
Prevalence of Anti-SARS-CoV-2 Antibodies in HIV-Positive Patients in Wroclaw, Poland—Unexpected Difference between First and Second Wave


Abstract
1. Introduction
Objective of the Work
2. Materials and Methods
2.1. Material
2.2. Methods
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ssentongo, P.; Heilbrunn, E.S.; Ssentongo, A.E.; Advani, S.; Chinchilli, V.M.; Nunez, J.J.; Du, P. Prevalence of HIV in patients hospitalized for COVID-19 and associated outcomes: A systematic review and meta-analysis. MedRxiv 2020. [Google Scholar] [CrossRef]
- COVID-19 Stats: COVID-19 Incidence, by Age Group—United States, 1 March–14 November 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 69, 1664. [CrossRef] [PubMed]
- Snider, B.; Patel, B.; McBean, E. Asymptomatic Cases, the Hidden Challenge in Predicting COVID-19 Caseload Increases. Infect. Dis. Rep. 2021, 13, 340–347. [Google Scholar] [CrossRef] [PubMed Central]
- Mannar, D.; Leopold, K.; Subramaniam, S. Glycan reactive anti-HIV-1 antibodies bind the SARS-CoV-2 spike protein but do not block viral entry. Sci. Rep. 2021, 11, 12448. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Lopinavir-ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomized, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Melchjorsen, J.; Risør, M.W.; Søgaard, O.S.; O’Loughlin, K.L.; Chow, S.; Paludan, S.R.; Ellermann-Eriksen, S.; Hedley, D.W.; Minderman, H.; Østergaard, L.; et al. Tenofovir selectively regulates production of inflammatory cytokines and shifts the IL-12/IL-10 balance in human primary cells. J. Acquir. Immune. Defic. Syndr. 2011, 57, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Zídek, Z.; Holý, A.; Franková, D. Antiretroviral agent (R)-9-(2-phosphonomethoxypropyl) adenine stimulates cytokine and nitric oxide production. Eur. J. Pharmacol. 1997, 331, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Zídek, Z.; Holý, A.; Franková, D. Immunomodulatory properties of antiviral acyclic nucleotide analogues: Cytokine stimulatory and nitric oxide costimulatory effects. Int. J. Immunopharmacol. 1997, 19, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Zídek, Z.; Franková, D.; Holý, A. Activation by 9-(R)-[2-(phosphonomethoxy) propyl] adenine of chemokine (RANTES, macrophage inflammatory protein 1alpha) and cytokine (tumor necrosis factor alpha, interleukin-10 [IL-10], IL-1beta) production. Antimicrob. Agents Chemother. 2001, 45, 3381–3386. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef]
- Catanzaro, M.; Fagiani, F.; Racchi, M.; Corsini, E.; Govoni, S.; Lanni, C. Immune response in COVID-19: Addressing a pharmacological challenge by targeting pathways triggered by SARS-CoV-2. Sig. Transduct. Target. Ther. 2020, 5, 84. [Google Scholar] [CrossRef]
- Lorent, D.; Nowak, R.; Roxo, C.; Lenartowicz, E.; Makarewicz, A.; Zaremba, B.; Nowak, S.; Kuszel, L.; Stefaniak, J.; Kierzek, R.; et al. Prevalence of Anti-SARS-CoV-2 Antibodies in Poznań, Poland, after the First Wave of the COVID-19 Pandemic. Vaccines 2021, 9, 541. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartin, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; Ridder, D.D.; Petrovis, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Available online: https://www.pzh.gov.pl/wp-content/uploads/2021/02/Suplement-do-Rozdzialu-7-seroprewalencja.pdf (accessed on 3 November 2022).
- Kowalska, M.; Niewiadomska, E.; Barański, K.; Kaleta-Pilarska, A.; Brożek, G.; Zejda, J.E. Association between Influenza Vaccination and Positive SARS-CoV-2 IgG and IgM Tests in the General Population of Katowice Region, Poland. Vaccines 2021, 9, 415. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Available online: https://koronawirusunas.pl/wojewodztwo-dolnoslaskie (accessed on 3 November 2022).
