
Brought to Light: How Ultraviolet Disinfection Can Prevent the Nosocomial Transmission of COVID-19 and Other Infectious Diseases


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
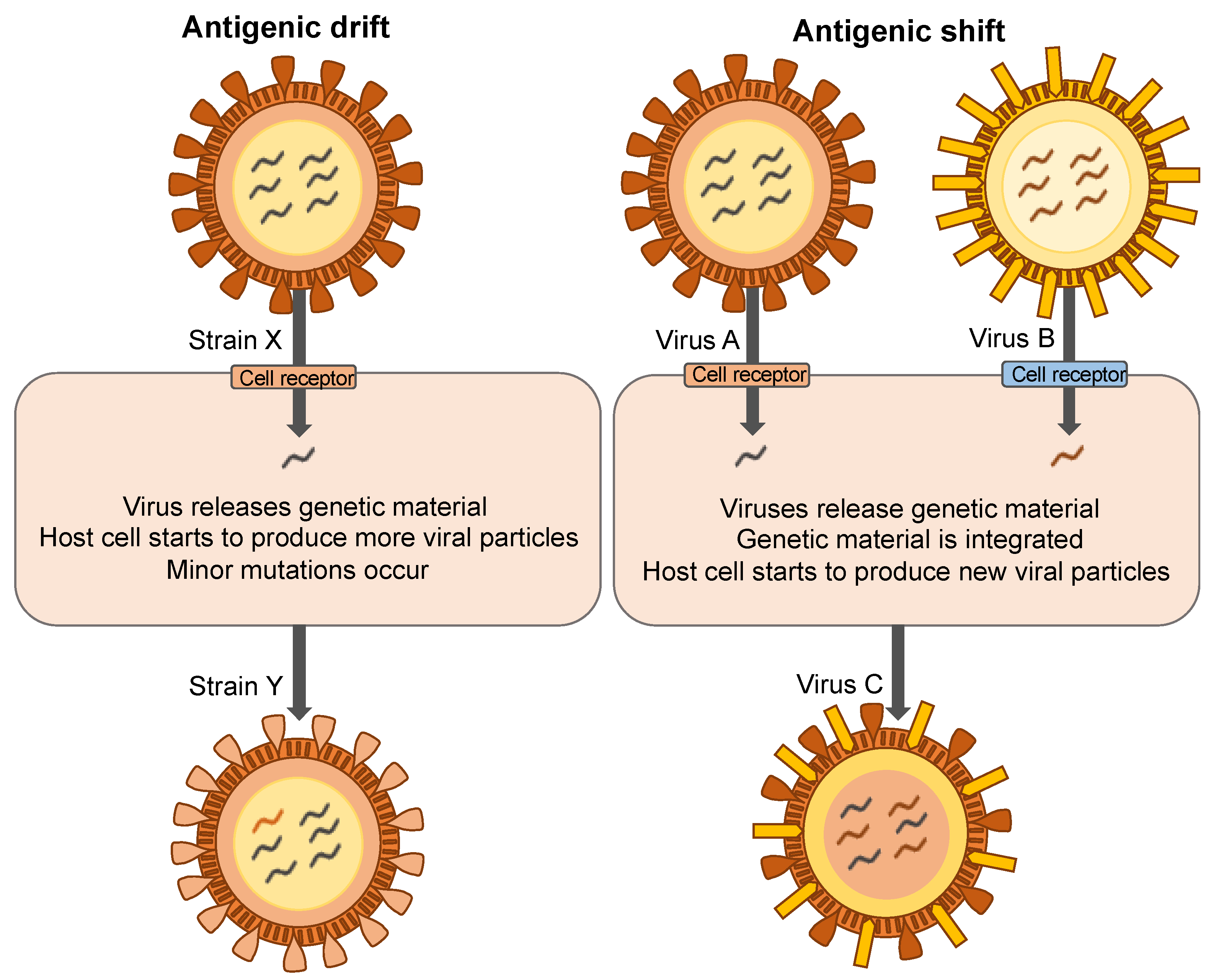
1.1. Mechanisms of Viral Mutation
1.2. Mechanisms of Antibiotic Resistance
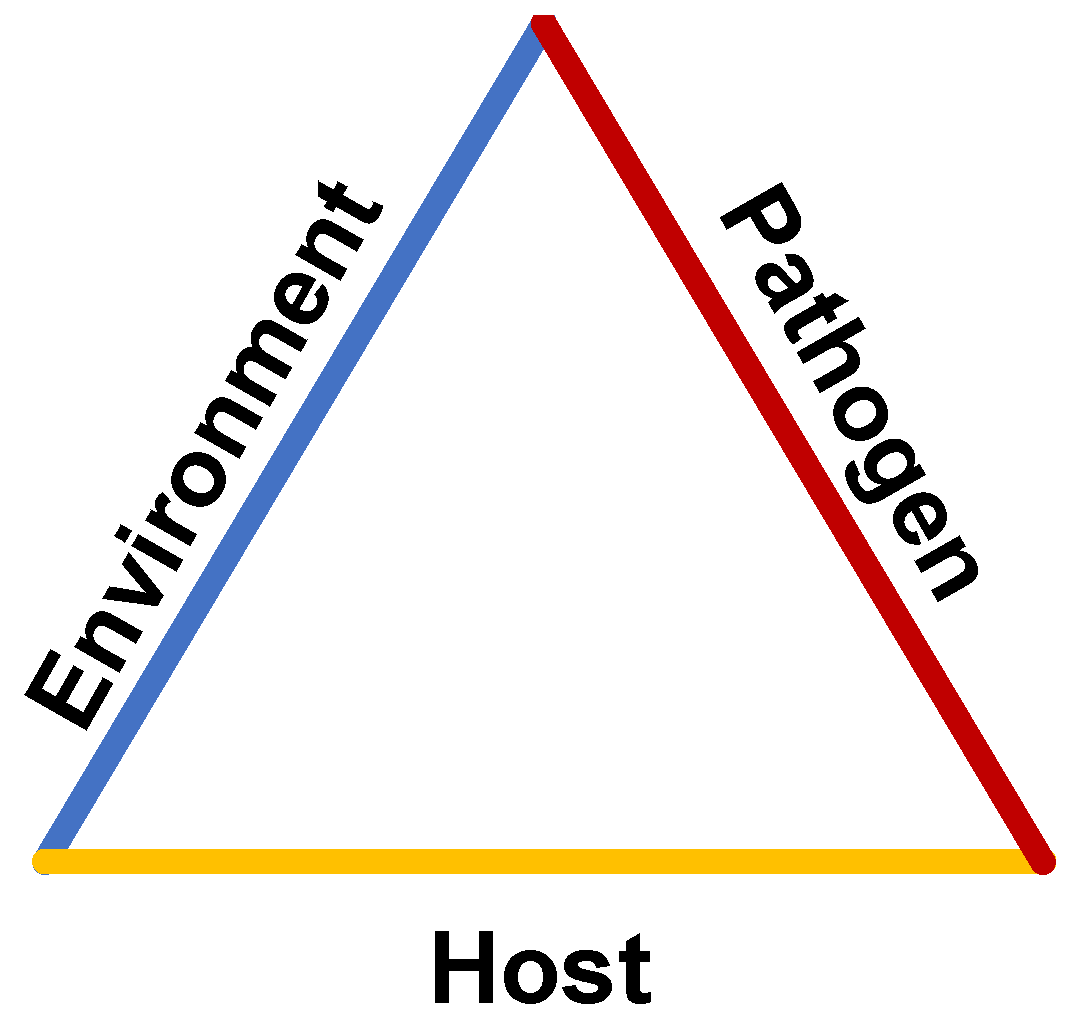
1.3. Disease Transmission in Healthcare Facilities
1.4. Current Approach to Infection Control
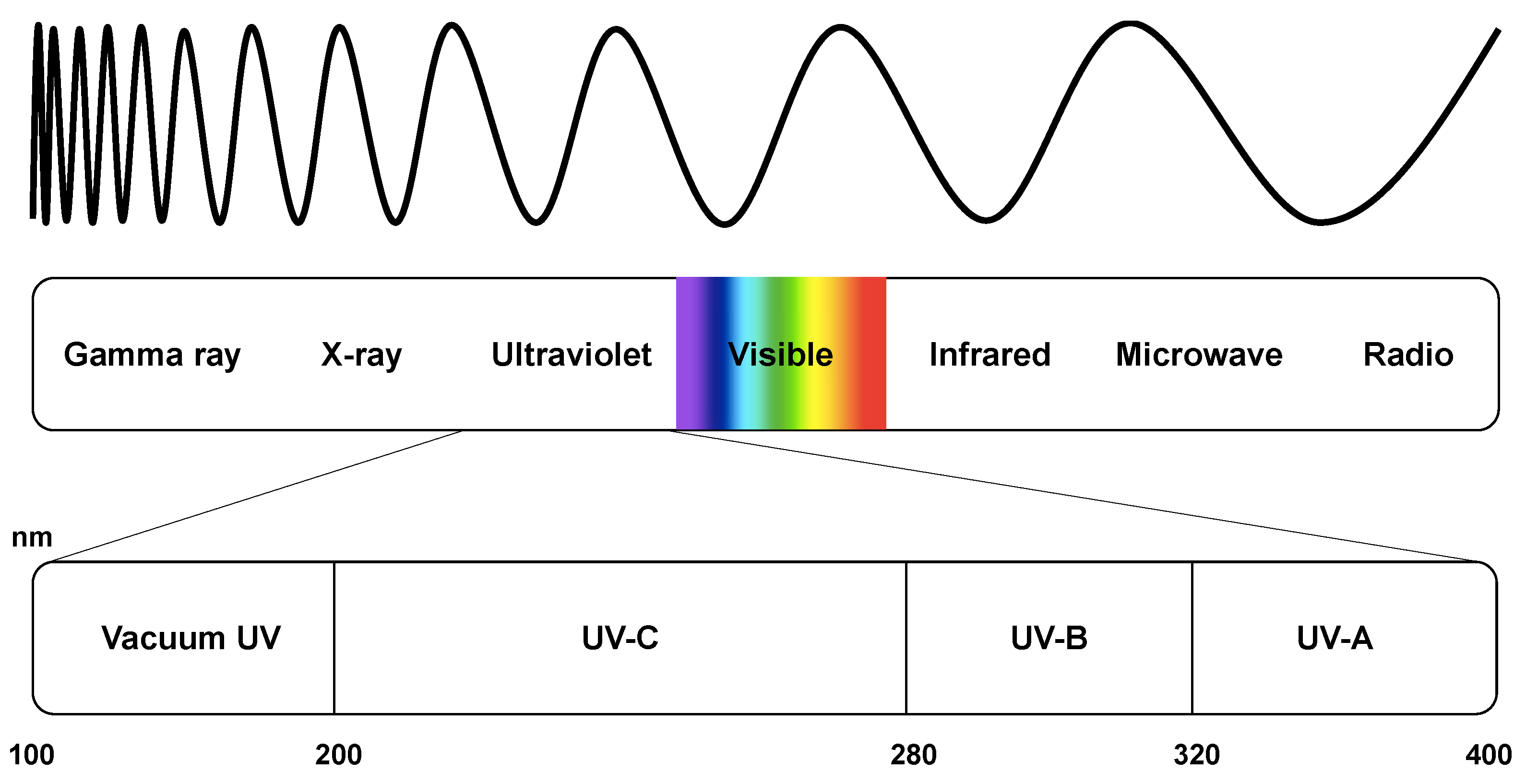
2. Ultraviolet Germicidal Irradiation
2.1. Ultraviolet Disinfection History
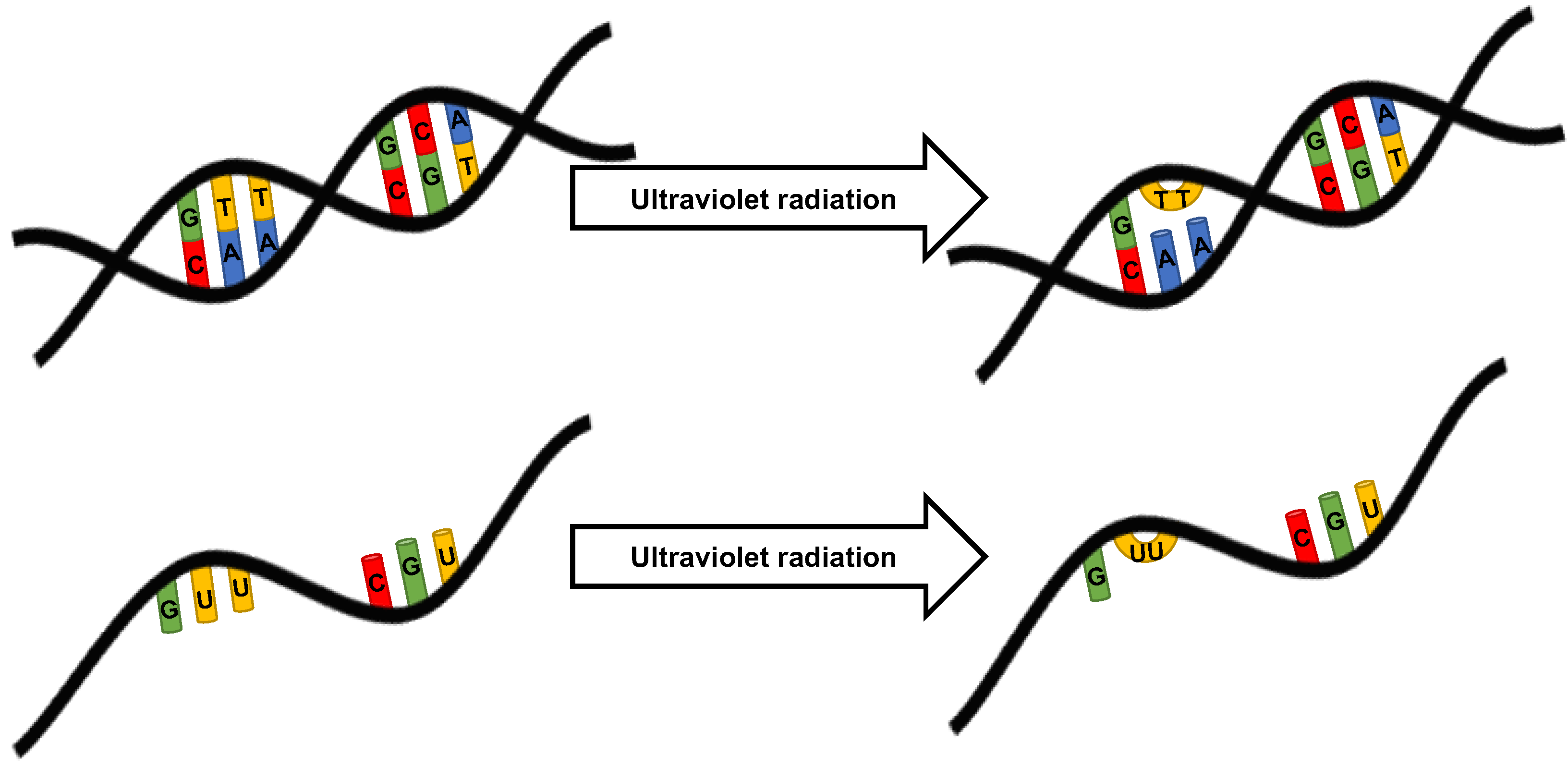
2.2. Mechanism of UV Microbial Inactivation
2.3. Clinical Applicability of Ultraviolet Disinfection
2.4. Activity of UVC against Clinical Pathogens
3. Airborne Transmission of Pathogens
3.1. UV Disinfection of Air
3.2. Upper Room UV Systems
4. Surface Transmission of Pathogens
4.1. UV Disinfection of Non-Porous Surfaces
4.2. UV Disinfection of Porous Materials
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Russo, P.L.; Stewardson, A.J.; Cheng, A.C.; Bucknall, T.; Mitchell, B.G. The Prevalence of Healthcare Associated Infections among Adult Inpatients at Nineteen Large Australian Acute-Care Public Hospitals: A Point Prevalence Survey. Antimicrob. Resist. Infect. Control 2019, 8, 114. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate Point-Prevalence Survey of Health Care-Associated Infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Douglas, S. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention; National Center for Preparedness, Detection, and Control of Infectious Diseases: Atlanta, GA, USA, 2009.
