
Females Present Different Single-Leg Squat Kinematics and Muscle Activation Strategies than Males Even after Hip Abductor Fatigue

 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Experimental Design
2.2. Participants
3. Procedures
3.1. Maximal Voluntary Isometric Contractions
3.2. EMG Data Acquisition
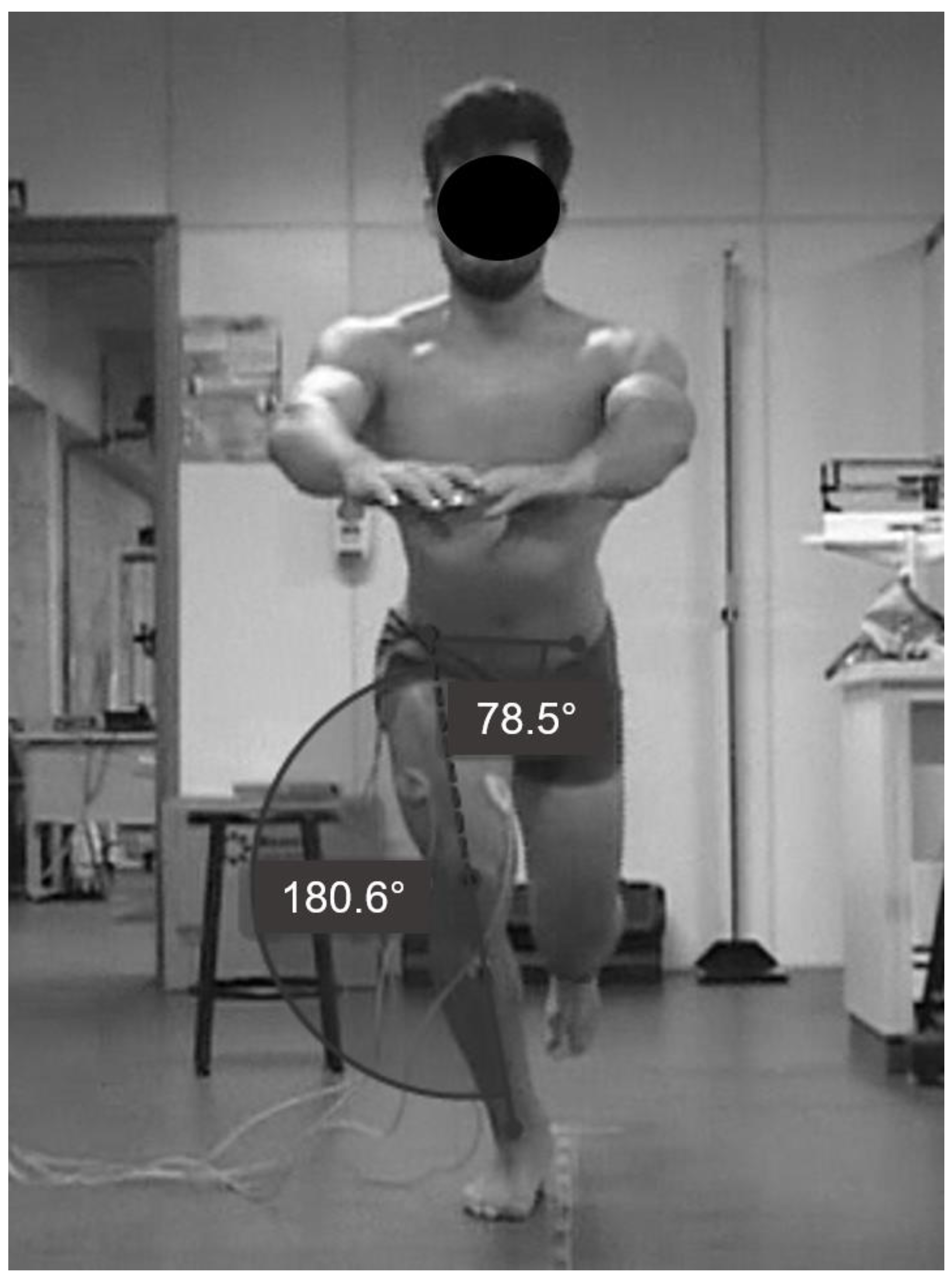
3.3. Frontal Plane Kinematics during Single-Leg Squat
3.4. Estimated 1RM
3.5. Isometric Sustained Hip Abductor Fatigue Protocol
4. Data Analysis
5. Statistical Analysis
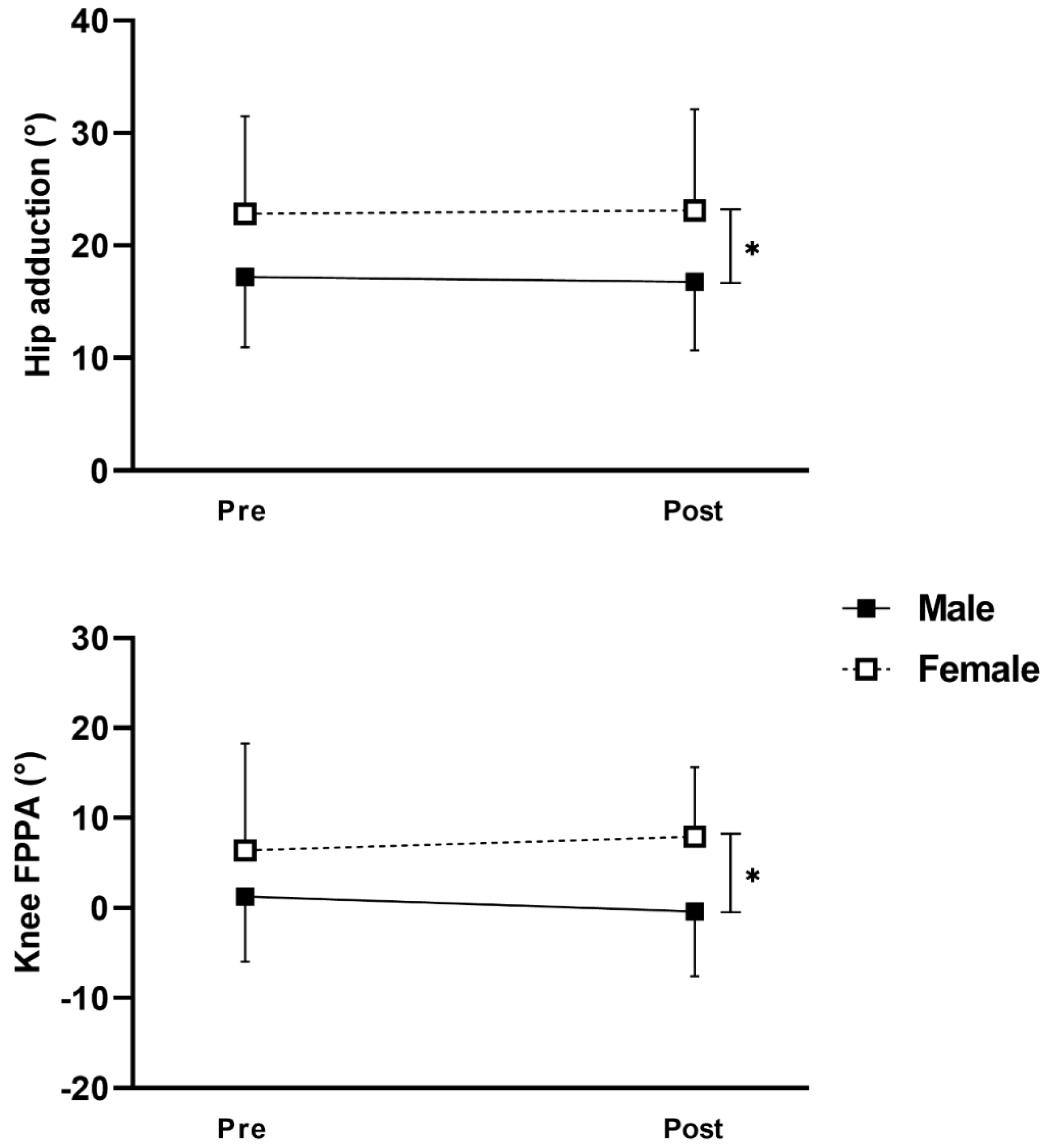
6. Results
7. Discussion
8. Conclusions
9. Declarations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rodrigues, R.; Daiana Klein, K.; Dalcero Pompeo, K.; Aurélio Vaz, M. Are there neuromuscular differences on proximal and distal joints in patellofemoral pain people? A systematic review and meta-analysis. J. Electromyogr. Kinesiol. 2022, 64, 102657. [Google Scholar] [CrossRef] [PubMed]
- Petersen, W.; Taheri, P.; Forkel, P.; Zantop, T. Return to play following ACL reconstruction: A systematic review about strength deficits. Arch. Orthop. Trauma. Surg. 2014, 134, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Pompeo, K.D.; da Rocha, E.S.; Melo, M.A.; de Oliveira, N.T.; Oliveira, D.F.; Sonda, F.C.; Dos Santos, P.F.; Rodrigues, R.; Baroni, B.M.; Vaz, M.A. Can we replace exercises targeted on core/hip muscles by exercises targeted on leg/foot muscles in women with patellofemoral pain? A randomized controlled trial. Phys. Ther. Sport 2022, 58, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Neumann, D.A. Kinesiology of the hip: A focus on muscular actions. J. Orthop. Sports Phys. Ther. 2010, 40, 82–94. [Google Scholar] [CrossRef]
- Maniar, N.; Schache, A.G.; Pizzolato, C.; Opar, D.A. Muscle contributions to tibiofemoral shear forces and valgus and rotational joint moments during single leg drop landing. Scand. J. Med. Sci. Sports 2020, 30, 1664–1674. [Google Scholar] [CrossRef] [PubMed]
- Ebert, J.R.; Edwards, P.K.; Fick, D.P.; Janes, G.C. A Systematic Review of Rehabilitation Exercises to Progressively Load the Gluteus Medius. J. Sport Rehabil. 2017, 26, 418–436. [Google Scholar] [CrossRef] [PubMed]
- Neamatallah, Z.; Herrington, L.; Jones, R. An investigation into the role of gluteal muscle strength and EMG activity in controlling HIP and knee motion during landing tasks. Phys. Ther. Sport 2020, 43, 230–235. [Google Scholar] [CrossRef]
- Jacobs, C.A.; Uhl, T.L.; Mattacola, C.G.; Shapiro, R.; Rayens, W.S. Hip abductor function and lower extremity landing kinematics: Sex differences. J. Athl. Train. 2007, 42, 76–83. [Google Scholar] [PubMed]
