: A Multicenter, Cross-Cultural Study of Patients Referred for Outpatient Assessment. COVID, 2(9), 1253-1264. https://doi.org/10.3390/covid2090092