- Browne, K.; Chakraborty, S.; Chen, R.; Willcox, M.D.; Black, D.S.; Walsh, W.R.; Kumar, N. A New Era of Antibiotics: The Clinical Potential of Antimicrobial Peptides. Int. J. Mol. Sci. 2020, 21, 7047. [Google Scholar] [CrossRef]
- Kramer, A.; Schwebke, I.; Kampf, G. How Long Do Nosocomial Pathogens Persist on Inanimate Surfaces? A Systematic Review. BMC Infect. Dis. 2006, 6, 130. [Google Scholar] [CrossRef]
- Blanco, N.; O’Hara, L.M.; Harris, A.D. Transmission Pathways of Multidrug-Resistant Organisms in the Hospital Setting: A Scoping Review. Infect. Control Hosp. Epidemiol. 2019, 40, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Carling, P.C.; Parry, M.F.; Bruno-Murtha, L.A.; Dick, B. Improving Environmental Hygiene in 27 Intensive Care Units to Decrease Multidrug-Resistant Bacterial Transmission. Crit. Care Med. 2010, 38, 1054–1059. [Google Scholar] [CrossRef]
- Carling, P.C.; Parry, M.M.; Rupp, M.E.; Po, J.L.; Dick, B.; Von Beheren, S. Healthcare Environmental Hygiene Study Group Improving Cleaning of the Environment Surrounding Patients in 36 Acute Care Hospitals. Infect. Control Hosp. Epidemiol. 2008, 29, 1035–1041. [Google Scholar] [CrossRef]
- Cohen, B.; Liu, J.; Cohen, A.R.; Larson, E. Association Between Healthcare-Associated Infection and Exposure to Hospital Roommates and Previous Bed Occupants with the Same Organism. Infect. Control Hosp. Epidemiol. 2018, 39, 541–546. [Google Scholar] [CrossRef]
- Goodman, E.R.; Platt, R.; Bass, R.; Onderdonk, A.B.; Yokoe, D.S.; Huang, S.S. Impact of an Environmental Cleaning Intervention on the Presence of Methicillin-Resistant Staphylococcus Aureus and Vancomycin-Resistant Enterococci on Surfaces in Intensive Care Unit Rooms. Infect. Control Hosp. Epidemiol. 2008, 29, 593–599. [Google Scholar] [CrossRef]
- Hayden, M.K.; Bonten, M.J.M.; Blom, D.W.; Lyle, E.A.; van de Vijver, D.A.M.C.; Weinstein, R.A. Reduction in Acquisition of Vancomycin-Resistant Enterococcus after Enforcement of Routine Environmental Cleaning Measures. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2006, 42, 1552–1560. [Google Scholar] [CrossRef]
- Everett, B.R.; Sitton, J.T.; Wilson, M. Efficacy and Cost-Benefit Analysis of a Global Environmental Cleaning Algorithm on Hospital-Acquired Infection Rates. J. Patient Saf. 2017, 13, 207–210. [Google Scholar] [CrossRef]
- Honigsbaum, M. Pandemic. Lancet 2009, 373, 1939. [Google Scholar] [CrossRef]
- Mercatelli, D.; Giorgi, F.M. Geographic and Genomic Distribution of SARS-CoV-2 Mutations. Front. Microbiol. 2020, 11, 1800. [Google Scholar] [CrossRef]
- Anand, S.; Chen, Y.; Prévost, J.; Gasser, R.; Beaudoin-Bussières, G.; Abrams, C.; Pazgier, M.; Finzi, A. Interaction of Human ACE2 to Membrane-Bound SARS-CoV-1 and SARS-CoV-2 S Glycoproteins. Viruses 2020, 12, 1104. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Y.; Wu, L.; Niu, S.; Song, C.; Zhang, Z.; Lu, G.; Qiao, C.; Hu, Y.; Yuen, K.-Y.; et al. Structural and Functional Basis of SARS-CoV-2 Entry by Using Human ACE2. Cell 2020, 181, 894–904.e9. [Google Scholar] [CrossRef]
- Peng, R.; Wu, L.-A.; Wang, Q.; Qi, J.; Gao, G.F. Cell Entry by SARS-CoV-2. Trends Biochem. Sci. 2021, 46, 848–860. [Google Scholar] [CrossRef] [PubMed]
- Alizon, S.; Haim-Boukobza, S.; Foulongne, V.; Verdurme, L.; Trombert-Paolantoni, S.; Lecorche, E.; Roquebert, B.; Sofonea, M.T. Rapid Spread of the SARS-CoV-2 Delta Variant in Some French Regions, June 2021. Eurosurveillance 2021, 26, 2100573. [Google Scholar] [CrossRef]
- Khateeb, J.; Li, Y.; Zhang, H. Emerging SARS-CoV-2 Variants of Concern and Potential Intervention Approaches. Crit. Care 2021, 25, 244. [Google Scholar] [CrossRef]
- Zhang, Z.; Zheng, Y.; Niu, Z.; Zhang, B.; Wang, C.; Yao, X.; Peng, H.; Franca, D.N.; Wang, Y.; Zhu, Y.; et al. SARS-CoV-2 Spike Protein Dictates Syncytium-Mediated Lymphocyte Elimination. Cell Death Differ. 2021, 28, 2765–2777. [Google Scholar] [CrossRef]
- Ozono, S.; Zhang, Y.; Ode, H.; Sano, K.; Tan, T.S.; Imai, K.; Miyoshi, K.; Kishigami, S.; Ueno, T.; Iwatani, Y.; et al. SARS-CoV-2 D614G Spike Mutation Increases Entry Efficiency with Enhanced ACE2-Binding Affinity. Nat. Commun. 2021, 12, 848. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Rella, S.A.; Kulikova, Y.A.; Dermitzakis, E.T.; Kondrashov, F.A. Rates of SARS-CoV-2 Transmission and Vaccination Impact the Fate of Vaccine-Resistant Strains. Sci. Rep. 2021, 11, 15729. [Google Scholar] [CrossRef]
- Rezasoltani, S.; Yadegar, A.; Hatami, B.; Asadzadeh Aghdaei, H.; Zali, M.R. Antimicrobial Resistance as a Hidden Menace Lurking Behind the COVID-19 Outbreak: The Global Impacts of Too Much Hygiene on AMR. Front. Microbiol. 2020, 11, 590683. [Google Scholar] [CrossRef]
- Founou, R.C.; Blocker, A.J.; Noubom, M.; Tsayem, C.; Choukem, S.P.; Dongen, M.V.; Founou, L.L. The COVID-19 Pandemic: A Threat to Antimicrobial Resistance Containment. Future Sci. OA 2021, 7, FSO736. [Google Scholar] [CrossRef] [PubMed]
- Manesh, A.; Varghese, G.M. Rising Antimicrobial Resistance: An Evolving Epidemic in a Pandemic. Lancet Microbe 2021, 2, e419–e420. [Google Scholar] [CrossRef]
- Knight, G.M.; Glover, R.E.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E.; et al. Antimicrobial Resistance and COVID-19: Intersections and Implications. eLife 2021, 10, e64139. [Google Scholar] [CrossRef]
- Mahoney, A.R.; Safaee, M.M.; Wuest, W.M.; Furst, A.L. The Silent Pandemic: Emergent Antibiotic Resistances Following the Global Response to SARS-CoV-2. iScience 2021, 24, 102304. [Google Scholar] [CrossRef]
