
Gambling and Gaming in the United Kingdom during the COVID-19 Lockdown

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Survey Tools
2.3. Statistical Analysis
2.3.1. Changes to Gaming and Gambling Activities
2.3.2. Changes to Wellbeing
2.3.3. Path Analysis of Problem Gaming, Problem Gaming and Wellbeing over Time
3. Results
3.1. Demographics and Participation Rates
3.2. Gaming and Problem Gaming during the COVID-19 Lockdown
3.3. Gambling and Problem Gambling during the COVID-19 Lockdown
3.4. Wellbeing during the COVID-19 Lockdown—Interactions with Demographics, Gaming and Gambling
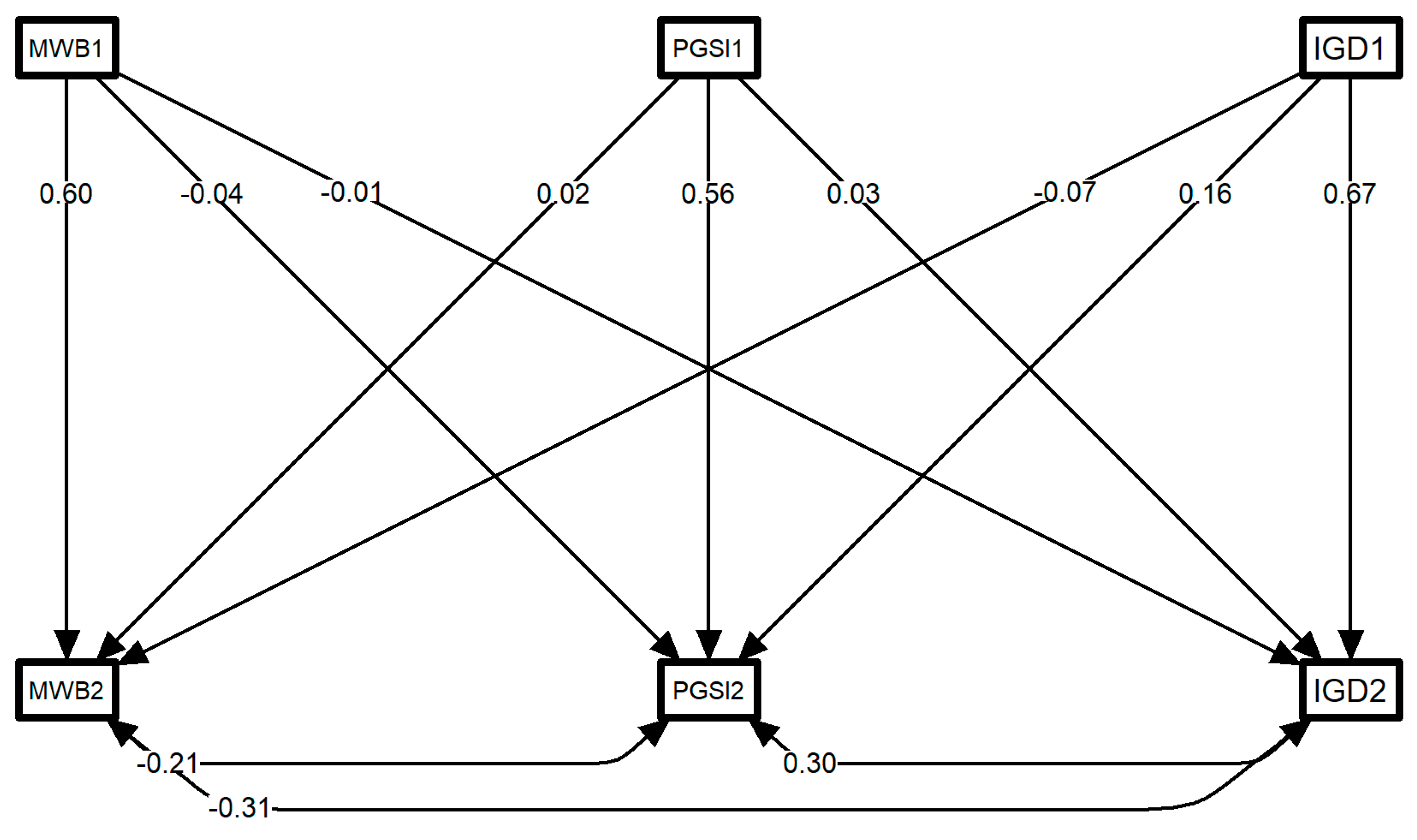
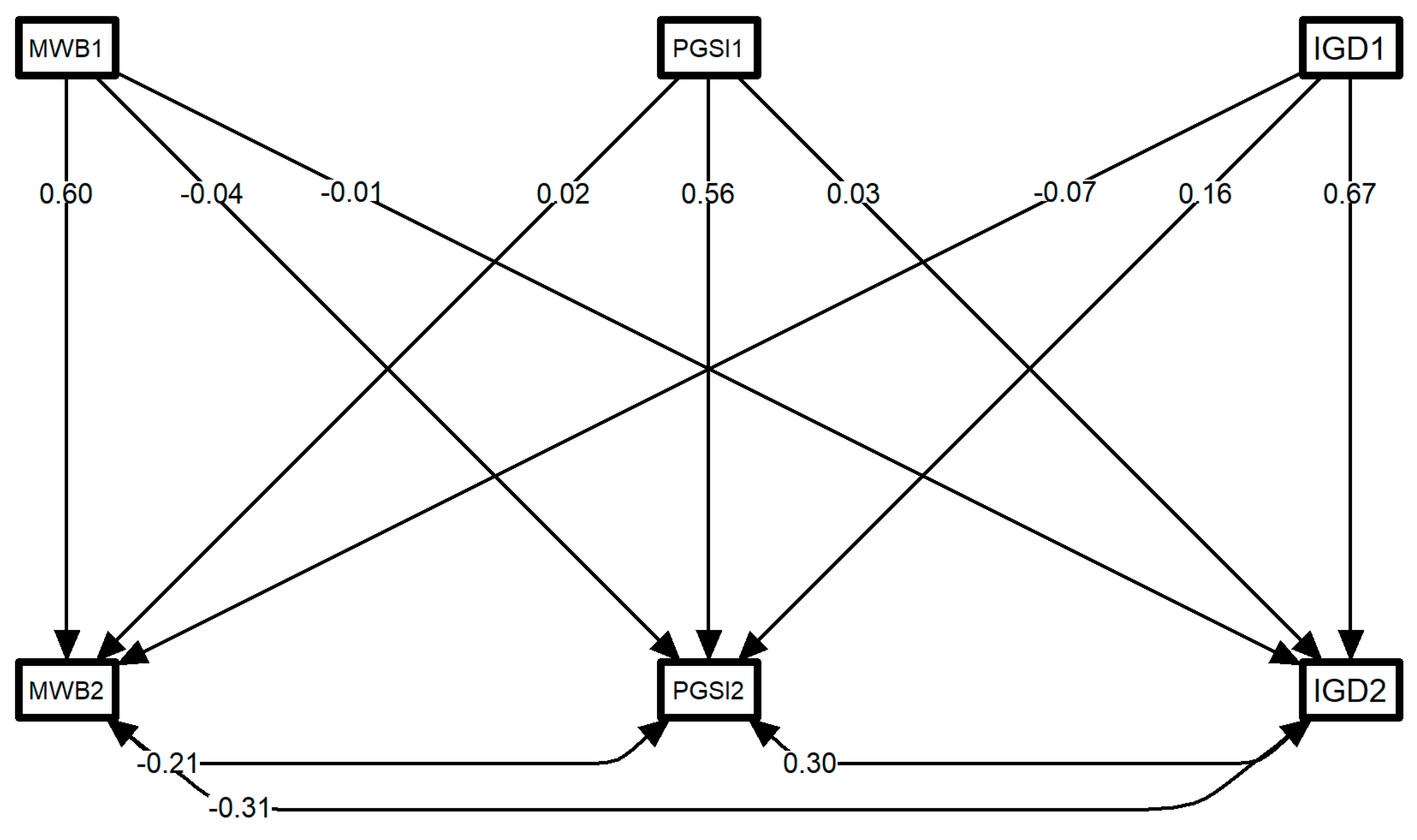
3.5. Path Analysis—Interactions between Gaming, Gambling and Wellbeing over Time
4. Discussion
4.1. Video Gaming during Lockdown
4.2. Gambling during Lockdown
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, S.P. Chancellor Sunak Warns of “Tough Times” for UK Economy. Available online: https://www.bbc.co.uk/news/business-52279871 (accessed on 14 December 2021).
