
Diabetic Foot Osteomyelitis Caused by Co-Infection with Methicillin-Resistant Staphylococcus aureus and Multidrug-Resistant Extended-Spectrum ß-Lactamase-Producing Escherichia coli: A Case Report

 , and
, and 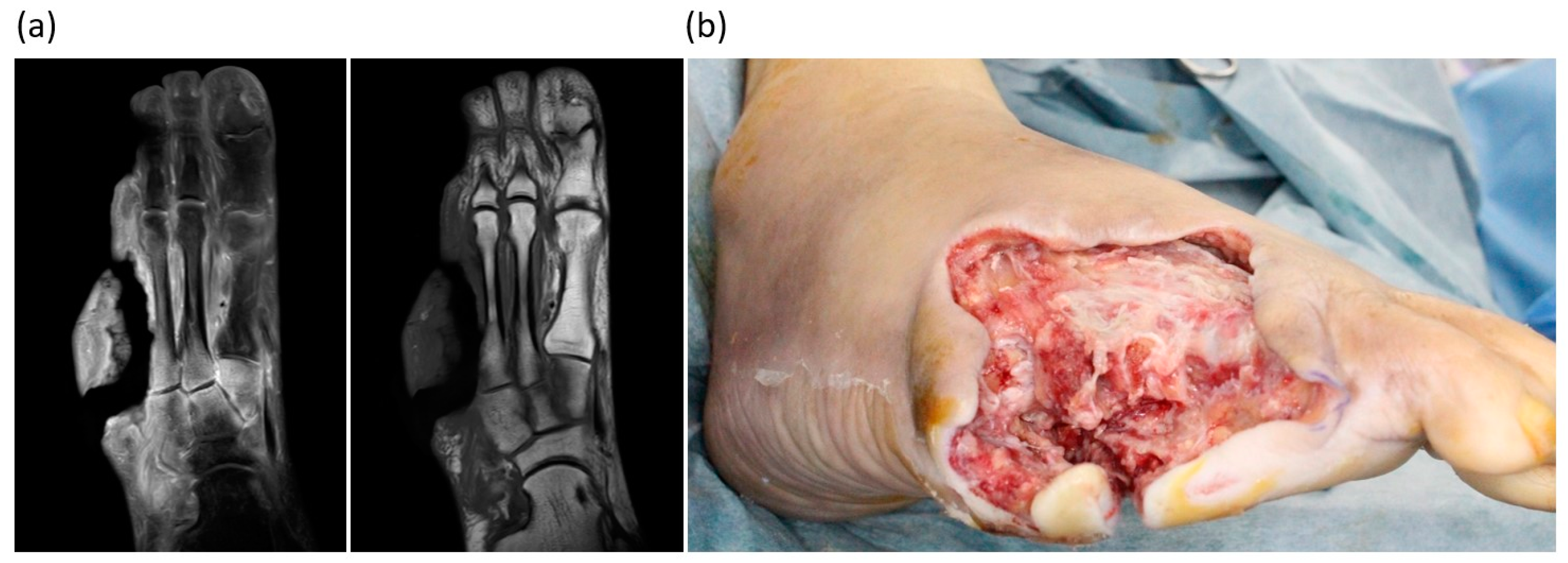{kind=link}
{kind=link}
Abstract
:1. Introduction
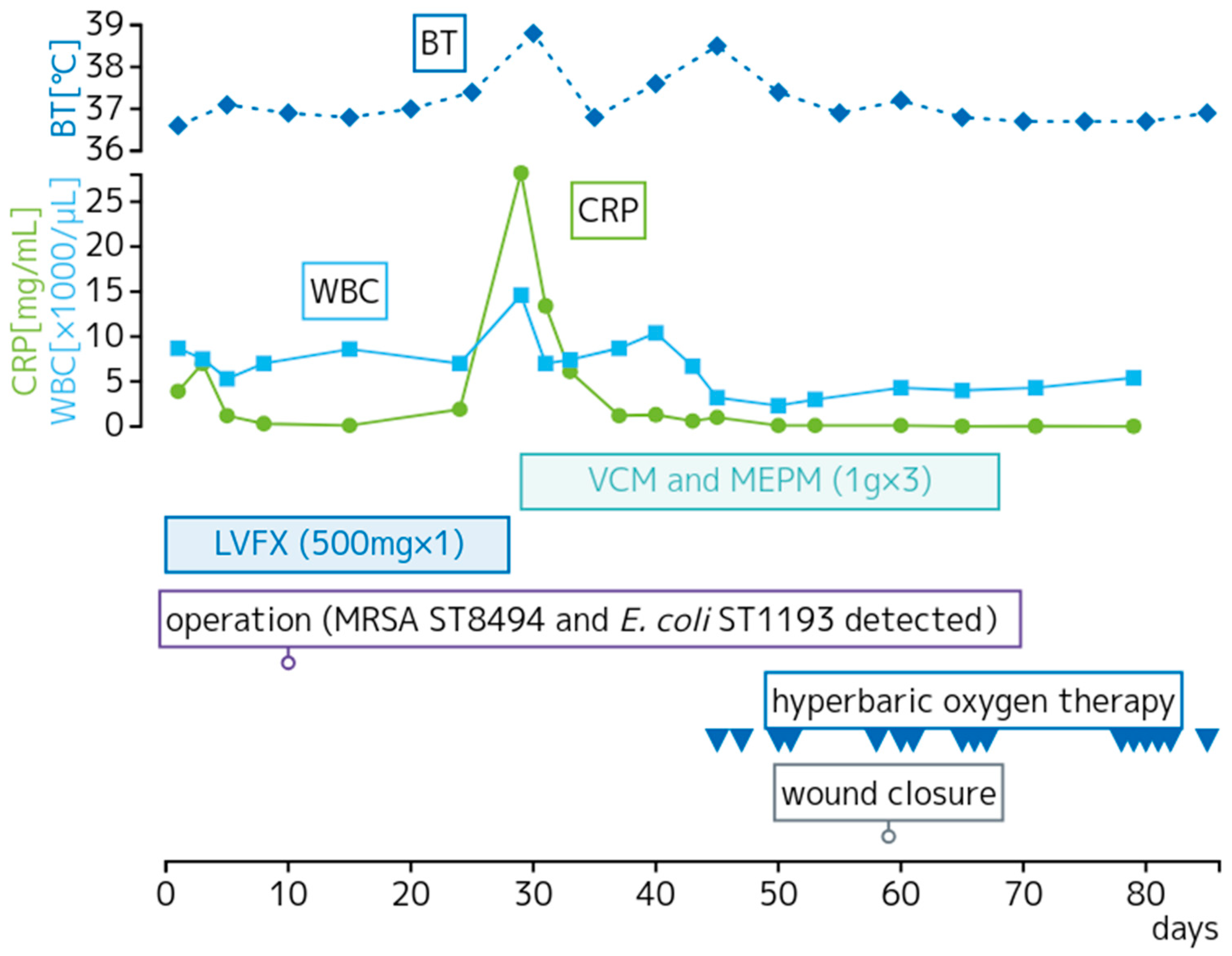
2. Detailed Case Description
3. Discussion
3.1. Microbiological Characteristics of MRSA ST764 and E. coli ST1193
3.2. Virulence Genes of MRSA and MDR ESBL-Producing E. coli
3.3. Antimicrobial Resistance Genes of MRSA and MDR ESBL-Producing E. coli
3.4. Clinical and Epidemiological Characteristics of DFI and DFO
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lavery, L.A.; Ryan, E.C.; Ahn, J.; Crisologo, P.A.; Oz, O.K.; La Fontaine, J.; Wukich, D.K. The infected diabetic foot: Re-evaluating the Infectious Diseases Society of America diabetic foot infection classification. Clin. Infect. Dis. 2020, 70, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Uçkay, I. Treating diabetic foot osteomyelitis: A practical state-of-the-art update. Medicina 2021, 57, 339. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.; Ziegler, R.; Mattner, F.; Schwab, F.; Gastmeier, P.; Martin, M. Increase of patients co-colonised or co-infected with methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus faecium or extended-spectrum ß-lactamase-producing Enterobacteriaceae. Infection 2011, 39, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Goodman, K.E.; Simner, P.J.; Tamma, P.D.; Milstone, A.M. Infection control implications of heterogeneous resistance mechanisms in carbapenem-resistant Enterobacteriaceae (CRE). Expert Rev. Anti-Infect. Ther. 2016, 14, 95–108. [Google Scholar] [CrossRef]
- Takano, T.; Hung, W.-C.; Shibuya, M.; Higuchi, W.; Iwao, Y.; Nishiyama, A.; Reva, I.; Khokhlova, O.E.; Yabe, S.; Ozaki, K.; et al. A new local variant (ST764) of the globally disseminated ST5 lineage of hospital-associated methicillin-resistant Staphylococcus aureus (MRSA) carrying the virulence determinants of community-associated MRSA. Antimicrob. Agents Chemother. 2013, 57, 1589–1595. [Google Scholar] [CrossRef] [PubMed]
- Aung, M.S.; Kawaguchiya, M.; Urushibara, N.; Sumi, A.; Ito, M.; Kudo, K.; Morimoto, S.; Hosoya, S.; Kobayashi, N. Molecular characterization of methicillin-resistant Staphylococcus aureus from outpatients in Northern Japan: Increasing tendency of ST5/ST764 MRSA-IIa with arginine catabolic mobile element. Microb. Drug Resist. 2017, 23, 616–625. [Google Scholar] [CrossRef]
- Xiao, Y.; Han, W.; Wang, B.; Xu, Y.; Zhao, H.; Wang, X.; Rao, L.; Zhang, J.; Shen, L.; Zhou, H.; et al. Phylogenetic analysis and virulence characteristics of methicillin-resistant Staphylococcus aureus ST764-SCCmec II: An emerging hypervirulent clone ST764-t1084 in China. Emerg. Microbes Infect. 2023, 12, 2165969. [Google Scholar] [CrossRef]
- Kondo, S.; Phokhaphan, P.; Tongsima, S.; Ngamphiw, C.; Phornsiricharoenphant, W.; Ruangchai, W.; Disratthakit, A.; Tingpej, P.; Mahasirimongkol, S.; Lulitanond, A.; et al. Molecular characterization of methicillin-resistant Staphylococcus aureus genotype ST764-SCCmec type II in Thailand. Sci. Rep. 2022, 12, 2085. [Google Scholar] [CrossRef]