- Teillant, A.; Gandra, S.; Barter, D.; Morgan, D.J.; Laxminarayan, R. Potential Burden of Antibiotic Resistance on Surgery and Cancer Chemotherapy Antibiotic Prophylaxis in the USA: A Literature Review and Modelling Study. Lancet Infect. Dis. 2015, 15, 1429–1437. [Google Scholar] [CrossRef]
- Smith, R.; Coast, J. The True Cost of Antimicrobial Resistance. BMJ 2013, 346, f1493. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care (ACSQHC). AURA 2019: Third Australian Report on Antimicrobial Use and Resistance in Human Health; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2019; ISBN 978-1-925948-00-4.
- Kussell, E.; Kishony, R.; Balaban, N.Q.; Leibler, S. Bacterial Persistence. Genetics 2005, 169, 1807–1814. [Google Scholar] [CrossRef]
- Langsrud, S.; Sundheim, G.; Borgmann-Strahsen, R. Intrinsic and Acquired Resistance to Quaternary Ammonium Compounds in Food-Related Pseudomonas Spp. J. Appl. Microbiol. 2003, 95, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.S. Disinfectant Resistance Mechanisms, Cross-Resistance, and Co-Resistance. Int. Biodeterior. Biodegrad. 2003, 51, 271–276. [Google Scholar] [CrossRef]
- Hong, Y.; Teska, P.J.; Oliver, H.F. Effects of Contact Time and Concentration on Bactericidal Efficacy of 3 Disinfectants on Hard Nonporous Surfaces. Am. J. Infect. Control 2017, 45, 1284–1285. [Google Scholar] [CrossRef]
- Russell, A.D. Bacterial Resistance to Disinfectants: Present Knowledge and Future Problems. J. Hosp. Infect. 1999, 43, S57–S68. [Google Scholar] [CrossRef]
- Han, J.H.; Sullivan, N.; Leas, B.F.; Pegues, D.A.; Kaczmarek, J.L.; Umscheid, C.A. Cleaning Hospital Room Surfaces to Prevent Health Care—Associated Infections. Ann. Intern. Med. 2015, 163, 598–607. [Google Scholar] [CrossRef]
- Plowman, R. The Socioeconomic Burden of Hospital Acquired Infection. Eurosurveillance 2000, 5, 49–50. [Google Scholar] [CrossRef]
- McGregor, J.C.; Perencevich, E.N.; Furuno, J.P.; Langenberg, P.; Flannery, K.; Zhu, J.; Fink, J.C.; Bradham, D.D.; Harris, A.D. Comorbidity Risk-Adjustment Measures Were Developed and Validated for Studies of Antibiotic-Resistant Infections. J. Clin. Epidemiol. 2006, 59, 1266–1273. [Google Scholar] [CrossRef]
- Allegranzi, B.; Pittet, D. Role of Hand Hygiene in Healthcare-Associated Infection Prevention. J. Hosp. Infect. 2009, 73, 305–315. [Google Scholar] [CrossRef]
- Assadian, O.; Harbarth, S.; Vos, M.; Knobloch, J.K.; Asensio, A.; Widmer, A.F. Practical Recommendations for Routine Cleaning and Disinfection Procedures in Healthcare Institutions: A Narrative Review. J. Hosp. Infect. 2021, 113, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.; Todi, S.; Myatra, S.N.; Samaddar, D.P. Guidelines for Prevention of Hospital Acquired Infections. Indian J. Crit. Care Med. 2014, 18, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Schorderet-Weber, S.; Noack, S.; Selzer, P.M.; Kaminsky, R. Blocking Transmission of Vector-Borne Diseases. Int. J. Parasitol. Drugs Drug Resist. 2017, 7, 90–109. [Google Scholar] [CrossRef] [PubMed]
- Suleyman, G.; Alangaden, G.; Bardossy, A.C. The Role of Environmental Contamination in the Transmission of Nosocomial Pathogens and Healthcare-Associated Infections. Curr. Infect. Dis. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Dancer, S.J. Controlling Hospital-Acquired Infection: Focus on the Role of the Environment and New Technologies for Decontamination. Clin. Microbiol. Rev. 2014, 27, 665–690. [Google Scholar] [CrossRef]
- Doll, M.; Stevens, M.; Bearman, G. Environmental Cleaning and Disinfection of Patient Areas. Int. J. Infect. Dis. 2018, 67, 52–57. [Google Scholar] [CrossRef]
- Cook, T.M.; Piatt, C.J.; Barnes, S.; Edmiston, C.E. The Impact of Supplemental Intraoperative Air Decontamination on the Outcome of Total Joint Arthroplasty: A Pilot Analysis. J. Arthroplasty 2019, 34, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Klompas, M. Coronavirus Disease 2019 (COVID-19): Protecting Hospitals From the Invisible. Ann. Intern. Med. 2020, 172, 619–620. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among Front-Line Health-Care Workers and the General Community: A Prospective Cohort Study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Quigley, A.L.; Stone, H.; Nguyen, P.Y.; Chughtai, A.A.; MacIntyre, C.R. Estimating the Burden of COVID-19 on the Australian Healthcare Workers and Health System during the First Six Months of the Pandemic. Int. J. Nurs. Stud. 2021, 114, 103811. [Google Scholar] [CrossRef] [PubMed]
- Ueki, H.; Furusawa, Y.; Iwatsuki-Horimoto, K.; Imai, M.; Kabata, H.; Nishimura, H.; Kawaoka, Y. Effectiveness of Face Masks in Preventing Airborne Transmission of SARS-CoV-2. mSphere 2020, 5, e00637-20. [Google Scholar] [CrossRef]
- World Health Organization, Regional Office for Europe. Infection Prevention and Control: Guidance to Action Tools; World Health Organization, Regional Office for Europe: København, Denmark, 2021; ISBN 978-92-890-5543-7. [Google Scholar]
- Jefferson, T.; Del Mar, C.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Bawazeer, G.A.; van Driel, M.L.; Foxlee, R.; Rivetti, A. Physical Interventions to Interrupt or Reduce the Spread of Respiratory Viruses: Systematic Review. BMJ 2009, 339, b3675. [Google Scholar] [CrossRef]
- Chou, D.T.S.; Achan, P.; Ramachandran, M. The World Health Organization ‘5 Moments of Hand Hygiene’. J. Bone Joint Surg. Br. 2012, 94-B, 441–445. [Google Scholar] [CrossRef]
- Gordin, F.M.; Schultz, M.E.; Huber, R.A.; Gill, J.A. Reduction in Nosocomial Transmission of Drug-Resistant Bacteria After Introduction of an Alcohol-Based Handrub. Infect. Control Hosp. Epidemiol. 2005, 26, 650–653. [Google Scholar] [CrossRef] [PubMed]
