

Participation in Everyday Leisure and Its Influencing Factors for People with Intellectual Disabilities: A Scoping Review of the Empirical Findings


Abstract
1. Introduction
2. Leisure as an Important Domain of Life
- As activity—some activities involve planning, the use of facilities or equipment, and the involvement of other people. Others are much more spontaneous.
- As time—leisure takes place in ‘non-obligated time’, in other words, those occasions when we are free of responsibilities and the demands of others.
- As a state of mind—when we feel free to choose our activity to please ourselves, without external pressure or rewards [17].
3. Leisure Participation of Individuals with Intellectual Disabilities
4. Method
4.1. Scoping Review Questions
- What perspectives for action and research can be identified to support and ensure the participation of people with intellectual disabilities in leisure time?
- What characteristics are used to define leisure participation for people with mild to moderate intellectual disabilities and for people with severe to profound intellectual disabilities?
- What are the patterns of participation in everyday leisure activities of people with mild to moderate intellectual disabilities in comparison to people with severe to profound intellectual disabilities?
- What are the factors that facilitate or hinder the use of leisure time and participation in leisure activities of people with intellectual disabilities?
4.2. Review Protocol
Inclusion and Exclusion Criteria and Search Strategy
- Mild intellectual disability;
- Moderate intellectual disability;
- Severe intellectual disability;
- Profound intellectual disability.
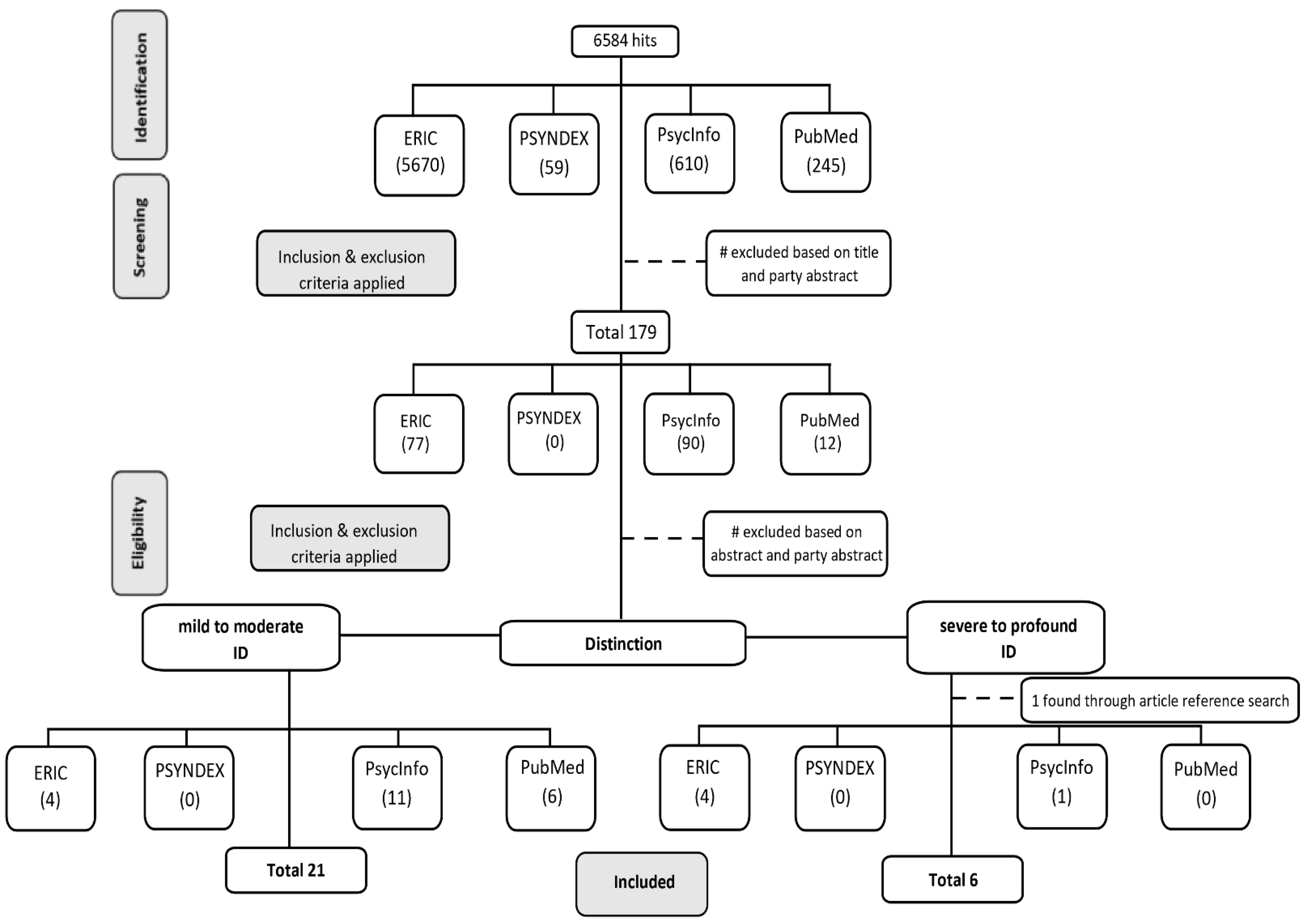
4.3. Study Selection
4.4. Study Charting and Analysis
5. Results
5.1. Overview
5.2. Definitions and Assessment of Leisure Participation
5.2.1. Participants with Mild to Moderate ID
5.2.2. Participants with Severe to Profound ID
5.3. Patterns of Leisure Participation
5.3.1. Patterns of Leisure Participants with Mild to Moderate ID
5.3.2. Patterns of Leisure Participants with Severe to Profound ID
5.4. Influencing Factors on Leisure Participation
5.4.1. Body and Mental Functioning
5.4.2. Activity Limitations
5.4.3. Contextual Characteristics
Personal Factors
Environmental Factors
6. Discussion
6.1. Perspectives for Practice and Further Research
6.2. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Ref. | Authors | Sample and Diagnosis | Age (Year) | Type | Outcome Measures | Type of Leisure Participation | Main Findings (Pattern of Leisure Participation & Influencing Factors) |
|---|---|---|---|---|---|---|---|
| [60] | Beart; Hawkins; Kroese; Smithson; Tolosa 2001 UK | n = 29 (mild to moderate ID) | >16 | Qualitative | Focused interview (focus group) | Activities performed, facilitators to perform these activities, leisure wishes/interests, barriers to involvement | ‘It was found that participants undertook a wide variety of community-based leisure pursuits. Many of these activities took place in day centre time, as opposed to genuine leisure time. A range of activities which participants would wish to try in the future were identified. However, there were a number of perceived barriers which would make it difficult to access these opportunities. All five groups identified these barriers as being a lack of transport and carer/friend support.’ |
| [56] | Yu; Spevack; Hiebert; Martin; Goodman; Martin; Harapiak; Martin 2002 Canada | n = 12 (severe ID) n = 7 (profound ID) | 22–45 | Quantitative | Observation | Leisure activities for enjoyment: listening to music, watching TV, attending a concert in the gym, coffee and lunch breaks | ‘[…] groups showed more happiness indices during leisure than work activities, although the difference for the profound group was small (8% vs. 5%) compared to the severe group (18% vs. 4%).’ |
| [50] | Duvdevany; Arar 2004 Israel | n = 85 (ID) | 18–55 | Quantitative | Leisure Activities List [73], four further questionnaires (demographic, quality of life (QOL), loneliness, social relationship) | Subjective engagement (satisfaction, happiness, loneliness) during leisure activities, frequency of active and passive activities, and subjective assessment of independence | ‘The main findings show no significant differences between the two groups (people who live in foster homes and people who live in community settings) in the number of friendships or feelings of loneliness. Foster residents were more involved and more independent in their leisure activities than were those who live in community residences. […]’ |
| [58] | Wilson; Reid; Green 2006 USA | n = 3 (severe disabilities) | 25–29 | Quantitative | Interview (open-ended); structured interview; observations | Target behavior: participant leisure engagement in naturally occurring leisure times and responding to choices from the staff | ‘[…] during the choice presentation condition, each participant engaged in leisure activity during half or more of the observation intervals during each observation session […].’ ‘Corresponding with the lack of staff choice presentations during baseline, no participant was observed to make any leisure choices during baseline.’ ‘The comparison observations in other Supported Independent Living (SIL) situations further suggest that in-home leisure involvement of adults with severe disabilities can be problematic in these types of settings.’ |