- Yamasaki, F.; Takeuchi, S.; Uehara, Y.; Matsushita, M.; Arise, K.; Morimoto, N.; Seo, H. Prevalence and characteristics of methicillin-resistant Staphylococcus aureus colonization among healthcare professionals in a university hospital in Japan. J. Gen. Fam. Med. 2019, 20, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Pitout, J.D.D.; Peirano, G.; Chen, L.; DeVinney, R.; Matsumura, Y. Escherichia coli ST1193: Following in the Footsteps of E. coli ST131. Antimicrob. Agents Chemother. 2022, 66, e0051122. [Google Scholar] [CrossRef]
- Gomes, D.J.; Bardossy, A.C.; Chen, L.; Forero, A.; Gorzalski, A.; Holmstadt, H.; Causey, K.; Njoku, C.; Stone, N.D.; Ogundimu, A.; et al. Transmission of novel Klebsiella pneumoniae carbapenemase-producing Escherichia coli sequence type 1193 among residents and caregivers in a community-based, residential care setting—Nevada, 2018. Infect. Control Hosp. Epidemiol. 2020, 41, 1341–1343. [Google Scholar] [CrossRef] [PubMed]
- Cherubini, S.; Perilli, M.; Azzini, A.M.; Tacconelli, E.; Maccacaro, L.; Bazaj, A.; Naso, L.; Amicosante, G.; LTCF-Veneto Working Group; Lo Cascio, G.; et al. Resistome and virulome of multi-drug resistant E. coli ST131 isolated from residents of long-term care facilities in the Northern Italian region. Diagnostics 2022, 12, 213. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, Y.; Sato, T.; Tsukamoto, N.; Nakajima, C.; Suzuki, Y.; Takahashi, S.; Yokota, S.-I. Clonal/subclonal changes and accumulation of CTX-M-type β-lactamase genes in fluoroquinolone-resistant Escherichia coli ST131 and ST1193 strains isolated during the past 12 years, Japan. J. Glob. Antimicrob. Resist. 2021, 27, 150–155. [Google Scholar] [CrossRef]
- Tchesnokova, V.L.; Rechkina, E.; Chan, D.; Haile, H.G.; Larson, L.; Ferrier, K.; Schroeder, D.W.; Solyanik, T.; Shibuya, S.; Hansen, K.; et al. pandemic uropathogenic fluoroquinolone-resistant Escherichia coli have enhanced ability to persist in the gut and cause bacteriuria in healthy women. Clin. Infect. Dis. 2020, 70, 937–939. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Noguchi, T.; Tanaka, M.; Kanahashi, T.; Yamamoto, M.; Nagao, M.; Takakura, S.; Ichiyama, S.; on behalf of the 89th JAID BRG. Population structure of Japanese extraintestinal pathogenic Escherichia coli and its relationship with antimicrobial resistance. J. Antimicrob. Chemother. 2017, 72, 1040–1049. [Google Scholar] [CrossRef] [PubMed]
- Tchesnokova, V.L.; Rechkina, E.; Larson, L.; Ferrier, K.; Weaver, J.L.; Schroeder, D.W.; She, R.; Butler-Wu, S.M.; Aguero-Rosenfeld, M.E.; Zerr, D.; et al. Rapid and Extensive Expansion in the United States of a New Multidrug-resistant Escherichia coli Clonal Group, Sequence Type 1193. Clin. Infect. Dis. 2019, 68, 334–337. [Google Scholar] [CrossRef]
- Holland, M.S.; Nobrega, D.; Peirano, G.; Naugler, C.; Church, D.L.; Pitout, J.D.D. Molecular epidemiology of Escherichia coli causing bloodstream infections in a centralized Canadian region: A population-based surveillance study. Clin. Microbiol. Infect. 2020, 26, 1554.e1–1554.e8. [Google Scholar] [CrossRef]
- Birgy, A.; Madhi, F.; Jung, C.; Levy, C.; Cointe, A.; Bidet, P.; Hobson, C.A.; Bechet, S.; Sobral, E.; Vuthien, H.; et al. Diversity and trends in population structure of ESBL-producing Enterobacteriaceae in febrile urinary tract infections in children in France from 2014 to 2017. J. Antimicrob. Chemother. 2020, 75, 96–105. [Google Scholar] [CrossRef]