- Kampiatu, P.; Cozean, J. A Controlled, Crossover Study of a Persistent Antiseptic to Reduce Hospital-Acquired Infection. Afr. J. Infect. Dis. 2015, 9, 6–9. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Son, C.; Chuck, T.; Childers, T.; Usiak, S.; Dowling, M.; Andiel, C.; Backer, R.; Eagan, J.; Sepkowitz, K. Practically Speaking: Rethinking Hand Hygiene Improvement Programs in Health Care Settings. Am. J. Infect. Control 2011, 39, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Pittet, D. Improving Adherence to Hand Hygiene Practice: A Multidisciplinary Approach. Emerg. Infect. Dis. 2001, 7, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Duckro, A.N.; Blom, D.W.; Lyle, E.A.; Weinstein, R.A.; Hayden, M.K. Transfer of Vancomycin-Resistant Enterococci via Health Care Worker Hands. Arch. Intern. Med. 2005, 165, 302–307. [Google Scholar] [CrossRef]
- Dancer, S.J. Hospital Cleaning in the 21st Century. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1473–1481. [Google Scholar] [CrossRef]
- WHO. Use of Disinfectants: Alcohol and Bleach; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Fischer, R.J.; Morris, D.H.; van Doremalen, N.; Sarchette, S.; Matson, M.J.; Bushmaker, T.; Yinda, C.K.; Seifert, S.N.; Gamble, A.; Williamson, B.N.; et al. Effectiveness of N95 Respirator Decontamination and Reuse against SARS-CoV-2 Virus. Emerg. Infect. Dis. 2020, 26, 2253–2255. [Google Scholar] [CrossRef]
- Dick, A.W.; Perencevich, E.N.; Pogorzelska-Maziarz, M.; Zwanziger, J.; Larson, E.L.; Stone, P.W. A Decade of Investment in Infection Prevention: A Cost-Effectiveness Analysis. Am. J. Infect. Control 2015, 43, 4–9. [Google Scholar] [CrossRef]
- Kowalski, W.J. Ultraviolet Germicidal Irradiation Handbook: UVGI for Air and Surface Disinfection; Springer: New York, NY, USA, 2009; ISBN 978-3-642-01998-2. [Google Scholar]
- Downes, A.; Blunt, T.P. The Influence of Light upon the Development of Bacteria 1. Nature 1877, 16, 218. [Google Scholar] [CrossRef]
- Ward, H.M.V. Experiments on the Action of Light on Bacillus Anthracis. Proc. R. Soc. Lond. 1893, 52, 393–400. [Google Scholar] [CrossRef]
- Gates, F.L. A study of the bactericidal action of ultra violet light. J. Gen. Physiol. 1930, 14, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Reed, N.G. The History of Ultraviolet Germicidal Irradiation for Air Disinfection. Public Health Rep. 2010, 125, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Hollaender, A.; Emmons, C.W. Wavelength dependence of mutation production in the ultraviolet with special emphasis on fungi. Cold Spring Harb. Symp. Quant. Biol. 1941, 9, 179–186. [Google Scholar] [CrossRef]
- Bolton, J.; Bertrand, D.; Zia, B.; Hargey, T.; Clancy, J. Inactivation of Cryptosporidium Parvum by Medium-Pressure Ultraviolet Light in Finished Drinking Water. In Proceedings of the AWWA 1998 Annual Conference, Dallas, TX, USA, 21–24 June 1998; Volume A, pp. 389–403. [Google Scholar]
- Clancy, J.L.; Bukhari, Z.; Hargy, T.M.; Bolton, J.R.; Dussert, B.W.; Marshall, M.M. Using UV to Inactivate Cryptosporidium. J. Am. Water Works Assoc. 2000, 92, 97–104. [Google Scholar] [CrossRef]
- Zhao, H.; Traganos, F.; Darzynkiewicz, Z. Kinetics of the UV-Induced DNA Damage Response in Relation to Cell Cycle Phase. Correlation with DNA Replication. Cytom. Part J. Int. Soc. Anal. Cytol. 2010, 77, 285–293. [Google Scholar] [CrossRef]
- Rothman, R.H.; Setlow, R.B. An action spectrum for cell killing and pyrimidine dimer formation in chinese hamster V-79 cells. Photochem. Photobiol. 1979, 29, 57–61. [Google Scholar] [CrossRef]
- Sinha, R.P.; Häder, D.P. UV-Induced DNA Damage and Repair: A Review. Photochem. Photobiol. Sci. Off. J. Eur. Photochem. Assoc. Eur. Soc. Photobiol. 2002, 1, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.L.; Plagemann, P.G.W. Effect of Ultraviolet Light on Mengovirus: Formation of Uracil Dimers, Instability and Degradation of Capsid, and Covalent Linkage of Protein to Viral RNA. J. Virol. 1974, 13, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Beck, S.E.; Hull, N.M.; Poepping, C.; Linden, K.G. Wavelength-Dependent Damage to Adenoviral Proteins Across the Germicidal UV Spectrum. Environ. Sci. Technol. 2018, 52, 223–229. [Google Scholar] [CrossRef]
- Espinoza, J.H.; Mercado-Uribe, H. Visible Light Neutralizes the Effect Produced by Ultraviolet Radiation in Proteins. J. Photochem. Photobiol. B 2017, 167, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, R.; Bandla, S. Ultraviolet Pasteurization for Food Industry. Int. J. Food Sci. Nutr. Eng. 2012, 2, 12–15. [Google Scholar] [CrossRef]
- Chatterley, C.; Linden, K. Demonstration and Evaluation of Germicidal UV-LEDs for Point-of-Use Water Disinfection. J. Water Health 2010, 8, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Kujundzic, E.; Hernandez, M.; Miller, S.L. Ultraviolet Germicidal Irradiation Inactivation of Airborne Fungal Spores and Bacteria in Upper-Room Air and HVAC in-Duct Configurations. J. Environ. Eng. Sci. 2007, 6, 1–9. [Google Scholar] [CrossRef]
- Koutchma, T. Advances in Ultraviolet Light Technology for Non-Thermal Processing of Liquid Foods. Food Bioprocess Technol. 2009, 2, 138–155. [Google Scholar] [CrossRef]
- Spencer, M.; Vignari, M.; Bryce, E.; Johnson, H.B.; Fauerbach, L.; Graham, D. A Model for Choosing an Automated Ultraviolet-C Disinfection System and Building a Case for the C-Suite: Two Case Reports. Am. J. Infect. Control 2017, 45, 288–292. [Google Scholar] [CrossRef]