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Grint, D.J.; Wing, K.; Houlihan, C.; Gibbs, H.P.; Evans, S.J.W.; Williamson, E.; I McDonald, H.; Bhaskaran, K.; Evans, D.; Walker, A.J.; et al. Severity of SARS-CoV-2 alpha variant (B.1.1.7) in England. Clin Infect Dis. 2021, 6, ciab754. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zejda, J.; Brożek, G.; Kowalska, M.; Barański, K.; Kaleta-Pilarska, A.; Nowakowski, A.; Xia, Y.; Buszman, P. Seroprevalence of Anti-SARS-CoV-2 Antibodies in a Random Sample of Inhabitants of the Katowice Region, Poland. Int. J. Environ. Res. Public Health 2021, 18, 3188. [Google Scholar] [CrossRef]
- Lombardi, F.; Ricci, R.; Belmonti, S.; Fabbiani, M.; Borghetti, A.; Baldin, G.; Ciccullo, A.; Tamburrini, E.; Visconti, E.; Sanguinetti, M.; et al. Seroprevalence of SARS-CoV-2 Antibodies in HIV-Infected Patients in Rome, Italy during the COVID-19 Outbreak. Diagnostics 2021, 11, 1154. [Google Scholar] [CrossRef]
- del Amo, J.; Polo, R.; Moreno, S.; Díaz, A.; Martínez, E.; Arribas, J.R.; Jarrín, I.; Hernán, M.A. Incidence and Severity of COVID-19 in HIV-Positive Persons Receiving Antiretroviral Therapy: A Cohort Study. Ann. Intern. Med. 2020, 173, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Elfiky, A.A. Ribavirin, Remdesivir, Sofosbuvir, Galidesivir, andTenofovir against SARS-CoV-2 RNA dependent RNApolymerase (RdRp): A molecular docking study. Life Sci. 2020, 253, 117592. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, M.; Srinivasula, S.; Bhattacharjee, A.; Cheng, L.; Martiniova, L.; Herscovitch, P.; Lertora, J.; Kiesewetter, D. Antiretroviral tissue kinetics: In vivo imaging using positron emission tomography. Antimicrob. Agents Chemother. 2009, 53, 4086–4095. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, S.; Yu, K.-M.; Kim, Y.-I.; Kim, S.-M.; Kim, E.-H.; Kim, S.-G.; Kim, E.J.; Casel, M.A.B.; Rollon, R.; Jang, S.-G.; et al. Antiviral efficacies ofFDA-approved drugs against SARS-CoV-2 infection in ferrets. mBio 2020, 11, e01114-20. [Google Scholar] [CrossRef] [PubMed]
