
Gender Medicine: A New Possible Frontiers of Venous Thromboembolism


{kind=link}
Abstract
1. Background
2. Men and Women Regarding Thromboembolic Risk
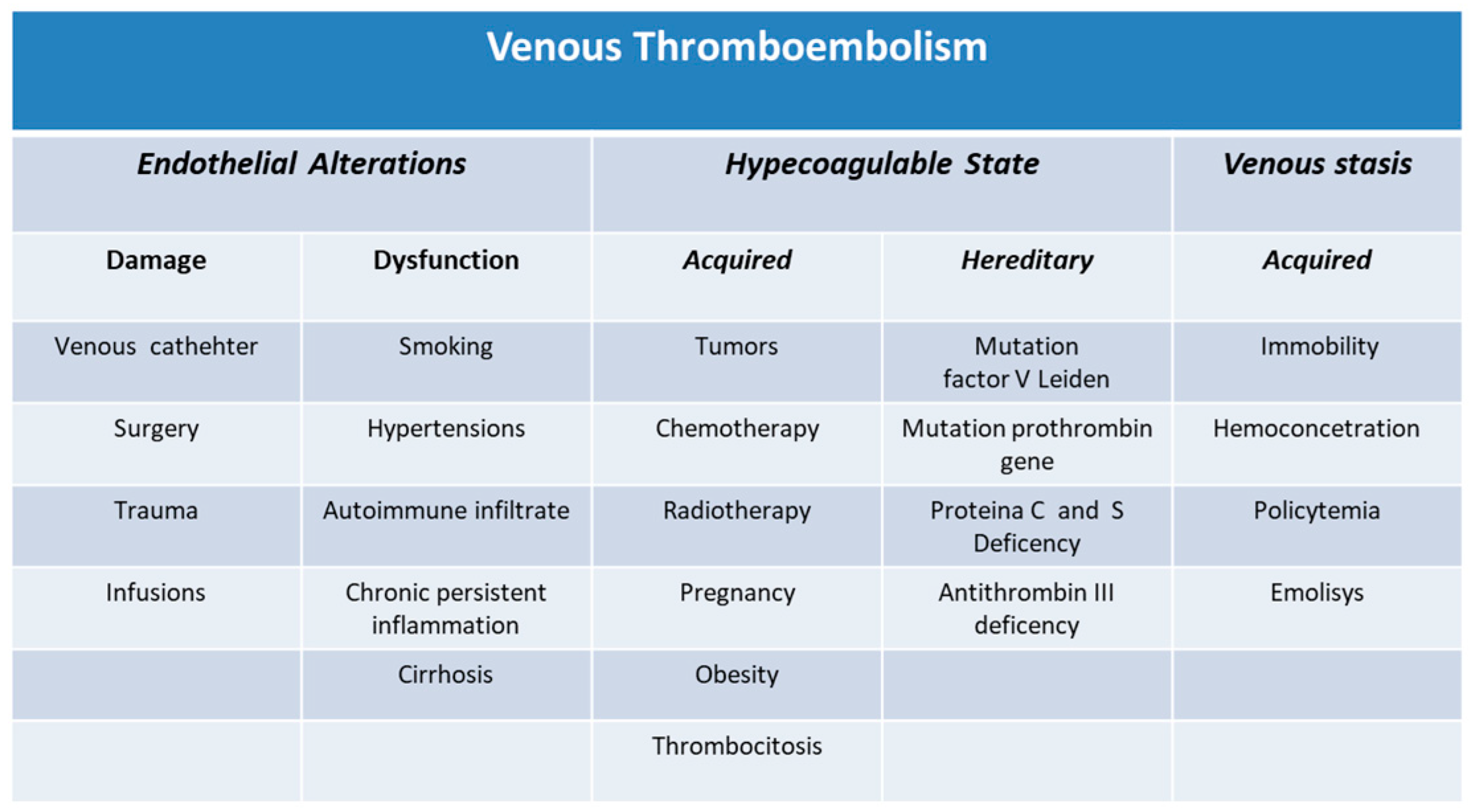
3. Factors Involved in Venous Thromboembolism
3.1. Acquired Predispositions to Thrombosis
3.2. Acquired Predispositions to Thrombosis and Reproductive Factors in Women
3.3. Inherited Predispositions to Thrombosis
Sex Differences in Endothelial Function
4. VTE Outcomes and Gender Differences
5. Superficial VTE and Gender
6. VTE, Cancers, and Gender
VTE and COVID-19 Infection
7. Conclusions
8. Take Home Messages
- Men tend to have a greater risk of having thromboembolism than women;
- At present, the gender differences regarding VTE are not well clarified;
- The relevance of sex hormones in the pathogenesis of VTE is recognized only in some typical situations of the female gender;
- In women, syncope is the condition of PTE onset often linked to hemodynamic instability;
- Women with PTE have higher in-hospital and 30-day mortality due to the advanced age of onset and comorbidities;
- Some cases of idiopathic VTE have revealed occult cancers at follow up;
- Women are predisposed to major bleeding during anticoagulant therapy due to different pharmacokinetics in comparison to men;
- It will be necessary to identify which factors, in both sexes, contribute to VTE.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Roach, R.E.J.; Lijfering, W.M.; Rosendaal, F.R.; Cannegieter, S.C.; le Cessie, S. Sex difference in risk of second but not of first venous thrombosis: Paradox explained. Circulation 2014, 129, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.A., Jr.; Spencer, F.A. Risk factors for venous thromboembolism. Circulation 2003, 107, I-9-16. [Google Scholar] [CrossRef] [PubMed]
- Giustozzi, M.; Valerio, L.; Agnelli, G.; Becattini, C.; Fronk, E.-M.; Klok, F.A.; Konstantinides, S.V.; Vedovati, M.C.; Cohen, A.T.; Barco, S. Sex-specific differences in the presentation, clinical course, and quality of life of patients with acute venous thromboembolism according to baseline risk factors. Insights from the PREFER in VTE. Eur. J. Intern. Med. 2021, 88, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Kobbervig, C.E.; James, A.H.; Petterson, T.M.; Bailey, K.R.; Melton, L.J. Trends in the Incidence of Venous Thromboembolism during Pregnancy or Postpartum: A 30-Year Population-Based Study. Ann. Intern. Med. 2005, 143, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Mannucci, P.M. Classic thrombophilic gene variants. Thromb. Haemost. 2015, 114, 885–889. [Google Scholar] [CrossRef]
- Croles, F.N.; Nasserinejad, K.; Duvekot, J.J.; Kruip, M.J.; Meijer, K.; Leebeek, F.W. Pregnancy, thrombophilia, and the risk of a first venous thrombosis: Systematic review and bayesian meta-analysis. BMJ 2017, 359, j4452. [Google Scholar] [CrossRef]
- Arnesen, C.A.L.; Veres, K.; Horváth-Puhó, E.; Hansen, J.-B.; Sørensen, H.T.; Brækkan, S.K. Estimated lifetime risk of venous thromboembolism in men and women in a Danish nationwide cohort: Impact of competing risk of death. Eur. J. Epidemiol. 2022, 37, 195–203. [Google Scholar] [CrossRef]
- Arshad, N.; Isaksen, T.; Hansen, J.-B.; Brækkan, S.K. Time trends in incidence rates of venous thromboembolism in a large cohort recruited from the general population. Eur. J. Epidemiol. 2017, 32, 299–305. [Google Scholar] [CrossRef]