- Lee, S.P.; Powers, C. Fatigue of the hip abductors results in increased medial-lateral center of pressure excursion and altered peroneus longus activation during a unipedal landing task. Clin. Biomech. 2013, 28, 524–529. [Google Scholar] [CrossRef]
- Gafner, S.C.; Hoevel, V.; Punt, I.M.; Schmid, S.; Armand, S.; Allet, L. Hip-abductor fatigue influences sagittal plane ankle kinematics and shank muscle activity during a single-leg forward jump. J. Electromyogr. Kinesiol. 2018, 43, 75–81. [Google Scholar] [CrossRef]
- Dury, J.; Michel, F.; Ravier, G. Fatigue of hip abductor muscles implies neuromuscular and kinematic adaptations of the ankle during dynamic balance. Scand. J. Med. Sci. Sports 2022, 32, 1324–1334. [Google Scholar] [CrossRef] [PubMed]
- Viggiani, D.; Callaghan, J.P. Hip Abductor Fatigability and Recovery Are Related to the Development of Low Back Pain During Prolonged Standing. J. Appl. Biomech. 2018, 34, 39–46. [Google Scholar] [CrossRef]
- Herrington, L. The Effect of Hip Abductor Muscle Fatigue on Frontal Plane Knee Projection Angle During Step Landing. Int. J. Athl. Ther. Train. 2014, 19, 38–43. [Google Scholar] [CrossRef]
- Benjaminse, A.; Webster, K.E.; Kimp, A.; Meijer, M.; Gokeler, A. Revised Approach to the Role of Fatigue in Anterior Cruciate Ligament Injury Prevention: A Systematic Review with Meta-Analyses. Sports Med. 2019, 49, 565–586. [Google Scholar] [CrossRef]
- Cowan, S.M.; Crossley, K.M. Does gender influence neuromotor control of the knee and hip? J. Electromyogr. Kinesiol. 2009, 19, 276–282. [Google Scholar] [CrossRef]
- Alsaleh, S.A.; Murphy, N.A.; Miller, S.C.; Morrissey, D.; Lack, S.D. Local neuromuscular characteristics associated with patellofemoral pain: A systematic review and meta-analysis. Clin. Biomech. 2021, 90, 105509. [Google Scholar] [CrossRef]
- Nakagawa, T.H.; Moriya, E.T.; Maciel, C.D.; Serrao, F.V. Trunk, pelvis, hip, and knee kinematics, hip strength, and gluteal muscle activation during a single-leg squat in males and females with and without patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 2012, 42, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.L.; Johnson, A.E.; Griffin, L. Sex differences in neuromuscular control of quadriceps. Eur. J. Appl. Physiol. 2020, 120, 2193–2202. [Google Scholar] [CrossRef]
- Merchant, A.C.; Arendt, E.A.; Dye, S.F.; Fredericson, M.; Grelsamer, R.P.; Leadbetter, W.B.; Post, W.R.; Teitge, R.A. The female knee: Anatomic variations and the female-specific total knee design. Clin. Orthop. Relat. Res. 2008, 466, 3059–3065. [Google Scholar] [CrossRef]