- Duncan, C. Coronavirus: More than 6.5 Million Jobs to Be Lost in UK Lockdown, Study Predicts. The Independent. 2020. Available online: https://www.independent.co.uk/news/uk/home-news/coronavirus-lockdown-job-losses-unemployment-recession-university-essex-study-a9472966.html (accessed on 14 December 2021).
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Iwasaki, Y. Counteracting stress through leisure coping: A prospective health study. Psychol. Health Med. 2006, 11, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Lashua, B.; Johnson, C.W.; Parry, D.C. Leisure in the time of coronavirus: A rapid response special issue. Leis. Sci. 2021, 43, 6–11. [Google Scholar] [CrossRef]
- Clement, J. Video Gaming in the United Kingdom—Statistics & Facts. Available online: https://www.statista.com/topics/1763/gaming-in-the-united-kingdom/#:~:text=Between%202019%20and%202020%2C%20the,at%205.3%20billion%20British%20pounds (accessed on 14 December 2021).
- Lock, S. Gambling Industry in the United Kingdom (UK)—Statistics & Facts. Available online: https://www.statista.com/topics/3400/gambling-industry-in-the-united-kingdom-uk/ (accessed on 14 December 2021).
- Ko, C.-H.; Yen, J.-Y. Impact of COVID-19 on gaming disorder: Monitoring and prevention. J. Behav. Addict. 2020, 9, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Google. Google Trends—UK Searches for Online Slots. Available online: https://trends.google.com/trends/explore?date=2020-01-01%202020-03-31&geo=GB&q=online%20slots (accessed on 14 December 2021).
- Poker Sites Surge as Casual Players Return 2020. Personal communication, 29 March 2020.
- Yahya, A.S.; Khawaja, S. Problem gambling during the COVID-19 pandemic. Prim. Care Companion CNS Disord. 2020, 22, 27146. [Google Scholar] [CrossRef]
- Department for Digital, Culture, Media & Sport; Huddleston, N. Government Urges Gambling Industry to Tackle Risks of Problem Gambling during Coronavirus Outbreak. Available online: https://www.gov.uk/government/news/government-urges-gambling-industry-to-tackle-risks-of-problem-gambling-during-coronavirus-outbreak (accessed on 14 December 2021).
- Roberts, A.; Sharman, S.; Coid, J.; Murphy, R.; Bowden-Jones, H.; Cowlishaw, S.; Landon, J. Gambling and negative life events in a nationally representative sample of UK men. Addict. Behav. 2017, 75, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.T.A.; Griffiths, M.D. A qualitative investigation of problem gambling as an escape-based coping strategy. Psychol. Psychother. Theory Res. Pract. 2007, 80, 107–125. [Google Scholar] [CrossRef]
- Grubbs, J.B.; Rosansky, J.A. Problem gambling, coping motivations, and positive expectancies: A longitudinal survey study. Psychol. Addict. Behav. 2020, 34, 414–419. [Google Scholar] [CrossRef]
- Melodia, F.; Canale, N.; Griffiths, M.D. The role of avoidance coping and escape motives in problematic online gaming: A systematic literature review. Int. J. Ment. Health Addict. 2020, 1–27. [Google Scholar] [CrossRef]
- Kardefelt-Winther, D. The moderating role of psychosocial well-being on the relationship between escapism and excessive online gaming. Comput. Hum. Behav. 2014, 38, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Blasi, M.D.; Giardina, A.; Giordano, C.; Coco, G.L.; Tosto, C.; Billieux, J.; Schimmenti, A. problematic video game use as an emotional coping strategy: Evidence from a sample of MMORPG gamers. J. Behav. Addict. 2019, 8, 25–34. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H. The concept of “harm” in internet gaming disorder. J. Behav. Addict. 2018, 7, 562–564. [Google Scholar] [CrossRef]