- Darnell, M.E.R.; Subbarao, K.; Feinstone, S.M.; Taylor, D.R. Inactivation of the Coronavirus That Induces Severe Acute Respiratory Syndrome, SARS-CoV. J. Virol. Methods 2004, 121, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Heilingloh, C.S.; Aufderhorst, U.W.; Schipper, L.; Dittmer, U.; Witzke, O.; Yang, D.; Zheng, X.; Sutter, K.; Trilling, M.; Alt, M.; et al. Susceptibility of SARS-CoV-2 to UV Irradiation. Am. J. Infect. Control 2020, 48, 1273–1275. [Google Scholar] [CrossRef]
- Conner-Kerr, T.A.; Sullivan, P.K.; Gaillard, J.; Franklin, M.E.; Jones, R.M. The Effects of Ultraviolet Radiation on Antibiotic-Resistant Bacteria in Vitro. Ostomy. Wound Manag. 1998, 44, 50–56. [Google Scholar]
- Pan, M.; Lednicky, J.A.; Wu, C.-Y. Collection, Particle Sizing and Detection of Airborne Viruses. J. Appl. Microbiol. 2019, 127, 1596–1611. [Google Scholar] [CrossRef]
- Heneghan, C.J.; Spencer, E.A.; Brassey, J.; Plüddemann, A.; Onakpoya, I.J.; Evans, D.H.; Conly, J.M.; Jefferson, T. SARS-CoV-2 and the Role of Airborne Transmission: A Systematic Review. F1000Research 2021, 10, 232. [Google Scholar] [CrossRef]
- Tang, J.W.; Bahnfleth, W.P.; Bluyssen, P.M.; Buonanno, G.; Jimenez, J.L.; Kurnitski, J.; Li, Y.; Miller, S.; Sekhar, C.; Morawska, L.; et al. Dismantling Myths on the Airborne Transmission of Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2). J. Hosp. Infect. 2021, 110, 89–96. [Google Scholar] [CrossRef]
- Wilson, N.; Corbett, S.; Tovey, E. Airborne Transmission of COVID-19. BMJ 2020, 370, m3206. [Google Scholar] [CrossRef]
- Noorimotlagh, Z.; Jaafarzadeh, N.; Martínez, S.S.; Mirzaee, S.A. A Systematic Review of Possible Airborne Transmission of the COVID-19 Virus (SARS-CoV-2) in the Indoor Air Environment. Environ. Res. 2021, 193, 110612. [Google Scholar] [CrossRef] [PubMed]
- Baraniuk, C. COVID-19: What Do We Know about Airborne Transmission of SARS-CoV-2? BMJ 2021, 373, n1030. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Jimenez, J.L.; Prather, K.A.; Tufekci, Z.; Fisman, D.; Schooley, R. Ten Scientific Reasons in Support of Airborne Transmission of SARS-CoV-2. Lancet 2021, 397, 1603–1605. [Google Scholar] [CrossRef]
- Hwang, S.E.; Chang, J.H.; Oh, B.; Heo, J. Possible Aerosol Transmission of COVID-19 Associated with an Outbreak in an Apartment in Seoul, South Korea, 2020. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 104, 73–76. [Google Scholar] [CrossRef]
- Kang, M.; Wei, J.; Yuan, J.; Guo, J.; Zhang, Y.; Hang, J.; Qu, Y.; Qian, H.; Zhuang, Y.; Chen, X.; et al. Probable Evidence of Fecal Aerosol Transmission of SARS-CoV-2 in a High-Rise Building. Ann. Intern. Med. 2020, 173, M20-0928. [Google Scholar] [CrossRef]
- Miller, S.L.; Nazaroff, W.W.; Jimenez, J.L.; Boerstra, A.; Buonanno, G.; Dancer, S.J.; Kurnitski, J.; Marr, L.C.; Morawska, L.; Noakes, C. Transmission of SARS-CoV-2 by Inhalation of Respiratory Aerosol in the Skagit Valley Chorale Superspreading Event. Indoor Air 2021, 31, 314–323. [Google Scholar] [CrossRef]
- Spagnolo, A.M.; Ottria, G.; Amicizia, D.; Perdelli, F.; Cristina, M.L. Operating Theatre Quality and Prevention of Surgical Site Infections. J. Prev. Med. Hyg. 2013, 54, 131–137. [Google Scholar]
- Milstone, L.M.; Hu, R.-H.; Dziura, J.D.; Zhou, J. Impact of Epidermal Desquamation on Tissue Stores of Iron. J. Dermatol. Sci. 2012, 67, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Whyte, W.; Hodgson, R.; Tinkler, J.; Graham, J. The Isolation of Bacteria of Low Pathogenicity from Faulty Orthopaedic Implants. J. Hosp. Infect. 1981, 2, 219–230. [Google Scholar] [CrossRef]
- Benito, N.; Mur, I.; Ribera, A.; Soriano, A.; Rodríguez-Pardo, D.; Sorlí, L.; Cobo, J.; Fernández-Sampedro, M.; del Toro, M.D.; Guío, L.; et al. The Different Microbial Etiology of Prosthetic Joint Infections According to Route of Acquisition and Time after Prosthesis Implantation, Including the Role of Multidrug-Resistant Organisms. J. Clin. Med. 2019, 8, 673. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, W.J.; Bahnfleth, W.P. Airborne Respiratory Diseases and Mechanical Systems for Control of Microbes. HPAC Heat. Pip. Air Cond. 1998, 70, 7. [Google Scholar]
- Abraham, G.; Smith, P.M.L.B.; McCabe, P. Hepa Filter Replacement Experience in a Biological Laboratory. J. Am. Biol. Saf. Assoc. 1998, 3, 134–142. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Guo, J.; Xiong, Y.; Kang, T.; Xiang, Z.; Qin, C. Bacterial Community Analysis of Floor Dust and HEPA Filters in Air Purifiers Used in Office Rooms in ILAS, Beijing. Sci. Rep. 2020, 10, 6417. [Google Scholar] [CrossRef]
- Guieysse, B.; Hort, C.; Platel, V.; Munoz, R.; Ondarts, M.; Revah, S. Biological Treatment of Indoor Air for VOC Removal: Potential and Challenges. Biotechnol. Adv. 2008, 26, 398–410. [Google Scholar] [CrossRef]
- Rumchev, K.; Spickett, J.; Bulsara, M.; Phillips, M.; Stick, S. Association of Domestic Exposure to Volatile Organic Compounds with Asthma in Young Children. Thorax 2004, 59, 746–751. [Google Scholar] [CrossRef]
- Barnewall, R.E.; Bischoff, W.E. Removal of SARS-CoV-2 Bioaerosols Using Ultraviolet Air Filtration. Infect. Control Hosp. Epidemiol. 2021, 42, 1014–1015. [Google Scholar] [CrossRef]
- Qiao, Y.; Yang, M.; Marabella, I.A.; McGee, D.A.J.; Aboubakr, H.; Goyal, S.; Hogan, C.J., Jr.; Olson, B.A.; Torremorell, M. Greater than 3-Log Reduction in Viable Coronavirus Aerosol Concentration in Ducted Ultraviolet-C (UV–C) Systems. Environ. Sci. Technol. 2021, 55, 4174–4182. [Google Scholar] [CrossRef]
- First, M.; Rudnick, S.N.; Banahan, K.F.; Vincent, R.L.; Brickner, P.W. Fundamental Factors Affecting Upper-Room Ultraviolet Germicidal Irradiation—Part I. Experimental. J. Occup. Environ. Hyg. 2007, 4, 321–331. [Google Scholar] [CrossRef]