- Næss, I.A.; Christiansen, S.C.; Romundstad, P.; Cannegieter, S.C.; Rosendaal, F.R.; Hammerstrøm, J. Incidence and mortality of venous thrombosis: A population-based study. J. Thromb. Haemost. 2007, 5, 692–699. [Google Scholar] [CrossRef]
- Alotaibi, G.S.; Wu, C.; Senthilselvan, A.; McMurtry, M.S. Secular trends in incidence and mortality of acute venous thromboembolism: The AB-VTE population-based study. Am. J. Med. 2016, 129, 879.e19–879.e25. [Google Scholar] [CrossRef]
- Kort, D.; van Rein, N.; van der Meer, F.J.M.; Vermaas, H.W.; Wiersma, N.; Cannegieter, S.C.; Lijfering, W.M. Relationship between neighborhood socioeconomic status and venous thromboembolism: Results from a population-based study. J. Thromb. Haemost. 2017, 15, 2352–2360. [Google Scholar] [CrossRef] [PubMed]
- McHugh, K.B.; Visani, L.; DeRosa, M.; Covezzoli, A.; Rossi, E.; Goldhaber, S.Z. Gender comparisons in pulmonary embolism (results from the International Cooperative Pulmonary Embolism Registry [ICOPER]). Am. J. Cardiol. 2002, 89, 616–619. [Google Scholar] [CrossRef]
- Barrios, D.; Morillo, R.; Guerassimova, I.; Barbero, E.; Escobar-Morreale, H.; Cohen, A.T.; Becattini, C.; Tapson, V.; Yusen, R.; Jimenez, D. Sex differences in the characteristics and short-term prognosis of patients presenting with acute symptomatic pulmonary embolism. PLoS ONE 2017, 12, e0187648. [Google Scholar] [CrossRef] [PubMed]
- Ortel, T.L.; Neumann, I.; Ageno, W.; Beyth, R.; Clark, N.P.; Cuker, A.; Hutten, B.A.; Jaff, M.R.; Manja, V.; Schulman, S.; et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: Treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020, 4, 4693–4738. [Google Scholar] [CrossRef]
- Heit, J.A.; Spencer, F.A.; White, R.H. The epidemiology of venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 3–14. [Google Scholar] [CrossRef]
- Roach, R.E.J.; Cannegieter, S.C.; Lijfering, W.M. Differential risks in men and women for first and recurrent venous thrombosis: The role of genes and environment. J. Thromb. Haemost. 2014, 12, 1593–1600. [Google Scholar] [CrossRef]
- Braekkan, S.K.; Borch, K.H.; Mathiesen, E.B.; Njølstad, I.; Wilsgaard, T.; Hansen, J.-B. Body Height and Risk of Venous Thromboembolism: The Tromso Study. Am. J. Epidemiol. 2010, 171, 1109–1115. [Google Scholar] [CrossRef]
- Eurofound and European Commission Joint Research Centre. European jobs monitor 2021: Gender gaps and the employment structure. In European Jobs Monitor Series; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar]
- Johansson, E.; Mathiassen, S.E.; Rasmusse, C.L.; Hallman, D.M. Sitting, standing and moving during work and leisure among male and female office workers of different age: A compositional data analysis. BMC Public Health 2020, 20, 826. [Google Scholar] [CrossRef]
- Stein, P.D.; Beemath, A.; Olson, R.E. Trends in the incidence of pulmonary embolism and deep vein thrombosis in hospitalized patients. Am. J. Cardiol. 2005, 95, 1525–1526. [Google Scholar] [CrossRef]
- Severinsen, M.T.; Kristensen, S.R.; Johnsen, S.P.; Dethlefsen, C.; Tjønneland, A.; Overvad, K. Smoking and venous thromboembolism: A Danish follow-up study. J. Thromb. Haemost. 2009, 7, 1297–1303. [Google Scholar] [CrossRef]