- Ding, Y.; Zhang, J.; Yao, K.; Gao, W.; Wang, Y. Molecular characteristics of the new emerging global clone ST1193 among clinical isolates of Escherichia coli from neonatal invasive infections in China. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 833–840. [Google Scholar] [CrossRef]
- Archer, G.L. Staphylococcus aureus: A Well–Armed Pathogen. Clin. Infect. Dis. 1998, 26, 1179–1181. [Google Scholar] [CrossRef]
- Peng, H.L.; Novick, R.P.; Kreiswirth, B.; Kornblum, J.; Schlievert, P. Cloning, characterization, and sequencing of an accessory gene regulator (agr) in Staphylococcus aureus. J. Bacteriol. 1988, 170, 4365–4372. [Google Scholar] [CrossRef] [PubMed]
- Kwapisz, E.; Garbacz, K.; Kosecka-Strojek, M.; Schubert, J.; Bania, J.; Międzobrodzki, J. Presence of egc-positive major clones ST 45, 30 and 22 among methicillin-resistant and methicillin-susceptible oral Staphylococcus aureus strains. Sci. Rep. 2020, 10, 18889. [Google Scholar] [CrossRef] [PubMed]
- Aires de Sousa, M.; Bartzavali, C.; Spiliopoulou, I.; Sanches, I.S.; Crisóstomo, M.I.; de Lencastre, H. Two international methicillin-resistant Staphylococcus aureus clones endemic in a university hospital in Patras, Greece. J. Clin. Microbiol. 2003, 41, 2027–2032. [Google Scholar] [CrossRef] [PubMed]
- Neela, V.; Ehsanollah, G.R.; Zamberi, S.; Van Belkum, A.; Mariana, N.S. Prevalence of Panton–Valentine leukocidin genes among carriage and invasive Staphylococcus aureus isolates in Malaysia. Int. J. Infect. Dis. 2009, 13, e131–e132. [Google Scholar] [CrossRef]
- Prévost, G.; Cribier, B.; Couppié, P.; Petiau, P.; Supersac, G.; Finck-Barbançon, V.; Monteil, H.; Piemont, Y. Panton-Valentine leucocidin and gamma-hemolysin from Staphylococcus aureus ATCC 49775 are encoded by distinct genetic loci and have different biological activities. Infect. Immun. 1995, 63, 4121–4129. [Google Scholar] [CrossRef]
- Sdougkos, G.; Chini, V.; Papanastasiou, D.; Christodoulou, G.; Tagaris, G.; Dimitracopoulos, G.; Spiliopoulou, I. Methicillin-resistant Staphylococcus aureus producing Panton–Valentine leukocidin as a cause of acute osteomyelitis in children. Clin. Microbiol. Infect. 2007, 13, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Chini, V.; Petinaki, E.; Foka, A.; Paratiras, S.; Dimitracopoulos, G.; Spiliopoulou, I. Spread of Staphylococcus aureus clinical isolates carrying Panton–Valentine leukocidin genes during a 3-year period in Greece. Clin. Microbiol. Infect. 2006, 12, 29–34. [Google Scholar] [CrossRef]
- Bakthavatchalam, Y.D.; Nabarro, L.E.B.; Ralph, R.; Veeraraghavan, B. Diagnosis and management of Panton-Valentine leukocidin toxin associated Staphylococcus aureus infection: An update. Virulence 2007, 8, 1036. [Google Scholar] [CrossRef]
- Nhan, T.-X.; Leclercq, R.; Cattoir, V. Prevalence of toxin genes in consecutive clinical isolates of Staphylococcus aureus and clinical impact. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 719–725. [Google Scholar] [CrossRef]
- Vittorakis, E.; Vică, M.L.; Zervaki, C.O.; Vittorakis, E.; Maraki, S.; Mavromanolaki, V.E.; Schürger, M.E.; Neculicioiu, V.S.; Papadomanolaki, E.; Sinanis, T.; et al. Examining the prevalence and antimicrobial susceptibility of S. aureus Strains in hospitals: An analysis of the pvl gene and Its co-occurrence with other virulence factors. Microorganisms 2023, 11, 841. [Google Scholar] [CrossRef]