- Escombe, A.R.; Moore, D.A.J.; Gilman, R.H.; Navincopa, M.; Ticona, E.; Mitchell, B.; Noakes, C.; Martínez, C.; Sheen, P.; Ramirez, R.; et al. Upper-Room Ultraviolet Light and Negative Air Ionization to Prevent Tuberculosis Transmission. PLoS Med. 2009, 6, e1000043. [Google Scholar] [CrossRef] [PubMed]
- Wells, W.F.; Wells, M.W.; Wilder, T.S. The environmental control of epidemic contagion. Am. J. Epidemiol. 1942, 35, 97–121. [Google Scholar] [CrossRef]
- Kane, D.W.; Finley, C.; Brown, D. UV-C Light and Infection Rate in a Long Term Care Ventilator Unit. Can. J. Infect. Control 2018, 33, 5. [Google Scholar]
- Ethington, T.; Newsome, S.; Waugh, J.; Lee, L.D. Cleaning the Air with Ultraviolet Germicidal Irradiation Lessened Contact Infections in a Long-Term Acute Care Hospital. Am. J. Infect. Control 2018, 46, 482–486. [Google Scholar] [CrossRef]
- Miller, S.L. Upper Room Germicidal Ultraviolet Systems for Air Disinfection Are Ready for Wide Implementation. Am. J. Respir. Crit. Care Med. 2015, 192, 407–409. [Google Scholar] [CrossRef]
- Nardell, E.A.; Bucher, S.J.; Brickner, P.W.; Wang, C.; Vincent, R.L.; Becan-McBride, K.; James, M.A.; Michael, M.; Wright, J.D. Safety of Upper-Room Ultraviolet Germicidal Air Disinfection for Room Occupants: Results from the Tuberculosis Ultraviolet Shelter Study. Public Health Rep. 2008, 123, 52–60. [Google Scholar] [CrossRef]
- Carlsson, D.J.; Wiles, D.M. Surface Changes during the Photo-Oxidation of Polypropylene. J. Polym. Sci. B 1970, 8, 419–424. [Google Scholar] [CrossRef]
- Kramer, A.; Assadian, O. Survival of Microorganisms on Inanimate Surfaces. In Use of Biocidal Surfaces for Reduction of Healthcare Acquired Infections; Borkow, G., Ed.; Springer International Publishing: Cham, Switzerland, 2014; pp. 7–26. ISBN 978-3-319-08057-4. [Google Scholar]
- Riddell, S.; Goldie, S.; Hill, A.; Eagles, D.; Drew, T.W. The Effect of Temperature on Persistence of SARS-CoV-2 on Common Surfaces. Virol. J. 2020, 17, 145. [Google Scholar] [CrossRef]
- Wagenvoort, J.H.T.; De Brauwer, E.I.G.B.; Penders, R.J.R.; Willems, R.J.; Top, J.; Bonten, M.J. Environmental Survival of Vancomycin-Resistant Enterococcus Faecium. J. Hosp. Infect. 2011, 77, 282–283. [Google Scholar] [CrossRef]
- Kim, K.-H.; Fekety, R.; Batts, D.H.; Brown, D.; Cudmore, M.; Silva, J.; Waters, D. Isolation of Clostridium Difficile from the Environment and Contacts of Patients with Antibiotic-Associated Colitis. J. Infect. Dis. 1981, 143, 42–50. [Google Scholar] [CrossRef]
- Woodside, J.; Weaver, T. Guide to Infection Prevention in Emergency Medical Services; Association for Professionals in Infection Control and Epidemiology: Washington, DC, USA, 2013; ISBN 978-1-933013-54-1. [Google Scholar]
- Alfa, M.J.; Olson, N.; Murray, B.-L. Adenosine Tri-Phosphate (ATP)-Based Cleaning Monitoring in Health Care: How Rapidly Does Environmental ATP Deteriorate? J. Hosp. Infect. 2015, 90, 59–65. [Google Scholar] [CrossRef]
- Eckstein, B.C.; Adams, D.A.; Eckstein, E.C.; Rao, A.; Sethi, A.K.; Yadavalli, G.K.; Donskey, C.J. Reduction of Clostridium Difficile and Vancomycin-Resistant Enterococcus Contamination of Environmental Surfaces after an Intervention to Improve Cleaning Methods. BMC Infect. Dis. 2007, 7, 61. [Google Scholar] [CrossRef] [PubMed]
- Engelhart, S.; Krizek, L.; Glasmacher, A.; Fischnalle, E.; Marklein, G.; Exner, M. Pseudomonas Aeruginosa outbreak Ina Haematology-Oncology Unit Associated Withcontaminated Surface Cleaning Equipment. J. Hosp. Infect. 2002, 52, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tian, H.; Zhang, L.; Zhang, M.; Guo, D.; Wu, W.; Zhang, X.; Kan, G.L.; Jia, L.; Huo, D.; et al. Reduction of Secondary Transmission of SARS-CoV-2 in Households by Face Mask Use, Disinfection and Social Distancing: A Cohort Study in Beijing, China. BMJ Glob. Health 2020, 5, e002794. [Google Scholar] [CrossRef] [PubMed]
- National Center for Immunization and Respiratory Diseases (NCIRD). Division of Viral Diseases Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. In CDC COVID-19 Science Briefs; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. [Google Scholar]
- Nerandzic, M.M.; Thota, P.; Sankar, C.T.; Jencson, A.; Cadnum, J.L.; Ray, A.J.; Salata, R.A.; Watkins, R.R.; Donskey, C.J. Evaluation of a Pulsed Xenon Ultraviolet Disinfection System for Reduction of Healthcare-Associated Pathogens in Hospital Rooms. Infect. Control Hosp. Epidemiol. 2015, 36, 192–197. [Google Scholar] [CrossRef]
- Brunk, C.F. Distribution of Dimers in Ultraviolet-Irradiated DNA. Nat. New Biol. 1973, 241, 74–76. [Google Scholar] [CrossRef]
- Eggertson, L.; Sibbald, B. Hospitals Battling Outbreaks of C. Difficile. CMAJ Can. Med. Assoc. J. 2004, 171, 19–21. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bryce, E.; Zurberg, T.; Zurberg, M.; Shajari, S.; Roscoe, D. Identifying Environmental Reservoirs of Clostridium Difficile with a Scent Detection Dog: Preliminary Evaluation. J. Hosp. Infect. 2017, 97, 140–145. [Google Scholar] [CrossRef]
- Browne, K.; Wood, D.; Clezy, K.; Lehm, J.; Walsh, W.R. Reduction of Bacterial Load with the Addition of Ultraviolet-C Disinfection inside the Hyperbaric Chamber. Diving Hyperb. Med. J. 2020, 50, 332–337. [Google Scholar] [CrossRef]
- Browne, K.L.; Crowley, J.D.; Tan, C.J.; O’Sullivan, C.B.; Walsh, W.R. Effect of Ultraviolet-C Light on the Environmental Bacterial Bioburden in Various Veterinary Facilities. Am. J. Vet. Res. 2021, 82, 582–588. [Google Scholar] [CrossRef]