| [28] | Buttimer; Tierney 2005 Ireland | n = 34 (mild/moderate ID) n = 34 (parents) | >16 | Quantitative | TLAB questionnaire [74] | Frequency of involvement in different kinds of activities (previous participation in a specific leisure activity and frequency); barriers of involvement | ‘Leisure activities which were mostly solitary and passive in nature were identified as those being most commonly engaged in. Barriers to leisure were also identified, with ‘access to’ and ‘location of’ the leisure facilities being barriers perceived by both students and parents.’ |
| [57] | Zijlstra; Vlaskamp 2005 Netherlands | n = 196 (PIMD) | >18 | Quantitative | Questionnaire, diary | Duration, frequency, location, and content of leisure activities in residential facilities during weekends | ‘A total mean of 3.8 h of leisure activities is provided for during the full weekend, almost half of which includes watching television or listening to music. Leisure activities are almost exclusively offered by professionals. Parents or volunteers only provide a minimum of activities during weekends.’ |
| [61] | Sellinger; Hodapp; Dykens 2006 USA | n = 223 (ID) | 5–54 | Quantitative | Behavior checklist, Leisure Activities Questionnaire [75] | Frequency of involvement in ‘common leisure activities for persons with mental retardation’ | ‘Individuals with Williams syndrome less often participated in visual-spatial activities, those with Prader-Willi syndrome more often performed both visual-spatial and visual strategy activities, and those with Williams and Down syndromes more often performed musical activities. With increasing chronological ages, all groups increased in their social activities […].’ |
| [51] | Yalon-Chamowitz; Weiss 2008 Israel | n = 33 (moderate ID & severe cerebral palsy) | 20–39 | Quantitative | Questionnaire adapted from short feedback questionnaire [76] and based on Witmer and Singer’s [77] presence questionnaire, structured observation | Subjective enjoyment of the game, the degree of success at it, the extent of control within game, concentration span and fatigue, as well as the degree of their involvement in choosing the game | ‘The VR-based activities were perceived by the participants to be enjoyable and successful. Moreover, participants demonstrated clear preferences, initiation and learning. They performed consistently and maintained a high level of interest throughout the intervention period.’ |
| [52] | Patterson; Pegg 2009 Australia | n = 10 (mild to moderate ID) | 19–57 | Qualitative | Semi-structured interviews | Participation in community-based serious leisure activities; questions about interest, importance, duration/frequency, friendship, belonging, barriers, enjoyment, goals for the future | ‘The results of this study found that people with disabilities have the ability to participate in serious leisure activities and to successfully engage at such a level so as to enable them to develop increased levels of confidence, skills and self-esteem.’ |
| [49] | Solish; Perry; Minnes 2010 Canada | n = 90 (Typically Developed children (TD)) n = 65 (Autism Spectrum Disorder (ASD)) n = 30 (ID) | 5–17 | Quantitative | The activities questionnaire (participation in social, recreational, leisure activities) | Number and frequency of social, recreational, and leisure activities with peers; leisure partners; number and nature of friendships | ‘The TD children participated in significantly more social and recreational activities and had more friends than the children with disabilities. […]’ Children with ASD or ID participated in more social activities with their parents or other adults than peers. Children with ID had more friends than children with ASD. |
| [62] | Azaiza; Rimmerman; Croitori; Naon 2011 Israel | n = 153 (ID) | 16–65 | Quantitative | Questionnaire | ‘Items assessing health condition, physical functioning, cognitive functioning, Activities of Daily Living and Instrumental Activities of Daily Living (ADL & IADL), participation in employment and service utilisation’ | Employed participants participated more in leisure activities than unemployed participants. Cognitive functioning correlates strongly with participation in leisure activities. Physical functioning correlates weakly with participation in leisure activities. Participation in leisure activities correlated moderately with knowledge of services and accessibility to services. All the correlations were significant. |
| [26] | Badia; Orgaz; Verdugo; Ullán; Martínez 2011 Spain | N = 237 (DD) n = 161 (mild to moderate ID) n = 14 (severe ID) | 17–65 | Quantitatve | Leisure activity participation, preference, and interests (activity photographs), questionnaire (personal and disability-related factors) | Type and number of leisure activities and activities in which the individual would like to increase participation; degree of unmet leisure involvement based on the selection of activities in which the individual has an interest, but in which he or she is not participating; internal and external barriers for leisure participation | ‘The results show that participation in leisure activities is determined more by personal factors and perceived barriers than by disability-related factors.’ Perceived barriers accounted for the degree of participation in physical and social leisure activities. Participation in leisure activities at home were equally explained by personal and environmental factors. |
| [63] | Dusseljee; Rijken; Cardol; Curfs; Groenewegen 2011 Netherlands | n = 653 (mild or moderate ID) | 15–88 | Quantitative | Interviews and questionnaires of those who could not be interviewed | Community participation in the domains of work, social contacts, and leisure activities; assessment of participation in leisure activities by two items: ‘(1) whether the person with ID sometimes visited a restaurant, café, cinema or theatre; and (2) whether he/she was engaged in leisure activities not specifically for people with ID’ | ‘Most people with mild or moderate ID in the Netherlands have work or other daytime activities, have social contacts and have leisure activities. However, people aged 50 years and over and people with moderate ID participate less in these domains than those under 50 years and people with mild ID. Moreover, people with ID hardly participate in activities with people without ID.’ |