- Lopez-Aguilar, C.; Perez-Roth, E.; Moreno, A.; Duran, M.C.; Casanova, C.; Aguirre-Jaime, A.; Mendez-Alvarez, S. Association between the presence of the panton-valentine leukocidin-encoding gene and a lower rate of survival among hospitalized pulmonary patients with staphylococcal disease. J. Clin. Microbiol. 2007, 45, 274–276. [Google Scholar] [CrossRef] [PubMed]
- Víquez-Molina, G.; Aragón-Sánchez, J.; Pérez-Corrales, C.; Murillo-Vargas, C.; López-Valverde, M.E.; Lipsky, B.A. Virulence factor genes in Staphylococcus aureus isolated from diabetic foot soft tissue and bone infections. Int. J. Low. Extrem. Wounds 2018, 17, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Begier, E.; Rosenthal, N.A.; Gurtman, A.; Kartashov, A.; Donald, R.G.K.; Lockhart, S.P. Epidemiology of invasive Escherichia coli infection and antimicrobial resistance status among patients treated in US hospitals: 2009–2016. Clin. Infect. Dis. 2021, 73, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Sarshar, M.; Behzadi, P.; Ambrosi, C.; Zagaglia, C.; Palamara, A.T.; Scribano, D. FimH and anti-adhesive therapeutics: A disarming strategy against uropathogens. Antibiotics 2020, 9, 397. [Google Scholar] [CrossRef]
- Emódy, L.; Kerényi, M.; Nagy, G. Virulence factors of uropathogenic Escherichia coli. Int. J. Antimicrob. Agents 2003, 22, 29–33. [Google Scholar] [CrossRef]
- Yamamoto, S. Molecular epidemiology of uropathogenic Escherichia coli. J. Infect. Chemother. 2007, 13, 68–73. [Google Scholar] [CrossRef]
- Vieira, M.A.M. Pathogenicity islands. O Mundo Saúde 2009, 33, 406–414. [Google Scholar] [CrossRef]
- Wiles, T.J.; Kulesus, R.R.; Mulvey, M.A. Origins and virulence mechanisms of uropathogenic Escherichia coli. Exp. Mol. Pathol. 2008, 85, 11–19. [Google Scholar] [CrossRef]
- Kot, B. Antimicrobial Resistance Among Uropathogenic Escherichia coli. Pol. J. Microbiol. 2019, 68, 403–415. [Google Scholar] [CrossRef]
- Bielaszewska, M.; Schiller, R.; Lammers, L.; Bauwens, A.; Fruth, A.; Middendorf, B.; Schmidt, M.A.; Tarr, P.I.; Dobrindt, U.; Karch, H.; et al. Heteropathogenic virulence and phylogeny reveal phased pathogenic metamorphosis in Escherichia coli O2:H6. EMBO Mol. Med. 2014, 6, 347–357. [Google Scholar] [CrossRef]
- Firoozeh, F.; Saffari, M.; Neamati, F.; Zibaei, M. Detection of virulence genes in Escherichia coli isolated from patients with cystitis and pyelonephritis. Int. J. Infect. Dis. 2014, 29, 219–222. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, S.; Han, L.; Guo, X.; Chen, M.; Ni, Y.; Zhang, Y.; Cui, Z.; He, P. Drug resistance and virulence of uropathogenic Escherichia coli from Shanghai, China. J. Antibiot. 2014, 67, 799–805. [Google Scholar] [CrossRef]