- Kuipers, S.; Cannegieter, S.C.; Middeldorp, S.; Robyn, L.; Büller, H.R.; Rosendaal, F.R. The Absolute Risk of Venous Thrombosis after Air Travel: A Cohort Study of 8,755 Employees of International Organisations. PLoS Med. 2007, 4, e290. [Google Scholar] [CrossRef] [PubMed]
- Holmegard, H.N.; Nordestgaard, B.G.; Schnohr, P.; Tybjaerg-Hansen, A.; Benn, M. Endogenous sex hormones and risk of venous thromboembolism in women and men. J. Thromb. Haemost. 2014, 12, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Roetker, N.; MacLehose, R.; Hoogeveen, R.; Ballantyne, C.M.; Basu, S.; Cushman, M.; Folsom, A.R. Prospective study of endogenous hormones and incidence of venous thromboembolism: The atherosclerosis risk in communities study. Thromb. Haemost. 2018, 118, 1940–1950. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.D.; Beemath, A.; Olson, R.E. Obesity as a risk factor in venous thromboembolism. Am. J. Med. 2005, 118, 978–980. [Google Scholar] [CrossRef]
- Steffen, L.M.; Cushman, M.; Peacock, J.M.; Heckbert, S.R.; Jacobs, D.R., Jr.; Rosamond, W.D.; Folsom, A.R. Metabolic syndrome and risk of venous thromboembolism: Longitudinal Investigation of Thromboembolism Etiology. J. Thromb. Haemost. 2009, 7, 746–751. [Google Scholar] [CrossRef]
- Siegerink, B.; Lijfering, W.M.; Hansen, J.-B.; Cannegieter, S.C.; Rosendaal, F.R.; Braekkan, S.K. Role of Obesity in the Etiology of Deep Vein Thrombosis and Pulmonary Embolism: Current Epidemiological Insights. Semin. Thromb. Hemost. 2013, 39, 533–540. [Google Scholar] [CrossRef]
- Morelli, V.M.; de Mutsert, R.; de Roos, A.; Lamb, H.J.; Vlieg, A.v.; Bos, M.H.A.; Rosendaal, F.R.; Lijfering, W.M.; Cannegieter, S.C. Association between hepatic triglyceride content and coagulation factors: The Netherlands epidemiology of obesity study. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 3004–3014. [Google Scholar] [CrossRef]
- Lawler, P.R.; Bhatt, D.L.; Godoy, L.C.; Lüscher, T.F.; Bonow, R.O.; Verma, S.; Ridker, P.M. Targeting cardiovascular inflammation: Next steps in clinical translation. Eur. Heart J. 2020, 42, 113–131. [Google Scholar] [CrossRef]
- Roach, R.E.J.; Lijfering, W.M.; Flinterman, L.E.; Rosendaal, F.R.; Cannegieter, S.C. Increased risk of CVD after VT is determined by common etiologic factors. Blood 2013, 121, 4948–4954. [Google Scholar] [CrossRef]
- Minno, M.N.D.D.; Tufano, A.; Russolillo, A.; Minno, G.D.; Tarantino, G. High prevalence of nonalcoholic fatty liver in patients with idiopathic venous thromboembolism. World J. Gastroenterol. 2010, 16, 6119–6122. [Google Scholar] [CrossRef]
- Camhi, S.M.; Bray, G.A.; Bouchard, C.; Greenway, F.L.; Johnson, W.; Newton, R.; Ravussin, E.; Ryan, D.; Smith, S.R.; Katzmarzyk, P.T. The Relationship of Waist Circumference and BMI to Visceral, Subcutaneous, and Total Body Fat: Sex and Race Differences. Obesity 2011, 19, 402–408. [Google Scholar] [CrossRef]
- Robert-Ebadi, H.; Le Gal, G.; Carrier, M.; Couturaud, F.; Perrier, A.; Bounameaux, H.; Righini, M. Differences in clinical presentation of pulmonary embolism in women and men. J. Thromb. Haemost. 2010, 8, 693–698. [Google Scholar] [CrossRef]
- Douxfils, J.; Morimont, L.; Bouvy, C. Oral Contraceptives and Venous Thromboembolism: Focus on Testing that May Enable Prediction and Assessment of the Risk. Semin. Thromb. Hemost. 2020, 46, 872–886. [Google Scholar] [CrossRef]