| [27] | Badia; Orgaz; Verdugo; Ullán 2013 Spain | N = 237 (DD) n= 167 (ID) | 17–65 | Quantitative | Leisure activity participation, preference and interests (activity photographs), questionnaire (personal and disability-related factors) | Actual performance of different types of leisure activities, wish to perform these activities more often, interest in participating in these activities | ‘Leisure social activities and recreation activities at home were mostly solitary and passive in nature and were identified as those being most commonly engaged in. Respondents expressed preference for more social and physical activity, and they were interested in trying out a large number of physical activities. Age and type of schooling determine participation in leisure activity. The results underscore the differences in leisure activity participation, preference and interest depending on the severity of the disability.’ |
| [23] | Badia; Orgaz; Verdugo; Ullán; Martínez 2013 Spain | N = 125 (ID) n = 52 (mild ID) n = 64 (moderate to severe ID) | 17–65 | Quantitative | The Spanish version of the Leisure Assessment Inventory (LAI) [26]: leisure activity participation, preference and interests (activity photographs), subjective scale of integral quality scale | Leisure participation dimensions are leisure activities, preference, interest, and constraints | ‘No relationship was found between objective quality of life and leisure participation. However, correlations between some leisure participation dimensions and specific subjective quality of life domains were observed. The results establish a predictive relationship between leisure participation and material, emotional, and physical well-being. […]’ |
| [46] | Dolva; Kleiven; Kollstad 2014 Norway | n = 38 (parents of adolescents with Down Syndrome) | 14 | Qualitative | Structured parent interviews | Focus on leisure activities that engage adolescents with Down syndrome in their everyday life outside school | ‘The adolescents’ leisure appears as active and social. However, social participation largely involved parents and family, while socializing with other adolescents mainly took place within formal activities adapted for disabled.’ |
| [64] | Dykens 2014 USA | n = 123 (parents of people with Prader-Willi Syndrome, mild ID) | 4–48 | Quantitative | Questionnaires (demographic variables, behavior), Recreation and Leisure Questionnaire [61], IQ test, semi-structured interview (adaptive behavior) | Frequency of engagement in 30 specific leisure activities, reasons for engagement | Watching TV was the most frequent recreational activity, and was associated with compulsivity and skin picking. BMIs were negatively correlated with physical play, and were highest in those who watched TV and played computer games. Computer games, puzzles, and physical activities were associated with a higher IQ and adaptive scores. |
| [53] | Lövgren; Bertilsdotter Rosqvist 2015 Sweden | n = 13 (ID) | 38–60 | Qualitative | Semi-structured interviews, field-visits | Everyday life, work vs. leisure, and retirement, ageing, and identity were highlighted | ‘Structured activities are arranged by disability services in order to normalise living conditions and provide recreation for disabled people. However, the range of activities is constrained by financial resources, by notions of gender and age and by an institutionalised emphasis on the work ethic—leading to constructions of leisure partly as ‘time beside’ where ‘free time’ activities should not interfere with the duties of the working week.’ ‘This ‘free time’ was mainly associated with household chores, exercise […] and some social activities. Media consumption was described as a common activity, and appeared to sometimes be a social activity but more commonly to be a way of dealing with loneliness.’ |
| [65] | Venkatesan; Vashodharakumar 2016 India | n = 90 (TD) n = 30 (ID) | 8–39 | Quantitative | Self-developed semi-structures demographic data sheet, survey | Leisure participation is operationalized as nature, types, content, spread, and extent of leisure activities; community exposure refers to areas of social activity which may be used or can become an opportunity included in an individual’s leisure pursuits | ‘Concurrently, opportunities for community exposure indicate an overall identical trend of limited social visits (Mean: 4.58; SD: 3.26) which is lowest for persons with intellectual disabilities (Mean: 1.33; SD: 1.3), followed by significantly higher frequency for those with visual impairments (Mean: 3.50; SD: 1.75), hearing loss (Mean: 4.00; SD: 2.27) and the typical group (Mean: 9.50; SD: 1.59).’ |
| [54] | Hall 2017 USA | n = 14 (mild to moderate ID) | 21–35 | Qualitative | Semi-structured interview | Questions about experiences of inclusion in community activities (at work, recreation, and leisure activities) and the context of their experiences | ‘The young adults were involved in a variety of work, volunteer, recreation and leisure activities. Their experiences were influenced by the social interactions they had in each environment, the level of acceptance they felt, physical accommodations, the availability of transportation and supports offered by job coaches and other service provider staff, volunteers, co-workers, family members and friends.’ |