- Bunduki, G.K.; Heinz, E.; Phiri, V.S.; Noah, P.; Feasey, N.; Musaya, J. Virulence factors and antimicrobial resistance of uropathogenic Escherichia coli (UPEC) isolated from urinary tract infections: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 753. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.R.; Kuskowski, M.A.; Gajewski, A.; Soto, S.; Horcajada, J.P.; de Anta, M.T.J.; Vila, J. Extended virulence genotypes and phylogenetic background of Escherichia coli isolates from patients with cystitis, pyelonephritis, or prostatitis. J. Infect. Dis. 2005, 191, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Kudinha, T.; Kong, F.; Johnson, J.R.; Andrew, S.D.; Anderson, P.; Gilbert, G.L. Multiplex PCR-based reverse line blot assay for simultaneous detection of 22 virulence genes in uropathogenic Escherichia coli. Appl. Environ. Microbiol. 2012, 78, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Calhau, V.; Domingues, S.; Ribeiro, G.; Mendonça, N.; Da Silva, G.J. Interplay between pathogenicity island carriage, resistance profile and plasmid acquisition in uropathogenic Escherichia coli. J. Med. Microbiol. 2015, 64, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.J.; Logue, C.M.; Johnson, J.R.; Kuskowski, M.A.; Sherwood, J.S.; Barnes, H.J.; DebRoy, C.; Wannemuehler, Y.M.; Obata-Yasuoka, M.; Spanjaard, L.; et al. Associations between multidrug resistance, plasmid content, and virulence potential among extraintestinal pathogenic and commensal Escherichia coli from humans and poultry. Foodborne Pathog. Dis. 2012, 9, 37–46. [Google Scholar] [CrossRef]
- Fonseca-Martínez, S.A.; Martínez-Vega, R.A.; Farfán-García, A.E.; González Rugeles, C.I.; Criado-Guerrero, L.Y. Association Between Uropathogenic Escherichia coli Virulence Genes and Severity of Infection and Resistance to Antimicrobials. Infect. Drug Resist. 2023, 16, 3707–3718. [Google Scholar] [CrossRef]
- Allami, M.; Bahreini, M.; Sharifmoghadam, M.R. Antimicrobial resistance, phylogenetic typing, and virulence genes profile analysis of uropathogenic Escherichia coli isolated from patients in southern Iraq. J. Appl. Genet. 2022, 63, 401–412. [Google Scholar] [CrossRef]
- Karam, M.R.A.; Habibi, M.; Bouzari, S. Relationships between virulence factors and antimicrobial resistance among Escherichia coli isolated from urinary tract infections and commensal isolates in Tehran, Iran. Osong Public Health Res. Perspect. 2018, 9, 217–224. [Google Scholar] [CrossRef]
- Lindberg, S.; Xia, Y.; Sondén, B.; Goransson, M.; Hacker, J.; Uhlin, B.E. Regulatory interactions among adhesin gene systems of uropathogenic Escherichia coli. Infect. Immun. 2008, 76, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Hagan, E.C.; Mobley, H.L.T. Uropathogenic Escherichia coli outer membrane antigens expressed during urinary tract infection. Infect. Immun. 2007, 75, 3941–3949. [Google Scholar] [CrossRef] [PubMed]
- Sarowska, J.; Futoma-Koloch, B.; Jama-Kmiecik, A.; Frej-Madrzak, M.; Ksiazczyk, M.; Bugla-Ploskonska, G.; Choroszy-Krol, I. Virulence factors, prevalence and potential transmission of extraintestinal pathogenic Escherichia coli isolated from different sources: Recent reports. Gut Pathog. 2019, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Lienard, A.; Hosny, M.; Jneid, J.; Schuldiner, S.; Cellier, N.; Sotto, A.; La Scola, B.; Lavigne, J.-P.; Pantel, A. Escherichia coli Isolated from Diabetic Foot Osteomyelitis: Clonal Diversity, Resistance Profile, Virulence Potential, and Genome Adaptation. Microorganisms 2021, 9, 380. [Google Scholar] [CrossRef] [PubMed]
- Crémet, L.; Broquet, A.; Brulin, B.; Jacqueline, C.; Dauvergne, S.; Brion, R.; Asehnoune, K.; Corvec, S.; Heymann, D.; Caroff, N. Pathogenic potential of Escherichia coli clinical strains from orthopedic implant infections towards human osteoblastic cells. Pathog. Dis. 2015, 73, ftv065. [Google Scholar] [CrossRef]