- Bukhari, S.; Fatima, S.; Barakat, A.F.; Fogerty, A.E.; Weinberg, I.; Elgendy, I.Y. Venous thromboembolism during pregnancy and postpartum period. Eur. J. Intern. Med. 2021, 97, 8–17. [Google Scholar] [CrossRef]
- Martinelli, I.; De Stefano, V.; Mannucci, P.M. Inherited risk factors for venous thromboembolism. Nat. Rev. Cardiol. 2014, 11, 140–156. [Google Scholar] [CrossRef] [PubMed]
- Zöller, B.; Svensson, P.J.; Dahlbäck, B.; Lind-Hallden, C.; Hallden, C.; Elf, J. Genetic risk factors for venous thromboembolism. Expert Rev. Hematol. 2020, 13, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Koster, T.; Vandenbroucke, J.P.; Rosendaal, F.R.; Briët, E.; Rosendaal, F.R.; Blann, A.D. Role of clotting factor VIII in effect of von Willebrand factor on occurrence of deep-vein thrombosis. Lancet 1995, 345, 152–155. [Google Scholar] [CrossRef]
- van Hylckama, V.A.; van der Linden, I.K.; Bertina, R.M.; Rosendaal, F.R. High levels of factor IX increase the risk of venous thrombosis. Blood 2000, 95, 3678–3682. [Google Scholar]
- Graw, J.; Brackmann, H.-H.; Oldenburg, J.; Schneppenheim, R.; Spannagl, M.; Schwaab, R. Haemophilia A: From mutation analysis to new therapies. Nat. Rev. Genet. 2005, 6, 488–501. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, M.I.; Grossmann, V.; Spronk, H.M.H.; Schulz, A.; Jünger, C.; Laubert-Reh, D.; Mazur, J.; Gori, T.; Zeller, T.; Pfeiffer, N.; et al. Distribution, genetic and cardiovascular determinants of FVIII:c—Data from the population-based Gutenberg Health Study. Int. J. Cardiol. 2015, 187, 166–174. [Google Scholar] [CrossRef] [PubMed]
- de Haan, H.G.; Vlieg, A.V.H.; van der Gaag, K.J.; de Knijff, P.; Rosendaal, F.R. Male-specific risk of first and recurrent venous thrombosis: A phylogenetic analysis of the Y chromosome. J. Thromb. Haemost. 2016, 14, 1971–1977. [Google Scholar] [CrossRef] [PubMed]
- Barco, S.; Nijkeuter, M.; Middeldorp, S. Pregnancy and venous thromboembolism. Semin. Thromb. Hemost. 2013, 39, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Dumesic, D.A.; Oberfield, S.E.; Stener-Victorin, E.; Marshall, J.C.; Laven, J.S.; Legro, R.S. Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr. Rev. 2015, 36, 487–525. [Google Scholar] [CrossRef] [PubMed]
- McCartney, C.R.; Marshall, J.C. Polycystic ovary syndrome. N. Engl. J. Med. 2016, 375, 54–64. [Google Scholar] [CrossRef]
- Peng, Z.; Sun, Y.; Lv, X.; Zhang, H.; Liu, C.; Dai, S. Interleukin-6 Levels in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0148531. [Google Scholar] [CrossRef]
- Schiffer, L.; Kempegowda, P.; Arlt, W.; O’Reilly, M.W. Mechanisms in endocrinology: The sexually dimorphic role of androgens in human metabolic disease. Eur. J. Endocrinol. 2017, 177, R125–R143. [Google Scholar] [CrossRef] [PubMed]
- Scicchitano, P.; Dentamaro, I.; Carbonara, R.; Bulzis, G.; Dachille, A.; Caputo, P.; Riccardi, R.; Locorotondo, M.; Mandurino, C.; Ciccone, M.M. Cardiovascular Risk in Women with PCOS. Int. J. Endocrinol. Metab. 2012, 10, 611–618. [Google Scholar] [CrossRef]
- Stanhewicz, A.; Wenner, M.M.; Stachenfeld, N.S. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am. J. Physiol. Circ. Physiol. 2018, 315, H1569–H1588. [Google Scholar] [CrossRef]