| [48] | Taheri; Perry; Minnes 2017 Canada | n = 197 (parents of children with severe DD; 41% only ID) | 4–19 | Quantitative | Survey (addressing child-, family-, and community-related variables), modified version of the Activity Questionnaire [49] | Frequency of participation in seven types of leisure activities; (1) unstructured play; (2) social outings; (3) special occasions; (4) sports team; (5) lessons (e.g., swimming); (6) community activities (e.g., Sunday school); and (7) activities for children with special needs | ‘Overall, the final model significantly accounted for 30% of the variance in activity participation. Higher adaptive behaviour, greater parental socialisation and placement in an integrated school programme were significant predictors of greater activity participation [(participation in social, recreational and leisure activities)].’ |
| [47] | Dolva; Kollstad; Kleiven 2019 Norway | n = 22 (Down Syndrome) | 17 | Qualitative | Semi-structured interviews, observations | Leisure pattern: ‘Leisure activities which are done day by day during an ordinary week, e.g., Tell me: “What did you do after school today?” Followed up: “With whom? Where? How was it?”’ | ‘Generally, the adolescents described their social life as rich and varied, occurring in several contexts with different companions. Their thoughts of friendships were quite extensive, also including less close relationships. Three main contextual patterns of social participation were revealed: (a) the family at home pattern, (b) the peer group pattern and (c) the arranged company pattern.’ |
| [22] | Doistua; Lazcano; Madarlaga 2020 Spain | N = 400 n = 100 (intellectual disabilities) | 15–29 | Quantitative | Ad hoc questionnaire (individual responsibility for leisure, satisfaction with leisure, perception of the relationship between the enjoyment of an activity, and individual responsibility for organizing their activities) | Relationship between self-managed leisure, satisfaction, benefits perceived by young people with disabilities | ‘Results revealed the following conclusions. First gender and type of disability relate to the degree of self-management associated with leisure. Second, there was a significant association between the degree of satisfaction with leisure and level of self-management associated with leisure and this relationship varied by disability type but not gender. Third, leisure independently organized by young people (self-managed) was associated with higher perceived psychological benefits (emotional and cognitive) connected with their leisure engagement.’ |
| [66] | Gilor; Klibanski; Kfir 2020 Israel | n = 18 (leisure activities’ organisers; without ID) | / | Qualitative | Semi-structured interviews | Organizations’ perspective: Difficulties in organising and implementing leisure activities for children with disabilities | ‘The difficulties that the participants encountered in the implementation of leisure activities for children with disability are related to the following topics: funding, access (transportation, as well as dissemination of the relevant information), inclusion and the attitude of the surrounding society.’ ‘The difficulties mentioned by the study’s interviewees are similar to those mentioned in studies that examined participation in leisure activities from the perspective of the people with disability, and their parents’. |
| [55] | Mihaila; Handen; Christian; Hartley 2020 USA | n = 44 | >25 | Quantitative | Leisure activities from the Victoria Longitudinal Study (VLS) questionnaire [77], TLAB [74], daily diary (in depth-description of the daily leisure activity) | Average daily leisure activity (physical, social, cognitively stimulating, passive leisure), amount of time spent in the activity and leisure barriers | ‘Findings indicated that the majority of adults with Down Syndrome did not meet established physical leisure activity intensity recommendations […] and did not exceed levels of passive leisure […] found in general population […]. Adults with Down syndrome self-initiated and self-engaged in the majority of their leisure activity. Family members and paid staff allocated resources towards initiating and engaging as social partners in social and physical leisure, respectively.’ |
| [59] | van Delden; Wintels; van Oorsouw; Evers; Embregts; Heylen; Reidsma 2020 Netherlands | n = 9 (PIMD) | 24–62 | Quantitative | Alertness observation list (AOL), affective behavior—a tailored observation scheme; movement—simplified motion energy analysis (SMEA); semi-structured interviews (staff members) | Active leisure involvement: interaction, alertness, affective behavior, movement | ‘Clearly positive effects were seen for three participants. Effects were seen in the unexpected direction for four participants. No strong effects were found for the remaining three participants.’ ‘Interactive technologies may provide suitable activities for people with PIMD but individual differences play an important role.’ |
| [45] | Pochstein 2022 Germany | n = 15 (families of children with ID) | 8–15 | Qualitative | Focus group interviews (one for the children, one for the parents, and one for the club representatives) | Eight-week sports program in mainstream clubs; physical activity | ‘The children rated participation very positively and only very occasionally reported that they had been excluded. The parents confirmed this experience, but were nevertheless more critical in their assessment. […] sufficiently available and qualified staff, better access to sports facilities, and a wider range of inclusive groups are needed.’ |
References
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001.