- Hunter, S.K. Sex differences in fatigability of dynamic contractions. Exp. Physiol. 2016, 101, 250–255. [Google Scholar] [CrossRef]
- Munro, A.; Herrington, L.; Carolan, M. Reliability of 2-dimensional video assessment of frontal-plane dynamic knee valgus during common athletic screening tasks. J. Sport Rehabil. 2012, 21, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Begalle, R.L.; Distefano, L.J.; Blackburn, T.; Padua, D.A. Quadriceps and hamstrings coactivation during common therapeutic exercises. J. Athl. Train. 2012, 47, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Paz, I.; Frigotto, M.F.; Cardoso, C.A.; Rabello, R.; Rodrigues, R. Hip abduction machine is better than free weights to target the gluteus medius while minimizing tensor fascia latae activation. J. Bodyw. Mov. Ther. 2022, 30, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Gonçalves, V.; Casagrande, R.; Cemin, F.; Nodari, C.; Borges, I.; Fitarelli, L.; Bianchesse, J.; Rocha, E.S.D.; Rabello, R. Are proximal and distal neuromuscular parameters able to predict hip and knee frontal plane kinematics during single-leg landing? Phys. Ther. Sport 2023, 59, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Rabello, R.; Nodari, C.; Scudiero, F.; Borges, I.; Fitarelli, L.; Bianchesse, J.; Rodrigues, R. Effects of task and hip-abductor fatigue on lower limb alignment and muscle activation. Sport Sci. Health 2022, 18, 759–769. [Google Scholar] [CrossRef]
- Lombardi, V.P. Beggining Weight Training: The Safe and Effective Way; W.C. Brown: Dubuque, Iowa, 1989. [Google Scholar]
- Scholtes, S.A.; Salsich, G.B. A Dynamic Valgus Index that combines hip and knee angles: Assessment of utility in females with patellofemoral pain. Int. J. Sports Phys. Ther. 2017, 12, 333–340. [Google Scholar]
- Graci, V.; Van Dillen, L.R.; Salsich, G.B. Gender differences in trunk, pelvis and lower limb kinematics during a single leg squat. Gait Posture 2012, 36, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Geiser, C.F.; O’Connor, K.M.; Earl, J.E. Effects of isolated hip abductor fatigue on frontal plane knee mechanics. Med. Sci. Sports Exerc. 2010, 42, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Patrek, M.F.; Kernozek, T.W.; Willson, J.D.; Wright, G.A.; Doberstein, S.T. Hip-abductor fatigue and single-leg landing mechanics in women athletes. J. Athl. Train. 2011, 46, 31–42. [Google Scholar] [CrossRef]