- PsycEXTRA Dataset [Internet]. 2004. Available online: https://psycnet.apa.org/buy/PE (accessed on 1 August 2023).
- Pantosti, A.; Sanchini, A.; Monaco, M. Mechanisms of antimicrobial resistance in Staphylococcus aureus. Futur. Microbiol. 2007, 2, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Diep, B.A.; Otto, M. The role of virulence determinants in community-associated MRSA pathogenesis. Trends Microbiol. 2008, 16, 361–369. [Google Scholar] [CrossRef]
- Peng, H.; Liu, D.; Ma, Y.; Gao, W. Comparison of community- and healthcare-associated methicillin-resistant Staphylococcus aureus isolates at a Chinese tertiary hospital, 2012–2017. Sci. Rep. 2018, 8, 17916. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Bao, Y.; Ouyang, N.; Dai, X.; Pan, K.; Chen, B.; Deng, Y.; Wu, X.; Xu, F.; Li, H.; et al. Molecular epidemiology and characteristic of virulence gene of community-acquired and hospital-acquired methicillin-resistant Staphylococcus aureus isolates in Sun Yat-sen Memorial hospital, Guangzhou, Southern China. BMC Infect. Dis. 2016, 16, 339. [Google Scholar] [CrossRef] [PubMed]
- Zeng, S.; Luo, J.; Chen, X.; Huang, L.; Wu, A.; Zhuo, C.; Li, X. Molecular Epidemiology and Characteristics of CTX-M-55 Extended-Spectrum β-Lactamase-Producing Escherichia coli From Guangzhou, China. Front. Microbiol. 2021, 12, 730012. [Google Scholar] [CrossRef] [PubMed]
- Chong, Y.; Ito, Y.; Kamimura, T. Genetic evolution and clinical impact in extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Infect. Genet. Evol. 2011, 11, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Bevan, E.R.; Jones, A.M.; Hawkey, P.M. Global epidemiology of CTX-M β-lactamases: Temporal and geographical shifts in genotype. J. Antimicrob. Chemother. 2017, 72, 2145–2155. [Google Scholar] [CrossRef]
- Zhang, J.; Zheng, B.; Zhao, L.; Wei, Z.; Ji, J.; Li, L.; Xiao, Y. Nationwide high prevalence of CTX-M and an increase of CTX-M-55 in Escherichia coli isolated from patients with community-onset infections in Chinese county hospitals. BMC Infect. Dis. 2014, 14, 659. [Google Scholar] [CrossRef] [PubMed]
- Kiratisin, P.; Apisarnthanarak, A.; Saifon, P.; Laesripa, C.; Kitphati, R.; Mundy, L.M. The emergence of a novel ceftazidime-resistant CTX-M extended-spectrum ß-lactamase, CTX-M-55, in both community-onset and hospital-acquired infections in Thailand. Diagn. Microbiol. Infect. Dis. 2007, 58, 349–355. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef]
- Lavery, L.A.; Armstrong, D.G.; Wunderlich, R.P.; Mohler, M.J.; Wendel, C.S.; Lipsky, B.A. Risk factors for foot infections in individuals with diabetes. Diabetes Care 2006, 29, 1288–1293. [Google Scholar] [CrossRef]
- Lavery, L.A.; Peters, E.J.; Armstrong, D.G.; Wendel, C.S.; Murdoch, D.P.; Lipsky, B.A. Risk factors for developing osteomyelitis in patients with diabetic foot wounds. Diabetes Res. Clin. Pract. 2009, 83, 347–352. [Google Scholar] [CrossRef]
- Peters, E.J.; Lavery, L.A.; Armstrong, D.G. Diabetic lower extremity infection: Influence of physical, psychological, and social factors. J. Diabetes Complicat. 2005, 19, 107–112. [Google Scholar] [CrossRef] [PubMed]