- Dijkers, M.P. Issues in the conceptualization and measurement of participation: An overview. Arch. Phys. Med. Rehabil. 2010, 91, S5–S16. [Google Scholar] [CrossRef]
- Nakken, H.; Vlaskamp, C. A Need for a Taxonomy for Profound Intellectual and Multiple Disabilities. J. Policy Pr. Intellect. Disabil. 2007, 4, 83–87. [Google Scholar] [CrossRef]
- Green, C.W.; Reid, D.H. A behavioral approach to identifying sources of happiness and unhappiness among individuals with profound multiple disabilities. Behav. Modif. 1999, 23, 280–293. [Google Scholar] [CrossRef]
- van Delden, R.; Reidsma, D.; van Oorsouw, W.; Poppe, R.; van der Vos, P.; Lohmeijer, A.; Embregts, P.; Evers, V.; Heylen, D. Towards an Interactive Leisure Activity for People with PIMD. In Proceedings of the 14th International Conference on Computers Helping People with Special Needs, Paris, France, 9–11 July 2014; pp. 276–282. [Google Scholar] [CrossRef]
- Andrews, J.; Falkmer, M.; Girdler, S. Community participation interventions for children and adolescents with a neurodevelopmental intellectual disability: A systematic review. Disabil. Rehabil. 2015, 37, 825–833. [Google Scholar] [CrossRef]
- Dean, E.E.; Fisher, K.W.; Shogren, K.A.; Wehmeyer, M.L. Participation and Intellectual Disability: A Review of the Literature. Intellect. Dev. Disabil. 2016, 54, 427–439. [Google Scholar] [CrossRef]
- Gauthier-Boudreault, C.; Beaudoin, A.J.; Gallagher, F.; Couture, M. Scoping review of social participation of individuals with profound intellectual disability in adulthood: What can I do once I finish school? J. Intellect. Dev. Disabil. 2019, 44, 248–260. [Google Scholar] [CrossRef]
- Shikako-Thomas, K.; Majnemer, A.; Law, M.; Lach, L. Determinants of Participation in Leisure Activities in Children and Youth with Cerebral Palsy: Systematic Review. Phys. Occup. Ther. Pediatr. 2008, 28, 155–169. [Google Scholar] [CrossRef]
- Tonkin, B.L.; Ogilvie, B.D.; Greenwood, S.A.; Law, M.C.; Anaby, D.R. The participation of children and youth with disabilities in activities outside of school: A scoping review. Can. J. Occup. Ther. 2014, 81, 226–236. [Google Scholar] [CrossRef]
- Verdonschot, M.M.L.; de Witte, L.; Reichrath, E.; Buntinx, W.H.E.; Curfs, L.M.G. Community participation of people with an intellectual disability: A review of empirical findings. J. Intellect. Disabil. Res. 2009, 53, 303–318. [Google Scholar] [CrossRef]
- Verdonschot, M.M.L.; de Witte, L.; Reichrath, E.; Buntinx, W.H.E.; Curfs, L.M.G. Impact of environmental factors on community participation of persons with an intellectual disability: A systematic review. J. Intellect. Disabil. Res. 2009, 53, 54–64. [Google Scholar] [CrossRef]
- Juniu, S. The transformation of leisure. Leisure 2009, 33, 463–478. [Google Scholar] [CrossRef]
- Opaschowski, H.W. Pädagogik Der Freien Lebenszeit; 3. Aufl. Leske + Budrich: Opladen, Germany, 1996; pp. 1–304. [Google Scholar] [CrossRef]
- Stebbins, R.A. Right leisure: Serious, casual, or project-based? Neurorehabilitation 2008, 23, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Page, S.J.; Connell, J. Leisure. An Introduction; Pearson Education Limited: Singapore, 2010; pp. 1–79. [Google Scholar]
- Denziloe, J. Fun & Games. Practical Leisure Ideas for People with Profound Disabilities; Butterworth-Heinemann Ltd.: Oxford, UK, 1994. [Google Scholar]
- Caldwell, L.L.; Baldwin, C.K. A Serious Look at Leisure: The Role of Leisure Time and Recreation Activities in Positive Youth Development. In Community Youth Development: Programs, Policies, and Practices; SAGE Publications Inc.: Washington, DC, USA, 2003; pp. 181–200. [Google Scholar] [CrossRef]
- Caldwell, L.L.; Witt, P.A. Leisure, recreation, and play from a developmental context. New Dir. Youth Dev. 2011, 2011, 13–27. [Google Scholar] [CrossRef]