- Boese, A.C.; Kim, S.C.; Yin, K.-J.; Lee, J.-P.; Hamblin, M.H. Sex differences in vascular physiology and pathophysiology: Estrogen and androgen signaling in health and disease. Am. J. Physiol. Circ. Physiol. 2017, 313, H524–H545. [Google Scholar] [CrossRef]
- Cooke, P.S.; Nanjappa, M.K.; Ko, C.; Prins, G.S.; Hess, R.A. Estrogens in Male Physiology. Physiol. Rev. 2017, 97, 995–1043. [Google Scholar] [CrossRef]
- Pearson, L.J.; Yandle, T.G.; Nicholls, M.G.; Evans, J.J. Regulation of endothelin-1 release from human endothelial cells by sex steroids and angiotensin-II. Peptides 2008, 29, 1057–1061. [Google Scholar] [CrossRef] [PubMed]
- Wenner, M.M.; Sebzda, K.N.; Kuczmarski, A.V.; Pohlig, R.T.; Edwards, D.G. ETB receptor contribution to vascular dysfunction in postmenopausal women. Am. J. Physiol. Integr. Comp. Physiol. 2017, 313, R51–R57. [Google Scholar] [CrossRef] [PubMed]
- Westby, C.M.; Weil, B.R.; Greiner, J.J.; Stauffer, B.; Desouza, C.A. Endothelin-1 vasoconstriction and the age-related decline in endothelium-dependent vasodilatation in men. Clin. Sci. 2011, 120, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Flinterman, L.E.; Vlieg, A.V.H.; Rosendaal, F.R.; Cannegieter, S.C. Body height, mobility, and risk of first and recurrent venous thrombosis. J. Thromb. Haemost. 2015, 13, 548–554. [Google Scholar] [CrossRef]
- Agarwal, S.; Clark, D., III; Karan Sud, J.; Cho, L.; Menon, V. Gender disparities in outcomes and resource utilization for acute pulmonary embolism hospitalizations in theUnited States. Am. J. Cardiol. 2015, 116, 1270–1276. [Google Scholar] [CrossRef]
- Mansour, S.; Alotaibi, G.; Wu, C.; Alsaleh, K.; McMurtry, M.S. Sex disparities in hospitalization and mortality rates for venous thromboembolism. J. Thromb. Thrombolysis 2017, 44, 197–202. [Google Scholar] [CrossRef]
- Loffredo, L.; Violi, F.; Perri, L. Sex-related differences in patients with acute venous thromboembolism treated with new oral anticoagulants. A meta-analysis of the interventional trials. Int. J. Cardiol. 2016, 212, 255–258. [Google Scholar] [CrossRef]
- Raccah, B.H.; Amichai, P.; Donna, R.Z.; Hochberg-Klein, S.; Masarwa, R.; Muszkat, M.; Matok, I. Gender differences in efficacy and safety of direct oral anticoagulants in atrial fibrillation: Systematic review and network meta-analysis. Ann. Pharmacother. 2018, 52, 1135–1142. [Google Scholar] [CrossRef]
- Dentali, F.; Sironi, A.P.; Gianni, M.; Orlandini, F.; Guasti, L.; Grandi, A.M.; Franchini, M.; Ageno, W.; Squizzato, A. Gender difference in efficacy and safety of nonvitamin k antagonist oral anticoagulants in patients with nonvalvular atrial fibrillation or venous thromboembolism: A systematic review and a meta-analysis of the literature. Semin. Thromb. Hemost. 2015, 41, 774–787. [Google Scholar]
- Douketis, J.; Tosetto, A.; Marcucci, M.; Baglin, T.; Cosmi, B.; Cushman, M.; Kyrle, P.; Poli, D.; Tait, R.C.; Iorio, A. Risk of recurrence after venous thromboembolism in men and women: Patient level meta-analysis. BMJ 2011, 342, d813. [Google Scholar] [CrossRef]