- George, R.K.; Verma, A.K.; Agarwal, A.; Agarwal, G.; Mishra, S.K. An audit of foot infections in patients with diabetes mellitus following renal transplantation. Int. J. Low. Extrem. Wounds 2004, 3, 157–160. [Google Scholar] [CrossRef]
- Dörr, S.; Holland-Letz, A.-K.; Weisser, G.; Chatzitomaris, A.; Lobmann, R. Bacterial Diversity, Antimicrobial Resistance, and the Risk of Lower Limb Amputation in Younger and Older Individuals with Diabetic Foot Infection. Int. J. Low. Extrem. Wounds 2021, 22, 63–71. [Google Scholar] [CrossRef]
- Du, F.; Ma, J.; Gong, H.; Bista, R.; Zha, P.; Ren, Y.; Gao, Y.; Chen, D.; Ran, X.; Wang, C. Microbial infection and antimicrobial susceptibility of diabetic foot ulcer in china: Literature review. Front. Endocrinol. 2022, 13, 881659. [Google Scholar] [CrossRef] [PubMed]
- Mutluoglu, M.; Sivrioglu, A.K.; Eroglu, M.; Uzun, G.; Turhan, V.; Ay, H.; Lipsky, B.A. The implications of the presence of osteomyelitis on outcomes of infected diabetic foot wounds. Scand. J. Infect. Dis. 2013, 45, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.T.; Armstrong, D.G. Microbiology and antimicrobial therapy for diabetic foot infections. Infect. Chemother. 2018, 50, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. Antimicrobial Resistance Threats in the United States; Department of Health and Human Services: Washington, DC, USA, 2019; pp. 1–140. [CrossRef]
- Sidjabat, H.E.; Silveira, F.P.; Potoski, B.A.; Abu-Elmagd, K.M.; Adams-Haduch, J.M.; Paterson, D.L.; Doi, Y. Interspecies Spread of Klebsiella pneumoniae Carbapenemase Gene in a Single Patient. Clin. Infect. Dis. 2009, 49, 1736–1738. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, N.; Nakanouchi, J.; Yüzen, D.I.; Fung, S.; Fernandez, J.S.; Barberis, C.; Tuchscherr, L.; Ramirez, M.S. A Study on Acinetobacter baumannii and Staphylococcus aureus Strains Recovered from the Same Infection Site of a Diabetic Patient. Curr. Microbiol. 2019, 76, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Shettigar, K.; Jain, S.; Bhat, D.V.; Acharya, R.; Ramachandra, L.; Satyamoorthy, K.; Murali, T.S. Virulence determinants in clinical Staphylococcus aureus from monomicrobial and polymicrobial infections of diabetic foot ulcers. J. Med. Microbiol. 2016, 65, 1392–1404. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Mitov, I. Antimicrobial resistance rates in causative agents of infections in diabetic patients: Rising concerns. Expert Rev. Anti-Infect. Ther. 2013, 11, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Bansal, E.; Garg, A.; Bhatia, S.; Attri, A.; Chander, J. Spectrum of microbial flora in diabetic foot ulcers. Indian J. Pathol. Microbiol. 2008, 51, 204–208. [Google Scholar] [CrossRef]
- Boschetti, G.; Sgarabotto, D.; Meloni, M.; Bruseghin, M.; Whisstock, C.; Marin, M.; Ninkovic, S.; Pinfi, M.; Brocco, E. Antimicrobial Resistance Patterns in Diabetic Foot Infections, an Epidemiological Study in Northeastern Italy. Antibiotics 2021, 10, 1241. [Google Scholar] [CrossRef] [PubMed]