- Li, W.; Mills, D.; Nower, L. The relationship of loot box purchases to problem video gaming and problem gambling. Addict. Behav. 2019, 97, 27–34. [Google Scholar] [CrossRef]
- Close, J.; Spicer, S.G.; Nicklin, L.L.; Uther, M.; Lloyd, J.; Lloyd, H. Secondary analysis of loot box data: Are high-spending “whales” wealthy gamers or problem gamblers? Addict. Behav. 2021, 117, 106851. [Google Scholar] [CrossRef] [PubMed]
- Collins, E.; Cox, A.; Wilcock, C.; Sethu-Jones, G. Digital games and mindfulness apps: Comparison of effects on post work recovery. JMIR Ment. Health 2019, 6, e12853. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H.; Billieux, J.; Potenza, M.N. Problematic online gaming and the COVID-19 pandemic. J. Behav. Addict. 2020, 9, 184–186. [Google Scholar] [CrossRef]
- Lloyd, H.; Jenkinson, C.; Hadi, M.; Gibbons, E.; Fitzpatrick, R. Patient reports of the outcomes of treatment: A structured review of approaches. Health Qual. Life Outcomes 2014, 12, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peer, E.; Brandimarte, L.; Samat, S.; Acquisti, A. Beyond the Turk: Alternative platforms for crowdsourcing behavioral research. J. Exp. Soc. Psychol. 2017, 70, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Stavropoulos, V.; Beard, C.; Griffiths, M.D.; Buleigh, T.; Gomez, R.; Pontes, H.M. measurement invariance of the Internet Gaming Disorder Scale–Short-Form (IGDS9-SF) between Australia, the USA, and the UK. Int. J. Ment. Health Addict. 2018, 16, 377–392. [Google Scholar] [CrossRef]
- Volberg, R.A.; Williams, R. Developing a Short Form of the PGSI 2012. Report to the Gambling Commission. 2012. Available online: https://opus.uleth.ca/bitstream/handle/10133/3129/Developing a Short Form of the PGSI.pdf (accessed on 14 December 2021).
- Stewart-Brown, S.; Platt, S.; Tennant, A.; Maheswaran, H.; Parkinson, J.; Weich, S.; Tennant, R.; Taggart, F.; Clarke, A. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): A valid and reliable tool for measuring mental well-being in diverse populations and projects. J. Epidemiol. Community Health 2011, 65, A38–A39. [Google Scholar] [CrossRef] [Green Version]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Gambling Commission. Gambling Participation in 2019: Behaviour, Awareness and Attitudes: Questionnaire Document. Available online: https://www.gamblingcommission.gov.uk/PDF/survey-data/Survey-questionnaire-document.pdf (accessed on 14 December 2021).
- R Core Team. R: A Language and Environment for Statistical Computing. 2020. Available online: https://www.r-project.org/ (accessed on 14 December 2021).
- Blanca, M.J.; Alarcón, R.; Arnau, J. Non-normal data: Is ANOVA still a valid option? Psicothema 2017, 552–557. [Google Scholar] [CrossRef]
- Schmider, E.; Ziegler, M.; Danay, E.; Beyer, L.; Bühner, M. Is It really robust? Reinvestigating the robustness of ANOVA against violations of the normal distribution assumption. Methodology 2010, 6, 147–151. [Google Scholar] [CrossRef]
- Office for National Statistics. Research Report on Population Estimates by Ethnic Group and Religion. Available online: https://www.ons.gov.uk/generator?uri=/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/researchreportonpopulationestimatesbyethnicgroupandreligion/2019-12-04/3a58b254&format=xls (accessed on 14 December 2021).
- UK Furlough Scheme Now Covers 8.4 Million Workers. Available online: https://www.bbc.co.uk/news/business-52819591 (accessed on 14 December 2021).
- Office for National Statistics. Comparison of Furloughed Jobs Data: May to July 2020. Available online: https://www.ons.gov.uk/businessindustryandtrade/business/businessservices/articles/comparisonoffurloughedjobsdata/maytojuly2020 (accessed on 14 December 2021).