- Blanco-Molina, A.; Enea, I.; Gadelha, T.; Tufano, A.; Bura-Riviere, A.; Di Micco, P.; Bounameaux, H.; González, J.; Villalta, J.; Monreal, M. Sex Differences in Patients Receiving Anticoagulant Therapy for Venous Thromboembolism. Medicine 2014, 93, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A. Predicting the risk of venous thromboembolism recurrence. Am. J. Hematol. 2012, 87 (Suppl. S1), S63–S67. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Parpia, S.; Spencer, F.A.; Schulman, S.; Stevens, S.M.; Shah, V.; Bauer, K.A.; Douketis, J.D.; Lentz, S.R.; Kessler, C.M.; et al. Long-term risk of recurrence in patients with a first unprovoked venous thromboembolism managed according to d-dimer results; A cohort study. J. Thromb. Haemost. 2019, 17, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Tosetto, A.; Iorio, A.; Marcucci, M.; Eichinger, S.; Palareti, G.; Poli, D.; Tait, R.C.; Douketis, J. Predicting disease recurrence in patients with previous unprovoked venous thromboembolism: A proposed prediction score (DASH). J. Thromb. Haemost. 2012, 10, 1019–1025. [Google Scholar] [CrossRef]
- Carrier, M.; Blais, N.; Crowther, M.; Kavan, P.; Le Gal, G.; Moodley, O.; Shivakumar, S.; Suryanarayan, D.; Tagalakis, V.; Wu, C.; et al. Treatment Algorithm in Cancer-Associated Thrombosis: Updated Canadian Expert Consensus. Curr. Oncol. 2021, 28, 5434–5451. [Google Scholar] [CrossRef]
- Ferroni, P.; Guadagni, F.; Roselli, M. Risk Prediction and New Prophylaxis Strategies for Thromboembolism in Cancer. Cancers 2021, 13, 1556. [Google Scholar] [CrossRef]
- Nasser, N.; Fox, J.; Agbarya, A. Potential Mechanisms of Cancer-Related Hypercoagulability. Cancers 2020, 12, 566. [Google Scholar] [CrossRef]
- Galanaud, J.P.; Bosson, J.L.; Genty, C.; Presles, E.; Cucherat, M.; Sevestre, M.A.; Quere, I.; Decousus, H.; Leizorovicz, A. Superficial vein thrombosis and recurrent venous thromboembolism: A pooled analysis of two observational studies. J. Thromb. Haemost. 2012, 10, 1004–1011. [Google Scholar] [CrossRef]
- Cannegieter, S.C.; Horváth-Puhó, E.; Schmidt, M.; Dekkers, O.M.; Pedersen, L.; Vandenbroucke, J.P.; Sørensen, H.T. Risk of venous and arterial thrombotic events in patients diagnosed with superficial vein thrombosis: A nationwide cohort study. Blood 2015, 125, 229–235. [Google Scholar] [CrossRef]
- Decousus, H.; Quéré, I.; Presles, E.; Becker, F.; Barrellier, M.T.; Chanut, M.; Gillet, J.L.; Guenneguez, H.; Leandri, C.; Mismetti, P.; et al. Superficial vein thrombosis and venous thromboembolism: A large prospective epidemiological study. Ann. Intern. Med. 2010, 152, 218–224. [Google Scholar] [CrossRef]
- Frappé, P.; Buchmuller-Cordier, A.; Bertoletti, L.; Bonithon-Kopp, C.; Couzan, S.; Lafond, P.; Leizorovicz, A.; Merah, A.; Presles, E.; Preynat, P.; et al. Annual diagnosis rate of superficial vein thrombosis of the lower limbs: The STEPH community-based study. J. Thromb. Haemost. 2014, 12, 831–838. [Google Scholar] [CrossRef] [PubMed]
- van Royen, F.S.; van Smeden, M.; Moons, K.G.M.; Rutten, F.H.; Geersing, G.J. Management of superficial venous thrombosis based on individual risk profiles: Protocol for the development and validation of three prognostic prediction models in large primary care cohorts. Diagn. Progn. Res. 2021, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, M.N.D.; Ambrosino, P.; Ambrosini, F.; Tremoli, E.; Di Minno, G.; Dentali, F. Prevalence of deep vein thrombosis and pulmonary embolism in patients with superficial vein thrombosis: A systematic review and meta-analysis. J. Thromb. Haemost. 2016, 14, 964–972. [Google Scholar] [CrossRef]