- Dwyer, M.K.; Boudreau, S.N.; Mattacola, C.G.; Uhl, T.L.; Lattermann, C. Comparison of lower extremity kinematics and hip muscle activation during rehabilitation tasks between sexes. J. Athl. Train. 2010, 45, 181–190. [Google Scholar] [CrossRef]
- Bolgla, L.; Cook, N.; Hogarth, K.; Scott, J.; West, C. Trunk and hip electromyographic activity during single leg squat exercises do sex differences exist? Int. J. Sports Phys. Ther. 2014, 9, 756–764. [Google Scholar] [PubMed]
- Besomi, M.; Maclachlan, L.; Mellor, R.; Vicenzino, B.; Hodges, P.W. Tensor Fascia Latae Muscle Structure and Activation in Individuals With Lower Limb Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 965–985. [Google Scholar] [CrossRef] [PubMed]
- Steiner, M.; Baur, H.; Blasimann, A. Sex-specific differences in neuromuscular activation of the knee stabilizing muscles in adults—A systematic review. Arch. Physiother. 2023, 13, 4. [Google Scholar] [CrossRef]
- Bencke, J.; Strøm, M.; Curtis, D.J.; Bandholm, T.; Zebis, M.K. Differences in Thigh Muscle Activation Between Standing and Landing Exercises for Knee Injury Prevention and Rehabilitation. Int. J. Sports Phys. Ther. 2023, 18, 102–112. [Google Scholar] [CrossRef] [PubMed]
- González-Izal, M.; Malanda, A.; Gorostiaga, E.; Izquierdo, M. Electromyographic models to assess muscle fatigue. J. Electromyogr. Kinesiol. 2012, 22, 501–512. [Google Scholar] [CrossRef]
- González-Izal, M.; Malanda, A.; Navarro-Amézqueta, I.; Gorostiaga, E.M.; Mallor, F.; Ibañez, J.; Izquierdo, M. EMG spectral indices and muscle power fatigue during dynamic contractions. J. Electromyogr. Kinesiol. 2010, 20, 233–240. [Google Scholar] [CrossRef]
- Beaulieu, M.L.; Lamontagne, M.; Xu, L. Gender differences in time-frequency EMG analysis of unanticipated cutting maneuvers. Med. Sci. Sports Exerc. 2008, 40, 1795–1804. [Google Scholar] [CrossRef]
- Leporace, G.; Pereira, G.R.; Nadal, J.; Batista, L.A. Differences in time-frequency representation of lower limbs myoelectric activity during single and double leg landing in male athletes. J. Electromyogr. Kinesiol. 2011, 21, 506–511. [Google Scholar] [CrossRef]
- von Tscharner, V.; Goepfert, B. Gender dependent EMGs of runners resolved by time/frequency and principal pattern analysis. J. Electromyogr. Kinesiol. 2003, 13, 253–272. [Google Scholar] [CrossRef]
- Roman-Liu, D. The influence of confounding factors on the relationship between muscle contraction level and MF and MPF values of EMG signal: A review. Int. J. Occup. Saf. Erg. 2016, 22, 77–91. [Google Scholar] [CrossRef]