- Pontes, H.M.; Griffiths, M.D. Measuring DSM-5 internet gaming disorder: Development and validation of a short psychometric scale. Comput. Hum. Behav. 2015, 45, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Ng Fat, L.; Scholes, S.; Boniface, S.; Mindell, J.; Stewart-Brown, S. Evaluating and establishing national norms for mental wellbeing using the Short Warwick–Edinburgh Mental Well-Being Scale (SWEMWBS): Findings from the health survey for England. Qual. Life Res. 2017, 26, 1129–1144. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.; Cader, M.; Andrews, W.P.; Wijesekera, D.; Stewart-Brown, S.L. Responsiveness of the Short Warwick Edinburgh Mental Well-Being Scale (SWEMWBS): Evaluation a clinical sample. Health Qual. Life Outcomes 2018, 16, 239. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental Health and Health Behaviours before and during the Initial Phase of the COVID-19 Lockdown: Longitudinal Analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2020, 75, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Teng, Z.; Pontes, H.M.; Nie, Q.; Griffiths, M.D.; Guo, C. Depression and anxiety symptoms associated with internet gaming disorder before and during the COVID-19 pandemic: A longitudinal study. JBA 2021, 10, 169–180. [Google Scholar] [CrossRef]
- Giardina, A.; Di Blasi, M.D.B.; Schimmenti, A.; King, D.L.; Starcevic, V.; Billieux, J. Online gaming and prolonged self-isolation: Evidence from Italian gamers during the COVID-19 outbreak. Clin. Neuropsychiatry 2021, 18, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Balhara, Y.P.S.; Kattula, D.; Singh, S.; Chukkali, S.; Bhargava, R. Impact of lockdown following COVID-19 on the gaming behavior of college students. Indian J. Public Health 2020, 64, S172–S176. [Google Scholar] [CrossRef]
- Garea, S.; Drummond, A.; Sauer, J.D.; Hall, L.C.; Williams, M. Meta-analysis of the relationship between problem gambling, excessive gaming and loot box purchasing. Int. Gambl. Stud. 2020, 21, 460–479. [Google Scholar] [CrossRef]
- Brooks, G.A.; Clark, L. Associations between loot box use, problematic gaming and gambling, and gambling-related cognitions. Addict. Behav. 2019, 96, 26–34. [Google Scholar] [CrossRef]
- Zendle, D.; Cairns, P. Video game loot boxes are linked to problem gambling: Results of a large-scale survey. PLoS ONE 2018, 13, e0206767. [Google Scholar] [CrossRef]
- Zendle, D.; Meyer, R.; Over, H. Adolescents and Loot Boxes: Links with Problem Gambling and Motivations for Purchase. R Soc. Open Sci 2019, 6, 190049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zendle, D. Problem gamblers spend less money when loot boxes are removed from a game: A before and after study of Heroes of the Storm. PeerJ 2019, 7, e7700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zendle, D.; Cairns, P. Loot boxes are again linked to problem gambling: Results of a replication study. PLoS ONE 2019, 14, e0213194. [Google Scholar] [CrossRef] [Green Version]
- Auer, M.; Malischnig, D.; Griffiths, M.D. Gambling before and during the COVID-19 pandemic among European regular sports bettors: An empirical study using behavioral tracking data. Int. J. Ment. Health Addict. 2020, 1–8. [Google Scholar] [CrossRef]
- Gainsbury, S.M.; Swanton, T.B.; Burgess, M.T.; Blaszczynski, A. Impacts of the COVID-19 shutdown on gambling patterns in Australia: Consideration of problem gambling and psychological distress. J. Addict. Med. 2020, 15, 468. [Google Scholar] [CrossRef] [PubMed]
- Gambling Commission. Gambling Business Data on Gambling during COVID-19 [Updated December 2020]. Available online: https://www.gamblingcommission.gov.uk/news-action-and-statistics/Statistics-and-research/Covid-19-research/Covid-19-updated-December-2020/Gambling-business-data-on-gambling-during-Covid-19-updated-December-2020.aspx (accessed on 14 December 2021).
- Gambling Commission. Market Overview for December 2020—Operator Data. Available online: https://www.gamblingcommission.gov.uk/news-action-and-statistics/Statistics-and-research/Covid-19-research/Covid-19-updated-December-2020/Market-overview-for-December-2020-operator-data.aspx (accessed on 14 December 2021).