- Pomero, F.; Di Minno, M.; Premunian, E.T.; Malato, A.; Pasca, S.; Barillari, G.; Fenoglio, L.; Siragusa, S.; Di Minno, G.; Ageno, W.; et al. A clinical score to rule out the concomitant presence of deep vein thrombosis in patients presenting with superficial vein thrombosis: The ICARO study. Thromb. Res. 2015, 136, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Riondino, S.; Guadagni, F.; Formica, V.; Ferroni, P.; Roselli, M.; Riondino, F.G.S. Gender Differences in Cancer-associated Venous Thromboembolism. Curr. Med. Chem. 2017, 24, 2589–2601. [Google Scholar] [CrossRef]
- Cohen, A.; Lim, C.S.; Davies, A.H. Venous Thromboembolism in Gynecological Malignancy. Int. J. Gynecol. Cancer 2017, 27, 1970–1978. [Google Scholar] [CrossRef]
- Tasaka, N.; Minaguchi, T.; Hosokawa, Y.; Takao, W.; Itagaki, H.; Nishida, K.; Akiyama, A.; Shikama, A.; Ochi, H.; Satoh, T. Prevalence of venous thromboembolism at pretreatment screening and associated risk factors in 2086 patients with gynecological cancer. J. Obstet. Gynaecol. Res. 2020, 46, 765–773. [Google Scholar] [CrossRef]
- Bleau, N.; Patenaude, V.; Abenhaim, H.A. Risk of venous thrombo-embolic events in pregnant patients with cancer. J. Matern. Neonatal Med. 2016, 29, 380–384. [Google Scholar] [CrossRef]
- Greiber, I.K.; Mikkelsen, A.P.; Karlsen, M.A.; Storgaard, L.; Viuff, J.; Mellemkjær, L.; Hjortshøj, C.S.; Hjortshøj, Ø. Cancer in pregnancy increases the risk of venous thromboembolism: A nationwide cohort study. BJOG Int. J. Obstet. Gynaecol. 2020, 128, 1151–1159. [Google Scholar] [CrossRef]
- Farge, D.; Bounameauxb, H.; Bauersachscd, R.M.; Brennere, B. Women, thrombosis, and cancer: A gender-specific analysis. Thromb. Res. 2017, 151, S21–S29. [Google Scholar] [CrossRef]
- Jara-Palomares, L.; Otero, R.; Jiménez, D.; Praena-Fernández, J.M.; Rivas, A.; Font, C.; Wells, P.S.; López-Reyes, R.; González-Martínez, J.; Monreal, M. Sex Differences in Patients with Occult Cancer After Venous Thromboembolism. Clin. Appl. Thromb. 2017, 24, 489–495. [Google Scholar] [CrossRef]
- Schmidt, M.; Horvath-Puho, E.; Thomsen, R.; Smeeth, L.; Sørensen, H.T. Acute infections and venous thromboembolism. J. Intern. Med. 2011, 271, 608–618. [Google Scholar] [CrossRef]
- Connolly-Andersen, A.-M.; Whitaker, H.; Klingström, J.; Ahlm, C. Risk of Venous Thromboembolism Following Hemorrhagic Fever with Renal Syndrome: A Self-controlled Case Series Study. Clin. Infect. Dis. 2017, 66, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Magadum, A.; Kishore, R. Cardiovascular Manifestations of COVID-19 Infection. Cells 2020, 9, 2508. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; O’Donnell, J.S.; Sharif, K.; Emery, P.; Bridgewood, C. Immune mechanisms of pulmonary intravascular coagulopathy in COVID-19 pneumonia. Lancet Rheumatol. 2020, 2, e437–e445. [Google Scholar] [CrossRef]
- Zhou, X.; Cheng, Z.; Luo, L.; Zhu, Y.; Lin, W.; Ming, Z.; Chen, W.; Hu, Y. Incidence and impact of disseminated intravascular coagulation in COVID-19 a systematic review and meta-analysis. Thromb. Res. 2021, 201, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Patone, M.; Mei, X.W.; Saatci, D.; Dixon, S.; Khunti, K.; Zaccardi, F.; Watkinson, P.; Shankar-Hari, M.; Doidge, J.; et al. Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: Self-controlled case series study. BMJ 2021, 374, n1931. [Google Scholar] [CrossRef]