- Twigg, H.L.; Schnizlein-Bick, C.T.; Weiden, M.; Valentine, F.; Wheat, J.; Day, R.B.; Rominger, H.; Zheng, L.; Collman, R.G.; Coombs, R.W.; et al. Measurement of antiretroviral drugs in the lungs of HIV-infected patients. HIV Ther. 2010, 4, 247–251. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Parienti, J.J.; Prazuck, T.; Peyro-Saint-Paul, L.; Fournier, A.; Valentin, C.; Brucato, S.; Verdon, R.; Sève, A.; Colin, M.; Lesne, F.; et al. Effect of Tenofovir Disoproxil Fumarate and Emtricitabine on nasopharyngeal SARS-CoV-2 viral load burden amongst outpatients with COVID-19: A pilot, randomized, open-label phase 2 trial. eClinicalMedicine 2021, 38, 100993. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, Y.; Li, P.; Ding, Y.; Liu, M.; Liu, L.; Yi, B.; Wu, T.; Dong, H.; Lao, X.; Ding, K.; et al. Epidemiological feature, viral shedding, and antibody seroconversion among asymptomatic SARS-CoV-2 carriers and symptomatic/presymptomatic COVID-19 patients. J. Infect. Public Health 2021, 14, 845–851. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marchi, S.; Viviani, S.; Remarque, E.J.; Ruello, A.; Bombardieri, E.; Bollati, V.; Milani, G.P.; Manenti, A.; Lapini, G.; Rebuffat, A.; et al. Characterization of antibody response in asymptomatic and symptomatic SARS-CoV-2 infection. PLoS ONE 2021, 16, e0253977. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Boyton, R.J.; Altmann, D.M. The immunology of asymptomatic SARS-CoV-2 infection: What are the key questions? Nat. Rev. Immunol. 2021, 21, 762–768. [Google Scholar] [CrossRef]
- Leister, I.; Ponocny-Seliger, E.; Kollaritsch, H.; Dungel, P.; Holzer, B.; Grillari, J.; Redl, H.; Ponocny, I.; Wilfing, C.; Aigner, L.; et al. Antibody seroprevalence and rate of asymptomatic infections with SARS-CoV-2 in Austrian hospital personnel. BMC Infect. Dis. 2021, 21, 915. [Google Scholar] [CrossRef]
- Mishra, N.; Kumar, S.; Singh, S.; Bansal, T.; Jain, N.; Saluja, S.; Kumar, R.; Bhattacharyya, S.; Palanichamy, J.K.; Mir, R.A.; et al. Cross-neutralization of SARS-CoV-2 by HIV-1 specific broadly neutralizing antibodies and polyclonal plasma. LoS Pathog. 2021, 17, e1009958. [Google Scholar] [CrossRef]
- Karim, F.; Gazy, I.; Cele, S.; Zungu, Y.; Krause, R.; Bernstein, M.; Ganga, Y.; Rodel, H.; Mthabela, N.; Mazibuko, M.; et al. Alex Sigal HIV status alters disease severity and immune cell responses in β variant SARS-CoV-2 infection wave. medRxiv 2021. [Google Scholar] [CrossRef]