- Håkansson, A. Changes in gambling behavior during the COVID-19 pandemic—A Web survey study in Sweden. Int. J. Environ. Res Public Health 2020, 17, 4013. [Google Scholar] [CrossRef]
- Lindner, P.; Forsström, D.; Jonsson, J.; Berman, A.H.; Carlbring, P. Transitioning between online gambling modalities and decrease in total gambling activity, but no indication of increase in problematic online gambling intensity during the first phase of the COVID-19 outbreak in Sweden: A time series forecast study. Front. Public Health 2020, 8, 554542. [Google Scholar] [CrossRef]
- Xuereb, S.; Kim, H.S.; Clark, L.; Wohl, M.J.A. Substitution behaviors among casino gamblers during COVID-19 precipitated casino closures. PsyArXiv 2020, 10, 31234. [Google Scholar]
- Sharman, S.; Roberts, A.; Bowden-Jones, H.; Strang, J. Gambling in COVID-19 lockdown in the UK: Depression, stress, and anxiety. Front. Psychiatry 2021, 12, 621497. [Google Scholar] [CrossRef]
- Fluharty, M.; Paul, E.; Fancourt, D. Predictors and patterns of gambling behaviour across the COVID-19 lockdown: Findings from a UK cohort study. J. Affect. Disord. 2022, 298, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Price, A. Online gambling in the midst of COVID-19: A nexus of mental health concerns, substance use and financial stress. Int J. Ment. Health Addict. 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Hipp, L.; Bünning, M.; Munnes, S.; Sauermann, A. Problems and pitfalls of retrospective survey questions in COVID-19 studies. In Survey Research Methods; European Survey Research Association: Konstanz, Germany, 2020; pp. 109–114. [Google Scholar] [CrossRef]
- Soman, D. Effects of payment mechanism on spending behavior: The role of rehearsal and immediacy of payments. J. Consum. Res. 2001, 27, 460–474. [Google Scholar] [CrossRef]
- Jaspers, E.; Lubbers, M.; De Graaf, N.D. Measuring once twice: An evaluation of recalling attitudes in survey research. Eur. Sociol. Rev. 2009, 25, 287–301. [Google Scholar] [CrossRef] [Green Version]
- Teng, Z.; Pontes, H.M.; Nie, Q.; Xiang, G.; Griffiths, M.D.; Guo, C. Internet gaming disorder and psychosocial well-being: A longitudinal study of older-aged adolescents and emerging adults. Addict. Behav. 2020, 110, 106530. [Google Scholar] [CrossRef]
- Ellis, L.A.; Lee, M.D.; Ijaz, K.; Smith, J.; Braithwaite, J.; Yin, K. COVID-19 as ‘game changer’ for the physical activity and mental well-being of augmented reality game players during the pandemic: Mixed methods survey study. J. Med. Internet Res. 2020, 22, e25117. [Google Scholar] [CrossRef]

{kind=link}
| Demographics n = 631 | ||
|---|---|---|
| Media Age (SD) | 45.28 (15.33) | |
| Gender F (% Female) | 319 | 50.55% |
| Ethnicity: | ||
| White | 521 | 82.57% |
| Black/African/Caribbean/Black British | 26 | 4.12% |
| Asian/Asian British | 47 | 7.45% |
| Mixed/Multiple ethnic groups | 20 | 3.17% |
| Other ethnic group | 15 | 2.38% |
| Occupation: | ||
| Full-time education | 31 | 4.91% |
| Full-time employee furloughed during lockdown | 42 | 6.66% |
| Full-time employee | 233 | 36.93% |
| Looking after the home/family | 64 | 10.14% |
| Other/Prefer not to answer | 77 | 12.20% |