- Anderson, A. The five-factor model for leisure management: Pedagogies for assessing personality differences in positive youth development programmes. World Leis. J. 2017, 59, 70–76. [Google Scholar] [CrossRef]
- Larson, R.W. Toward a psychology of positive youth development. Am. Psychol. 2000, 55, 170–183. [Google Scholar] [CrossRef]
- Doistua, J.; Lazcano, I.; Madariaga, A. Self-Managed Leisure, Satisfaction, and Benefits Perceived by Disabled Youth in Northern Spain. Front. Psychol. 2020, 11, 716. [Google Scholar] [CrossRef]
- Badia, M.; Orgaz, M.B.; Verdugo, M.; Ullán, A.M.; Martínez, M. Relationships between Leisure Participation and Quality of Life of People with Developmental Disabilities. J. Appl. Res. Intellect. Disabil. 2013, 26, 533–545. [Google Scholar] [CrossRef]
- Aitchison, C. From leisure and disability to disability leisure: Developing data, definitions and discourses. Disabil. Soc. 2003, 18, 955–969. [Google Scholar] [CrossRef]
- Aitchison, C. Exclusive discourses: Leisure studies and disability. Leis. Stud. 2009, 28, 375–386. [Google Scholar] [CrossRef]
- Badia, M.; Orgaz, B.M.; Verdugo, M.A.; Ullán, A.M.; Martínez, M.M. Personal factors and perceived barriers to participation in leisure activities for young and adults with developmental disabilities. Res. Dev. Disabil. 2011, 32, 2055–2063. [Google Scholar] [CrossRef] [PubMed]
- Badia, M.; Orgaz, M.B.; Verdugo, M.; Ullán, A.M. Patterns and determinants of leisure participation of youth and adults with developmental disabilities. J. Intellect. Disabil. Res. 2013, 57, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Buttimer, J.; Tierney, E. Patterns of leisure participation among adolescents with a mild intellectual disability. J. Intellect. Disabil. 2005, 9, 25–42. [Google Scholar] [CrossRef]
- Melbøe, L.; Ytterhus, B. Disability leisure: In what kind of activities, and when and how do youths with intellectual disabilities participate? Scand. J. Disabil. Res. 2016, 19, 245–255. [Google Scholar] [CrossRef]
- Eratay, E. Effectiveness of leisure time activities program on social skills and behavioral problems in individuals with intellectual disabilities. Acad. J. 2013, 8, 1437–1448. [Google Scholar]
- Eldeniz, M.; Cay, E. Examining Leisure Activity Engagement of Students with Intellectual Disability. Int. J. Educ. Methodol. 2020, 6, 57–66. [Google Scholar] [CrossRef]
- Dahan-Oliel, N.; Shikako-Thomas, K.; Majnemer, A. Quality of life and leisure participation in children with neurodevelopmental disabilities: A thematic analysis of the literature. Qual. Life Res. 2012, 21, 427–439. [Google Scholar] [CrossRef]
- Dattilo, J.; Schleien, S.J. Understanding leisure services for individuals with mental retardation. Ment. Retard. 1994, 32, 53–59. [Google Scholar]
- Von Elm, E.; Schreiber, G.; Haupt, C.C. Methodische Anleitung für Scoping Reviews (JBI-Methodologie). Z. Für Evidenz Fortbild. Und Qual. Im Gesundh. 2019, 143, 1–7. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Èvid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Felce, D.; Perry, J. Quality of life: Its definition and measurement. Res. Dev. Disabil. 1995, 16, 51–74. [Google Scholar] [CrossRef] [PubMed]
- Schalock, R.L.; Verdugo, M.A.; Gomez, L.E.; Reinders, H.S. Moving Us Toward a Theory of Individual Quality of Life. Am. J. Intellect. Dev. Disabil. 2016, 121, 1–12. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Colquhoun, H.; Garritty, C.M.; Hempel, S.; Horsley, T.; Langlois, E.V.; Lillie, E.; O’Brien, K.K.; Tunçalp, Ö.; et al. Scoping reviews: Reinforcing and advancing the methodology and application. Syst. Rev. 2021, 10, 263. [Google Scholar] [CrossRef]
- World Health Organization International Classification of Diseases 11th Revision. Available online: https://icd.who.int/browse11/l-m/en (accessed on 29 March 2023).