- Wen, X.-S.; Jiang, D.; Gao, L.; Zhou, J.-Z.; Xiao, J.; Cheng, X.-C.; Bin He, B.; Chen, Y.; Lei, P.; Tan, X.-W.; et al. Clinical characteristics and predictive value of lower CD4+T cell level in patients with moderate and severe COVID-19: A multicenter retrospective study. BMC Infect. Dis. 2021, 21, 57. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, L.; Xu, L.; Lin, C. T cell response in patients with COVID-19. Blood Sci. 2020, 2, 76–78. [Google Scholar] [CrossRef]
- del Amo, J.; Polo, R.; Moreno, S.; Diaz, A.; Martínez, E.; Arribas, J.R.; Jarrín, I.; Hernán, M.A. Antiretrovirals and Risk of COVID-19 Diagnosis and Hospitalization in HIV-Positive Persons. Epidemiology 2020, 31, e49–e51. [Google Scholar] [CrossRef]
- Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa. Erratum to: Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2022, 74, 1321, Erratum for: Clin Infect Dis. 2021, 73, e2005–e2015. [CrossRef] [PubMed] [PubMed Central]
- Charre, C.; Icard, V.; Pradat, P.; Brochier, C.; Lina, B.; Chidiac, C.; Cotte, L. Coronavirus disease 2019 attack rate in HIV-infected patients and in preexposure prophylaxis users. AIDS 2020, 34, 1765–1770. [Google Scholar] [CrossRef]


{kind=link}
| First Samples | Second Samples | |
|---|---|---|
| Number of participants | 216 | 154 |
| Women | 42 | 32 |
| Men | 174 | 122 |
| without ARV Treatment | 36 | 0 |
| with ARV Treatment | 180 | 214 |
| Age (years) | 41 (21–77) | 41 (21–77) |
| Median Age | 39 | 39 |
| Viral Load, copies/mL | 4,433,357–not detected | 141–not detected |
| CD4 (+) T cells/µL median (min–max) | 608 (65–1502) | 606 (41–1350) |
| CD8 (+) T cells/µL median (min–max) | 779 (192–4000) | 756 (163–2569) |
| CD4 (+) T cells/CD8 (+) T cells ratio median (min–max) | 0.775 (0.05–2.99) | 0.785 (0.11–3.03) |
| First Positive Sample (Date) | 10 March 2020 | 15 September 2020 |
| Last Positive Sample (Date) | 29 September 2020 | 18 February 2021 |
| A Treatment Drug Containing Tenofovir | Number | Cumulative Number | Percent | Cumulative Percentage |
|---|---|---|---|---|
| BIC/FTC/TAF | 20 | 20 | 9.17431 | 9.1743 |
| FTC/TDF | 30 | 98 | 13.76147 | 44.95413 |
| FTC/TAF 200 mg/10 mg | 1 | 218 | 0.45872 | 100.0000 |
| FTC/TAF 200 mg/25 mg | 91 | 141 | 41.74312 | 64.6789 |
| EVG/COBI/FTC/TAF | 76 | 217 | 34.86239 | 99.5413 |
| First Term | Second Term | Total | |