| Part-time employee furloughed during lockdown | 21 | 3.33% |
| Part-time employee (<30 h/week) | 56 | 8.87% |
| Seeking opportunities/work | 38 | 6.02% |
| Self-employed | 69 | 10.94% |
| Gamers/Gamblers | ||
| % Plays video games | 465 | 73.69% |
| % Gambled | 449 | 71.16% |
| Both gambled and played games | 283 | 44.85% |
| Before Lockdown | After Lockdown | Change (* = p < 0.01) | |
|---|---|---|---|
| Mean days played per week | 2.35 | 3.80 | 1.45 * |
| Mean hours played per day | 1.54 | 2.80 | 1.26 * |
| Mean in-app purchase monthly spend (n = 127) | £6.05 | £18.40 | £12.36 * |
| Mean loot box monthly spend (n = 28) | £5.87 | £32.36 | £26.48 * |
| Mean risky loot box index score | 15.61 | 17.89 | 2.29 |
| Mean IGD score | 13.40 | 15.25 | 1.85 * |
| Mean IGD scores, item-by-item | |||
| Preoccupation | 1.77 | 2.25 | 0.48 * |
| Irritability | 1.38 | 1.57 | 0.20 * |
| Time | 1.60 | 1.94 | 0.34 * |
| Loss of control | 1.35 | 1.51 | 0.16 * |
| Loss of interest | 1.48 | 1.77 | 0.30 * |
| Continued gaming | 1.29 | 1.35 | 0.06 |
| Deception | 1.14 | 1.18 | 0.05 |
| Escape | 2.29 | 2.56 | 0.27 * |
| Jeopardised job/relationship | 1.10 | 1.11 | 0.00 |
| Before Lockdown | After Lockdown | Change (* = p < 0.01) | Online/ Offline | |
|---|---|---|---|---|
| Gambling Activities (% gamble every week) | ||||
| Overall Weekly Gamblers | 60.36% | 56.12% | −4.23% | |
| Offline Gamblers | 5.79% | 0.22% | −5.57% * | |
| Online Gamblers | 16.93% | 21.16% | 4.23% | |
| Individual Gambling Activities (% gamble every week) | ||||
| Lottery | 36.97% | 38.31% | 1.34% | Both |
| Scratchcards | 9.80% | 9.58% | −0.22% * | Both |
| Online Instant Wins | 3.34% | 5.12% | 1.78% | Online |
| Offline Fruit Machines | 2.90% | 0.22% | −2.67% * | Offline |
| Online Fruits and Slots | 8.46% | 11.58% | 3.12% | Online |
| Offline Gaming Machines | 3.12% | 0.00% | −3.12% * | Offline |
| Offline Bingo | 1.34% | 0.00% | −1.34% * | Offline |
| Online Bingo | 4.90% | 5.79% | 0.89% | Online |
| Sports | 21.83% | 13.36% | −8.46% * | Both |
| Virtual Sports | 1.78% | 2.23% | 0.45% | Online |
| eSports | 0.67% | 0.89% | 0.22% | Online |
| Politics Other Events | 0.45% | 0.45% | 0.00% | Both |
| Offline Casino | 0.89% | 0.00% | −0.89% * | Offline |
| Online Casino | 4.23% | 6.46% | 2.23% | Online |
| Private Betting | 1.34% | 3.34% | 2.00% * | Both |
| Other | 4.45% | 5.35% | 0.89% | Both |
| PGSI: Mean Score | 0.57 | 0.49 | −0.08 | |
| Problem Gambler Status | ||||
| Non Problem Gamblers | 310 | 321 | 11 | |
| Low Risk Gamblers | 82 | 71 | −11 | |
| Moderate Risk | 43 | 47 | 4 | |
| Problem Gambler | 14 | 10 | −4 |
| Variable | Population | n | WEMWBS-SF | ANOVA | |||
|---|---|---|---|---|---|---|---|
| Before | After | Change | p | ges | |||
| Time | Full cohort | 631 | 23.3 | 21.3 | −2 * | 1.28 × 10−42 | 0.062 |
| Sex:time | F | 319 | 23.2 | 21 | −2.2 | ||
| M | 312 | 23.2 | 21.6 | −1.6 * | 6.00 × 10−3 | 0.002 | |
| Maritial status:time | Co-habiting with partner | 115 | 22.9 | 21.1 | −1.8 | 7.24 × 10−1 | 0.000913 |
| Divorced/separated | 43 | 23.3 | 20.9 | −2.4 | |||
| In a relationship | 41 | 22.1 | 19.8 | −2.3 | |||
| Married | 280 | 24.1 | 22.2 | −1.9 | |||
| Prefer not to say | 7 | 24.3 | 21 | −3.3 | |||