- Nuzzo, J.L. Sex differences in skeletal muscle fiber types: A meta-analysis. Clin. Anat. 2024, 37, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Neyroud, D.; Ruttimann, J.; Mannion, A.F.; Millet, G.Y.; Maffiuletti, N.A.; Kayser, B.; Place, N. Comparison of neuromuscular adjustments associated with sustained isometric contractions of four different muscle groups. J. Appl. Physiol. 2013, 114, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Herrington, L.; Alenezi, F.; Alzhrani, M.; Alrayani, H.; Jones, R. The reliability and criterion validity of 2D video assessment of single leg squat and hop landing. J. Electromyogr. Kinesiol. 2017, 34, 80–85. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (n = 15) | Female (n = 15) | |
|---|---|---|
| Age (y) | 26.6 ± 4.2 | 25.6 ± 4.8 |
| Body mass (kg) | 85.7 ± 9.2 | 61 ± 8.8 * |
| Height (m) | 1.77 ± 0.05 | 1.63 ± 0.09 * |
| Body mass index (kg/m2) | 27.1 ± 2.2 | 22.9 ± 2.7 * |
| Estimated 1RM (kg) | 18.8 ± 3.1 | 12.1 ± 2.3 * |
| 20% of estimated 1RM (kg) | 3.8 ± 0.6 | 2.5 ± 0.5 * |
| Time to exhaustion (s) | 149.9 ± 56.3 | 159.6 ± 65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaviraghi, P.; Chaida Sonda, F.; Fernandes Frigotto, M.; Molinari, T.; Pizarro Chaffe, L.; Flor, J.L.; Rabello, R.; Rodrigues, R. Females Present Different Single-Leg Squat Kinematics and Muscle Activation Strategies than Males Even after Hip Abductor Fatigue. Biomechanics 2024, 4, 282-293. https://doi.org/10.3390/biomechanics4020017
Gaviraghi P, Chaida Sonda F, Fernandes Frigotto M, Molinari T, Pizarro Chaffe L, Flor JL, Rabello R, Rodrigues R. Females Present Different Single-Leg Squat Kinematics and Muscle Activation Strategies than Males Even after Hip Abductor Fatigue. Biomechanics. 2024; 4(2):282-293. https://doi.org/10.3390/biomechanics4020017
Chicago/Turabian StyleGaviraghi, Pablo, Francesca Chaida Sonda, Michele Fernandes Frigotto, Talita Molinari, Luiza Pizarro Chaffe, José Luis Flor, Rodrigo Rabello, and Rodrigo Rodrigues. 2024. "Females Present Different Single-Leg Squat Kinematics and Muscle Activation Strategies than Males Even after Hip Abductor Fatigue" Biomechanics 4, no. 2: 282-293. https://doi.org/10.3390/biomechanics4020017
APA StyleGaviraghi, P., Chaida Sonda, F., Fernandes Frigotto, M., Molinari, T., Pizarro Chaffe, L., Flor, J. L., Rabello, R., & Rodrigues, R. (2024). Females Present Different Single-Leg Squat Kinematics and Muscle Activation Strategies than Males Even after Hip Abductor Fatigue. Biomechanics, 4(2), 282-293. https://doi.org/10.3390/biomechanics4020017