- Gardner, S.E.; Hillis, S.L.; Heilmann, K.; Segre, J.A.; Grice, E.A. The Neuropathic Diabetic Foot Ulcer Microbiome Is Associated with Clinical Factors. Diabetes 2013, 62, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Kandemir, O.; Akbay, E.; Şahin, E.; Milcan, A.; Gen, R. Risk factors for infection of the diabetic foot with multi-AMR microorganisms. J. Infect. 2007, 54, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A. Bone of Contention: Diagnosing Diabetic Foot Osteomyelitis. Clin. Infect. Dis. 2008, 47, 528–530. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; LeFrock, J.L.; Lew, D.P.; Mader, J.T.; Norden, C.; et al. Diagnosis and Treatment of Diabetic Foot Infections. Clin. Infect. Dis. 2004, 39, 885–910. [Google Scholar] [CrossRef] [PubMed]
- Lazaro-Martinez, J.L.; Tardaguila-Garcia, A.; Garcia-Klepzig, J.L. Diagnostic and therapeutic update on diabetic foot osteomyelitis. Endocrinol. Diabetes Nutr. 2017, 64, 100–108. [Google Scholar] [CrossRef] [PubMed]
- King, C.M.; Castellucci-Garza, F.M.; Lyon, L.; Doyle, M.D.; Nimick, C.; Williams, M.L.; Ryan, E.C.; Crisologo, P.A.; La Fontaine, J.; Wukich, D.K.; et al. Microorganisms Associated with Osteomyelitis of the Foot and Ankle. J. Foot Ankle Surg. 2020, 59, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Lindbloom, B.J.; James, E.R.; McGarvey, W.C. Osteomyelitis of the Foot and Ankle: Diagnosis, epidemiology, and treatment. Foot Ankle Clin. 2014, 19, 569–588. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Senneville, É.; Abbas, Z.G.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes/Metab. Res. Rev. 2020, 36, e3280. [Google Scholar] [CrossRef] [PubMed]
- Jaroenarpornwatana, A.; Koonalinthip, N.; Chawaltanpipat, S.; Janchai, S. Is the duration of diabetic foot ulcers an independent risk factor for developing diabetic foot osteomyelitis? Foot 2023, 56, 102000. [Google Scholar] [CrossRef] [PubMed]
- Reina-Bueno, M.; Palomo-Toucedo, I.C.; Castro-Méndez, A.; Domínguez-Maldonado, G.; Vázquez-Bautista, M.D.C. Methicillin-resistant Staphylococcus aureus diabetic foot crossed infection: A case report. Pathogens 2020, 9, 549. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitaya, S.; Miura, C.; Suzuki, A.; Imai, Y.; Tokuda, K.; Kanamori, H. Diabetic Foot Osteomyelitis Caused by Co-Infection with Methicillin-Resistant Staphylococcus aureus and Multidrug-Resistant Extended-Spectrum ß-Lactamase-Producing Escherichia coli: A Case Report. Appl. Microbiol. 2023, 3, 1046-1056. https://doi.org/10.3390/applmicrobiol3030072
Kitaya S, Miura C, Suzuki A, Imai Y, Tokuda K, Kanamori H. Diabetic Foot Osteomyelitis Caused by Co-Infection with Methicillin-Resistant Staphylococcus aureus and Multidrug-Resistant Extended-Spectrum ß-Lactamase-Producing Escherichia coli: A Case Report. Applied Microbiology. 2023; 3(3):1046-1056. https://doi.org/10.3390/applmicrobiol3030072
Chicago/Turabian StyleKitaya, Shiori, Chieko Miura, Ayano Suzuki, Yoshimichi Imai, Koichi Tokuda, and Hajime Kanamori. 2023. "Diabetic Foot Osteomyelitis Caused by Co-Infection with Methicillin-Resistant Staphylococcus aureus and Multidrug-Resistant Extended-Spectrum ß-Lactamase-Producing Escherichia coli: A Case Report" Applied Microbiology 3, no. 3: 1046-1056. https://doi.org/10.3390/applmicrobiol3030072
APA StyleKitaya, S., Miura, C., Suzuki, A., Imai, Y., Tokuda, K., & Kanamori, H. (2023). Diabetic Foot Osteomyelitis Caused by Co-Infection with Methicillin-Resistant Staphylococcus aureus and Multidrug-Resistant Extended-Spectrum ß-Lactamase-Producing Escherichia coli: A Case Report. Applied Microbiology, 3(3), 1046-1056. https://doi.org/10.3390/applmicrobiol3030072