| Single | 145 | 22.2 | 20.1 | −2.1 | |||
| Income:time | £10,001–£15,000 | 49 | 22.9 | 21.4 | −1.5 | 2.56 × 10−1 | 0.003 |
| £15,001– £20,000 | 73 | 22.8 | 21 | −1.8 | |||
| £20,001–£25,000 | 86 | 22.5 | 20.7 | −1.8 | |||
| £25,001–£30,000 | 71 | 23.4 | 20.6 | −2.8 | |||
| £30,001–£40,000 | 64 | 23.7 | 21.7 | −2 | |||
| Above £40,000 | 75 | 23.8 | 22.2 | −1.6 | |||
| Below £10,000 | 73 | 22.1 | 20.6 | −1.5 | |||
| Not earning | 118 | 24.2 | 21.8 | −2.4 | |||
| Prefer not to answer | 22 | 23.4 | 21.5 | −1.9 | |||
| Ethnicity:time | Asian | 47 | 22.8 | 21.5 | −1.3 | 2.37 × 10−1 | 0.002 |
| Black African/Caribbean | 26 | 24.2 | 21.3 | −2.9 | |||
| Mixed | 20 | 23.2 | 20.4 | −2.8 | |||
| Other | 17 | 21.7 | 20.6 | −1.1 | |||
| White | 521 | 23.3 | 21.3 | −2 | |||
| Gaming | |||||||
| IGDSF9 score before:time | 3.12 × 10−1 | 0.01 | |||||
| IGDSF9 score after:time | 1.10 × 10−4 | 0.03 | |||||
| Gambling | |||||||
| PGSI score before:time | 5.90 × 10−1 | 0.006 | |||||
| PGSI score after:time | 3.45 × 10−1 | 0.003 | |||||
| Path | β (ci-low, ci-high) | p |
|---|---|---|
| MWBS2~MWBS1 | 0.60 (0.54, 0.66) | 0.00 |
| MWBS2~SI1 | 0.02 (−0.06, 0.10) | 0.66 |
| MWBS2~IGD1 | −0.07 (−0.15, 0.01) | 0.08 |
| PGSI2~MWBS1 | −0.04 (−0.11, 0.04) | 0.33 |
| PGSI2~PGSI1 | 0.56 (0.49, 0.63) | 0.00 |
| PGSI2~IGD1 | 0.16 (0.07, 0.26) | 0.00 |
| IGD2~MWBS1 | −0.01 (−0.08, 0.07) | 0.87 |
| IGD2~PGSI1 | 0.03 (−0.06, 0.11) | 0.58 |
| IGD2~IGD1 | 0.67 (0.61, 0.73) | 0.00 |
| MWBS2~~PGSI2 | −0.21 (−0.30, −0.12) | 0.00 |
| MWBS2~~IGD2 | −0.31 (−0.39, −0.23) | 0.00 |
| PGSI2~~IGD2 | 0.30 (0.20, 0.40) | 0.00 |
| MWBS1~~PGSI1 | −0.24 (−0.32, −0.15) | 0.00 |
| MWBS1~~IGD1 | −0.32 (−0.40, −0.24) | 0.00 |
| PGSI1~~IGD1 | 0.34 (0.24, 0.44) | 0.00 |
| MWBS2~~MWBS2 | 0.61 (0.55, 0.67) | 0.00 |
| PGSI2~~PGSI2 | 0.58 (0.51, 0.65) | 0.00 |
| IGD2~~IGD2 | 0.54 (0.47, 0.60) | 0.00 |
| MWBS1~~MWBS1 | 1.00 (1.00, 1.00) | NA |
| PGSI1~~PGSI1 | 1.00 (1.00, 1.00) | NA |
| IGD1~~IGD1 | 1.00 (1.00, 1.00) | NA |
| MWBS2~1 | 1.99, (1.39, 2.58) | 0.00 |
| PGSI2~1 | −0.06 (−0.68, 0.57) | 0.86 |
| IGD2~1 | 0.69 (0.13, 1.24) | 0.02 |
| MWBS1~1 | 6.10 (5.76, 6.45) | 0.00 |
| PGSI1~1 | 0.52 (0.42, 0.62) | 0.00 |
| IGD1~1 | 3.19 (2.96, 3.41) | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Close, J.; Spicer, S.G.; Nicklin, L.L.; Lloyd, J.; Whalley, B.; Lloyd, H. Gambling and Gaming in the United Kingdom during the COVID-19 Lockdown. COVID 2022, 2, 87-101. https://doi.org/10.3390/covid2020007
Close J, Spicer SG, Nicklin LL, Lloyd J, Whalley B, Lloyd H. Gambling and Gaming in the United Kingdom during the COVID-19 Lockdown. COVID. 2022; 2(2):87-101. https://doi.org/10.3390/covid2020007
Chicago/Turabian StyleClose, James, Stuart Gordon Spicer, Laura Louise Nicklin, Joanne Lloyd, Ben Whalley, and Helen Lloyd. 2022. "Gambling and Gaming in the United Kingdom during the COVID-19 Lockdown" COVID 2, no. 2: 87-101. https://doi.org/10.3390/covid2020007
APA StyleClose, J., Spicer, S. G., Nicklin, L. L., Lloyd, J., Whalley, B., & Lloyd, H. (2022). Gambling and Gaming in the United Kingdom during the COVID-19 Lockdown. COVID, 2(2), 87-101. https://doi.org/10.3390/covid2020007