- Anderson, D.J.; Gergen, M.F.; Smathers, E.; Sexton, D.J.; Chen, L.F.; Weber, D.J.; Rutala, W.A. Decontamination of Targeted Pathogens from Patient Rooms Using an Automated Ultraviolet-C-Emitting Device. Infect. Control Hosp. Epidemiol. 2013, 34, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M.; Havill, N.L.; Moore, B.A. Terminal Decontamination of Patient Rooms Using an Automated Mobile UV Light Unit. Infect. Control Hosp. Epidemiol. 2011, 32, 737–742. [Google Scholar] [CrossRef]
- Yang, J.-H.; Wu, U.-I.; Tai, H.-M.; Sheng, W.-H. Effectiveness of an Ultraviolet-C Disinfection System for Reduction of Healthcare-Associated Pathogens. J. Microbiol. Immunol. Infect. 2019, 52, 487–493. [Google Scholar] [CrossRef]
- Anderson, D.J.; Chen, L.F.; Weber, D.J.; Moehring, R.W.; Lewis, S.S.; Triplett, P.F.; Blocker, M.; Becherer, P.; Schwab, J.C.; Knelson, L.P.; et al. Enhanced Terminal Room Disinfection and Acquisition and Infection Caused by Multidrug-Resistant Organisms and Clostridium Difficile (the Benefits of Enhanced Terminal Room Disinfection Study): A Cluster-Randomised, Multicentre, Crossover Study. Lancet Lond. Engl. 2017, 389, 805–814. [Google Scholar] [CrossRef]
- Anderson, D.J.; Moehring, R.W.; Weber, D.J.; Lewis, S.S.; Chen, L.F.; Schwab, J.C.; Becherer, P.; Blocker, M.; Triplett, P.F.; Knelson, L.P.; et al. Effectiveness of Targeted Enhanced Terminal Room Disinfection on Hospital-Wide Acquisition and Infection with Multidrug-Resistant Organisms and Clostridium Difficile: A Secondary Analysis of a Multicentre Cluster Randomised Controlled Trial with Crossover Design (BETR Disinfection). Lancet Infect. Dis. 2018, 18, 845–853. [Google Scholar] [CrossRef]
- Blue, J.; O’Neill, C.; Speziale, P.; Revill, J.; Ramage, L.; Ballantyne, L. Use of a Fluorescent Chemical as a Quality Indicator for a Hospital Cleaning Program. Can. J. Infect. Control Off. J. Community Hosp. Infect. Control Assoc.-Can. Rev. Can. Prev. Infect. 2008, 23, 216–219. [Google Scholar]
- Pittet, D.; Hugonnet, S.; Harbarth, S.; Mourouga, P.; Sauvan, V.; Touveneau, S.; Perneger, T.V. Effectiveness of a Hospital-Wide Programme to Improve Compliance with Hand Hygiene. Lancet 2000, 356, 1307–1312. [Google Scholar] [CrossRef]
- Datta, R.; Platt, R.; Yokoe, D.S.; Huang, S.S. Environmental Cleaning Intervention and Risk of Acquiring Multidrug-Resistant Organisms From Prior Room Occupants. Arch. Intern. Med. 2011, 171, 491–494. [Google Scholar] [CrossRef]
- Pavia, M.; Simpser, E.; Becker, M.; Mainquist, W.K.; Velez, K.A. The Effect of Ultraviolet-C Technology on Viral Infection Incidence in a Pediatric Long-Term Care Facility. Am. J. Infect. Control 2018, 46, 720–722. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.M.; Donzanti, M.J.; Minahan, D.J.; Shirazi, J.; Hatem, C.L.; Hayward-Piatkovskyi, B.; Dang, A.M.; Nelson, K.M.; Bothi, K.L.; Gleghorn, J.P. Mask Reuse in the COVID-19 Pandemic: Creating an Inexpensive and Scalable Ultraviolet System for Filtering Facepiece Respirator Decontamination. Glob. Health Sci. Pract. 2020, 8, 582–595. [Google Scholar] [CrossRef]
- Kea, B.; Johnson, A.; Lin, A.; Lapidus, J.; Cook, J.N.; Choi, C.; Chang, B.P.; Probst, M.A.; Park, J.; Atzema, C.; et al. An International Survey of Healthcare Workers Use of Personal Protective Equipment during the Early Stages of the COVID-19 Pandemic. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12392. [Google Scholar] [CrossRef] [PubMed]
- Ludwig-Begall, L.F.; Wielick, C.; Jolois, O.; Dams, L.; Razafimahefa, R.M.; Nauwynck, H.; Demeuldre, P.-F.; Napp, A.; Laperre, J.; Thiry, E.; et al. “Don, Doff, Discard” to “Don, Doff, Decontaminate”—FFR and Mask Integrity and Inactivation of a SARS-CoV-2 Surrogate and a Norovirus Following Multiple Vaporised Hydrogen Peroxide-, Ultraviolet Germicidal Irradiation-, and Dry Heat Decontaminations. PLoS ONE 2021, 16, e0251872. [Google Scholar] [CrossRef]
- Kayani, B.J.; Weaver, D.T.; Gopalakrishnan, V.; King, E.S.; Dolson, E.; Krishnan, N.; Pelesko, J.; Scott, M.J.; Hitomi, M.; Cadnum, J.L.; et al. UV-C Tower for Point-of-Care Decontamination of Filtering Facepiece Respirators. Am. J. Infect. Control 2021, 49, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Ludwig-Begall, L.F.; Wielick, C.; Dams, L.; Nauwynck, H.; Demeuldre, P.-F.; Napp, A.; Laperre, J.; Haubruge, E.; Thiry, E. The Use of Germicidal Ultraviolet Light, Vaporized Hydrogen Peroxide and Dry Heat to Decontaminate Face Masks and Filtering Respirators Contaminated with a SARS-CoV-2 Surrogate Virus. J. Hosp. Infect. 2020, 106, 577–584. [Google Scholar] [CrossRef]
- Tande, B.M.; Carson, P.; Rutala, W.; Guerrero, D.M. Designing Healthcare Facilities to Maximize the Effectiveness of UV Disinfection. Am. J. Infect. Control 2014, 42, S42–S43. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Browne, K. Brought to Light: How Ultraviolet Disinfection Can Prevent the Nosocomial Transmission of COVID-19 and Other Infectious Diseases. Appl. Microbiol. 2021, 1, 537-556. https://doi.org/10.3390/applmicrobiol1030035
Browne K. Brought to Light: How Ultraviolet Disinfection Can Prevent the Nosocomial Transmission of COVID-19 and Other Infectious Diseases. Applied Microbiology. 2021; 1(3):537-556. https://doi.org/10.3390/applmicrobiol1030035
Chicago/Turabian StyleBrowne, Katrina. 2021. "Brought to Light: How Ultraviolet Disinfection Can Prevent the Nosocomial Transmission of COVID-19 and Other Infectious Diseases" Applied Microbiology 1, no. 3: 537-556. https://doi.org/10.3390/applmicrobiol1030035
APA StyleBrowne, K. (2021). Brought to Light: How Ultraviolet Disinfection Can Prevent the Nosocomial Transmission of COVID-19 and Other Infectious Diseases. Applied Microbiology, 1(3), 537-556. https://doi.org/10.3390/applmicrobiol1030035