- Askari, S.; Anaby, D.; Bergthorson, M.; Majnemer, A.; Elsabbagh, M.; Zwaigenbaum, L. Participation of Children and Youth with Autism Spectrum Disorder: A Scoping Review. Rev. J. Autism Dev. Disord. 2015, 2, 103–114. [Google Scholar] [CrossRef]
- Steinhardt, F.; Dolva, A.-S.; Jahnsen, R.; Ullenhag, A. Exploring two subdimensions of participation, involvement and engagement: A scoping review. Scand. J. Occup. Ther. 2022, 29, 441–463. [Google Scholar] [CrossRef]
- King, G.; Law, M.; King, S.; Rosenbaum, P.; Kertoy, M.K.; Young, N.L. A Conceptual Model of the Factors Affecting the Recreation and Leisure Participation of Children with Disabilities. Phys. Occup. Ther. Pediatr. 2003, 23, 63–90. [Google Scholar] [CrossRef] [PubMed]
- Maes, B.; Lambrechts, G.; Hostyn, I.; Petry, K. Quality-enhancing interventions for people with profound intellectual and multiple disabilities: A review of the empirical research literature. J. Intellect. Dev. Disabil. 2007, 32, 163–178. [Google Scholar] [CrossRef] [PubMed]
- Pochstein, F. “Sports for All”—An Evaluation of a Community Based Physical Activity Program on the Access to Mainstream Sport for Children with Intellectual Disability. Int. J. Environ. Res. Public Health 2022, 19, 11540. [Google Scholar] [CrossRef] [PubMed]
- Dolva, A.-S.; Kleiven, J.; Kollstad, M. Actual leisure participation of Norwegian adolescents with Down syndrome. J. Intellect. Disabil. 2014, 18, 159–175. [Google Scholar] [CrossRef]
- Dolva, A.; Kollstad, M.; Kleiven, J. Friendships and patterns of social leisure participation among Norwegian adolescents with Down syndrome. J. Appl. Res. Intellect. Disabil. 2019, 32, 1184–1193. [Google Scholar] [CrossRef]
- Taheri, A.; Perry, A.; Minnes, P. Exploring factors that impact activity participation of children and adolescents with severe developmental disabilities. J. Intellect. Disabil. Res. 2017, 61, 1151–1161. [Google Scholar] [CrossRef] [PubMed]
- Solish, A.; Perry, A.; Minnes, P. Participation of Children with and without Disabilities in Social, Recreational and Leisure Activities. J. Appl. Res. Intellect. Disabil. 2010, 23, 226–236. [Google Scholar] [CrossRef]
- Duvdevany, I.; Arar, E. Leisure activities, friendships, and quality of life of persons with intellectual disability: Foster homes vs community residential settings. Int. J. Rehabil. Res. 2004, 27, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Yalon-Chamovitz, S.; Weiss, P.L. (Virtual reality as a leisure activity for young adults with physical and intellectual disabilities. Res. Dev. Disabil. 2008, 29, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Patterson, I.; Pegg, S. Serious leisure and people with intellectual disabilities: Benefits and opportunities. Leis. Stud. 2009, 28, 387–402. [Google Scholar] [CrossRef]
- Lövgren, V.; Bertilsdotter Rosqvist, H. More time for what? Exploring intersecting notions of gender, work, age, and leisure time among people with cognitive disabilities. Int. J. Soc. Welf. 2015, 24, 263–272. [Google Scholar] [CrossRef]
- Hall, S.A. Community Involvement of Young Adults with Intellectual Disabilities: Their Experiences and Perspectives on Inclusion. J. Appl. Res. Intellect. Disabil. 2017, 30, 859–871. [Google Scholar] [CrossRef]
- Mihaila, I.; Handen, B.L.; Christian, B.T.; Hartley, S.L. Leisure activity in middle-aged adults with Down syndrome: Initiators, social partners, settings and barriers. J. Appl. Res. Intellect. Disabil. 2020, 33, 865–875. [Google Scholar] [CrossRef]
- Yu, D.C.T.; Spevack, S.; Hiebert, R.; Martin, T.L.; Goodman, R.; Martin, T.G.; Harapiak, S.; Martin, G.L. Happiness Indices among Persons with Profound and Severe Disabilities during Leisure and Work Activities: A Comparison. Educ. Train. Ment. Retard. Dev. Disabil. 2002, 37, 421–426. Available online: http://www.jstor.org/stable/23880075 (accessed on 28 March 2023).