|---|---|---|---|
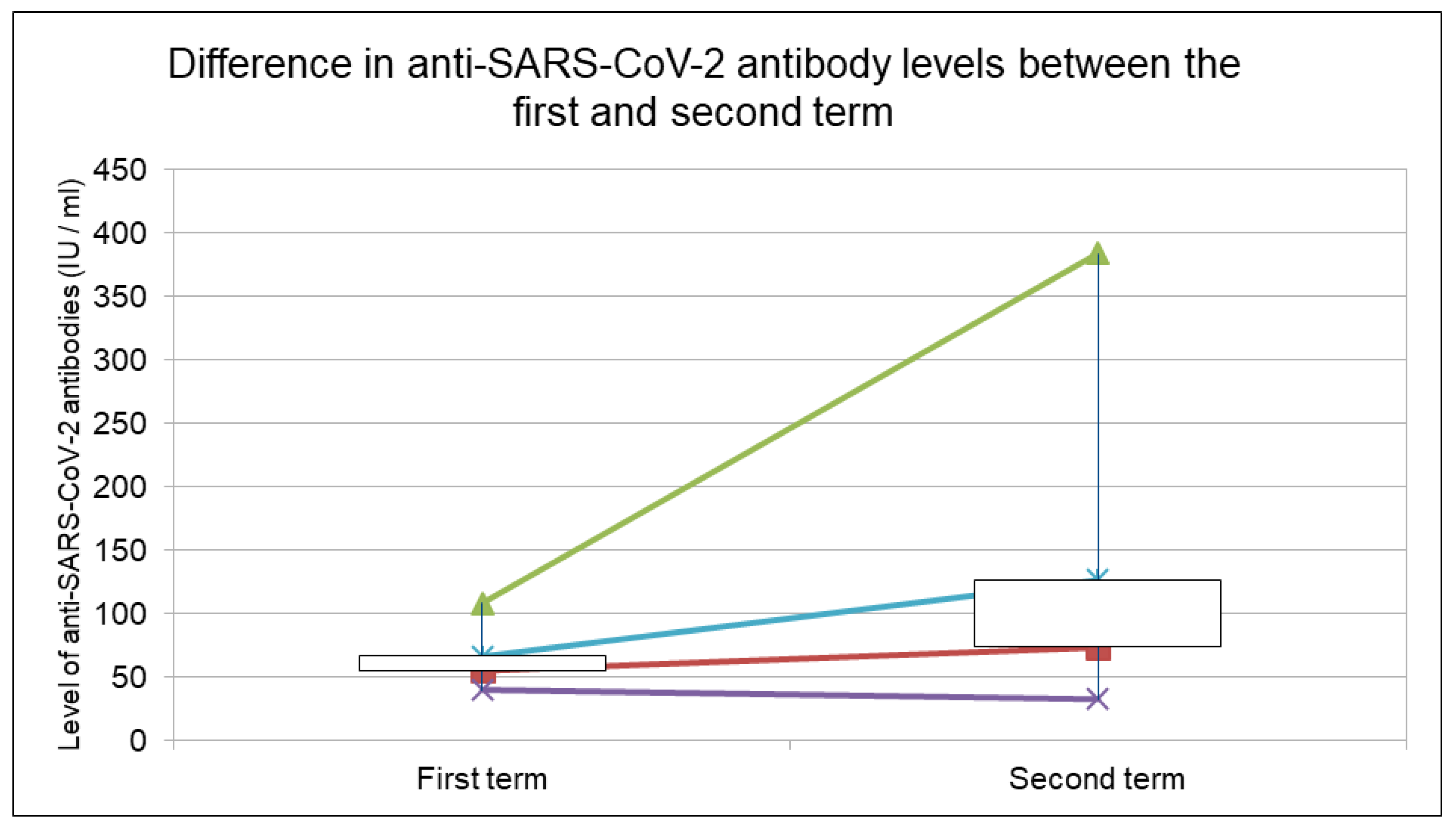
| Positive Samples | 9 (4.17%) | 22 (14.29%) | 31 (14.35%) |
| Level of anti-SARS-CoV-2 antibodies average value (min–max) IU/mL | 65.81 (39.4–107.8) | 125.98 (32–384) | 108.51 (32–384) |
| Age | 37.4 (26–53) | 37.2 (26–60) | 37.2 (26–60) |
| Female | 2 (22.2%) | 5 (22.7%) | 7 (22.6%) |
| Male | 7 (77.8%) | 17 (77.3%) | 24 (77.4%) |
| Correlation of the Presence or Level of Anti-SARS-CoV-2 Antibodies with the Number of Lymphocytes CD4+, CD8+, the Ratio of CD4+/CD8+, and Age | ||||
|---|---|---|---|---|
| Number of CD4+ T Cells | Number of CD8+ T Cells | Ratio of CD4+ T Cells to CD8+ T Cells | Age | |
| presence of anti-SARS-CoV-2 antibodies—Spearman’s rank order correlation | 0.027176 | 0.029565 | −0.00078 | −0.09257 |
| presence of anti-SARS-CoV-2 antibodies -Kendall tau correlation | 0.021075 | 0.023614 | −0.00033 | −0.07603 |
| level of anti-SARS-CoV-2 antibodies—Spearman’s rank order correlation | 0.506073 | 0.903972 | 0.525919 | 0.460506 |
| level of anti-SARS-CoV-2 antibodies—Kendall tau correlation | 0.414195 | 0.891751 | 0.517723 | 0.484320 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciepłucha, H.D.; Zalewska, M.; Kujawa, K.; Szetela, B. Prevalence of Anti-SARS-CoV-2 Antibodies in HIV-Positive Patients in Wroclaw, Poland—Unexpected Difference between First and Second Wave. COVID 2022, 2, 1748-1757. https://doi.org/10.3390/covid2120125
Ciepłucha HD, Zalewska M, Kujawa K, Szetela B. Prevalence of Anti-SARS-CoV-2 Antibodies in HIV-Positive Patients in Wroclaw, Poland—Unexpected Difference between First and Second Wave. COVID. 2022; 2(12):1748-1757. https://doi.org/10.3390/covid2120125
Chicago/Turabian StyleCiepłucha, Hubert Dawid, Małgorzata Zalewska, Krzysztof Kujawa, and Bartosz Szetela. 2022. "Prevalence of Anti-SARS-CoV-2 Antibodies in HIV-Positive Patients in Wroclaw, Poland—Unexpected Difference between First and Second Wave" COVID 2, no. 12: 1748-1757. https://doi.org/10.3390/covid2120125
APA StyleCiepłucha, H. D., Zalewska, M., Kujawa, K., & Szetela, B. (2022). Prevalence of Anti-SARS-CoV-2 Antibodies in HIV-Positive Patients in Wroclaw, Poland—Unexpected Difference between First and Second Wave. COVID, 2(12), 1748-1757. https://doi.org/10.3390/covid2120125