- Mansory, E.M.; Srigunapalan, S.; Lazo-Langner, A. Venous Thromboembolism in Hospitalized Critical and Noncritical COVID-19 Patients: A Systematic Review and Meta-analysis. TH Open 2021, 05, e286–e294. [Google Scholar] [CrossRef]
- Mai, V.; Tan, B.K.; Mainbourg, S.; Potus, F.; Cucherat, M.; Lega, J.-C.; Provencher, S. Venous thromboembolism in COVID-19 compared to non-COVID-19 cohorts: A systematic review with meta-analysis. Vasc. Pharmacol. 2021, 139, 106882. [Google Scholar] [CrossRef]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Jerndal, H.; Lundevaller, E.H.; Sund, M.; Lindmark, K.; Connolly, A.-M.F. Risks of deep vein thrombosis, pulmonary embolism, and bleeding after covid-19: Nationwide self-controlled cases series and matched cohort study. BMJ 2022, 377, e069590. [Google Scholar] [CrossRef] [PubMed]
- Kalita, J.; Misra, U.K.; Singh, V.K.; Kumar, S.; Jain, N. Does gender difference matter in cerebral venous thrombosis? J. Clin. Neurosci. 2022, 102, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Gazioglu, S.; Dinc, G. Cerebral venous sinus thrombosis in pregnancy and puerperium. Acta Neurol. Belg. 2020, 121, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Spadaro, A.; Scott, K.R.; Koyfman, A.; Long, B. Cerebral venous thrombosis: Diagnosis and management in the emergency department setting. Am. J. Emerg. Med. 2021, 47, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Gangat, N.; Guglielmelli, P.; Betti, S.; Farrukh, F.; Msc, A.C.; Barbui, T.; Vannucchi, A.M.; De Stefano, V.; Tefferi, A. Cerebral venous thrombosis and myeloproliferative neoplasms: A three-center study of 74 consecutive cases. Am. J. Hematol. 2021, 96, 1580–1586. [Google Scholar] [CrossRef]
- Castiglione, M.; Jiang, Y.P.; Mazzeo, C.; Lee, S.; Chen, J.S.; Kaushansky, K.; Yin, W.; Lin, R.Z.; Zheng, H.; Zhan, H. Endothelial JAK2V617F mutation leads to thrombosis, vasculopathy, and cardiomyopathy in a murine model of myeloproliferative neoplasm. J. Thromb. Haemost. 2020, 18, 3359–3370. [Google Scholar] [CrossRef]
- Rizk, J.G.; Gupta, A.; Sardar, P.; Henry, B.M.; Lewin, J.C.; Lippi, G.; Lavie, C.J. Clinical Characteristics and Pharmacological Management of COVID-19 Vaccine–Induced Immune Thrombotic Thrombocytopenia with Cerebral Venous Sinus Thrombosis. JAMA Cardiol. 2021, 6, 1451. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciarambino, T.; Crispino, P.; Para, O.; Giordano, M. Gender Medicine: A New Possible Frontiers of Venous Thromboembolism. Stresses 2023, 3, 167-181. https://doi.org/10.3390/stresses3010013
Ciarambino T, Crispino P, Para O, Giordano M. Gender Medicine: A New Possible Frontiers of Venous Thromboembolism. Stresses. 2023; 3(1):167-181. https://doi.org/10.3390/stresses3010013
Chicago/Turabian StyleCiarambino, Tiziana, Pietro Crispino, Ombretta Para, and Mauro Giordano. 2023. "Gender Medicine: A New Possible Frontiers of Venous Thromboembolism" Stresses 3, no. 1: 167-181. https://doi.org/10.3390/stresses3010013
APA StyleCiarambino, T., Crispino, P., Para, O., & Giordano, M. (2023). Gender Medicine: A New Possible Frontiers of Venous Thromboembolism. Stresses, 3(1), 167-181. https://doi.org/10.3390/stresses3010013