- Zijlstra, H.P.; Vlaskamp, C. Leisure provision for persons with profound intellectual and multiple disabilities: Quality time or killing time? J. Intellect. Disabil. Res. 2005, 49, 434–448. [Google Scholar] [CrossRef]
- Wilson, P.G.; Reid, D.H.; Green, C.W. Evaluating and increasing in-home leisure activity among adults with severe disabilities in supported independent living. Res. Dev. Disabil. 2006, 27, 93–107. [Google Scholar] [CrossRef] [PubMed]
- van Delden, R.W.; Wintels, S.C.; van Oorsouw, W.M.W.J.; Evers, V.; Embregts, P.J.C.M.; Heylen, D.K.J.; Reidsma, D. Alertness, movement, and affective behaviour of people with profound intellectual and multiple disabilities (PIMD) on introduction of a playful interactive product: Can we get your attention? J. Intellect. Dev. Disabil. 2020, 45, 66–77. [Google Scholar] [CrossRef]
- Beart, S.; Hawkins, D.; Kroese, B.S.; Smithson, P.; Tolosa, I. Barriers to accessing leisure opportunities for people with learning disabilities. Br. J. Learn. Disabil. 2001, 29, 133–138. [Google Scholar] [CrossRef]
- Sellinger, M.H.; Hodapp, R.M.; Dykens, E.M. Leisure Activities of Individuals with Prader-Willi, Williams, and Down Syndromes. J. Dev. Phys. Disabil. 2006, 18, 59–71. [Google Scholar] [CrossRef]
- Azaiza, F.; Rimmerman, A.; Croitoru, T.; Naon, D. Participation in leisure activities by Arab adults with intellectual disabilities living in the community. Int. J. Soc. Welf. 2011, 20, 97–103. [Google Scholar] [CrossRef]
- Dusseljee, J.C.E.; Rijken, P.M.; Cardol, M.; Curfs, L.M.G.; Groenewegen, P.P. Participation in daytime activities among people with mild or moderate intellectual disability. J. Intellect. Disabil. Res. 2011, 55, 4–18. [Google Scholar] [CrossRef]
- Dykens, E.M. Leisure Activities in Prader-Wlli Syndrome: Implications for Health, Cognition and Adaptive Functioning. J. Autism Dev. Disord. 2014, 44, 294–302. [Google Scholar] [CrossRef]
- Venkatesan, S.; Yashodharakumar, G.Y. Leisure and Community Exposure in Persons with Disabilities. J. Disabil. Manag. Spec. Educ. 2016, 6, 1–14. [Google Scholar]
- Gilor, O.; Klibanski, H.; Kfir, D. Implementation and Organisation of Leisure Activities for Children with Disabilities: Coping with Difficulties. Int. J. Disabil. Dev. Educ. 2020, 69, 491–509. [Google Scholar] [CrossRef]
- Vlaskamp, C. Assessing people with profound intellectual and multiple disabilities. In Assessing Adults with Intellectual Disability: A Service Providers’ Guide; Hogg, J., Langa, A., Eds.; Blackwell Publishing: Hoboken, NJ, USA, 2005; pp. 152–163. [Google Scholar]
- Law, M.; Anaby, D.; DeMatteo, C.; Hanna, S. Participation patterns of children with acquired brain injury. Brain Inj. 2011, 25, 587–595. [Google Scholar] [CrossRef]
- Sadan, E. Community Empowerment, Poverty and Leisure Education. In Leisure Education, Community Development and Populations with Special Needs; Sivan, A., Ruskin, H., Eds.; CAB International: Wallingford, UK, 2000; pp. 131–142. [Google Scholar]
- Theuniessen, G.; Wüllenweber, E. Entwicklung von Freizeitkompetenzen für geistig behinderte Menschen mit hohem Unterstützungsbedarf. In Zwischen Tradition und Innovation. Methoden und Handlung-skonzepte in der Heilpädagogik und Behindertenhilfe; Theunissen, G., Wüllenweber, E., Eds.; Lebenshilfe-Verlag: Marburg, Germany, 2009; pp. 81–88. [Google Scholar]
- Markowetz, R. Freizeit von Menschen mit Behinderungen. In Freizeit im Leben Behinderter Menschen: Theoretische Grundlagen und Sozialintegrative Praxis; Markowetz, R., Cloerkes, G., Eds.; Universitätsverlag Winter GmbH Heidelberg: Heidelberg, Germany, 2000; pp. 9–38. [Google Scholar]
- Opaschowski, H.W. Pädagogik und Didaktik der Freizeit; Springer Fachmedien: Wiesbaden, Germany, 1990; pp. 1–216. Available online: https://link.springer.com/book/10.1007/978-3-663-07868-5 (accessed on 29 March 2023).
- Schwartz, S.H. Are there universal aspects in the structure and contents of human values? J. Soc. Issues 1994, 50, 19–45. [Google Scholar] [CrossRef]
- Dattilo, J.; Hoge, G. Project Trail: Leisure Assessment Battery for People with Cognitive Impairments; University of Georgia: Athens, GA, USA, 1997. [Google Scholar]
- Kizony, R.; Katz, N.; Weiss, P.L. Adapting an immersive virtual reality system for rehabilitation. J. Vis. Comput. Animat. 2003, 14, 261–268. [Google Scholar] [CrossRef]
- Witmer, B.G.; Singer, M.J. Measuring presence in virtual environments: A presence questionnaire. Presence Teleoper. Virtual Environ. 1998, 3, 225–240. [Google Scholar] [CrossRef]
- Jopp, D.; Hertzog, C. Activities, self-referent beliefs and cognitive performance: Evidence for direct and mediated effects. Psychol. Aging 2007, 22, 811–825. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heister, N.; Zentel, P.; Köb, S. Participation in Everyday Leisure and Its Influencing Factors for People with Intellectual Disabilities: A Scoping Review of the Empirical Findings. Disabilities 2023, 3, 269-294. https://doi.org/10.3390/disabilities3020018
Heister N, Zentel P, Köb S. Participation in Everyday Leisure and Its Influencing Factors for People with Intellectual Disabilities: A Scoping Review of the Empirical Findings. Disabilities. 2023; 3(2):269-294. https://doi.org/10.3390/disabilities3020018
Chicago/Turabian StyleHeister, Noemi, Peter Zentel, and Stefanie Köb. 2023. "Participation in Everyday Leisure and Its Influencing Factors for People with Intellectual Disabilities: A Scoping Review of the Empirical Findings" Disabilities 3, no. 2: 269-294. https://doi.org/10.3390/disabilities3020018
APA StyleHeister, N., Zentel, P., & Köb, S. (2023). Participation in Everyday Leisure and Its Influencing Factors for People with Intellectual Disabilities: A Scoping Review of the Empirical Findings. Disabilities, 3(2), 269-294. https://doi.org/10.3390/disabilities3020018